

School Teachers’ Perceptions of Adolescent Human Papillomavirus (HPV) Vaccination: A Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Selection Process and Data Synthesis
2.4. Quality Assessment
3. Results
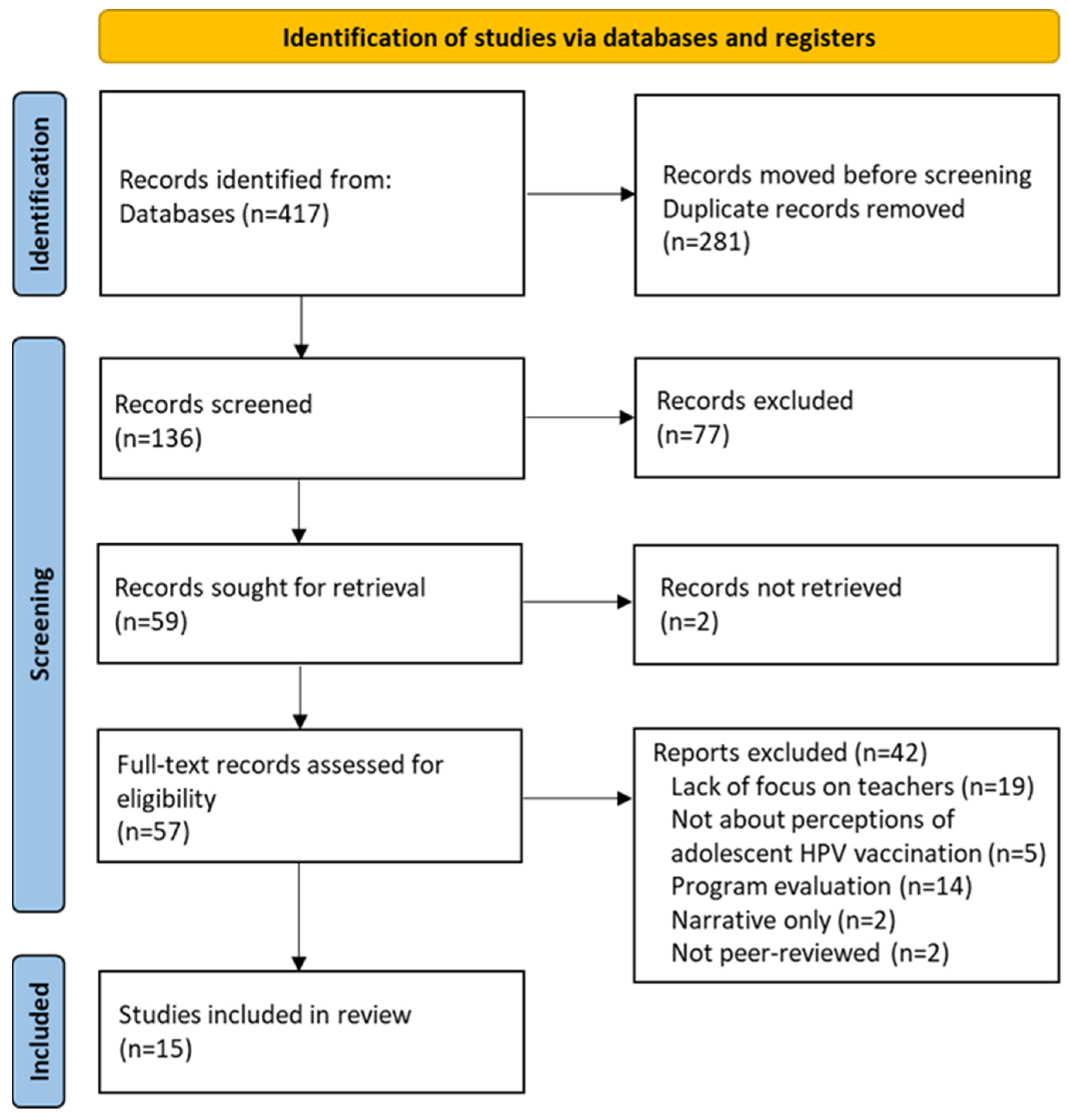
3.1. Search Results
3.2. Study Characteristics
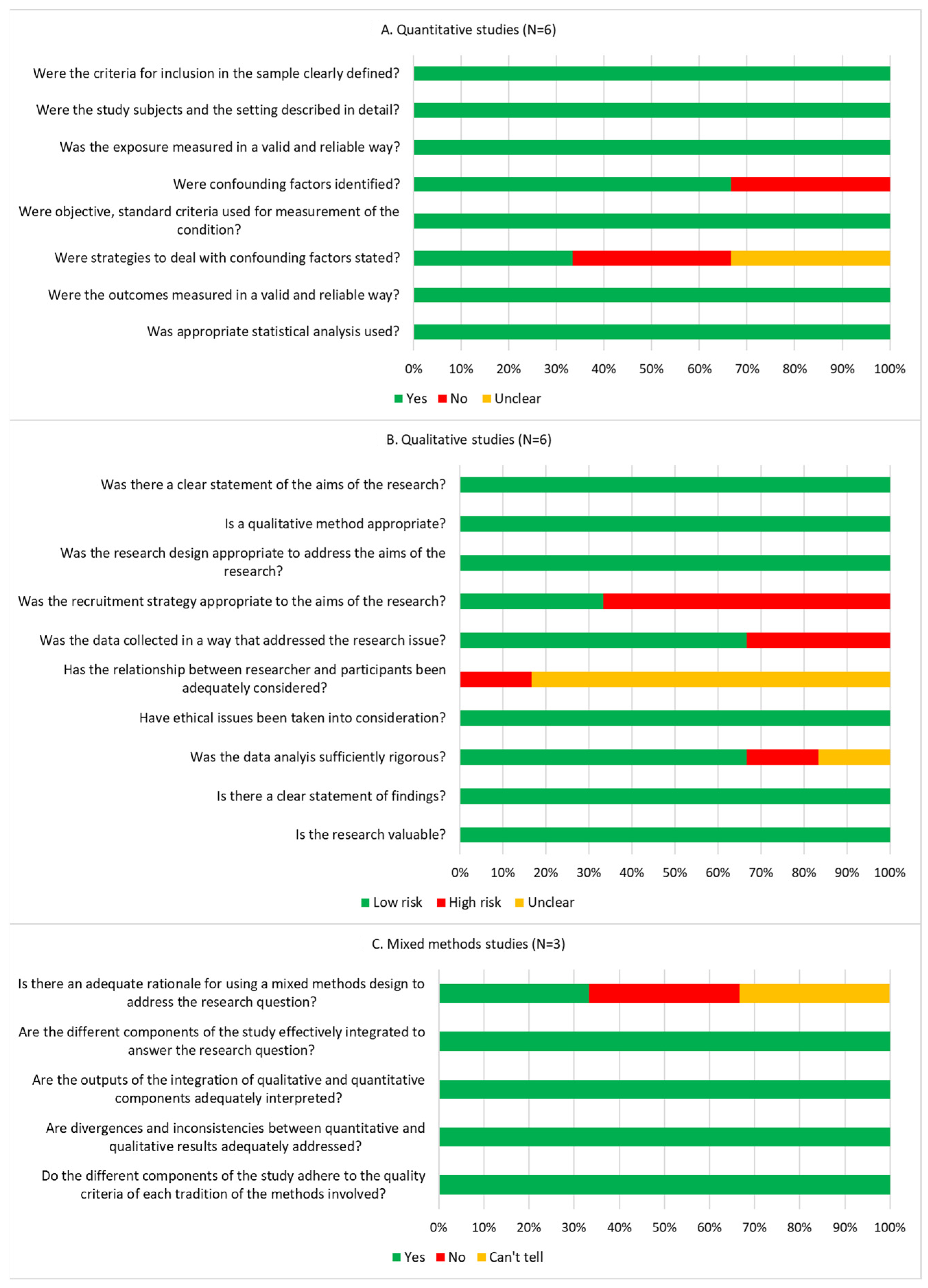
3.3. Quality Assessment of the Included Studies
3.4. Synthesis of Evidence
3.4.1. Lack of Knowledge
3.4.2. Negative Attitudes towards HPV Vaccines
3.4.3. Fear of Parents’ HPV Vaccine Disapproval
3.4.4. Drivers of Teachers’ Acceptance of Adolescent HPV Vaccination
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shapiro, G.K. HPV vaccination: An underused strategy for the prevention of cancer. Curr. Oncol. 2022, 29, 3780–3792. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Human Papillomavirus (HPV) Vaccination Coverage. 2022. Available online: https://immunizationdata.who.int/pages/coverage/hpv.html (accessed on 13 October 2023).
- Hendry, M.; Lewis, R.; Clements, A.; Damery, S.; Wilkinson, C. “HPV? Never heard of it!”: A systematic review of girls’ and parents’ information needs, views and preferences about human papillomavirus vaccination. Vaccine 2013, 31, 5152–5167. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, R.R.; Smith, A.; Coyne-Beasley, T. A systematic literature review to examine the potential for social media to impact HPV vaccine uptake and awareness, knowledge, and attitudes about HPV and HPV vaccination. Hum. Vaccines Immunother. 2019, 15, 1465–1475. [Google Scholar] [CrossRef] [PubMed]
- Garbutt, J.; Wang, R.; Graham, S.; McKay, V.; Haire-Joshu, D.; Barker, A.; Liu, L. Provider and Practice Factors Associated With On-Time HPV Vaccination in Primary Care. Acad. Pediatr. 2023, 23, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Daley, E.M.; Vamos, C.A.; Thompson, E.L.; Zimet, G.D.; Rosberger, Z.; Merrell, L.; Kline, N.S. The feminization of HPV: How science, politics, economics and gender norms shaped US HPV vaccine implementation. Papillomavirus Res. 2017, 3, 142–148. [Google Scholar] [CrossRef] [PubMed]
- White, L.S.; Maulucci, E.; Kornides, M.; Aryal, S.; Alix, C.; Sneider, D.; Gagnon, J.; Winfield, E.C.; Fontenot, H.B. HPV Vaccination Rates of 7th Grade Students After a Strong Recommending Statement from the School Nurse. J. Sch. Nurs. 2022, 10598405221118824. [Google Scholar] [CrossRef] [PubMed]
- Duffy, B.; Fotinatos, N.; Smith, A.; Burke, J. Puberty, health and sexual education in Australian regional primary schools: Year 5 and 6 teacher perceptions. Sex Educ. 2013, 13, 186–203. [Google Scholar] [CrossRef]
- Galemore, C.A.; Marion, S.; Moran Fossile, K.; O’Toole, S.; Ragan, K.; Robertson, B. Leading during a pandemic: A school nurse administrator roundtable. NASN Sch. Nurse 2022, 37, 155–164. [Google Scholar] [CrossRef]
- Galemore, C.; Alattar, H.Y.; Fatica, K.; Huey, A.; Schulz, K. Millennial school nurses: A roundtable discussion. NASN Sch. Nurse 2019, 34, 329–334. [Google Scholar] [CrossRef]
- Szefler, S.J.; Fitzgerald, D.A.; Adachi, Y.; Doull, I.J.; Fischer, G.B.; Fletcher, M.; Hong, J.; García-Marcos, L.; Pedersen, S.; Østrem, A.; et al. A worldwide charter for all children with asthma. Pediatr. Pulmonol. 2020, 55, 1282–1292. [Google Scholar] [CrossRef]
- Gottvall, M.; Tydén, T.; Larsson, M.; Stenhammar, C.; Höglund, A.T. Challenges and opportunities of a new HPV immunization program: Perceptions among Swedish school nurses. Vaccine 2011, 29, 4576–4583. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.L.; Goodson, P.; Thompson, B.; Wilson, K.L. School nurses’ knowledge, attitudes, perceptions of role as opinion leader, and professional practice regarding human papillomavirus vaccine for youth. J. Sch. Health 2015, 85, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.L.; Ashwood, D.; Richardson, G.B. School nurses’ professional practice in the HPV vaccine decision-making process. J. Sch. Nurs. 2016, 32, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.L.; DiClemente, R.; Shepard, A.L.; Wilson, K.L.; Fehr, S.K. Factors associated with school nurses’ HPV vaccine attitudes for school-aged youth. Psychol. Health Med. 2017, 22, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Grandahl, M.; Larsson, M.; Tydén, T.; Stenhammar, C. School nurses’ attitudes towards and experiences of the Swedish school-based HPV vaccination programme–A repeated cross sectional study. PLoS ONE 2017, 12, e0175883. [Google Scholar] [CrossRef] [PubMed]
- McNally, K.; Roess, A.; Weinstein, A.; Lindley, L.; Wallin, R. School Nurses’ Experiences and Roles in Promoting and Administering the HPV Vaccine: A Systematic Review Using the Socioecological Framework. J. Sch. Nurs. 2023, 40, 43–57. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- The Joanna Briggs Institute. JBI Critical Appraisal Checklist for Analytical cross Sectional Studies; The Joanna Briggs Institute: Adelaide, Australia, 2016. [Google Scholar]
- Long, H.A.; French, D.P.; Brooks, J.M. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res. Methods Med. Health Sci. 2020, 1, 31–42. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Choi, K.B.; Mo, H.S.; Kim, J.S. Factors associated with the intention to recommend human papillomavirus vaccination among K orean school health teachers. J. Spec. Pediatr. Nurs. 2013, 18, 297–310. [Google Scholar] [CrossRef]
- Spratt, J.; Shucksmith, J.; Philip, K.; McNaughton, R. Active agents of health promotion? The school’s role in supporting the HPV vaccination programme. Sex Educ. 2013, 13, 82–95. [Google Scholar] [CrossRef]
- Rosberger, Z.; Krawczyk, A.; Stephenson, E.; Lau, S. HPV vaccine education: Enhancing knowledge and attitudes of community counselors and educators. J. Cancer Educ. 2014, 29, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Kamada, M.; Inui, H.; Kagawa, T.; Mineda, A.; Tamura, T.; Fujioka, T.; Motoki, T.; Hirai, H.; Ishii, E.; Irahara, M. What information can change the attitude of teachers toward the human papillomavirus vaccine? J. Obstet. Gynaecol. Res. 2018, 44, 778–787. [Google Scholar] [CrossRef] [PubMed]
- Ishiwada, N.; Suzuki, C.; Hasebe, S.; Tsuchiya, A.; Takeuchi, N.; Hishiki, H.; Sato, Y.; Sugita, K. The effects of health education on health science teachers’ intention to recommend adolescent HPV vaccine for female students in Japan. Hum. Vaccines Immunother. 2020, 16, 2752–2757. [Google Scholar] [CrossRef] [PubMed]
- Bocquier, A.; Branchereau, M.; Gauchet, A.; Bonnay, S.; Simon, M.; Ecollan, M.; Chevreul, K.; Mueller, J.E.; Gagneux-Brunon, A.; Thilly, N.; et al. Promoting HPV vaccination at school: A mixed methods study exploring knowledge, beliefs and attitudes of French school staff. BMC Public Health 2023, 23, 486. [Google Scholar] [CrossRef] [PubMed]
- Ailloud, J.; Branchereau, M.; Fall, E.; Juneau, C.; Partouche, H.; Bonnay, S.; Oudin-Doglioni, D.; Michel, M.; Gagneux-Brunon, A.; Bruel, S.; et al. How can we improve the acceptability of vaccination against Human Papillomavirus (HPV) in France? An original qualitative study with focus groups comprising parents and school staff, interviewed separately. Vaccine 2023, 41, 4594–4608. [Google Scholar] [CrossRef] [PubMed]
- Siu JY-m Lee, A.; Chan, P.K. Schoolteachers’ experiences of implementing school-based vaccination programs against human papillomavirus in a Chinese community: A qualitative study. BMC Public Health 2019, 19, 1514. [Google Scholar]
- Clave Llavall, A.; de Wildt, G.; Meza, G.; Tattsbridge, J.; Jones, L. Nurses’ and teachers’ perceived barriers and facilitators to the uptake of the Human Papilloma Virus (HPV) vaccination program in Iquitos, Peru: A qualitative study. PLoS ONE 2021, 16, e0255218. [Google Scholar] [CrossRef] [PubMed]
- Ajah, L.; Iyoke, C.; Ezeonu, P.; Ugwu, G.; Onoh, R.; Ibo, C. Association between knowledge of cervical cancer/screening and attitude of teachers to immunization of adolescent girls with human papilloma virus vaccine in Abakaliki, Nigeria. Am. J. Cancer Prev. 2015, 3, 8–12. [Google Scholar]
- Masika, M.M.; Ogembo, J.G.; Chabeda, S.V.; Wamai, R.G.; Mugo, N. Knowledge on HPV vaccine and cervical cancer facilitates vaccine acceptability among school teachers in Kitui County, Kenya. PLoS ONE 2015, 10, e0135563. [Google Scholar] [CrossRef]
- Vermandere, H.; Naanyu, V.; Degomme, O.; Michielsen, K. Implementation of an HPV vaccination program in Eldoret, Kenya: Results from a qualitative assessment by key stakeholders. BMC Public Health 2015, 15, 875. [Google Scholar] [CrossRef] [PubMed]
- Keehn, D.C.; Chamberlain, R.M.; Tibbits, M.; Kahesa, C.; Msami, K.; Soliman, A.S. Using key informants to evaluate barriers to education and acceptability of the HPV vaccine in Tanzania: Implications for cancer education. J. Cancer Educ. 2021, 36, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Enebe, J.T.; Enebe, N.O.; Agunwa, C.C.; Nduagubam, O.C.; Okafor, I.I.; Aniwada, E.C.; Aguwa, E.N. Awareness, acceptability and uptake of cervical cancer vaccination services among female secondary school teachers in enugu, nigeria: A cross-sectional study. Pan Afr. Med. J. 2021, 39, 62. [Google Scholar] [CrossRef] [PubMed]
- Warsi, S.K.; Nielsen, S.M.; Franklin, B.A.; Abdullaev, S.; Ruzmetova, D.; Raimjanov, R.; Nagiyeva, K.; Safaeva, K. Formative Research on HPV Vaccine Acceptance among Health Workers, Teachers, Parents, and Social Influencers in Uzbekistan. Vaccines 2023, 11, 754. [Google Scholar] [CrossRef] [PubMed]
- Racey, C.S.; Donken, R.; Fox, E.; Porter, I.; Bettinger, J.A.; Mark, J.; Bonifacio, L.; Dawar, M.; Gagel, M.; Kling, R.; et al. Characterization of vaccine confidence among teachers in British Columbia, Canada: A population-based survey. PLoS ONE 2023, 18, e0288107. [Google Scholar] [CrossRef] [PubMed]
- Clay, D.L.; Cortina, S.; Harper, D.C.; Cocco, K.M.; Drotar, D. Schoolteachers’ experiences with childhood chronic illness. Child. Health Care 2004, 33, 227–239. [Google Scholar] [CrossRef]
- Reiter, P.L.; Stubbs, B.; Panozzo, C.A.; Whitesell, D.; Brewer, N.T. HPV and HPV vaccine education intervention: Effects on parents, healthcare staff, and school staff. Cancer Epidemiol. Biomark. Prev. 2011, 20, 2354–2361. [Google Scholar] [CrossRef] [PubMed]
- Schmeler, K.M.; Sturgis, E.M. Expanding the benefits of HPV vaccination to boys and men. Lancet 2016, 387, 1798–1799. [Google Scholar] [CrossRef]
- Rhodes, D.; Visker, J.D.; Cox, C.; Sas, A.; Banez, J.C. Effects of an online educational module on school nurses’ knowledge of HPV vaccination. J. Contin. Educ. Nurs. 2017, 48, 431–436. [Google Scholar] [CrossRef]
- Adeyanju, G.C.; Sprengholz, P.; Betsch, C.; Essoh, T.-A. Caregivers’ willingness to vaccinate their children against childhood diseases and human papillomavirus: A cross-sectional study on vaccine hesitancy in Malawi. Vaccines 2021, 9, 1231. [Google Scholar] [CrossRef]
- Knopf, J.A.; Finnie, R.K.; Peng, Y.; Hahn, R.A.; Truman, B.I.; Vernon-Smiley, M.; Johnson, V.C.; Johnson, R.L.; Fielding, J.E.; Muntaner, C.; et al. School-based health centers to advance health equity: A community guide systematic review. Am. J. Prev. Med. 2016, 51, 114–126. [Google Scholar] [CrossRef]
- Davies, C.; Marshall, H.S.; Zimet, G.; McCaffery, K.; Brotherton, J.M.; Kang, M.; Garland, S.; Kaldor, J.; McGeechan, K.; Skinner, S.R.; et al. Effect of a School-Based Educational Intervention About the Human Papillomavirus Vaccine on Psychosocial Outcomes Among Adolescents: Analysis of Secondary Outcomes of a Cluster Randomized Trial. JAMA Netw. Open 2021, 4, e2129057. [Google Scholar] [CrossRef] [PubMed]
- Batista Ferrer, H.; Trotter, C.L.; Hickman, M.; Audrey, S. Barriers and facilitators to uptake of the school-based HPV vaccination programme in an ethnically diverse group of young women. J. Public Health 2016, 38, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; Clément, P.; Bettinger, J.A.; Comeau, J.L.; Deeks, S.; Guay, M.; MacDonald, S.; MacDonald, N.E.; Mijovic, H.; et al. Challenges and opportunities of school-based HPV vaccination in Canada. Hum. Vaccines Immunother. 2019, 15, 1650–1655. [Google Scholar] [CrossRef] [PubMed]
- Audrey, S.; Ferrer, H.B.; Ferrie, J.; Evans, K.; Bell, M.; Yates, J.; Roderick, M.; MacLeod, J.; Hickman, M. Impact and acceptability of self-consent procedures for the school-based human papillomavirus vaccine: A mixed-methods study protocol. BMJ Open 2018, 8, e021321. [Google Scholar] [CrossRef] [PubMed]
- Leenders, H.; De Jong, J.; Monfrance, M.; Haelermans, C. Building strong parent–teacher relationships in primary education: The challenge of two-way communication. Camb. J. Educ. 2019, 49, 519–533. [Google Scholar] [CrossRef]
- Ahmed, D.; VanderEnde, K.; Harvey, P.; Bhatnagar, P.; Kaur, N.; Roy, S.; Singh, N.; Denzongpa, P.; Haldar, P.; Loharikar, A. Human papillomavirus (HPV) vaccine introduction in Sikkim state: Best practices from the first statewide multiple-age cohort HPV vaccine introduction in India–2018–2019. Vaccine 2022, 40, A17–A25. [Google Scholar] [CrossRef]
- Brewer, N.T.; Mitchell, C.G.; Dailey, S.A.; Hora, L.; Fisher-Borne, M.; Tichy, K.; McCoy, T. HPV vaccine communication training in healthcare systems: Evaluating a train-the-trainer model. Vaccine 2021, 39, 3731–3736. [Google Scholar] [CrossRef]
- Frayon, S. New Caledonian biology teachers’ opinions about vaccination: Preliminary findings. Health Educ. J. 2020, 79, 594–606. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Characteristics | n (%) | |
|---|---|---|
| Region | Asia | 5 (33.3%) |
| North America | 1 (6.7%) | |
| South America | 1 (6.7%) | |
| Africa | 5 (33.3%) | |
| Europe | 3 (20.0%) | |
| Region income level | High | 7 (46.7%) |
| Upper-middle | 2 (13.3%) | |
| Lower-middle | 6 (40.0%) | |
| School level | Elementary/primary school | 5 (33.3%) |
| Secondary (middle/high) school | 6 (40.0%) | |
| Both primary and secondary school | 2 (13.3%) | |
| Not specified | 2 (13.3%) | |
| Teacher type | Health/Health Sciences | 2 (13.3%) |
| Sciences/Life Sciences | 1 (6.7%) | |
| Arts and Math | 1 (6.7%) | |
| Not specified | 11 (73.3%) | |
| Study design | Quantitative | 6 (40.0%) |
| Qualitative | 6 (40.0%) | |
| Mixed methods | 3 (20.0%) | |
| Primary outcome measure | Acceptance of HPV vaccination | 7 (46.7%) |
| Willingness to recommend HPV vaccination | 5 (33.3%) | |
| Both acceptance of and willingness to recommend HPV vaccination | 3 (20.0%) | |
| Study | Aim | Country | Study Design and Size | School Level | Gender-Neutral HPV Vaccination ǂ | Key Findings |
|---|---|---|---|---|---|---|
| High income region † | ||||||
| Choi et al., 2013 [22] | To identify factors associated with Korean health teachers’ intention to recommend the HPV vaccine | Republic of Korea | Quant N = 119 | Elementary, Middle, High | No, female-only | Less than 12% of teachers reported having recommended HPV vaccination to students and parents. The mean score of the intention to recommend the HPV vaccine was 5.29 out of 10. Teachers had the highest intention to recommend the vaccine to high school students or their parents (6.12), followed by middle school students or their parents (5.32) and elementary school students or their parents (4.45). Teachers did not consider themselves responsible for promoting the vaccine due to having a heavy workload. * |
| Spratt et al., 2013 [23] | To examine secondary school teachers’ views of their roles as partners in a school-based HPV vaccination program | Scotland | Qual N = 32 | Secondary | Yes | Teachers were concerned about the impact of vaccination on students’ current understanding of sex and sexuality. They showed unease that vaccination could potentially compromise childhood innocence. Some teachers feared negative publicity or parental complaints if they were seen to promote adolescent HPV vaccination. * |
| Rosberger et al., 2014 [24] | To explore the effect of a workshop intervention designed to provide the most up-to-date information among educators and counselors about their knowledge, attitudes, and beliefs about HPV and the HPV vaccine | Canada | Quant N = 37 | Not stated | Yes | Most teachers knew that HPV is sexually transmitted (86.5%) and that the HPV vaccine prevents cervical cancer (83.8%). Teachers reported low levels of confidence (M = 2.8/7) in discussing HPV vaccination with parents. Willingness to recommend the HPV vaccine was not significantly associated with knowledge nor confidence in providing accurate HPV vaccine information. Common types of additional information requested were regarding HPV vaccination in males and the long-term side effects of the vaccine. |
| Kamada et al., 2018 [25] | To determine the ways to increase teachers’ willingness to encourage the use of the HPV vaccine | Japan | Quant N = 247 | Not stated | No, female-only | While 63% knew that the HPV vaccine prevents cervical cancer, 36% knew that HPV causes cervical cancer. Seventy-seven percent of the teachers feared vaccine side effects and 69% would not recommend the vaccine to their daughters and students. The information they most wanted was a proof of the HPV vaccine’s preventive effect. |
| Ishiwada et al., 2020 [26] | To identify the current status, issues, and barriers regarding HPV vaccination among health science teachers | Japan | Quant N = 37 | High | No, female-only | Teachers were initially uncertain (51.3%) and fearful (30.8%) about HPV vaccination. Teachers were significantly more inclined to recommend the HPV vaccine to students (p < 0.05) once they were more informed about HPV and became less fearful of HPV vaccine side effects. |
| Bocquier et al., 2023 [27] | To identify barriers, facilitators, and needs of the different school professionals involved in the implementation of HPV vaccination promotion interventions in French middle schools | France | Mixed N = 315 | Middle (94% public schools, 5% private schools) | Yes | Eighty percent of teachers knew that HPV is sexually transmitted, but less than half knew that HPV can cause genital warts, and oral and cervical cancers. Seventy-six percent knew that the HPV vaccine protects against HPV-related cancers, and 56% knew that the vaccine is recommended for boys. Teachers had positive attitudes towards the benefits of HPV vaccination (mean score > 5 on a scale of 1–7). Teachers had mixed views about providing HPV education at school; focus groups agreed that offering HPV vaccination does not fall within the school’s role. Perceived barriers included teachers’ additional workload and fear of parents’ negative reactions. |
| Ailloud et al., 2023 [28] | To evaluate knowledge, perceptions, beliefs, facilitators, and barriers to HPV vaccination among school staff from middle schools | France | Qual N = 14 | Middle | Yes | Teachers lacked HPV knowledge and saw HPV as a women’s issue. Teachers considered that children are too young to receive a sexually-related vaccine. HPV discussion in school was hindered because of sexuality being a taboo and a difficult topic for school staff. Some teachers believed that teachers are a legitimate means to conduct awareness sessions on HPV but felt burdened to do so at the same time. Teachers mentioned that the role of schools could be more important in transmitting information on HPV to students and parents. |
| Upper-middle income region † | ||||||
| Siu et al., 2019 [29] | To investigate how school teachers in primary and secondary schools perceive HPV and HPV vaccines | Hong Kong | Qual N = 35 | Primary, secondary | No, female-only | Teachers believed that cervical cancer protection and HPV vaccination were difficult concepts for their students who were too young to be considered vulnerable. Schools would oppose HPV vaccine promotion, and it was not prioritized compared to other health education topics (e.g., influenza). Teachers worried that HPV vaccine promotion could convey a negative message on sex attitudes. Parents’ attitudes affected teachers’ motivation. Without parental support, teachers could not justify school-based HPV vaccine promotion. |
| Llavall et al., 2021 [30] | To understand teachers’ perceived barriers and facilitators to implementing HPV vaccination program, HPV knowledge and attitudes, and recommendations on strategies to increase vaccination rates | Peru | Qual N = 10 | Primary | No, female-only | While teachers pointed out a necessity for their students to be protected against cervical cancer, there was distrust towards the HPV vaccine and fear generated in terms of harming adolescents’ fertility. Teachers thought parents were not informed about HPV and the vaccine. Teachers also reported that parents rejected the vaccine because it would lead to sexual initiation among children. Teachers reported perceived parents’ fear of serious side effects such as infertility. |
| Lower-middle income region † | ||||||
| Ajah et al., 2015 [31] | To describe the knowledge and attitude of secondary school teachers towards HPV vaccination; to explore the feasibility of enlisting teachers towards promoting vaccine uptake | Nigeria | Quant N = 412 | Middle, High | No, female-only | About 80% of teachers who were aware of cervical cancer knew that HPV caused cervical cancer. Among these, less than 40% knew the availability and benefits of the HPV vaccine, and 70% were willing to accept and recommend the vaccine to their daughters and students. Knowledge was significantly associated with HPV vaccine acceptability. |
| Masika et al., 2015 [32] | To assess primary school teachers’ knowledge and acceptability of HPV vaccine | Kenya | Mixed N = 339 | Primary (34 public schools, 3 private schools) | No, female-only | Teachers had low to moderate levels of knowledge about HPV and the HPV vaccine (mean score of 48%), especially men’s susceptibility to HPV infection (mean score of 8%). However, vaccine acceptability was high (89%). One-third of all teachers indicated insufficient vaccine information and fear of vaccine side effects as the main barriers. Nearly all respondents (98%) expressed interest to know more about the HPV vaccine, and 93% supported school-based vaccine delivery. |
| Vermandere et al., 2015 [33] | To verify teachers’ awareness of and support for HPV vaccination programs; to assess barriers in HPV vaccine promotion | Kenya | Qual N = 43 | Not stated | No, female-only | When asked about causes of cervical cancer, HPV was rarely mentioned as a primary cause. Teachers showed distrust towards the HPV vaccine. While protecting a girl’s fertility was a driver for HPV vaccine acceptance, the same vaccine generated fear in terms of harming the girl’s fertility. At least three teachers described perceived parental fear that vaccination would enhance sexual activity among children. Some were keen to provide information and promote the vaccine given their daily contact with the children. * |
| Keehn et al., 2021 [34] | To assess primary school teachers as key informants when assessing barriers to parent acceptance of the HPV vaccine | Tanzania | Mixed N = 155 | Primary | No, female-only | While 95% had heard of cervical cancer, only 37% and 29% of participants had heard of HPV and the HPV vaccine, respectively. Teachers from all seven schools included in this study mentioned parental lack of HPV knolwedge as the main barrier but were willing to promote the vaccine to parents. Common questions from focus groups included: inquiries about vaccine side effects and why boys are not being vaccinated at this time. |
| Enebe et al., 2021 [35] | To determine the level of awareness, acceptability and uptake of HPV vaccine among female secondary school teachers | Nigeria | Quant N = 377 | Secondary | No, female-only | Less than half (41.9%) of the teachers had high knowledge of cervical cancer, and 48.3% knew that HPV vaccination can prevent cervical cancer. Only 14.6% indicated having taught their students about cervical cancer or HPV vaccine. Acceptability was high among teachers who were aware of the vaccine, as the majority of teachers (93.6%) would recommend the vaccine to their children and students if the vaccine were given for free by the government. |
| Warsi et al., 2023 [36] | To understand barriers and drivers to general and HPV vaccination among key target groups (teachers) in Uzbekistan | Uzbekistan | Qual N = 32 | Elementary | No, female-only | Teachers’ vaccine hesitancy stemmed from knowledge gaps on vaccine safety. Few participants were aware of HPV, its relation to cervical cancer, and the HPV vaccine.* The primary anxieties of the teachers were any potential negative effects of the vaccine on students’ future fertility. Teachers highlighted the need for clear and credible information on the safety of the HPV vaccine to be confident in their support for the vaccine. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.; Gabay, E.K.; Cuccaro, P.M. School Teachers’ Perceptions of Adolescent Human Papillomavirus (HPV) Vaccination: A Systematic Review. Vaccines 2024, 12, 361. https://doi.org/10.3390/vaccines12040361
Choi J, Gabay EK, Cuccaro PM. School Teachers’ Perceptions of Adolescent Human Papillomavirus (HPV) Vaccination: A Systematic Review. Vaccines. 2024; 12(4):361. https://doi.org/10.3390/vaccines12040361
Chicago/Turabian StyleChoi, Jihye, Efrat K. Gabay, and Paula M. Cuccaro. 2024. "School Teachers’ Perceptions of Adolescent Human Papillomavirus (HPV) Vaccination: A Systematic Review" Vaccines 12, no. 4: 361. https://doi.org/10.3390/vaccines12040361