Value Frameworks for Vaccines: Which Dimensions Are Most Relevant?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
- -
- If we tell you that VACCINEX is a safe or unsafe vaccine, that is probably a relevant argument.
- -
- If we tell you that VACCINEX is in a nice or ugly package, that is probably not a relevant argument.
2.2. Sample
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Plotkin, S.L.; Plotkin, S.A. A Short History of Vaccination. In Plotkin’s Vaccines, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 1–15.e8. [Google Scholar]
- Gonzalez-Lorenzo, M.; Piatti, A.; Coppola, L.; Gramegna, M.; Demicheli, V.; Melegaro, A.; Tirani, M.; Parmelli, E.; Auxilia, F.; Moja, L. Conceptual frameworks and key dimensions to support coverage decisions for vaccines. Vaccine 2015, 33, 1206–1217. [Google Scholar] [CrossRef] [Green Version]
- WHO. Choosing Interventions That Are Cost-Effective. 2014. Available online: http://www.who.int/choice/en (accessed on 22 October 2020).
- Houweling, H.; Verweij, M.; Ruitenberg, E.J. Criteria for inclusion of vaccinations in public programmes. Vaccine 2010, 28, 2924–2931. [Google Scholar] [CrossRef] [PubMed]
- Burchett, H.; Mounier-Jack, S.; Griffiths, U.K.; Mills, A. National decision-making on adopting new vaccines: A systematic review. Health Policy Plan. 2011, 27, ii62–ii76. [Google Scholar] [CrossRef] [Green Version]
- Mantel, C.F.; Wang, S.A. The privilege and responsibility of having choices: Decision-making for new vaccines in developing countries. Health Policy Plan. 2012, 27, ii1–ii4. [Google Scholar] [CrossRef]
- Nolan, T. The Australian model of immunization advice and vaccine funding. Vaccine 2010, 28, A76–A83. [Google Scholar] [CrossRef] [Green Version]
- Kimman, T.G.; Boot, H.J.; Berbers, G.A.M.; Bondt, P.E.V.-D.; De Wit, G.A.; Demelker, H. Developing a vaccination evaluation model to support evidence-based decision making on national immunization programs. Vaccine 2006, 24, 4769–4778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press.: Oxford, UK, 2005; Volume 3. [Google Scholar]
- Walker, D.G.; Hutubessy, R.; Beutels, P. WHO Guide for standardisation of economic evaluations of immunization programmes. Vaccine 2010, 28, 2356–2359. [Google Scholar] [CrossRef]
- IOM. Vaccines for the 21st Century: A Tool for Decisionmaking; Stratton, K.R., Durch, J.S., Lawrence, R.S., Eds.; The National Academies Press: Washington, DC, USA, 2000; p. 472. [Google Scholar]
- Knobler, S.L.; Bok, K.; Gellin, B. Informing vaccine decision-making: A strategic multi-attribute ranking tool for vaccines—SMART Vaccines 2.0. Vaccine 2017, 35, A43–A45. [Google Scholar] [CrossRef] [PubMed]
- Phelps, C.; Madhavan, G.; Sangha, K.; Rappuoli, R.; Colwell, R.R.; Martinez, R.M.; Kelley, P.; King, L. A priority-setting aid for new vaccine candidates. Proc. Natl. Acad. Sci. USA 2014, 111, 3199–3200. [Google Scholar] [CrossRef] [Green Version]
- Van Der Putten, I.; Hiligsmann, M.; Paulus, A.; Hutubessy, R.; Evers, S.M.A. Identifying the Broader Value of Vaccines in Low and Middle Income Countries. Value Health 2014, 17, A548. [Google Scholar] [CrossRef] [Green Version]
- Bärnighausen, T.; Berkley, S.; Bhutta, Z.A.; Bishai, D.M.; Black, M.M.; Bloom, D.E.; Constenla, D.; Driessen, J.; Edmunds, J.; Evans, D.; et al. Reassessing the value of vaccines. Lancet Glob. Health 2014, 2, e251–e252. [Google Scholar] [CrossRef] [Green Version]
- Sevilla, J.P.; Bloom, D.E.; Cadarette, D.; Jit, M.; Lipsitch, M. Toward economic evaluation of the value of vaccines and other health technologies in addressing AMR. Proc. Natl. Acad. Sci. USA 2018, 115, 12911–12919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jit, M.; Hutubessy, R.; Png, M.E.; Sundaram, N.; Audimulam, J.; Salim, S.; Yoong, J. The broader economic impact of vaccination: Reviewing and appraising the strength of evidence. BMC Med. 2015, 13, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luyten, J.; Beutels, P.; Beutels, P. Costing Infectious Disease Outbreaks for Economic Evaluation. PharmacoEconomics 2009, 27, 379–389. [Google Scholar] [CrossRef]
- Barnighausen, T. Valuing vaccination. Proc. Natl. Acad. Sci. USA 2014, 111, 12313–12319. [Google Scholar] [CrossRef] [Green Version]
- Bloom, D.E.; Fan, V.Y.; Sevilla, J.P. The broad socioeconomic benefits of vaccination. Sci. Transl. Med. 2018, 10, eaaj2345. [Google Scholar] [CrossRef]
- Bloom, D.E.; Brenzel, L.; Cadarette, D.; Sullivan, J. Moving beyond traditional valuation of vaccination: Needs and opportunities. Vaccine 2017, 35, A29–A35. [Google Scholar] [CrossRef]
- Luyten, J.; Beutels, P. The Social Value Of Vaccination Programs: Beyond Cost-Effectiveness. Health Aff. 2016, 35, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Beutels, P.; Scuffham, P.A.; MacIntyre, C.R. Funding of drugs: Do vaccines warrant a different approach? Lancet Infect. Dis. 2008, 8, 727–733. [Google Scholar] [CrossRef]
- Luyten, J.; Kessels, R.; Goos, P.; Beutels, P. Public Preferences for Prioritizing Preventive and Curative Health Care Interventions: A Discrete Choice Experiment. Value Health 2015, 18, 224–233. [Google Scholar] [CrossRef] [Green Version]
- Luyten, J.; Dorgali, V.; Hens, N.; Beutels, P. Public preferences over efficiency, equity and autonomy in vaccination policy: An empirical study. Soc. Sci. Med. 2013, 77, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Luyten, J.; Bruyneel, L.; Van Hoek, A.J. Assessing vaccine hesitancy in the UK population using a generalized vaccine hesitancy survey instrument. Vaccine 2019, 37, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- Luyten, J.; Kessels, R.; Atkins, K.E.; Jit, M.; van Hoek, A.J. Quantifying the public’s view on social value judgments in vaccine decision-making: A discrete choice experiment. Soc. Sci. Med. 2019, 228, 181–193. [Google Scholar] [CrossRef] [Green Version]
- Gong, J.; Zhang, Y.; Yang, Z.; Huang, Y.; Feng, J.; Zhang, W. The framing effect in medical decision-making: A review of the literature. Psychol. Health Med. 2013, 18, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Daniels, N.; Sabin, J. Setting Limits Fairly: Learning How to Share Resources for Health; Oxford University Press.: Oxford, UK, 2008. [Google Scholar]
- Annemans, L.; Beutels, P.; Bloom, D.; Debacker, W.; Ethgen, O.; Luyten, J.; Van Wilder, P.; Van Laethem, Y.; Willem, L.; Simoens, S. Economic evaluation of vaccines: Belgian reflections on the need for a broader perspective. Value Health 2020, in press. [Google Scholar]
- Bilcke, J.; Beutels, P.; Brisson, P.M.; Jit, M. Accounting for Methodological, Structural, and Parameter Uncertainty in Decision-Analytic Models. Med. Decis. Mak. 2011, 31, 675–692. [Google Scholar] [CrossRef]
- Brazier, J.; Ratcliffe, J.; Saloman, J.; Tsuchiya, A. Measuring and Valuing Health Benefits for Economic Evaluation; Oxford University Press: Oxford, UK, 2016. [Google Scholar]



{kind=link}
{kind=link}
| Criterion | Favourable Framing | Unfavourable Framing |
|---|---|---|
| Medical aspects of disease and vaccine | ||
| Mortality risk | Anyone who becomes infected with the disease (against which VACCINEX protects) has a high risk of dying. | Those who become infected with the disease (against which VACCINEX protects) do not run a risk of dying. |
| Severity of symptoms | Those who become infected with the disease (against which VACCINEX protects) get severe symptoms. | Those who become infected with the disease (against which VACCINEX protects) will only have mild symptoms. |
| Duration of symptoms | The symptoms of the disease (against which VACCINEX protects) persist for life. | The symptoms of the disease (against which VACCINEX protects) are temporary. |
| Comorbidity risk | Those who get the disease (against which VACCINEX protects) are later also more likely to get other diseases. | Those who get the disease (against which VACCINEX protects) do not run a higher risk of developing other diseases later on. |
| Transmis-sibility | The virus (against which VACCINEX protects) is very contagious and it will infect many people in Flanders. | The virus (against which VACCINEX protects) is not contagious and will infect few people in Flanders. |
| Timing symptoms | Anyone who becomes infected with the disease (against which VACCINEX protects) immediately develops symptoms. In other diseases, these only break through after a few years. | Those who become infected with the disease (against which VACCINEX protects) will only develop symptoms after a few years. In other diseases, these often break through immediately. |
| Eradication potential | If many people are vaccinated with VACCINEX, the disease can be eradicated so that future generations no longer need to be vaccinated. | No matter how many people are vaccinated with VACCINEX, the disease will never be eradicated. Future generations will also have to be vaccinated. |
| Availability of treatment | Those who become infected with the disease (against which VACCINEX protects) cannot be treated for this. | Those who become infected with the disease (against which VACCINEX protects) can be treated for this. |
| Prevention alternatives | Vaccination with VACCINEX is the only effective way to prevent the disease. | The disease against which VACCINEX protects can also be avoided in other ways than through vaccination. |
| Prevalence disease | The disease (against which VACCINEX protects) is common in Flanders. | The disease (against which VACCINEX protects) is rare in Flanders. |
| Transmis-sion mode | The disease (against which VACCINEX protects) is not spread through sexual contact but through the respiratory tract. | The disease (against which VACCINEX protects) is not spread through the respiratory tract, but through sexual contact. |
| Fertility impact | Anyone who becomes infected with the disease (against which VACCINEX protects) suffers damage to fertility and can therefore have an effect on both the existence and health of the offspring. | Anyone who is infected with the disease (against which VACCINEX protects) does not suffer any damage to fertility and this will therefore have no effect on the existence or health of the offspring. |
| Effectiveness vaccine | VACCINEX offers highly effective disease protection. | VACCINEX offers little effective disease protection. |
| Scientific certainty | There is good scientific certainty about the effects of VACCINEX. | There is much scientific uncertainty about the effects of VACCINEX. |
| Mild side-effects | Anyone who is vaccinated with VACCINEX will not experience any mild side-effects (e.g., headache, mild fever). | Anyone who is vaccinated with VACCINEX is at risk of some mild side-effects (e.g., headache, mild fever). |
| Severe side-effects | Anyone who is vaccinated with VACCINEX will not experience any serious side-effects (e.g., convulsions, severe allergic reaction). | Anyone who is vaccinated with VACCINEX is at risk of some serious side-effects (e.g., convulsions, severe allergic reaction). |
| Herd immunity | When many people are vaccinated with VACCINEX, “herd immunity” occurs and unvaccinated people are indirectly protected against the disease (because the risk of infection decreases). | No matter how many people are vaccinated with VACCINEX, no “herd immunity” occurs. Consequently, only the vaccinated themselves are protected. There is no indirect protective effect for unvaccinated persons. |
| Socio-economic aspects of disease and vaccine | ||
| Cost vaccine | VACCINEX is inexpensive compared to other vaccines. | VACCINEX is expensive compared to other vaccines. |
| Cost disease (public) | Anyone who becomes infected with the disease (against which VACCINEX protects) must undergo expensive treatment and this costs the government a lot of money. | Those who become infected with the disease (against which VACCINEX protects) must undergo inexpensive treatment. This does not cost the government much money. |
| Cost disease (private) | Anyone who becomes infected with the disease (against which VACCINEX protects) must undergo treatment and this will cost the patient a lot of money. | Anyone who becomes infected with the disease (against which VACCINEX protects) must undergo treatment, but this will cost the patient little money. |
| Platform costs | VACCINEX is easy and inexpensive to implement because it can be linked to other vaccinations already rolled out. As a result, no separate doctor’s appointment has to be made. | VACCINEX is difficult and more expensive to implement because it cannot be linked to other vaccinations that have already been rolled out. This means that a separate doctor’s appointment must always be made. |
| Productivity costs: absenteeism disease | Those who become infected with the disease (against which VACCINEX protects) cannot go to work for a long time. This lost time costs society a lot of money. | Those who become infected with the disease (against which VACCINEX protects) can quickly return to work. The lost time does not cost society a lot of money. |
| Productivity costs: presenteeism disease | Those who become infected with the disease (against which VACCINEX protects) are much less productive at work for a long time. | Those who become infected with the disease (against which VACCINEX protects) are equally productive at work. |
| Caregiver impact | Those who become infected with the disease (against which VACCINEX protects) need long-term help from their partner (informal care). | Those who become infected with the disease (against which VACCINEX protects) do not need help from their partner (no informal care). |
| Effect school results | If children become infected with the disease (against which VACCINEX protects), it has serious effects on their study results. | If children become infected with the disease (against which VACCINEX protects), this has no effect on their study results. |
| Domestic production | VACCINEX is produced by a Flemish company and therefore provides more employment in Flanders than vaccines produced abroad. | VACCINEX is produced by a foreign company and therefore provides less employment in Flanders than vaccines that are produced here. |
| Innovation stimulus | VACCINEX reimbursement provides a scientific stimulus and leads to more scientific innovation. | VACCINEX reimbursement does not provide scientific incentives and does not lead to more scientific innovation. |
| Goodwill and image | The disease (against which VACCINEX protects) is bad for the international image of Flanders and that has economic consequences (e.g., on tourism). | The disease (against which VACCINEX protects) does not damage the international image of Flanders and has no impact on e.g., tourism. |
| Health inequality impact | VACCINEX helps to reduce health inequalities between rich and poor. | VACCINEX does not help to reduce health inequalities between rich and poor. |
| Public health awareness | VACCINEX improves the general awareness of public health and the efforts it requires. | VACCINEX does not improve public awareness of public health and the efforts it requires. |
| Perception and fear | People have an excessive fear for the disease against which VACCINEX protects. | People do not have an excessive fear for the disease against which VACCINEX protects. |
| Anti-vaccination | If VACCINEX is refunded, there will be no protests from anti-vaccination groups. | If VACCINEX is refunded, protests will arise from anti-vaccination groups. |
| Legal liability | VACCINEX exposes the government to potential litigation less than other vaccines. | VACCINEX exposes the government to potential litigation more than other vaccines. |
| Target group: affects dis-advantaged | The disease (against which VACCINEX protects) is more common in disadvantaged groups. | The disease (against which VACCINEX protects) is rare in disadvantaged groups. |
| Target group: affects migrants | The disease (against which VACCINEX protects) is more common in migrants. | The disease (against which VACCINEX protects) is rare in migrants. |
| Target group: affects babies | The disease (against which VACCINEX protects) is more common in babies and young children. | The disease (against which VACCINEX protects) is rare in babies and young children. |
| Target group: affects elderly | The disease (against which VACCINEX protects) is more common in elderly people. | The disease (against which VACCINEX protects) is rare in elderly people. |
| Target group: affects LGBT | The disease (against which VACCINEX protects) is more common in people from the LGBT (lesbian-gay-bisexual-transgender) community. | The disease (against which VACCINEX protects) is rare in people from the LGBT (lesbian-gay-bisexual-transgender) community. |
| Target group: affects women | The disease (against which VACCINEX protects) is more common in women. | The disease (against which VACCINEX protects) is rare in women. |
| Target group: affects pregnant women | The disease (against which VACCINEX protects) is more common in pregnant women. | The disease (against which VACCINEX protects) is rare in pregnant women. |
| Characteristic | Sample 1 | Sample 2 | |||
|---|---|---|---|---|---|
| Favourable Framing | Unfavourable Framing | ||||
| n | % | n | % | ||
| Gender | Male | 245 | 49% | 245 | 49% |
| Female | 255 | 51% | 255 | 51% | |
| Age | 18–24 | 55 | 11% | 54 | 11% |
| 25–34 | 75 | 15% | 75 | 15% | |
| 35–44 | 80 | 16% | 80 | 16% | |
| 45–54 | 95 | 19% | 95 | 19% | |
| 55–64 | 155 | 31% | 159 | 32% | |
| 65–75 | 40 | 8% | 33 | 7% | |
| Educational Level | None | 8 | 2% | 9 | 2% |
| Primary school | 45 | 9% | 40 | 8% | |
| Secondary school | 302 | 60% | 306 | 61% | |
| Higher, non-university | 111 | 22% | 92 | 18% | |
| University or post-university | 33 | 7% | 46 | 9% | |
| Other | 1 | 0% | 7 | 1% | |
| Province | Antwerp | 140 | 28% | 140 | 28% |
| Limburg | 65 | 13% | 65 | 13% | |
| East-Flanders | 115 | 23% | 115 | 23% | |
| Flemish-Brabant | 85 | 17% | 85 | 17% | |
| West-Flanders | 95 | 19% | 95 | 19% | |
| Monthly Net Income | < €1000 | 77 | 15% | 68 | 14% |
| €1000–€1200 | 55 | 11% | 62 | 12% | |
| €1200–€1400 | 50 | 10% | 61 | 12% | |
| €1400–€1600 | 47 | 9% | 60 | 12% | |
| €1600–€1800 | 52 | 10% | 44 | 9% | |
| €1800–€2000 | 54 | 11% | 63 | 13% | |
| €2000–€2300 | 60 | 12% | 49 | 10% | |
| €2300–€2900 | 47 | 9% | 43 | 9% | |
| €2900–€3400 | 39 | 8% | 14 | 3% | |
| €3400–€4000 | 9 | 2% | 11 | 2% | |
| > €4000 | 10 | 2% | 23 | 5% | |
| Civil State | Single | 160 | 32% | 164 | 33% |
| Factual cohabitant | 59 | 12% | 54 | 11% | |
| Married | 176 | 35% | 177 | 35% | |
| Widowed | 10 | 2% | 8 | 2% | |
| Legal cohabitant | 42 | 8% | 37 | 7% | |
| Divorced | 53 | 11% | 60 | 12% | |
| TOTAL | 500 | 100% | 500 | 100% | |
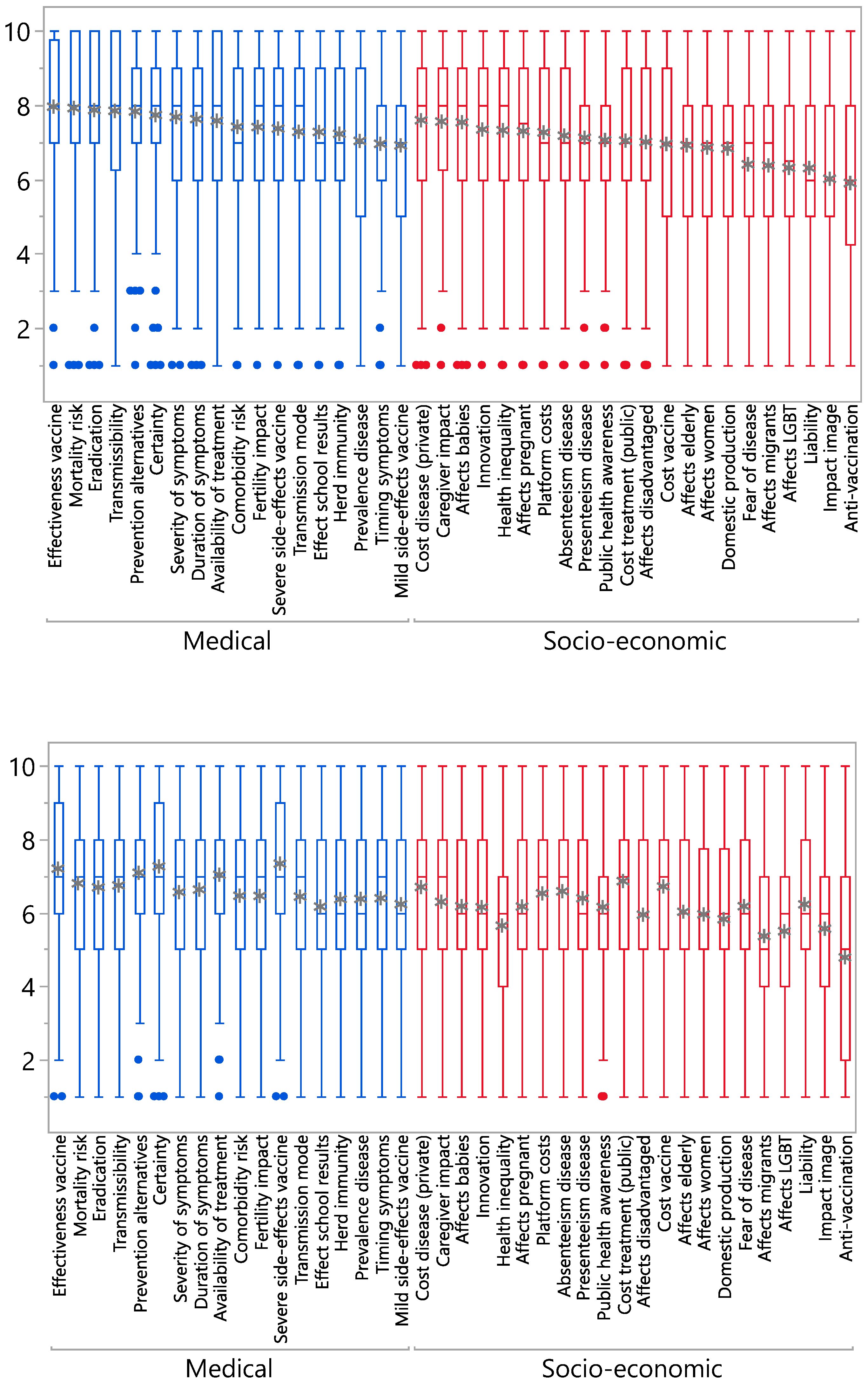
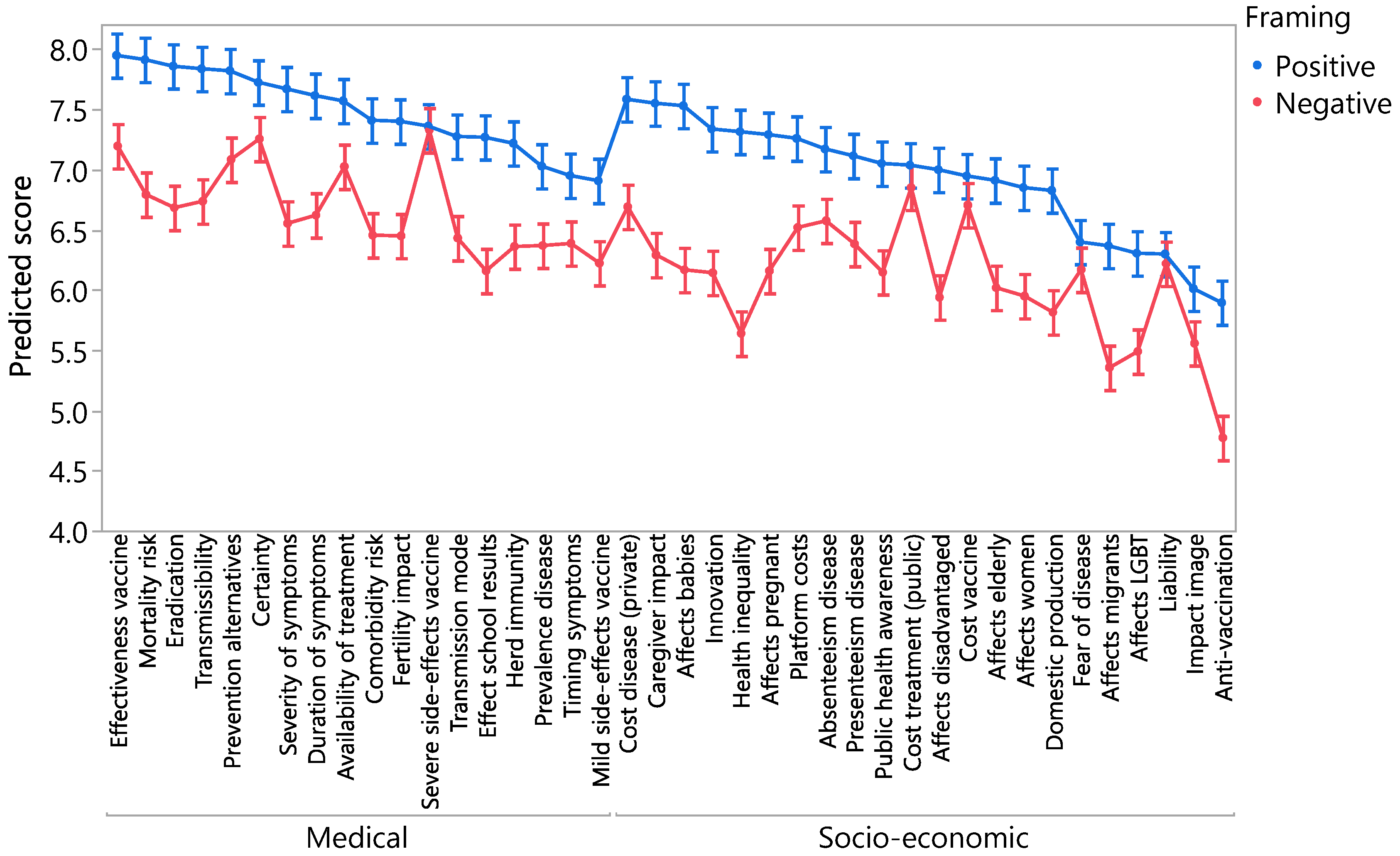
| A. Favourable Propositions | Mean | B. Unfavourable Propositions | Mean | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effectiveness vaccine | 7.9 | A | Severe side-effects vaccine | 7.3 | A | ||||||||||||||||||||||||||||||
| Mortality risk | 7.9 | A | Scientific certainty | 7.3 | A | B | |||||||||||||||||||||||||||||
| Eradication | 7.9 | A | B | Effectiveness vaccine | 7.2 | A | B | C | |||||||||||||||||||||||||||
| Transmissibility | 7.8 | A | B | C | Prevention alternatives | 7.1 | A | B | C | D | |||||||||||||||||||||||||
| Prevention alternatives | 7.8 | A | B | C | Availability of treatment | 7.0 | A | B | C | D | E | ||||||||||||||||||||||||
| Scientific certainty | 7.7 | A | B | C | D | Cost treatment (public) | 6.9 | A | B | C | D | E | F | ||||||||||||||||||||||
| Severity of symptoms | 7.7 | A | B | C | D | E | Mortality risk | 6.8 | B | C | D | E | F | G | |||||||||||||||||||||
| Duration of symptoms | 7.6 | A | B | C | D | E | F | Transmissibility | 6.7 | B | C | D | E | F | G | H | |||||||||||||||||||
| Cost disease (private) | 7.6 | A | B | C | D | E | F | Cost vaccine | 6.7 | C | D | E | F | G | H | ||||||||||||||||||||
| Availability of treatment | 7.6 | A | B | C | D | E | F | Cost disease (private) | 6.7 | C | D | E | F | G | H | I | |||||||||||||||||||
| Caregiver impact | 7.6 | A | B | C | D | E | F | G | Eradication | 6.7 | C | D | E | F | G | H | I | ||||||||||||||||||
| Target group: Affects babies | 7.5 | A | B | C | D | E | F | G | H | Duration of symptoms | 6.6 | D | E | F | G | H | I | J | |||||||||||||||||
| Comorbidity risk | 7.4 | B | C | D | E | F | G | H | I | Absenteeism disease | 6.6 | D | E | F | G | H | I | J | |||||||||||||||||
| Fertility impact | 7.4 | B | C | D | E | F | G | H | I | J | Severity of symptoms | 6.6 | D | E | F | G | H | I | J | ||||||||||||||||
| Severe side-effects vaccine | 7.4 | B | C | D | E | F | G | H | I | J | Platform costs | 6.5 | E | F | G | H | I | J | K | ||||||||||||||||
| Innovation | 7.3 | C | D | E | F | G | H | I | J | K | Comorbidity risks | 6.5 | F | G | H | I | J | K | L | ||||||||||||||||
| Health inequality | 7.3 | D | E | F | G | H | I | J | K | L | Fertility impact | 6.4 | F | G | H | I | J | K | L | ||||||||||||||||
| Target group: affects pregnant women | 7.3 | D | E | F | G | H | I | J | K | L | Transmission mode | 6.4 | F | G | H | I | J | K | L | ||||||||||||||||
| Transmission mode | 7.3 | D | E | F | G | H | I | J | K | L | Timing symptoms | 6.4 | F | G | H | I | J | K | L | ||||||||||||||||
| Effect school results | 7.3 | D | E | F | G | H | I | J | K | L | Presenteeism disease | 6.4 | F | G | H | I | J | K | L | ||||||||||||||||
| Platform costs | 7.3 | D | E | F | G | H | I | J | K | L | Prevalence disease | 6.4 | F | G | H | I | J | K | L | ||||||||||||||||
| Herd immunity | 7.2 | E | F | G | H | I | J | K | L | Herd immunity | 6.4 | F | G | H | I | J | K | L | |||||||||||||||||
| Absenteeism disease | 7.2 | E | F | G | H | I | J | K | L | Caregiver impact | 6.3 | G | H | I | J | K | L | M | |||||||||||||||||
| Presenteeism disease | 7.1 | F | G | H | I | J | K | L | Mild side-effects vaccine | 6.2 | H | I | J | K | L | M | |||||||||||||||||||
| Public health awareness | 7.1 | G | H | I | J | K | L | Liability | 6.2 | H | I | J | K | L | M | ||||||||||||||||||||
| cost treatment (public) | 7.0 | H | I | J | K | L | Fear and perception | 6.2 | I | J | K | L | M | N | |||||||||||||||||||||
| Prevalence disease | 7.0 | I | J | K | L | Target group: affects babies | 6.2 | I | J | K | L | M | N | ||||||||||||||||||||||
| Target group: affects disadvantaged | 7.0 | I | J | K | L | Target group: affects pregnant women | 6.2 | I | J | K | L | M | N | ||||||||||||||||||||||
| Timing symptoms | 7.0 | I | J | K | L | Effect school results | 6.2 | I | J | K | L | M | N | ||||||||||||||||||||||
| Cost vaccine | 6.9 | I | J | K | L | Public health awareness | 6.1 | J | K | L | M | N | |||||||||||||||||||||||
| Target group: affects elderly | 6.9 | I | J | K | L | Innovation | 6.1 | J | K | L | M | N | |||||||||||||||||||||||
| Mild side-effects vaccine | 6.9 | J | K | L | Target group: affects elderly | 6.0 | K | L | M | N | O | ||||||||||||||||||||||||
| Target group: affects women | 6.9 | K | L | M | Target group: affects women | 5.9 | L | M | N | O | |||||||||||||||||||||||||
| Domestic production | 6.8 | L | M | Target group: affects disadvantaged | 5.9 | L | M | N | O | ||||||||||||||||||||||||||
| Fear and perception | 6.4 | M | N | Domestic production | 5.8 | M | N | O | P | ||||||||||||||||||||||||||
| Target group: affects migrants | 6.4 | M | N | O | Health inequality | 5.6 | N | O | P | ||||||||||||||||||||||||||
| Target group: affects LGBT | 6.3 | N | O | Impact image | 5.6 | O | P | ||||||||||||||||||||||||||||
| Legal liability | 6.3 | N | O | Target group: affects LGBT | 5.5 | O | P | ||||||||||||||||||||||||||||
| Impact image | 6.0 | N | O | Target group: affects migrants | 5.4 | P | |||||||||||||||||||||||||||||
| Anti-vaccination | 5.9 | O | Anti-vaccination | 4.8 | Q |
| Favourable Statements | Unfavourable Statements | |||
|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 1 | Factor 2 | |
| Medical aspects | ||||
| Effectiveness vaccine | 0.81 | 0.14 | 0.82 | −0.02 |
| Mortality risk | 0.87 | 0.12 | 0.69 | 0.35 |
| Eradication | 0.76 | 0.21 | 0.42 | 0.48 |
| Transmissibility | 0.83 | 0.15 | 0.69 | 0.22 |
| Prevention alternatives | 0.79 | 0.14 | 0.73 | 0.14 |
| Certainty | 0.75 | 0.16 | 0.72 | −0.02 |
| Severity of symptoms | 0.78 | 0.20 | 0.61 | 0.36 |
| Duration of symptoms | 0.77 | 0.22 | 0.59 | 0.35 |
| Availability of treatment | 0.72 | 0.11 | 0.71 | 0.26 |
| Comorbidity risk | 0.72 | 0.24 | 0.48 | 0.53 |
| Fertility impact | 0.59 | 0.42 | 0.46 | 0.49 |
| Severe side-effects vaccine | 0.62 | 0.31 | 0.69 | 0.03 |
| Transmission mode | 0.48 | 0.45 | 0.41 | 0.51 |
| Effect school results | 0.53 | 0.43 | 0.33 | 0.59 |
| Herd immunity | 0.59 | 0.29 | 0.45 | 0.50 |
| Prevalence disease | 0.43 | 0.44 | 0.55 | 0.41 |
| Timing symptoms | 0.42 | 0.58 | 0.43 | 0.52 |
| Mild side-effects vaccine | 0.38 | 0.48 | 0.38 | 0.50 |
| Socio-economic aspects | ||||
| Cost disease (private) | 0.63 | 0.30 | 0.51 | 0.46 |
| Caregiver impact | 0.69 | 0.32 | 0.43 | 0.56 |
| Affects babies | 0.67 | 0.33 | 0.40 | 0.63 |
| Innovation | 0.40 | 0.51 | 0.37 | 0.50 |
| Health inequality | 0.45 | 0.46 | 0.10 | 0.64 |
| Affects pregnant | 0.53 | 0.41 | 0.37 | 0.66 |
| Platform costs | 0.48 | 0.37 | 0.50 | 0.46 |
| Absenteeism disease | 0.45 | 0.39 | 0.57 | 0.34 |
| Presenteeism disease | 0.43 | 0.55 | 0.48 | 0.50 |
| Public health awareness | 0.37 | 0.52 | 0.35 | 0.53 |
| Cost treatment (public) | 0.42 | 0.27 | 0.58 | 0.27 |
| Affects disadvantaged | 0.33 | 0.59 | 0.26 | 0.69 |
| Cost vaccine | 0.43 | 0.36 | 0.51 | 0.34 |
| Affects elderly | 0.35 | 0.58 | 0.25 | 0.72 |
| Affects women | 0.40 | 0.60 | 0.35 | 0.64 |
| Domestic production | 0.19 | 0.57 | 0.20 | 0.59 |
| Fear of disease | 0.12 | 0.49 | 0.50 | 0.51 |
| Affects migrants | 0.14 | 0.63 | 0.04 | 0.70 |
| Affects LGBT | 0.17 | 0.61 | 0.09 | 0.76 |
| Liability | 0.11 | 0.61 | 0.40 | 0.41 |
| Impact image | 0.04 | 0.45 | 0.12 | 0.62 |
| Anti-vaccination | −0.08 | 0.48 | −0.09 | 0.64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luyten, J.; Kessels, R.; Vandermeulen, C.; Beutels, P. Value Frameworks for Vaccines: Which Dimensions Are Most Relevant? Vaccines 2020, 8, 628. https://doi.org/10.3390/vaccines8040628
Luyten J, Kessels R, Vandermeulen C, Beutels P. Value Frameworks for Vaccines: Which Dimensions Are Most Relevant? Vaccines. 2020; 8(4):628. https://doi.org/10.3390/vaccines8040628
Chicago/Turabian StyleLuyten, Jeroen, Roselinde Kessels, Corinne Vandermeulen, and Philippe Beutels. 2020. "Value Frameworks for Vaccines: Which Dimensions Are Most Relevant?" Vaccines 8, no. 4: 628. https://doi.org/10.3390/vaccines8040628