
COVID-19 Vaccination and Predictive Factors in Immigrants to Europe: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Criteria of Selection
2.2. Quality Assessment
2.3. Data Analysis
3. Results
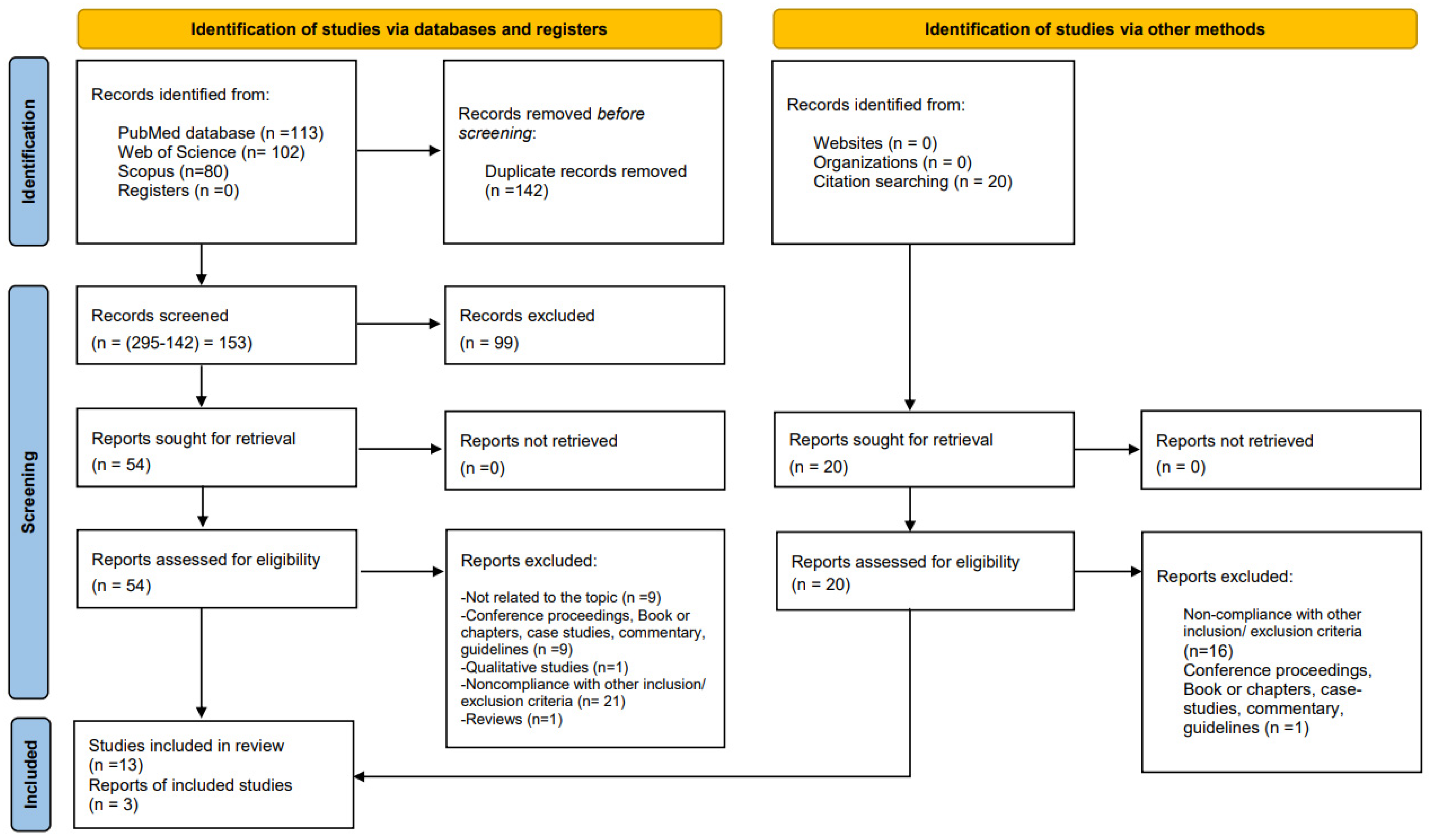
3.1. Screening and Selection Process
3.2. Overview of the Included Studies
3.3. Quality Assessment
3.4. Meta-Analyses
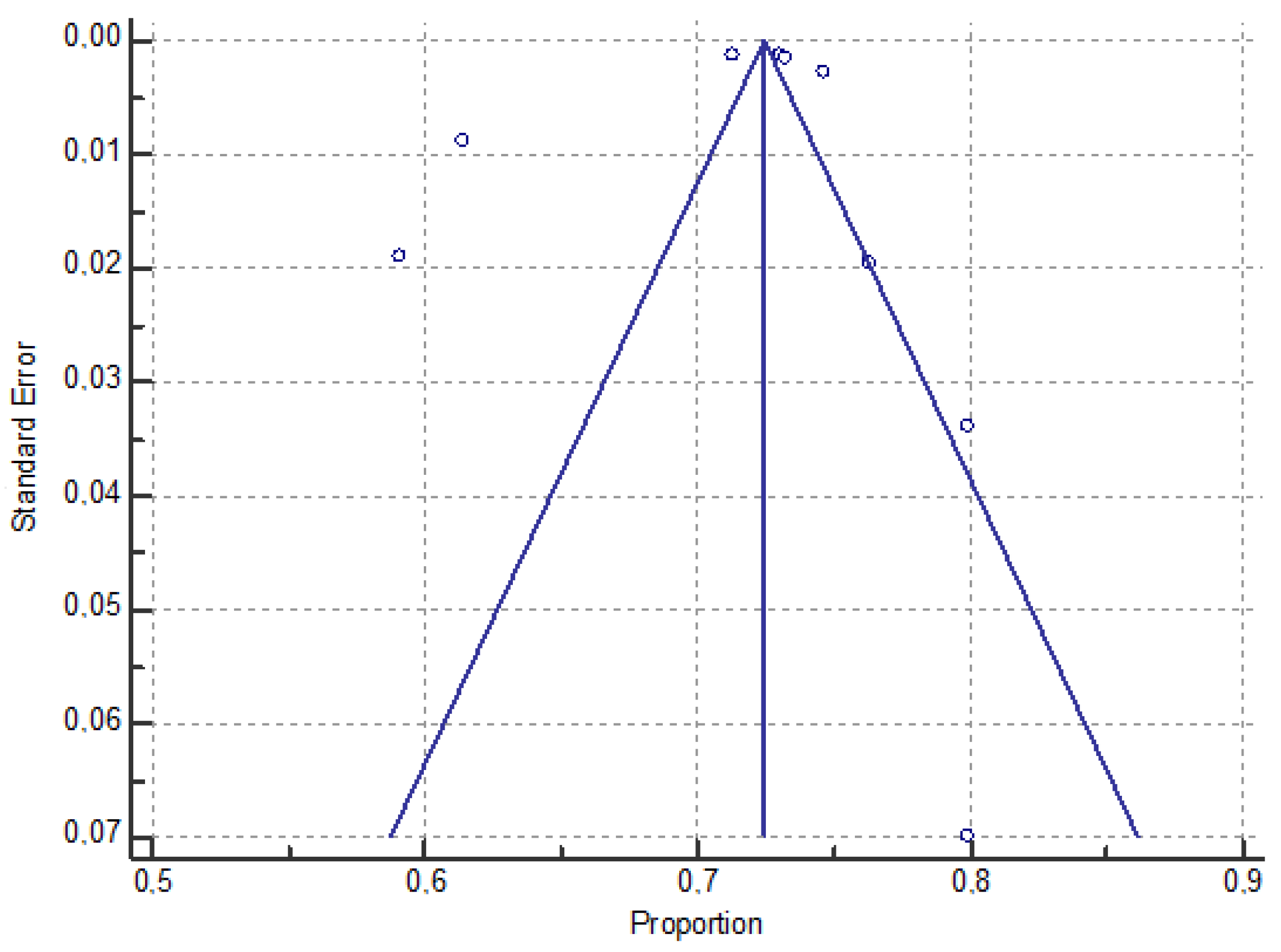
3.4.1. The Pooled Prevalence of Vaccination among Immigrant Groups
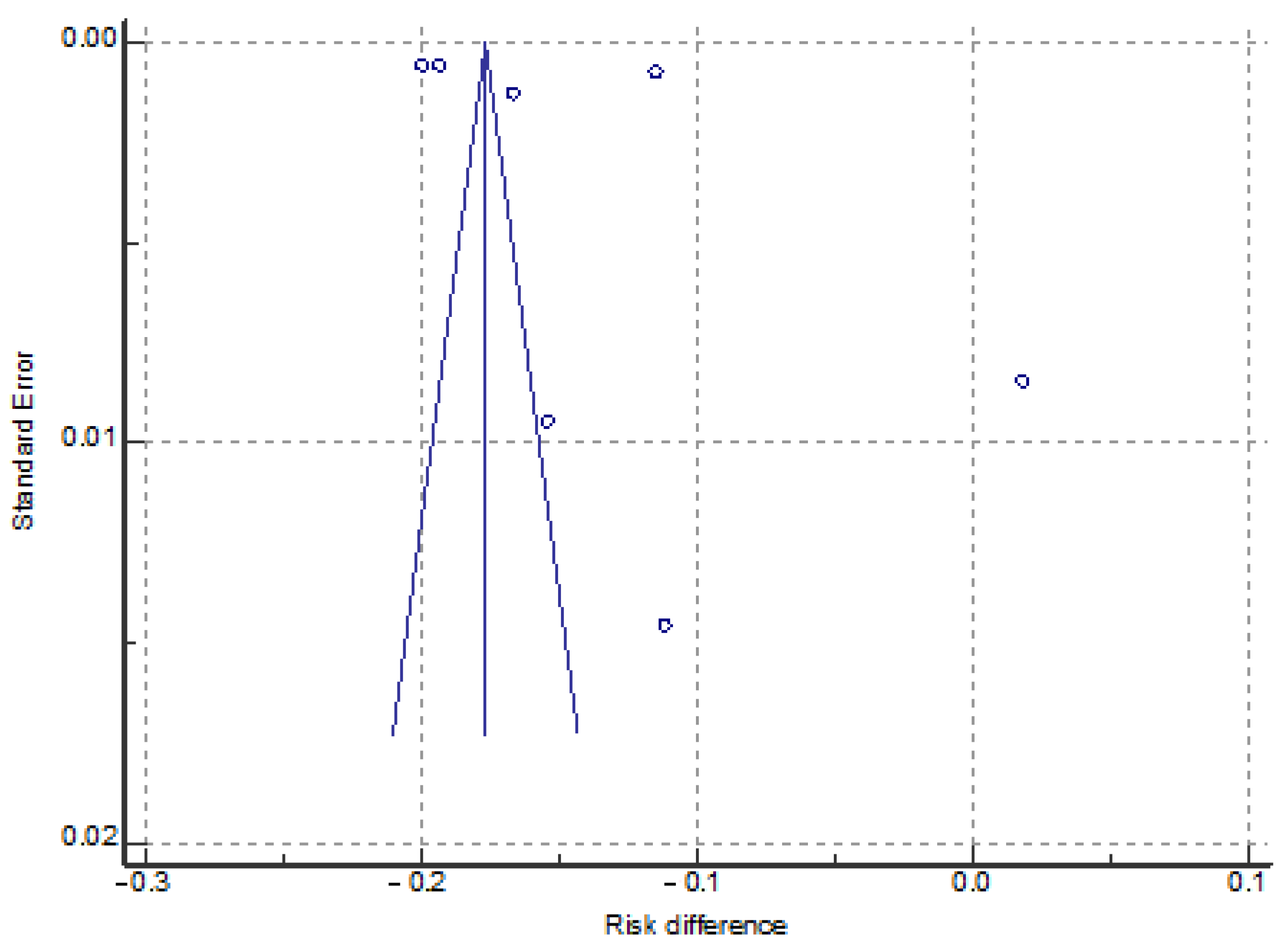
3.4.2. The Pooled Prevalence of Vaccination among Populations with and without an Immigrant Background
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Report on the Health of Refugees and Migrants. 2018. Available online: https://www.who.int/publications/i/item/9789240054462 (accessed on 28 September 2023).
- Holder, J. Tracking Coronavirus Vaccinations Around The World. The New York Times. Available online: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html (accessed on 28 September 2023).
- Han, X.; Xu, P.; Ye, Q. Analysis of COVID-19 vaccines: Types, thoughts, and application. J. Clin. Lab. Anal. 2021, 35, E23937. [Google Scholar] [CrossRef]
- Zaccagni, L.; Rinaldo, N.; Mazzoni, G.; Mandini, S.; Masotti, S.; Toselli, S.; De Luca, F.; Gualdi-Russo, E. Assessing the Impact of COVID-19 Prevention Measures on Adolescent Growth in Italy. Healthcare 2023, 11, 2101. [Google Scholar] [CrossRef]
- European Medicines Agency. Safety of COVID-19 Vaccines. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/covid-19-medicines/safety-covid-19-vaccines (accessed on 6 November 2023).
- IOM. Ensuring Migrants’ Equitable to COVID-19 Vaccines. Available online: https://www.iom.int/ensuring-migrants-equitable-access-covid-19-vaccines (accessed on 30 May 2023).
- European Commission. Statistics on Migration in Europe. Available online: https://commission.europa.eu/strategy-and-policy/priorities-2019-2024/promoting-our-european-way-life/statistics-migration-europe_en (accessed on 30 May 2023).
- El Arab, R.A.; Somerville, J.; Abuadas, F.H.; Rubinat-Arnaldo, E.; Sagbakken, M. Health and well-being of refugees, asylum seekers, undocumented migrants, and internally displaced persons under COVID-19: A scoping review. Front. Public Health 2023, 11, 1145002. [Google Scholar] [CrossRef]
- Magro, P.; Degli Antoni, M.; Formenti, B.; Viola, F.; Castelli, F.; Amadasi, S.; Quiros-Roldan, E. Characteristics of the population with mild COVID-19 symptoms eligible for early treatment attended in a single center in Northern Italy. J. Infect. Public Health 2023, 16, 104–106. [Google Scholar] [CrossRef]
- Crawshaw, A.F.; Farah, Y.; Deal, A.; Rustage, K.; Hayward, S.E.; Carter, J.; Knights, F.; Goldsmith, L.P.; Campos-Matos, I.; Wurie, F.; et al. Defining the determinants of vaccine uptake and undervaccination in migrant populations in Europe to improve routine and COVID-19 vaccine uptake: A systematic review. Lancet Infect. Dis. 2022, 22, e254–e266. [Google Scholar] [CrossRef]
- Abba-Aji, M.; Stuckler, D.; Galea, S.; McKee, M. Ethnic/racial minorities’ and migrants’ access to COVID-19 vaccines: A systematic review of barriers and facilitators. J. Migr. Health 2022, 5, 100086. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Hillen, M.A.; Medendorp, N.M.; Daams, J.G.; Smets, E.M.A. Patient-driven second opinions in oncology: A systematic review. Oncologist 2017, 22, 1197–1211. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Aysit, E.; Ikiisik, H.; Cakir, M.; Maral, I. The Relationship of COVID-19 Vaccination Status with Health Literacy of Syrians Living in Istanbul. Vaccines 2023, 11, 1394. [Google Scholar] [CrossRef]
- Bajos, N.; Spire, A.; Silberzan, L.; Sireyjol, A.; Jusot, F.; Meyer, L.; Franck, J.E.; Warszawski, J. EpiCov study group. When Lack of Trust in the Government and in Scientists Reinforces Social Inequalities in Vaccination Against COVID-19. Front. Public Health 2022, 10, 908152. [Google Scholar] [CrossRef] [PubMed]
- Bastola, K.; Nohynek, H.; Lilja, E.; Castaneda, A.E.; Austero, S.; Kuusio, H.; Skogberg, N. Incidence of SARS-CoV-2 Infection and Factors Associated With Complete COVID-19 Vaccine Uptake Among Migrant Origin Persons in Finland. Int. J. Public Health 2023, 68, 1605547. [Google Scholar] [CrossRef] [PubMed]
- Diaz, E.; Dimka, J.; Mamelund, S.E. Disparities in the offer of COVID-19 vaccination to migrants and non-migrants in Norway: A cross sectional survey study. BMC Public Health 2022, 22, 1288. [Google Scholar] [CrossRef]
- Führer, A.; Pacolli, L.; Yilmaz-Aslan, Y.; Brzoska, P. COVID-19 Vaccine Acceptance and Its Determinants among Migrants in Germany-Results of a Cross-Sectional Study. Vaccines 2022, 10, 1350. [Google Scholar] [CrossRef]
- Gram, M.A.; Moustsen-Helms, I.R.; Valentiner-Branth, P.; Emborg, H.D. Sociodemographic differences in COVID-19 vaccine uptake in Denmark: A nationwide register-based cohort study. BMC Public Health 2023, 23, 391. [Google Scholar] [CrossRef]
- Holz, M.; Mayerl, J.; Andersen, H.; Maskow, B. How Does Migration Background Affect COVID-19 Vaccination Intentions? A Complex Relationship Between General Attitudes, Religiosity, Acculturation and Fears of Infection. Front. Public Health 2022, 10, 854146. [Google Scholar] [CrossRef] [PubMed]
- Kraft, K.B.; Godøy, A.A.; Vinjerui, K.H.; Kour, P.; Kjøllesdal, M.K.R.; Indseth, T. COVID-19 vaccination coverage by immigrant background. Tidsskr. Nor. Laegeforen. 2021, 141. [Google Scholar] [CrossRef]
- Lajunen, T.; Wróbel, B. Acculturation, trust to health care system, and attitudes to COVID-19 vaccination: A comparative study between Polish immigrants in Norway, Polish in Poland, and Norwegians in Norway. Curr. Res. Ecol. Soc. Psychol. 2022, 3, 100047. [Google Scholar] [CrossRef]
- Longchamps, C.; Ducarroz, S.; Crouzet, L.; Vignier, N.; Pourtau, L.; Allaire, C.; Colleville, A.C.; El Aarbaoui, T.; Melchior, M. ECHO study group. COVID-19 vaccine hesitancy among persons living in homeless shelters in France. Vaccine 2021, 39, 3315–3318. [Google Scholar] [CrossRef]
- Madar, A.A.; Benavente, P.; Czapka, E.; Herrero-Arias, R.; Haj-Younes, J.; Hasha, W.; Deeb, G.; Møen, K.A.; Ortiz-Barreda, G.; Diaz, E. COVID-19: Information access, trust and adherence to health advice among migrants in Norway. Arch. Public Health 2022, 80, 15. [Google Scholar] [CrossRef]
- Maifredi, G.; Izzo, I.; Gasparotti, C.; Sileo, C.V.; Hiv-CoV Group; Castelli, F.; Quiros-Roldan, E. SARS-CoV-2 Infection and Vaccination Coverage among Fragile Populations in a Local Health Area of Northern Italy. Life 2022, 12, 1009. [Google Scholar] [CrossRef]
- Page, K.R.; Genovese, E.; Franchi, M.; Cella, S.; Fiorini, G.; Tlili, R.; Salazar, S.; Duvoisin, A.; Cailhol, J.; Jackson, Y. COVID-19 vaccine hesitancy among undocumented migrants during the early phase of the vaccination campaign: A multicentric cross-sectional study. BMJ Open 2022, 12, e056591. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.G.; Tunesi, S.; Consolazio, D.; Decarli, A.; Bergamaschi, W. Evaluation of the anti-COVID-19 vaccination campaign in the Metropolitan Area of Milan (Lombardy Region, Northern Italy). Epidemiol. Prev. 2021, 45, 568–579. [Google Scholar] [CrossRef]
- Svallfors, S.; Larsson, E.C.; Puranen, B.; Ekström, A.M. COVID-19 vaccine hesitancy among first-generation immigrants living in Sweden. Eur. J. Public Health 2023, 33, 687–694. [Google Scholar] [CrossRef]
- Vinjerui, K.V.; Kraft, K.B.; Godøy, A.A.; Kour, P.; Kjøllesdal, M.K.R.; Indseth, T. COVID-19 vaccination among immigrants from Europe and in their countries of birth. Tidsskr. Nor. Laegeforen. 2022, 142. [Google Scholar] [CrossRef]
- Voelker, D.K.; Trent, A.P.; Reel, J.J.; Gould, D. Frequency and psychosocial correlates of eating disorder symptomatology in male figure skaters. J. Appl. Sport. Psychol. 2017, 30, 119–126. [Google Scholar] [CrossRef]
- Zaccagni, L.; Gualdi-Russo, E. The Impact of Sports Involvement on Body Image Perception and Ideals: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 5228. [Google Scholar] [CrossRef] [PubMed]
- AlShurman, B.A.; Khan, A.F.; Mac, C.; Majeed, M.; Butt, Z.A. What Demographic, Social, and Contextual Factors Influence the Intention to Use COVID-19 Vaccines: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 9342. [Google Scholar] [CrossRef]
- Nichol, A.A.; Parcharidi, Z.; Al-Delaimy, W.K.; Kondilis, E. Rapid Review of COVID-19 Vaccination Access and Acceptance for Global Refugee, Asylum Seeker and Undocumented Migrant Populations. Int. J. Public Health 2022, 67, 1605508. [Google Scholar] [CrossRef]
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 vaccination intention in the first year of the pandemic: A systematic review. J. Clin. Nurs. 2022, 31, 62–86. [Google Scholar] [CrossRef]
- Naidoo, D.; Meyer-Weitz, A.; Govender, K. Factors Influencing the Intention and Uptake of COVID-19 Vaccines on the African Continent: A Scoping Review. Vaccines 2023, 11, 873. [Google Scholar] [CrossRef]
- Reich, J.A. Neoliberal Mothering and Vaccine Refusal: Imagined Gated Communities and the Privilege of Choice. Gend. Soc. 2014, 28, 679–704. [Google Scholar] [CrossRef]
- Barrio-Ruiz, C.; Ruiz de Viñaspre-Hernandez, R.; Colaceci, S.; Juarez-Vela, R.; Santolalla-Arnedo, I.; Durante, A.; Di Nitto, M. Language and Cultural Barriers and Facilitators of Sexual and Reproductive Health Care for Migrant Women in High-Income European Countries: An Integrative Review. JMWH 2024, 69, 71–90. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Marmot, M. Role of socialization in explaining social inequalities in Health. Soc. Sci. Med. 2005, 60, 2129–2133. [Google Scholar] [CrossRef] [PubMed]
- Dubbin, L.A.; Chan, J.S.; Shim, J.K. Cultural health capital and the interactional dynamics of patient-centered care. Soc. Sci. Med. 2013, 93, 113–120. [Google Scholar] [CrossRef]
- Askary, E.; Moradi Alamdarloo, S.; Keshtvarz Hesam Abadi, A. Safety of COVID-19 vaccination in pregnant women and their neonatal outcome: A narrative Review. J. Matern. Fetal Neonatal Med. 2023, 36, 2183750. [Google Scholar] [CrossRef] [PubMed]
- Kilada, S.; French, N.; Perkins, E.; Hungerford, D. Pregnant women’s attitudes and behaviours towards antenatal vaccination against Influenza and COVID-19 in the Liverpool City Region, United Kingdom: Cross-sectional survey. Vaccine X 2023, 15, 100387. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.K.; Sijercic, V.C.; Sayad, R.; Ruthig, G.R.; Abdelwahab, S.F.; El-Mokhtar, M.A.; Sayed, I.M. Risks and Preventions for Pregnant Women and Their Preterm Infants in a World with COVID-19: A Narrative Review. Vaccines 2023, 11, 640. [Google Scholar] [CrossRef] [PubMed]
- Fiammenghi, C.; Mbaye, N.A.; Pelleri, D.; Ceretti, E.; Gelatti, U.; Covolo, L. COVID-19 vaccination during pregnancy: A mixed-methods study of attitudes in a sample of Italian women and the role of health professionals’ communication. Patient Educ. Couns. 2023, 115, 107929. [Google Scholar] [CrossRef]
- Lloyd-Sherlock, P.; Ebrahim, S.; Geffen, L.; McKee, M. Bearing the brunt of COVID-19: Older people in low and middle income countries. BMJ 2020, 368, m1052. [Google Scholar] [CrossRef] [PubMed]
- Speletas, M.; Voulgaridi, I.; Bogogiannidou, Z.; Sarrou, S.; Kyritsi, M.A.; Theodoridou, A.; Dadouli, K.; Matziri, A.; Vontas, A.; Pappa, D.; et al. Dynamics of Anti-SARS-CoV-2 IgA and IgG Responses and Their Protective Effect against Fatal Disease after Booster COVID-19 Vaccination. Vaccines 2023, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Dandu, H.; Goel, A.; Kumar, M.; Malhotra, H.S.; Katiyar, H.; Agarwal, M.; Kumar, N.; Pandey, P.; Rani, S.; Yadav, G. Humoral and cellular immune response in patients of liver cirrhosis and immunocompetent recipient of ChAdOx1nCoV-19 Vaccine (Covishield). Clin. Exp. Med. 2024, 24, 24. [Google Scholar] [CrossRef] [PubMed]
- Deal, A.; Hayward, S.E.; Huda, M.; Knights, F.; Crawshaw, A.F.; Carter, J.; Hassan, O.B.; Farah, Y.; Ciftci, Y.; Rowland-Pomp, M.; et al. ESCMID Study Group for Infections in Travellers and Migrants (ESGITM). Strategies and action points to ensure equitable uptake of COVID-19 vaccinations: A national qualitative interview study to explore the views of undocumented migrants, asylum seekers, and refugees. J. Migr. Health 2021, 4, 100050. [Google Scholar] [CrossRef]
- Akbulut, S.; Boz, G.; Ozer, A.; Sahin, T.T.; Colak, C. Evaluation of the Turkish Population’s Perspective on COVID-19 Vaccine Hesitancy and Routine Childhood Vaccine Applications: National Survey Study. Vaccines 2023, 11, 779. [Google Scholar] [CrossRef]
- CDBIO. Guide to Health Literacy. Contributing to Trust Building and Equitable Access to Healthcare. Available online: https://www.coe.int/en/web/bioethics/guide-to-health-literacy#{%22128387839%22:[1]} (accessed on 4 October 2023).
- Plümper, T.; Neumayer, E. The Politics of COVID-19 Containment Policies in Europe. Int. J. Disaster Risk Reduct. 2022, 81, 103206. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors (Year) -Study Design- | Host Country | Country of Origin | Participant Groups (Sex, N, Education, Income, Comorbidities) | Age (Years) | Year and Method of Data Collection | Infection and/or Prevalence of COVID-19 Vaccination Willingness and Hesitancy | Main Factors of Refusal or Hesitancy to COVID-19 Vaccination |
|---|---|---|---|---|---|---|---|
| Aysit et al. (2023) [16] -cross-sectional- | Turkey | Syria | In the target group of 911 Syrians Under Temporary Protection in Istanbul, 598 questionnaires were distributed, including 571 people. 80.7% women. 26.6% high school level. 24.7% with chronic diseases. 45% with chronic diseases in the family. Mean duration of stay in Turkey: 6.14 ± 2.22 years. | ≥18 years 31.92 ± 6.14 | February, March, and May 2022 Questionnaires translated into Arabic | Vaccinated: 56.4% of males and 42.3% of females; 54.4% aged ≥35 years; 50% high school and above; 68.6% with regular job; 54.6% with chronic disease and 54.1 with a chronic disease in the family. The local population has a rate of at least one dose of vaccine above 90% vs. 45% of immigrants. | The study shows by logistic regression that the variables associated with COVID-19 vaccination status are male sex, older age, middle/upper economic status, and the presence of chronic diseases in the family. In addition, vaccination was more frequent in individuals with high levels of health literacy. |
| Bajos et al. (2022) [17] -random population-based cohort survey- | France | Partially specified for people native to French Overseas Departments (FOD) (Martinique, Guadeloupe, Reunion Island, Guyana, and Mayotte) and racially minoritized groups (immigrants or descendants of immigrants from the Maghreb, Turkey, Asia, and sub-Saharan African countries) | 80,971 persons living in metropolitan France. Among them there were native to FOD, racially minoritized first-generation and second-generation immigrants, non-racially minoritized first-generation and second-generation immigrants. All others constitute the mainstream population. | ≥18 years | July 2021 Computer-assisted web interviews (CAWI) or computer-assisted telephone interviews (CATI) | Vaccinated with at least 1 dose: 74.5% mainstream pop.; 56.2% born in FOD; racially minoritized groups: 52.5% (2nd generation) and 59.1% (1st gen); other immigrants: 75.6% (2nd gen) and 76.3% (1st gen). Refusal to vaccinate: 7.8% mainstream pop.; 14.2% born in FOD; racially minoritized groups: 12.8% (2nd generation) and 7.4% (1st gen); other immigrants: 7.1% (2nd gen) and 7.0% (1st gen). No trust at all in government: 17.5% mainstream pop.; 21.3% born in FOD; racially minoritized groups: 20.2% (2nd generation) and 11.8% (1st gen); other immigrants: 16.3% (2nd gen) and 12.1% (1st gen). No trust at all in scientists: 3.6% mainstream pop.; 8.9% born in FOD; racially minoritized groups: 6.8% (2nd gen) and 4.4% (1st gen); other immigrants: 3.2% (2nd gen) and 2.9% (1st gen). | The unvaccinated were found to be younger, less educated, lower income, and often from racially minoritized groups. The factors most associated with vaccination refusal were a lack of trust in the government and scientists to contain the spread of the epidemic. |
| Bastola et al. (2023) [18] -cross-sectional- | Finland | Russia, Estonia, Europe (excl. Russia, Estonia)/North America/Oceania, Middle East/North Africa, Africa (excl. North Africa), Southeast Asia, Asia (excl. Southeast Asia)/Latin America | 13,223 immigrants in Finland (48% females). FinMonik (based on the Survey on Wellbeing among Foreign-Born Population) sample: 89.3% lived in urban centers. 82.6% were aged ≥18 years at migration. Length of stay in Finland was ≥12 years in 51.9% of the sample. Among MigCOVID (based on the Impact of Coronavirus Epidemic on Wellbeing among Foreign-born Population) subsample (3668 immigrants): secondary level of education (46.3%); full-time or part-time workers for 64.5%; beginning or intermediate knowledge of the language in 64.2%; no psychological distress in 80.3%; no perceived discrimination 85%; perception of fairly good/good health in 71.8%. | 20–66 years | October 2020–February 2021 Registers, electronic or paper-based questionnaires in 18 languages, and multilingual telephone interviews | The highest incidence of infection was in immigrants from Africa (19.4%), and the lowest was in immigrants from Southeast Asia (5.1%). 61.4% of immigrants completed vaccine uptake: the complete vaccination uptake ranged from 85.0% (Southeast Asians) to 41.0% (Estonians). | In the FinMonik sample, the male sex, younger age, migration age <18 years, and shorter length of residence were associated with lower COVID-19 vaccine uptake. In the MigCovid subsample, younger age, being economically inactive, poorer language skills, experiences of discrimination, and psychological distress were associated with lower vaccine uptake. |
| Diaz et al. (2022) [19] -cross-sectional- | Norway | Sweden, Pakistan, Philippines, Poland, Somalia | 1284 immigrant residents in 6 parishes in Oslo (50.9% females). Education: no University: 40.4%. 3596 non-immigrants in the same parishes in Oslo (60.5% females). Education: no University: 37.8%. | ≥18 years | 16–24 June 2021 web-based survey | Vaccine offer: 68.1% of immigrants vs. 81.1% of non-immigrants Vaccine uptake (% of those offered): 79.9% in immigrants vs. 91.1% in non-immigrants Confirmed case of COVID-19: 8.4% in immigrants vs. 4.0 in non-immigrants | There are disparities between non-immigrants and immigrants in actual vaccine uptake. The vaccine offer was lower in immigrants than in non-immigrants. Females were more likely than males to receive the vaccine, while individuals with some university education were less likely. No differences were found by language spoken at home, or by country of origin. While length of residence was found to be an important explanatory variant, immigrants who had lived in Norway for less than 15 years were less likely to refer to the vaccine offer. |
| Führer et al. (2022) [20] -cross-sectional- | Germany | Germany, Turkey, Syria, Venezuela, Iran, etc. | 204 immigrants residing in Germany (57.1% females). Education: more than 10 years in 80.2% of immigrants. Median duration of stay in Germany: 6.5 years | ≥18 years Mean age: 37 years | September 2021–January 2022 German online questionnaire translated into 5 more languages | Acceptance Importance of COVID-19 vaccine: yes in 68.6%, no in 18.9%, undecided in 7.3%. Fear of side effects: 55%; no fear: 26.7%. Safe vaccination: 31%; no safe vaccination: 47.9%. Non-dangerousness of COVID-19: 42.7%; dangerousness:37%. Finally, 26% believe that nature should take its course, 52% believe in natural remedies, and 26% are afraid of syringes. Vaccination status 80% (n = 154) had already received at least one dose of COVID-19 vaccine; 2% (n = 4) had not been vaccinated but already had an appointment for vaccination; 17% (n = 33) had no appointment. | The overall vaccination rate of immigrants was comparable to that of the general population. The high vaccination rate found in this study may depend on the high level of education and safe residence status of the respondents. |
| Gram et al. (2023) [21] -nationwide register-based cohort study- | Denmark (5 geographical regions) | Immigrants of Western descent (born abroad, without any parent Danish citizen or born in Denmark), descendants of Western immigrants (born in Denmark, without any parent Danish citizen or born in Denmark), immigrants of non-Western descent (born abroad, without any parent Danish citizen or born in Denmark), descendants of non-Western immigrants (born in Denmark, without any parent Danish citizen or born in Denmark). | Overall, 5,164,558 individuals (50.5% females). By immigrant status: 341,830 immigrants of Western descent, 15,300 descendants of Western immigrants, 367,200 immigrants of non-Western.descent, 108,475 descendants of non-Western immigrants 4,330,606 Danish (born in Denmark or abroad with at least one parent who is both a Danish citizen and born in Denmark). | ≥12 yrs Overall mean age: 47 ± 20.7 yrs | From 27 December 2020 to 20 October 2021. Danish registries on infections and vaccinations | Vaccination coverage ranged between 85.5% and 88.7% across the 5 geographical regions. 87.1% received at least the first dose of COVID-19 vaccine. The coverage was similar between sexes, and lower in: -younger group (12–15 yrs) (70%); -no Danish individuals especially in descendants of non-Western immigrants (49.2%); -individuals without chronic diseases (86.0%); -individuals with an income <33,605 € (85.0%); -individuals with upper secondary school (85%) or primary school (83.9%) -individuals with a previous SARS-CoV-2 infection (79.5%); -individuals never PCR-tested (69.6%). | There was a high COVID-19 vaccine uptake in Denmark, but large socio-demographic differences in vaccine uptake have been identified that particularly affected younger age groups. |
| Holz et al. (2022) [22] -cross-sectional data collected via a third-party online access panel provider- | Germany | Countries of origin: 63.3% Europe; 21% non-Europe; 15.6% other | 477 first-generation immigrants residing in Germany (53.7% females). Education: 63.6% secondary degree. Mean years since migration: 22.6 ± 16.38. 532 native Germans without migration background (47.1% females). Education: 56.2% secondary degree. | 18–65 years Immigrants mean: 41.56 ± 12.71 years Non-immigrant Germans mean: 44.13 ± 13.67 yrs. | 15 March 2021–25 March 2021 Participants randomly drawn from the database of the panel provider and incentivized by earning 50 Euro-Cents per 10 min interview time | Vaccination intention % Definitely: 34.9% of immigrants vs 51.4% in native Germans. Not at all: 21.1% of immigrants vs. 14.2% of native Germans. | An increase in positive antecedents such as religiosity, which positively influence general attitudes such as fears of infection and intention to vaccinate were found in immigrants. However, a significant direct negative association with vaccination was also found in immigrants. Political trust and health consciousness have increased over the years since migration. European immigrants have less political trust, fear of personal contagion, and lower intention to vaccinate than non-European immigrants. |
| Kraft et al. (2021) [23] -cohort study- | Norway Different lengths of residence (<6 years, 6–10, 11–15, 16+ years of residence) were considered | Norway, Vietnam, Sri Lanka, Thailand, Denmark, Philippines, India, UK, Sweden, Iran, Iceland, Pakistan, Brazil, Finland, Netherlands, USA, Afghanistan, Bosnia-Herzegovina, Chile, China, Kosovo, Turkey, Germany, Ethiopia, Iraq, Syria, Morocco, Spain, Eritrea, France, Serbia, Ukraine, Somalia, Croatia, Russia, Lithuania, Poland, Bulgaria, Romania, Latvia, etc. | 746,062 Norway residents with a migratory background including 689,540 foreign-born, and 57,153 Norwegian-born with foreign-born parents (48% females). Higher education: foreign-born 32.00%; Norwegian-born with foreign-born parents 39.18%. Income: foreign-born: NOK 299898; Norwegian-born with foreign-born parents: NOK 304288. Reference group: 3,518,308 Norwegian-born with Norwegian-born parents (50% of females) Higher education: 36.30%. Income: NOK 402683 | ≥18 years Foreign-born: 44 ± 14 yrs Norwegian-born with foreign-born parents: 29 ± 12 yrs Norwegian-born: 50 ± 19 yrs. | At least 1 dose from 8 December 2020, to 20 October 2021. National Register of COVID-19 vaccinations | Vaccinated with at least 1 dose -Foreign-born: 73% -Norwegian-born with foreign-born parents: 82% (Norwegian-born: 93%) | COVID-19 vaccination coverage is lower in immigrant groups in Norway than in Norwegian-born persons. Based on different country backgrounds, vaccination coverage is high and hovers around 90% in immigrants from countries such as Vietnam (93%), Sri Lanka (91%), Thailand (91%), Denmark (89%), Philippines (89%), India (88%), the UK (88%), Sweden (88%), and Iran (87%). Relatively low coverage is observed in immigrants from countries such as Latvia (44%), Bulgaria (45%), Romania (45%), Poland (46%), and Lithuania (47%). There are also differences among immigrant groups partly attributable to income and education. |
| Lajunen, Wróbel (2022) [24] -cross-sectional- | Norway | Poland | 150 Polish first-generation immigrants in Norway (47.7% females). 256 Poles living in Poland (52.3% females). 264 Norwegians living in Norway (63.2% females). | ≥18 years Immigrants mean: 42.2 ± 11.8 yrs Poles living in Poland mean: 42.9 ± 11.8 yrs Norwegians mean: 38.9 ± 18.4 yrs | March–May 2021. Internet-based anonymous survey | Attitude to the COVID-19 vaccine was assessed using a scale constructed as the average of answers to eight items about the COVID-19 vaccine recorded with a five-point Likert scale from “totally disagree” (1) to “totally agree” (5): Poles in Norway: 3.08 ± 1.29 Poles in Poland 3.29 ± 1.14 Norwegians in Norway 4.31 ± 0.55 | The attitudes of Polish immigrants in Norway toward COVID-19 vaccination were found to be similar to Polish immigrants living in Poland. Confidence in the competence and values of the Norwegian health-care system among Polish immigrants was significantly lower than among the Norwegian population without immigrant background. This mistrust results in lower immunization rates among Polish immigrants, with a consequent possible increase in unnecessary suffering and health inequalities. |
| Longchamps et al. (2021) [25] -cross-sectional ECHO study- | France (Paris, Lyon, Strasbourg) | Europe (15.6%) Africa (59.5%) Eastern Mediterranean (21.5%) Other (3.4%) | N = 235 residents in 18 homeless shelters (66.3% males; 62.9% secondary school or less; 70.5% not employed 60.8% no legal residence in France). 27.9% Depression 25.5% chronic disease 76.4% trust in official information on COVID-19 | 19.3% of 18–24 y; 41.8% of 25–34 y; 25.9% of 35–49 y; 13% of ≥50 y | 2 May–28 June 2020 (before anti-COVID-19 vaccines were approved for use); Interview in person or by telephone Questionnaire administered in French, English, or the participant’s language (25% of the questionnaires were completed with the assistance of a trained translator contacted by telephone) | Vaccine hesitancy 40.9% (71.2% No; 28.8% I don’t know) By sex: Male: 32.5% Female: 55.5% By country of birth: Europe: 52.7% Africa: 43.6% Eastern M. 30.0% Other: 12.5% By household composition: Living alone: 36.9% Living with a partner: 56.1% By administrative status: Legal residence: 48.9% No legal residence: 35.9% By health literacy: Low: 50.9% Intermediate/high: 31.3% Findings are in line with observations from general population surveys | Determinants of vaccine hesitancy were sex, household composition, administrative status, and health literacy: being female (OR 2.55), living with a partner (OR 2.48), without legal residence (OR 0.51), and with low health literacy (OR 0.38) were associated with vaccine hesitancy. Women are more likely to express vaccine hesitancy than men. Health care is not always adapted to immigrants’ needs, resulting in inadequate or negative experiences. Low health literacy means limited capacity to seek and evaluate health information All messages on measures that can prevent COVID-19 should be adapted to be easily understood by all. |
| Madar et al. (2022) [26] -cross-sectional. It is part of the project Inncovid- | Norway | Poland, Spain, India, Somalia, Arabic language area | 529 immigrants living in Norway (47.6% females). Ethnicity: 33 Somali, 137 Arabic, 72 Tamil, 113 Spanish, 174 Polish. Years in Norway: 67.3% over 5 years. Health status: 60.7% excellent/very good | ≥18 years 81% between 26 and 55 years | Between 25 May and 1 July of 2020. Online survey. A questionnaire translated into five different languages (Polish, Arabic, Somali, Tamil and Spanish) with a completion time of around 15 min | COVID-19 infection -No (documented or presumed) in 96.5% of immigrants. -Yes (documented or presumed) in 3.7% of immigrants Information from health authorities: -Yes in 82% of immigrants Inaccuracy of information from social media: -Agree in 78.6% of immigrants | Immigrants in Norway believe they have received adequate information about COVID-19 and have high compliance with preventive measures, although many variations between groups were found. In particular, Poles reported the lowest levels of trust while Tamil- and Arabic-speaking respondents reported high levels of trust in the health-care system. The majority of immigrants agreed that by following the recommendations, they could avoid getting sick, but more skepticism was found among the Spanish and Polish. |
| Maifredi et al. (2022) [27] -cohort study- | Italy (Brescia) | Foreigners (inhabitants with non-Italian citizenship at enrollment) | 134,492 foreigners (51.4% females). Comorbidity: none (76.9%); 1 (15.6%); 2–3 (7.1%); >3 (1.40%). 869,718 Italians (50.9% females). Comorbidity: none (53.1%); 1 (20.1%); 2–3 (18.3%); >3 (8.0%). | >18 years Foreigners median: 40.6 yrs (31.5–50.8) Italians median: 53.7 yrs (39.6–68.5) | 30 September–31 December 2021. Brescia Local Health Agency Database | Unvaccinated (%) On 31 December 2021: -25.3% of foreigners -8.7% of Italians | Diagnosis of SARS-CoV-2 infection may be less attainable for foreigners due to misinformation, language barriers, and lack of trust in traditional medicine. This would explain the fact that only severe cases reached hospitals. The probability of undergoing COVID-19 vaccination increased with the male gender and the number of comorbidities among foreigners, while, among Italians, also age (50–69, or >70) contributed. Hesitancy to vaccinate against COVID-19 was higher among foreigners than among Italians. The likelihood of not being vaccinated among foreigners was significantly higher in women, people without chronic comorbidities, and people aged >50 years. |
| Page et al. (2022) [28] -multicentric cross-sectional survey- | Switzerland (Geneva), Italy (Milan), France (Paris) | Africa, the Americas, the Eastern Mediterranean, Europe, Asia, Western Pacific. | 670 undocumented immigrants: Geneva N = 441 (63.4% females); Milan N = 126 (67.2% females); Paris N = 103 (30.1% females). | >16 yrs Mean Age (yrs): Geneva 39 ± 17; Milan 41 ± 20; Paris 35 ± 16 | February–May 2021. Anonymous structured questionnaire translated into 10 languages available at health facilities. | Willingness to vaccinate -52% in Milan vs. 82% in Italy (December 2020) -14.6% in Paris vs. 71.8 in France (June 2020). -39% in Geneva | The vast majority of participants had perceived that COVID-19 vaccination was accessible to all, while the remainder predominantly thought they could not access it due to lack of health insurance. The low demand for vaccination was related to age, comorbidity, and views on vaccination. Women were more likely to be vaccinated than men. Social media (Milan) and community networks (Paris) were found to be negatively associated with demand. Hospitals were the preferred place for vaccination |
| Russo et al. (2021) [29] -cohort study- | Italy (Metropolitan Area of Milan: residents in Milan and Lodi) | Not reported | 2,981,997 persons (52.1% females). 414,920 persons with foreign nationality. | ≥19 years | Between 1 January and 30 September 2021. A new regional registry (NAR) of caregivers integrated with information from the permanent geo-referencing system. | Vaccinated with at least 1 dose: 73.2% immigrants 86.2% Italians -51.52% males -48.48% females | Women are less likely to get vaccinated than men, as are the age groups 50–59 years and 70+ years. In addition, residents of more deprived areas were found to be less likely to be vaccinated than those living in more affluent areas. Italian citizens were found to be more likely to vaccinate than foreigners. This willingness increased as the number of chronic conditions they had increased. Uptake of the vaccination campaign is influenced by the socio-demographic characteristics of the population and is a determining factor in the prevention of hospitalizations. |
| Svallfors et al. (2023) [30] -cross-sectional study- | Sweden | Middle East and North Africa (53%); Sub-Saharan Africa, Eastern Europe; Western Europe, North America, Australia or New Zealand; South America; Asia. | 2612 first-generation immigrants (49% females). Secondary level of education: 36%. Cohabiting or married: 63%. Place of residence: city (41%) or big city (36%). 18% had somewhat low or very low trust in Swedish authorities. | ≥16 yrs | April–May and August–September 2021. computer-assisted per- sonal interviews and web interviews. The survey was developed in Swedish and translated into 7 additional languages. | Vaccine hesitancy: 77% were vaccinated or intended to be vaccinated, considering it very important for themselves and others (58%). 21% had already had the infection. Of the 23% who were hesitant, 5% said they would not vaccinate, 7% probably not, 4% did not know, and 7% did not want to answer. 11% do not think vaccination is important for their health and 7% for others’ health. When this study started, 81% of Swedes over the age of 16 were fully vaccinated vs. 68% of those born abroad (August 2021). | Determinants of COVID-19 vaccination hesitancy were found to be: young age, arrival in Sweden during the 2015 migration wave, Eastern European origin, female gender, lower education level, lack of trust in authorities, and lower perception of vaccination benefits. |
| Vinjerui et al. (2022) [31] -cross-sectional- | Norway | Immigrants born in 22 EU countries: Austria, Belgium, Bulgaria, Denmark, Estonia, Finland, France, Iceland, Italy, Croatia, Latvia, Lithuania, the Netherlands, Poland, Portugal, Romania, Slovakia, Spain, Sweden, Czech Republic, Germany, Hungary. | 276,506 residents born abroad (46% females). Period of residence <6 yrs: 17%. Median income: 344,282 NOK 3,575,107 Norwegians (50% females). Median income: 401,387 NOK | ≥18 years Immigrants mean: 43.14 ± 14 yrs Non-migrant Norwegians mean: 50 ± 19 yrs | By 30 September 2021 National Register of COVID-19 vaccinations | Vaccination
coverage ranged from 24.3% (in Bulgaria) to 98.1% (in Portugal) in European countries, from 44.0% to 89.2% among immigrants of European descent in Norway in September 2021. Bulgarian immigrants showed the lowest COVID-19 vaccination coverage compared to other immigrants in Norway. Bulgaria was also the birth country in Europe with the lowest percentage of vaccinated people. | A covariation was found between the vaccination coverage of immigrant groups from Europe and the vaccination rate in their countries of birth. Vaccination coverage was higher in immigrants with a long period of residence in Norway than in those with a short period of residence, but there was no significant difference in the covariation with the country of birth for people who lived in Norway for a long or short period of residence. |
| References in Alphabetical Order | Clarity of Stated Aim (0–2) | Sample Selection | Comparability | Outcome | NOS Score (0–16) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample Representativeness (0–2) | Sample Size (0–2) | Non-Respondents (0–2) * | Ascertainment of the Exposure (0–2) | Control of Confounding Factors (0–1) | Comparability of Participants (0–1) | Assessment of the Outcome (0–2) | Statistical Tests (0–2) | |||
| Aysit et al. (2023) [16] | 2 | 1 | 2 | 1 | 2 | 0 | 0 | 2 | 2 | 12 |
| Bajos et al. (2022) [17] | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 13 |
| Bastola et al. (2023) [18] | 2 | 2 | 2 | 1 | 2 | 1 | 0 | 2 | 2 | 14 |
| Diaz et al. (2022) [19] | 2 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 10 |
| Führer et al. (2022) [20] | 2 | 0 | 0 | 0 | 2 | 0 | 0 | 1 | 2 | 7 |
| Gram et al. (2023) [21] | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 15 |
| Holz et al. (2022) [22] | 2 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 2 | 10 |
| Kraft at al. (2021) [23] | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 15 |
| Lajunen, Wróbel (2022) [24] | 2 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 6 |
| Longchamps et al. (2021) [25] | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 2 | 7 |
| Madar et al. (2022) [26] | 2 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 7 |
| Maifredi et al. (2022) [27] | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 15 |
| Page et al. (2022) [28] | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 1 | 2 | 9 |
| Russo et al. (2021) [29] | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 1 | 15 |
| Svallfors et al. (2023) [30] | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 1 | 1 | 8 |
| Vinjerui et al. (2022) [31] | 1 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 2 | 14 |
| Study or Subgroup | Sample Size | Proportion (%) | 95% CI | Weight (%) | |
|---|---|---|---|---|---|
| Bajos (2022) [17] * | 2799 | 59.09 | 57.25 to 60.92 | 10.96 |  |
| Bajos (2022) [17] ** | 2629 | 76.30 | 74.63 to 77.92 | 10.83 | |
| Bastola (2023) [18] | 13,223 | 61.40 | 60.57 to 62.23 | 12.97 | |
| Diaz (2022) [19] | 875 | 79.89 | 77.07 to 82.50 | 7.67 | |
| Fuhrer (2022) [20] | 204 | 79.90 | 73.74 to 85.17 | 3.15 | |
| Gram (2023) [21] | 709,030 | 71.30 | 71.20 to 71.41 | 13.62 | |
| Kraft (2021) [23] | 689,540 | 73.00 | 72.90 to 73.11 | 13.62 | |
| Maifredi(2022) [27] | 127,504 | 74.61 | 74.37 to 74.85 | 13.56 | |
| Russo (2021) [29] | 414,920 | 73.22 | 73.09 to 73.36 | 13.61 | |
| Total | 1,960,724 | 71.28 | 70.02 to 72.52 | 100.00 |
| Study | Difference | 95% CI | Weight (%) | |
|---|---|---|---|---|
| Bajos(2022) [17] * | −0.154 | −0.173 to −0.136 | 13.97 |  |
| Bajos(2022) [17] ** | 0.018 | 0.001 to 0.035 | 14.11 | |
| Diaz (2022) [19] | −0.112 | −0.141 to −0.084 | 13.07 | |
| Gram (2023) [21] | −0.194 | −0.195 to −0.193 | 14.72 | |
| Kraft (2021) [23] | −0.200 | −0.201 to −0.199 | 14.72 | |
| Maifredi (2022) [27] | −0.167 | −0.169 to −0.164 | 14.70 | |
| Russo (2021) [29] | −0.115 | −0.116 to −0.114 | 14.71 | |
| Total | −0.133 | −0.164 to −0.102 | 100.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gualdi-Russo, E.; Zaccagni, L. COVID-19 Vaccination and Predictive Factors in Immigrants to Europe: A Systematic Review and Meta-Analysis. Vaccines 2024, 12, 350. https://doi.org/10.3390/vaccines12040350
Gualdi-Russo E, Zaccagni L. COVID-19 Vaccination and Predictive Factors in Immigrants to Europe: A Systematic Review and Meta-Analysis. Vaccines. 2024; 12(4):350. https://doi.org/10.3390/vaccines12040350
Chicago/Turabian StyleGualdi-Russo, Emanuela, and Luciana Zaccagni. 2024. "COVID-19 Vaccination and Predictive Factors in Immigrants to Europe: A Systematic Review and Meta-Analysis" Vaccines 12, no. 4: 350. https://doi.org/10.3390/vaccines12040350