Immunogenicity and Immune Memory after a Pneumococcal Polysaccharide Vaccine Booster in a High-Risk Population Primed with 10-Valent or 13-Valent Pneumococcal Conjugate Vaccine: A Randomized Controlled Trial in Papua New Guinean Children

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Study Vaccines
2.4. Study Procedures and Specimen Collection
2.5. Immunogenicity Assessment
2.6. Safety Assessment
2.7. Statistical Methods
3. Results
3.1. Study Population
3.2. Reactogenicity, Safety and Morbidity
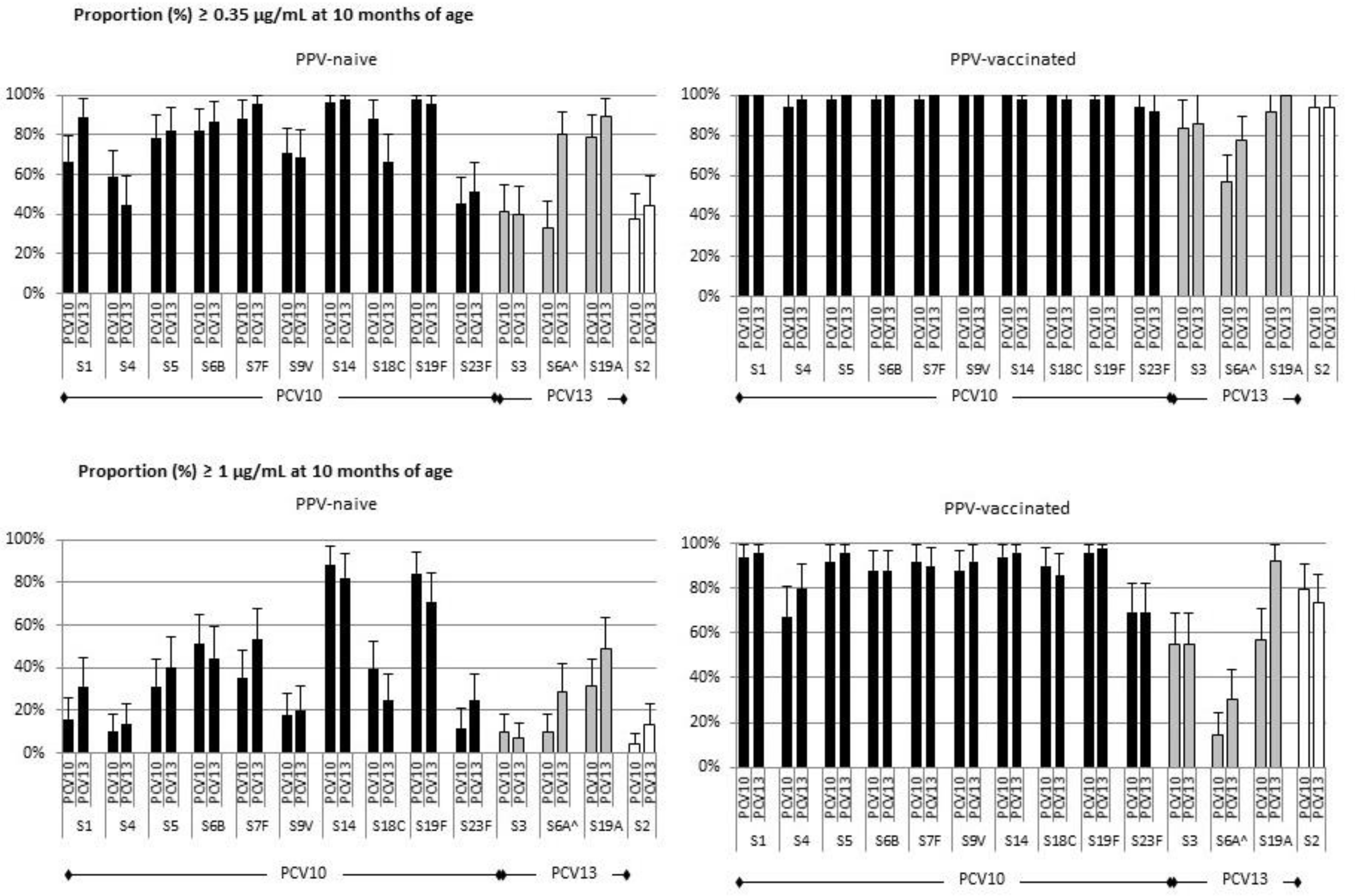
3.3. PPV Immunogenicity and Seroprotection Rates at 10 Months of Age in PCV10- and PCV13-Primed Children
3.4. Persistence of Serotype-Specific IgG Responses at 23 Months of Age
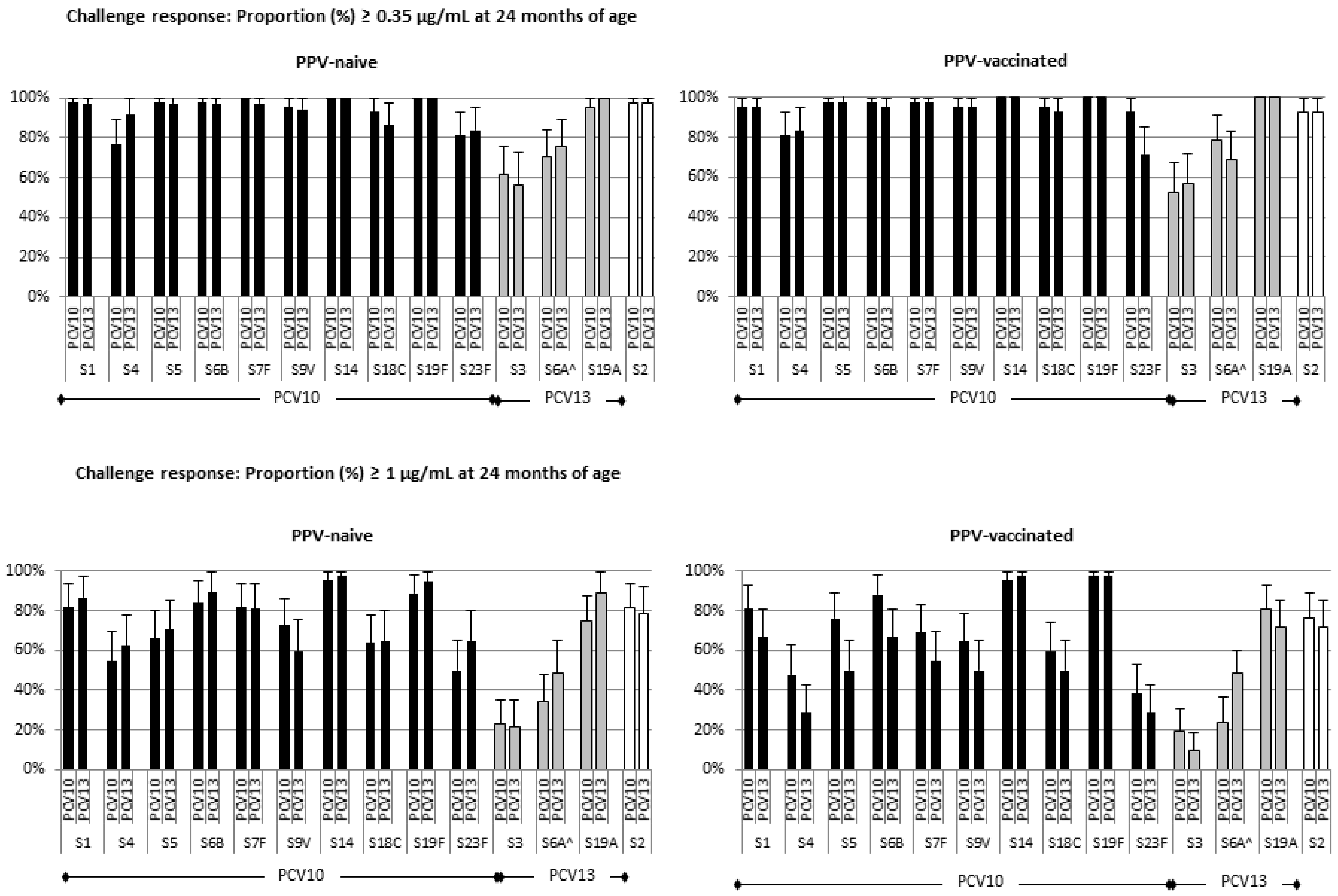
3.5. Response of PPV-Vaccinated and PPV-Naive Children to a Pneumococcal Challenge at 23 Months of Age
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- O’Brien, K.L.; Wolfson, L.J.; Watt, J.P.; Henkle, E.; Deloria-Knoll, M.; McCall, N.; Lee, E.; Mulholland, K.; Levine, O.S.; Cherian, T.; et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: Global estimates. Lancet 2009, 374, 893–902. [Google Scholar] [CrossRef]
- Whitney, C.G.; Goldblatt, D.; O’Brien, K.L. Dosing schedules for pneumococcal conjugate vaccine: Considerations for policy makers. Pediatr. Infect. Dis. J. 2014, 33 (Suppl 2), S172–S181. [Google Scholar] [CrossRef]
- Aho, C.; Michael, A.; Yoannes, M.; Greenhill, A.R.; Jacoby, P.; Reeder, J.; Pomat, W.; Saleu, G.; Namuigi, P.; Phuanukoonnon, S.; et al. Limited impact of neonatal or early infant schedules of 7-valent pneumooccal conjugate vaccination on nasopharyngeal carriage of Streptococcus pneumoniae in Papua New Guinean children: A randomized controlled trial. Vaccine Rep. 2016, 6, 36–43. [Google Scholar] [CrossRef]
- Greenhill, A.R.; Phuanukoonnon, S.; Michael, A.; Yoannes, M.; Orami, T.; Smith, H.; Murphy, D.; Blyth, C.; Reeder, J.; Siba, P.; et al. Streptococcus pneumoniae and Haemophilus influenzae in paediatric meningitis patients at Goroka General Hospital, Papua New Guinea: Serotype distribution and antimicrobial susceptibility in the pre-vaccine era. BMC Infect. Dis. 2015, 15, 485. [Google Scholar] [CrossRef] [PubMed]
- Pomat, W.S.; Van den Biggelaar, A.H.J.; Wana, S.; Greenhill, A.R.; Ford, R.; Orami, T.; Passey, M.; Jacoby, P.; Kirkham, L.A.; Lehmann, D.; et al. Safety and immunogenicity of pneumococcal conjugate vaccines in a high-risk population: A randomised controlled trial of 10-valent and 13-valent PCV in Papua New Guinean infants. Clin. Infect. Dis. 2018. [Google Scholar] [CrossRef] [PubMed]
- Russell, F.M.; Carapetis, J.R.; Balloch, A.; Licciardi, P.V.; Jenney, A.W.; Tikoduadua, L.; Waqatakirewa, L.; Pryor, J.; Nelson, J.; Byrnes, G.B.; et al. Hyporesponsiveness to re-challenge dose following pneumococcal polysaccharide vaccine at 12 months of age, a randomized controlled trial. Vaccine 2010, 28, 3341–3349. [Google Scholar] [CrossRef] [PubMed]
- Phuanukoonnon, S.; Reeder, J.; Pomat, W.; Van den Biggelaar, A.; Holt, P.; Saleu, G.; Opa, C.; Michael, A.; Aho, C.; Yoannes, M.; et al. A neonatal pneumococcal conjugate vaccine trial in Papua New Guinea: Study population, methods and operational challenges. PNG Med. J. 2010, 53, 191–206. [Google Scholar]
- Pomat, W.S.; van den Biggelaar, A.H.; Phuanukoonnon, S.; Francis, J.; Jacoby, P.; Siba, P.M.; Alpers, M.P.; Reeder, J.C.; Holt, P.G.; Richmond, P.C.; et al. Neonatal Pneumococcal Conjugate Vaccine Trial Study Team, Safety and immunogenicity of neonatal pneumococcal conjugate vaccination in Papua New Guinean children: A randomised controlled trial. PLoS ONE 2013, 8, e56698. [Google Scholar] [CrossRef]
- Lehmann, D.; Marshall, T.F.; Riley, I.D.; Alpers, M.P. Effect of pneumococcal vaccine on morbidity from acute lower respiratory tract infections in Papua New Guinean children. Ann. Trop. Paediatr. 1991, 11, 247–257. [Google Scholar] [CrossRef]
- Riley, I.D.; Lehmann, D.; Alpers, M.P.; Marshall, T.F.; Gratten, H.; Smith, D. Pneumococcal vaccine prevents death from acute lower-respiratory-tract infections in Papua New Guinean children. Lancet 1986, 2, 877–881. [Google Scholar] [CrossRef]
- Van den Biggelaar, A.H.J.; Richmond, P.C.; Fuery, A.; Anderson, D.; Opa, C.; Saleu, G.; Lai, M.; Francis, J.P.; Alpers, M.P.; Pomat, W.S.; et al. Pneumococcal responses are similar in Papua New Guinean children aged 3–5 years vaccinated in infancy with pneumococcal polysaccharide vaccine with or without prior pneumococcal conjugate vaccine, or without pneumococcal vaccination. PLoS ONE 2017, 12, e0185877. [Google Scholar] [CrossRef] [PubMed]
- Licciardi, P.V.; Toh, Z.Q.; Clutterbuck, E.A.; Balloch, A.; Marimla, R.A.; Tikkanen, L.; Lamb, K.E.; Bright, K.J.; Rabuatoka, U.; Tikoduadua, L.; et al. No long-term evidence of hyporesponsiveness after use of pneumococcal conjugate vaccine in children previously immunized with pneumococcal polysaccharide vaccine. J. Allergy Clin. Immunol. 2016, 137, 1772–1779. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, D.; Kirarock, W.; van den Biggelaar, A.H.J.; Passey, M.; Jacoby, P.; Saleu, G.; Masiria, G.; Nivio, B.; Greenhill, A.; Orami, T.; et al. Rationale and methods of a randomized controlled trial of immunogenicity, safety and impact on carriage of pneumococcal conjugate and polysaccharide vaccines in infants in Papua New Guinea. Pneumonia 2017, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Goldblatt, D.; Plikaytis, B.D.; Akkoyunlu, M.; Antonello, J.; Ashton, L.; Blake, M.; Burton, R.; Care, R.; Durant, N.; Feavers, I.; et al. Establishment of a new human pneumococcal standard reference serum, 007sp. Clin. Vaccine Immunol. 2011, 18, 1728–1736. [Google Scholar] [CrossRef] [PubMed]
- Balloch, A.; Licciardi, P.V.; Leach, A.; Nurkka, A.; Tang, M.L. Results from an inter-laboratory comparison of pneumococcal serotype-specific IgG measurement and critical parameters that affect assay performance. Vaccine 2010, 28, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Pneumoccal Serology Reference Laboratories Training Manual for Enzyme Linked Immunosorbent assay for the Quantitation of Streptococcus pneumoniae Serotype Specific IgG (Pn PS ELISA). Available online: https://www.vaccine.uab.edu/ELISA%20Protocol.pdf (accessed on 1 June 2017).
- Pomat, W.S.; Phuanukoonnon, S.; van den Biggelaar, A.H.; Richmond, P.; Francis, J.P.; Holt, P.G.; Siba, P.M.; Lehmann, D. Alternative pneumococcal vaccination schedules for high-risk populations: Immunogenicity of neonatal pneumococcal conjugate vaccine & pneumococcal polysaccharide vaccine in Papua New Guinean children. In Proceedings of the 7th International Symposium on Pneumococci and Pneumococcal Disease, Tel Aviv, Israel, 14–18 March 2010. [Google Scholar]
- Siber, G.R.; Chang, I.; Baker, S.; Fernsten, P.; O’Brien, K.L.; Santosham, M.; Klugman, K.P.; Madhi, S.A.; Paradiso, P.; Kohberger, R. Estimating the protective concentration of anti-pneumococcal capsular polysaccharide antibodies. Vaccine 2007, 25, 3816–3826. [Google Scholar] [CrossRef]
- Thisyakorn, U.; Chokephaibulkit, K.; Kosalaraksa, P.; Benjaponpitak, S.; Pancharoen, C.; Chuenkitmongkol, S. Immunogenicity and safety of 23-valent pneumococcal polysaccharide vaccine as a booster dose in 12- to 18-month-old children primed with 3 doses of 7-valent pneumococcal conjugate vaccine. Hum. Vaccine Immunother. 2014, 10, 1859–1865. [Google Scholar] [CrossRef]
- Balsells, E.; Guillot, L.; Nair, H.; Kyaw, M.H. Serotype distribution of Streptococcus pneumoniae causing invasive disease in children in the post-PCV era: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0177113. [Google Scholar] [CrossRef]
- Laferriere, C. The immunogenicity of pneumococcal polysaccharides in infants and children: A meta-regression. Vaccine 2011, 29, 6838–6847. [Google Scholar] [CrossRef]
- Mackenzie, G.A.; Hill, P.C.; Jeffries, D.J.; Hossain, I.; Uchendu, U.; Ameh, D.; Ndiaye, M.; Adeyemi, O.; Pathirana, J.; Olatunji, Y.; et al. Effect of the introduction of pneumococcal conjugate vaccination on invasive pneumococcal disease in The Gambia: A population-based surveillance study. Lancet Infect. Dis. 2016, 16, 703–711. [Google Scholar] [CrossRef]
- Plosker, G.L. 10-Valent pneumococcal non-typeable Haemophilus influenzae protein D-conjugate vaccine: A review in infants and children. Pediatr. Drugs 2014, 16, 425–444. [Google Scholar]
- Lee, L.H.; Frasch, C.E.; Falk, L.A.; Klein, D.L.; Deal, C.D. Correlates of immunity for pneumococcal conjugate vaccines. Vaccine 2003, 21, 2190–2196. [Google Scholar] [CrossRef]
- Le Polain De Waroux, O.; Flasche, S.; Prieto-Merino, D.; Goldblatt, D.; Edmunds, W.J. The efficacy and duration of protection of pneumococcal conjugate vaccines against nasopharyngeal carriage: A meta-regression model. Pediatr. Infect. Dis. J. 2015, 34, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Russell, F.M.; Balloch, A.; Licciardi, P.V.; Carapetis, J.R.; Tikoduadua, L.; Waqatakirewa, L.; Cheung, Y.B.; Mulholland, E.K.; Tang, M.L. Serotype-specific avidity is achieved following a single dose of the 7-valent pneumococcal conjugate vaccine, and is enhanced by 23-valent pneumococcal polysaccharide booster at 12 months. Vaccine 2011, 29, 4499–4506. [Google Scholar] [CrossRef] [PubMed]
- Russell, F.M.; Carapetis, J.R.; Burton, R.L.; Lin, J.; Licciardi, P.V.; Balloch, A.; Tikoduadua, L.; Waqatakirewa, L.; Cheung, Y.B.; Tang, M.L.; et al. Opsonophagocytic activity following a reduced dose 7-valent pneumococcal conjugate vaccine infant primary series and 23-valent pneumococcal polysaccharide vaccine at 12 months of age. Vaccine 2011, 29, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, D.; Vail, J.; Firth, M.J.; de Klerk, N.H.; Alpers, M.P. Benefits of routine immunizations on childhood survival in Tari, Southern Highlands Province, Papua New Guinea. Int. J. Epidemiol. 2005, 34, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Blanchard Rohner, G.; Snape, M.D.; Kelly, D.F.; John, T.; Morant, A.; Yu, L.M.; Borkowski, A.; Ceddia, F.; Borrow, R.; Siegrist, C.A.; et al. The magnitude of the antibody and memory B cell responses during priming with a protein-polysaccharide conjugate vaccine in human infants is associated with the persistence of antibody and the intensity of booster response. J. Immunol. 2008, 180, 2165–2173. [Google Scholar] [CrossRef] [PubMed]
- Granoff, D.M.; Pollard, A.J. Reconsideration of the use of meningococcal polysaccharide vaccine. Pediatr. Infect. Dis. J. 2007, 26, 716–722. [Google Scholar] [CrossRef]
- Poolman, J.; Borrow, R. Hyporesponsiveness and its clinical implications after vaccination with polysaccharide or glycoconjugate vaccines. Expert Rev. Vaccines 2011, 10, 307–322. [Google Scholar] [CrossRef]
- Papadatou, I.; Spoulou, V. Pneumococcal vaccination in high-risk individuals: Are we doing it right? Clin. Vaccine Immunol. 2016, 23, 388–395. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Adverse Event | PPV-Naive | PPV-Vaccinated | ||||||
|---|---|---|---|---|---|---|---|---|
| PCV10-Primed | PCV13-Primed | PCV10-Primed | PCV13-Primed | |||||
| Episodes | Incidence (ppy) (95% CI) | Episodes | Incidence (ppy) (95% CI) | Episodes | Incidence (ppy) (95% CI) | Episodes | Incidence (ppy) (95% CI) | |
| Any morbidity | 79 | 1.27 (1.02–1.59) | 84 | 1.54 (1.24–1.90) | 85 | 1.42 (1.15–1.76) | 83 | 1.36 (1.10–1.68) |
| Any ALRI | 25 | 0.40 (0.27–0.60) | 26 | 0.48 (0.32–0.70) | 30 | 0.50 (0.35–0.72) | 26 | 0.43 (0.29–0.62) |
| Moderate/severe ALRI | 12 | 0.19 (0.11–0.34) | 6 | 0.11 (0.05–0.24) | 13 | 0.22 (0.13–0.37) | 11 | 0.18 (0.10–0.33) |
| Hospitalizations | 7 | 0.11 (0.05–0.24) | 4 | 0.07 (0.03–0.19) | 0 | 0 (0–0) | 3 | 0.05 (0.02–0.15) |
| Serotypes | Priming | PPV-Naive | PPV-Vaccinated | ||||
|---|---|---|---|---|---|---|---|
| GMC IgG (µg/mL) (95% CI) | GM Fold Change (95% CI) | GMC IgG (µg/mL) (95% CI) | GM Fold Change (95% CI) | ||||
| 9 Months | 10 Months | 9 Months | 10 Months | ||||
| PCV10/PCV13 serotypes | |||||||
| 1 | PCV10 | 0.57 (0.46–0.70) | 0.51 (0.38–0.68) | 0.86 (0.69–1.08) | 0.70 (0.56–0.88) | 7.52 (5.62–10.06) | 10.45 (7.92–13.79) |
| PCV13 | 0.98 (0.76–1.27) | 0.79 (0.60–1.04) | 0.80 (0.70–0.90) | 0.83 (0.70–0.98) | 5.65 (4.25–7.51) | 6.82 (5.19–8.97) | |
| 4 | PCV10 | 0.42 (0.34–0.52) | 0.39 (0.32–0.49) | 0.90 (0.78–1.03) | 0.48 (0.40–0.59) | 1.68 (1.27–2.23) | 3.37 (2.63–4.30) |
| PCV13 | 0.43 (0.34–0.55) | 0.37 (0.28–0.48) | 0.84 (0.70–1.01) | 0.39 (0.32–0.46) | 2.44 (1.89–3.17) | 6.40 (4.97–8.25) | |
| 5 | PCV10 | 0.67 (0.56–0.82) | 0.64 (0.51–0.80) | 0.91 (0.79–1.04) | 0.64 (0.52–0.78) | 3.09 (2.45–3.91) | 4.91 (3.81–6.33) |
| PCV13 | 0.87 (0.69–1.10) | 0.72 (0.55–0.94) | 0.81 (0.69–0.94) | 0.77 (0.64–0.93) | 2.65 (2.15–3.26) | 3.38 (2.63–4.34) | |
| 6B | PCV10 | 1.00 (0.80–1.25) | 0.94 (0.74–1.19) | 0.97 (0.87–1.09) | 1.18 (0.93–1.51) | 3.85 (2.86–5.18) | 3.19 (2.56–3.96) |
| PCV13 | 0.96 (0.73–1.27) | 0.88 (0.66–1.18) | 0.91 (0.74–1.11) | 0.77 (0.63–0.95) | 4.08 (3.05–5.45) | 5.40 (3.99–7.31) | |
| 7F | PCV10 | 0.77 (0.65–0.92) | 0.73 (0.59–0.90) | 0.93 (0.82–1.05) | 0.81 (0.66–1.00) | 3.21 (2.54–4.05) | 3.82 (3.10–4.70) |
| PCV13 | 1.21 (0.97–1.51) | 1.01 (0.81–1.26) | 0.83 (0.72–0.95) | 0.92 (0.76–1.10) | 3.15 (2.52–3.96) | 3.45 (2.77–4.31) | |
| 9V | PCV10 | 0.54 (0.46–0.65) | 0.50 (0.39–0.64) | 0.87 (0.76–1.01) | 0.62 (0.52–0.74) | 4.45 (3.36–5.89) | 7.04 (5.26–9.41) |
| PCV13 | 0.66 (0.54–0.80) | 0.48 (0.39–0.59) | 0.78 (0.65–0.93) | 0.48 (0.39–0.59) | 3.32 (2.60–4.25) | 7.13 (5.45–9.34) | |
| 14 | PCV10 | 3.05 (2.45–3.78) | 2.64 (2.06–3.37) | 0.85 (0.74–0.98) | 2.93 (2.16–3.98) | 9.11 (6.39–12.98) | 3.05 (2.11–4.40) |
| PCV13 | 4.09 (2.99–6.60) | 3.31 (2.44–4.49) | 0.81 (0.72–0.90) | 3.49 (2.63–4.65) | 6.39 (4.63–8.82) | 1.86 (1.53–2.28) | |
| 18C | PCV10 | 1.02 (0.82–1.27) | 0.89 (0.71–1.11) | 0.84 (0.75–0.93) | 0.89 (0.71–1.11) | 2.69 (2.06–3.51) | 2.90 (2.24–3.75) |
| PCV13 | 0.66 (0.54–0.81) | 0.51 (0.41–0.64) | 0.77 (0.69–0.86) | 0.63 (0.52–0.78) | 2.82 (2.16–3.67) | 4.71 (3.59–6.17) | |
| 19F | PCV10 | 2.39 (1.91–3.00) | 2.52 (1.96–3.23) | 1.02 (0.90–1.16) | 2.30 (1.86–2.86) | 7.35 (5.45–9.93) | 3.10 (2.47–3.89) |
| PCV13 | 1.96 (1.51–2.56) | 1.73 (1.31–2.30) | 0.90 (0.76–1.06) | 1.58 (1.25–1.99) | 9.50 (7.41–12.18) | 6.25 (4.73–8.27) | |
| 23F | PCV10 | 0.38 (0.30–0.49) | 0.36 (0.28–0.46) | 0.91 (0.74–1.13) | 0.47 (0.38–0.60) | 1.63 (1.20–2.22) | 3.40 (2.57–4.49) |
| PCV13 | 0.45 (0.34–0.60) | 0.38 (0.27–0.52) | 0.84 (0.69–1.02) | 0.42 (0.32–0.56) | 2.08 (1.52–2.83) | 5.24 (3.68–7.47) | |
| PCV13 serotypes | |||||||
| 3 | PCV10 | 0.33 (0.24–0.44) | 0.29 (0.22–0.37) | 0.87 (0.76–1.00) | 0.36 (0.27–0.48) | 0.94 (0.70–1.27) | 2.38 (1.79–3.17) |
| PCV13 | 0.30 (0.21–0.41) | 0.28 (0.21–0.38) | 0.93 (0.80–1.07) | 0.30 (0.24–0.37) | 1.05 (0.83–1.35) | 3.61 (2.80–4.67) | |
| 6A^ | PCV10 | 0.24 (0.19–0.30) | 0.24 (0.18–0.31) | 0.95 (0.85–1.07) | 0.27 (0.21–0.35) | 0.45 (0.34–0.58) | 1.56 (1.32–1.84) |
| PCV13 | 0.64 (0.47–0.88) | 0.59 (0.44–0.80) | 0.92 (0.76–1.12) | 0.42 (0.33–0.52) | 0.67 (0.53–0.85) | 1.61 (1.31–1.98) | |
| 19A | PCV10 | 0.81 (0.65–1.02) | 0.79 (0.61–1.02) | 0.96 (0.85–1.09) | 0.91 (0.73–1.14) | 1.31 (0.93–1.83) | 1.41 (1.17–1.70) |
| PCV13 | 1.32 (0.94–1.84) | 1.02 (0.71–1.46) | 0.80 (0.66–0.97) | 1.14 (0.88–1.46) | 3.80 (2.80–5.15) | 3.38 (2.46–4.63) | |
| Non-PCV serotype | |||||||
| 2 | PCV10 | 0.30 (0.25–0.37) | 0.29 (0.24–0.35) | 0.94 (0.74–1.21) | 0.34 (0.27–0.44) | 2.05 (1.51–2.78) | 5.96 (4.33–8.22) |
| PCV13 | 0.38 (0.24–0.43) | 0.32 (0.25–0.43) | 0.84 (0.67–1.06) | 0.30 (0.26–0.35) | 1.80 (1.35–2.39) | 6.02 (4.45–8.15) | |
| Serotypes | Priming | 23 Months IgG GMC (µg/mL) (95% CI) | 24 Months IgG GMC (µg/mL) (95% CI) | Fold-Change 24 Months/23 Months (95% CI) | Relative Fold-Change (95% CI) | |||
|---|---|---|---|---|---|---|---|---|
| PPV-Naive | PPV-Vaccinated | PPV-Naive | PPV-Vaccinated | PPV-Naive | PPV-Vaccinated | PPV-Vaccinated/PPV-Naive | ||
| PCV10/PCV13 serotypes | ||||||||
| 1 | PCV10 | 0.58 (0.43–0.79) | 1.06 (0.81–1.39) | 2.45 (1.88–3.20) | 1.89 (1.43–2.51) | 4.13 (2.87–5.95) | 1.85 (1.49–2.28) | 0.62 (0.43–0.89) |
| PCV13 | 0.70 (0.49–1.02) | 0.85 (0.65–1.11) | 2.51 (1.85–3.42) | 1.39 (1.04–1.86) | 3.49 (2.46–4.95) | 1.76 (1.40–2.21) | 0.53 (0.37–0.76) | |
| 4 | PCV10 | 0.29 (0.23–0.38) | 0.47 (0.39–0.57) | 0.86 (0.63–1.16) | 0.85 (0.66–1.09) | 2.81 (2.07–3.81) | 1.84 (1.46–2.32) | 0.79 (0.55–1.15) |
| PCV13 | 0.41 (0.29–0.58) | 0.37 (0.29–0.47) | 1.34 (0.97–1.85) | 0.67 (0.54–0.83) | 3.23 (2.27–4.59) | 1.88 (1.50–2.36) | 0.54 (0.39–0.76) | |
| 5 | PCV10 | 0.68 (0.54–0.85) | 1.00 (0.81–1.23) | 1.62 (1.29–2.05) | 1.45 (1.15–1.83) | 2.34 (1.76–3.11) | 1.45 (1.15–1.82) | 0.77 (0.56–1.07) |
| PCV13 | 0.86 (0.65–1.14) | 0.86 (0.70–1.06) | 1.73 (1.30–2.32) | 1.08 (0.87–1.33) | 2.02 (1.59–2.57) | 1.28 (1.09–1.50) | 0.63 (0.49–0.82) | |
| 6B | PCV10 | 0.98 (0.76–1.25) | 1.39 (1.11–1.74) | 2.93 (2.24–3.83) | 2.34 (1.80–3.03) | 2.88 (2.16–3.85) | 1.72 (1.36–2.17) | 0.70 (0.50–0.99) |
| PCV13 | 1.26 (0.93–1.71) | 1.00 (0.76–1.32) | 3.93 (3.01–5.13) | 1.31 (1.02–1.69) | 3.15 (2.35–4.23) | 1.39 (1.13–1.70) | 0.39 (0.29–0.53) | |
| 7F | PCV10 | 0.72 (0.57–0.90) | 1.12 (0.93–1.34) | 1.85 (1.48–2.32) | 1.55 (1.25–1.92) | 2.52 (1.95–3.25) | 1.37 (1.18–1.60) | 0.67 (0.51–0.89) |
| PCV13 | 0.98 (0.76–1.27) | 0.83 (0.65–1.04) | 2.19 (1.69–2.85) | 1.24 (1.01–1.51) | 2.18 (1.77–2.68) | 1.53 (1.30–1.79) | 0.66 (0.52–0.83) | |
| 9V | PCV10 | 0.45 (0.35–0.58) | 0.84 (0.68–1.04) | 1.64 (1.27–2.11) | 1.30 (1.06–1.61) | 3.53 (2.51–4.98) | 1.57 (1.31–1.87) | 0.66 (0.47–0.92) |
| PCV13 | 0.62 (0.45–0.85) | 0.68 (0.55–0.85) | 1.51 (1.13–2.01) | 1.06 (0.85–1.31) | 2.36 (1.79–3.11) | 1.58 (1.26–1.98) | 0.69 (0.51–0.94) | |
| 14 | PCV10 | 2.37 (1.88–2.99) | 3.07 (2.55–3.70) | 4.92 (3.63–6.67) | 5.69 (4.21–7.68) | 2.00 (1.35–2.97) | 1.83 (1.40–2.38) | 1.08 (0.70–1.67) |
| PCV13 | 2.71 (2.05–3.58) | 2.08 (1.66–2.62) | 6.09 (4.49–8.24) | 4.33 (3.36–5.58) | 2.13 (1.53–2.97) | 2.12 (1.67–2.69) | 0.85 (0.59–1.22) | |
| 18C | PCV10 | 0.44 (0.35–0.56) | 0.60 (0.50–0.73) | 1.51 (1.15–1.98) | 1.07 (0.85–1.35) | 3.31 (2.33–4.70) | 1.77 (1.43–2.19) | 0.67 (0.47–0.95) |
| PCV13 | 0.55 (0.42–0.71) | 0.66 (0.52–0.84) | 1.40 (1.03–1.91) | 1.05 (0.83–1.33) | 2.49 (1.84–3.35) | 1.60 (1.31–1.95) | 0.70 (0.50–0.96) | |
| 19F | PCV10 | 1.51 (1.19–1.91) | 2.32 (1.87–2.87) | 5.14 (3.64–7.26) | 4.21 (3.28–5.39) | 3.31 (2.42–4.52) | 1.83 (1.46–2.30) | 0.64 (0.43–0.94) |
| PCV13 | 2.40 (1.78–3.21) | 2.27 (1.72–2.99) | 6.10 (4.25–8.76) | 4.69 (3.50–6.29) | 2.67 (2.00–3.55) | 2.12 (1.70–2.64) | 0.79 (0.56–1.12) | |
| 23F | PCV10 | 0.36 (0.28–0.47) | 0.52 (0.42–0.64) | 0.89 (0.69–1.15) | 0.84 (0.68–1.05) | 2.39 (1.72–3.32) | 1.62 (1.29–2.03) | 0.86 (0.62–1.21) |
| PCV13 | 0.52 (0.40–0.69) | 0.45 (0.34–0.60) | 1.31 (0.94–1.84) | 0.61 (0.46–0.82) | 2.54 (1.90–3.41) | 1.38 (1.11–1.71) | 0.52 (0.37–0.73) | |
| PCV13 serotypes | ||||||||
| 3 | PCV10 | 0.24 (0.20–0.30) | 0.26 (0.21–0.32) | 0.46 (0.36–0.59) | 0.41 (0.32–0.53) | 1.98 (1.64–2.39) | 1.60 (1.34–1.91) | 0.82 (0.64–1.06) |
| PCV13 | 0.24 (0.18–0.31) | 0.26 (0.21–0.32) | 0.41 (0.31–0.53) | 0.40 (0.33–0.49) | 1.71 (1.42–2.06) | 1.55 (1.32–1.82) | 0.94 (0.75–1.17) | |
| 6A^ | PCV10 | 0.38 (0.28–0.50) | 0.41 (0.33–0.51) | 0.55 (0.40–0.77) | 0.61 (0.47–0.81) | 1.49 (1.27–1.76) | 1.48 (1.19–1.84) | 1.00 (0.76–1.31) |
| PCV13 | 0.61 (0.44–0.85) | 0.42 (0.33–0.55) | 0.90 (0.65–1.25) | 0.51 (0.39–0.66) | 1.47 (1.19–1.83) | 1.23 (1.04–1.45) | 0.77 (0.59–1.00) | |
| 19A | PCV10 | 1.11 (0.88–1.40) | 1.36 (1.09–1.69) | 2.10 (1.50–2.93) | 2.00 (1.51–2.66) | 1.84 (1.39–2.44) | 1.44 (1.16–1.78) | 0.81 (0.57–1.16) |
| PCV13 | 2.20 (1.60–3.01) | 1.59 (1.16–2.18) | 4.27 (3.05–5.99) | 2.48 (1.80–3.44) | 1.94 (1.41–2.66) | 1.60 (1.30–1.96) | 0.75 (0.53–1.06) | |
| Non-PCV serotype | ||||||||
| 2 | PCV10 | 0.74 (0.57–0.95) | 1.00 (0.81–1.23) | 1.75 (1.43–2.14) | 1.54 (1.22–1.95) | 2.40 (1.89–3.05) | 1.56 (1.27–1.91) | 0.76 (0.58–1.00) |
| PCV13 | 0.62 (0.48–0.79) | 0.90 (0.69–1.16) | 1.84 (1.43–2.36) | 1.31 (1.01–1.70) | 3.04 (2.32–3.97) | 1.44 (1.21–1.71) | 0.55 (0.41–0.73) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van den Biggelaar, A.H.J.; Pomat, W.S.; Masiria, G.; Wana, S.; Nivio, B.; Francis, J.; Ford, R.; Passey, M.; Kirkham, L.-A.; Jacoby, P.; et al. Immunogenicity and Immune Memory after a Pneumococcal Polysaccharide Vaccine Booster in a High-Risk Population Primed with 10-Valent or 13-Valent Pneumococcal Conjugate Vaccine: A Randomized Controlled Trial in Papua New Guinean Children. Vaccines 2019, 7, 17. https://doi.org/10.3390/vaccines7010017
van den Biggelaar AHJ, Pomat WS, Masiria G, Wana S, Nivio B, Francis J, Ford R, Passey M, Kirkham L-A, Jacoby P, et al. Immunogenicity and Immune Memory after a Pneumococcal Polysaccharide Vaccine Booster in a High-Risk Population Primed with 10-Valent or 13-Valent Pneumococcal Conjugate Vaccine: A Randomized Controlled Trial in Papua New Guinean Children. Vaccines. 2019; 7(1):17. https://doi.org/10.3390/vaccines7010017
Chicago/Turabian Stylevan den Biggelaar, Anita H. J., William S. Pomat, Geraldine Masiria, Sandra Wana, Birunu Nivio, Jacinta Francis, Rebecca Ford, Megan Passey, Lea-Ann Kirkham, Peter Jacoby, and et al. 2019. "Immunogenicity and Immune Memory after a Pneumococcal Polysaccharide Vaccine Booster in a High-Risk Population Primed with 10-Valent or 13-Valent Pneumococcal Conjugate Vaccine: A Randomized Controlled Trial in Papua New Guinean Children" Vaccines 7, no. 1: 17. https://doi.org/10.3390/vaccines7010017