
Estimating the Total Societal Cost of a Hexavalent Vaccine versus a Pentavalent Vaccine with Hepatitis B in South Korea
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
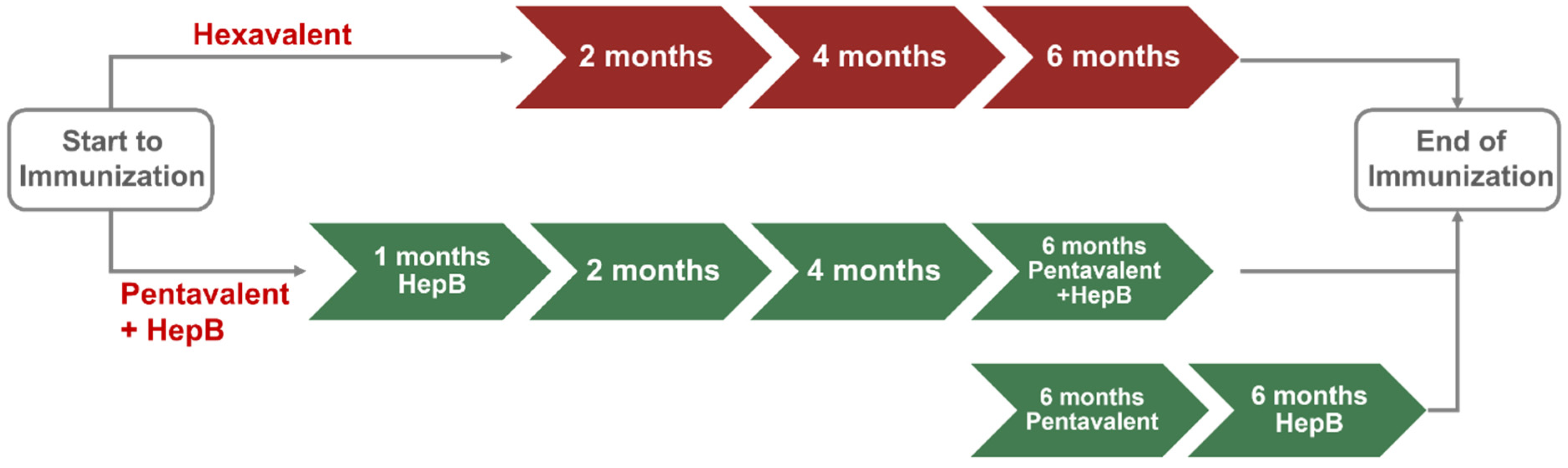
2.1. Vaccination Strategies
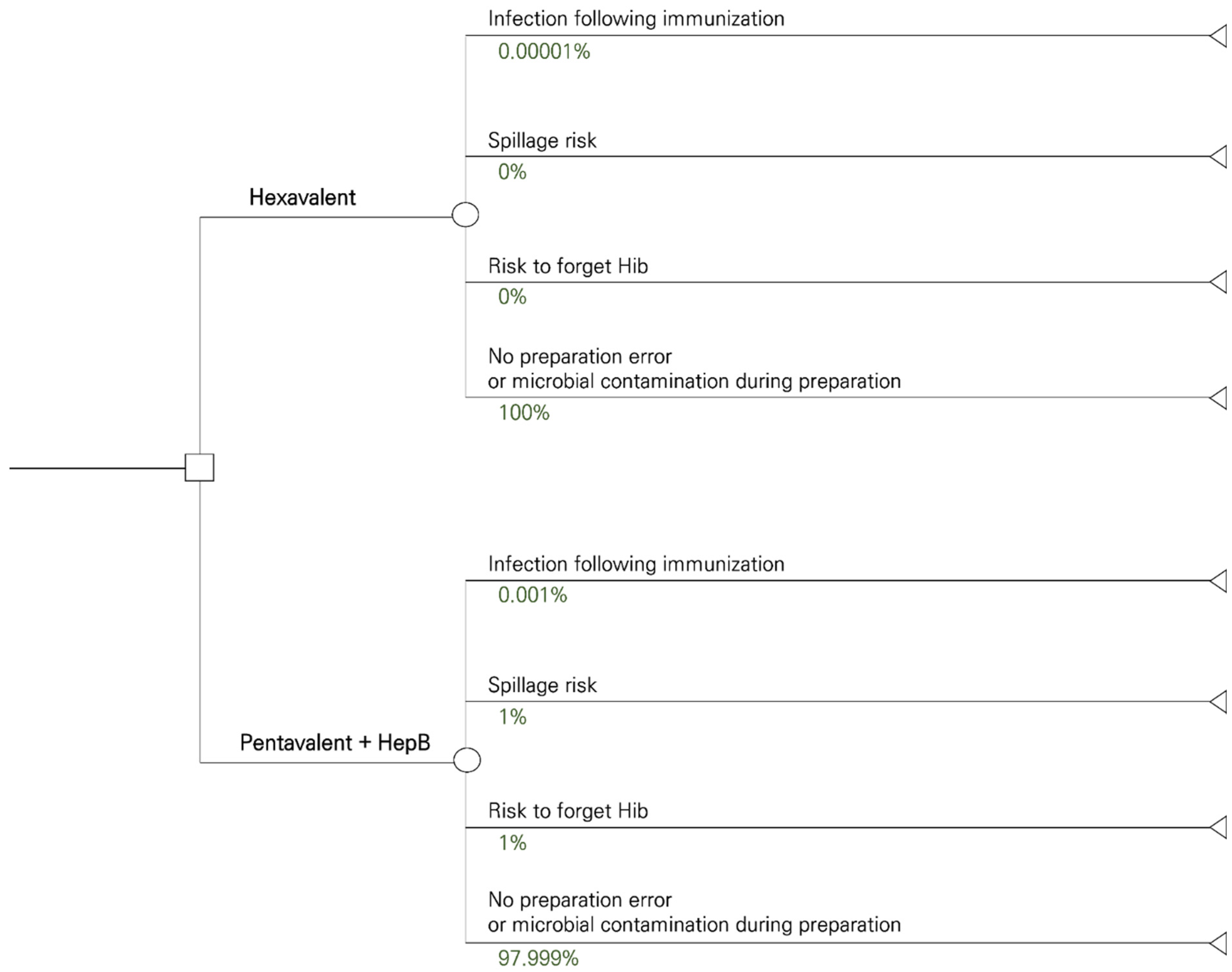
2.2. Model Overview
2.3. Input Parameters
2.3.1. Vaccine-Related Probabilities
2.3.2. Costs
2.4. Model Outcomes
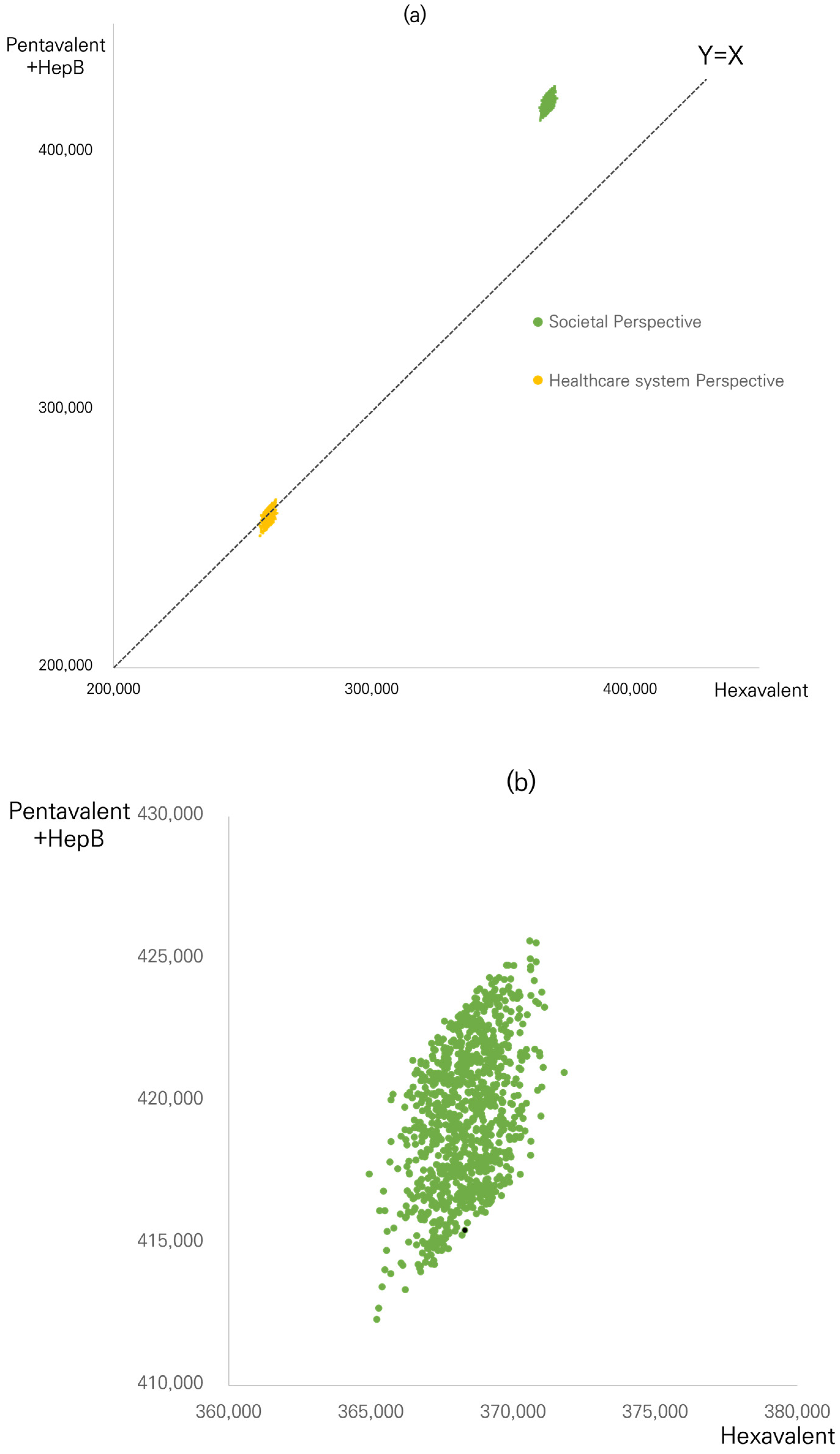
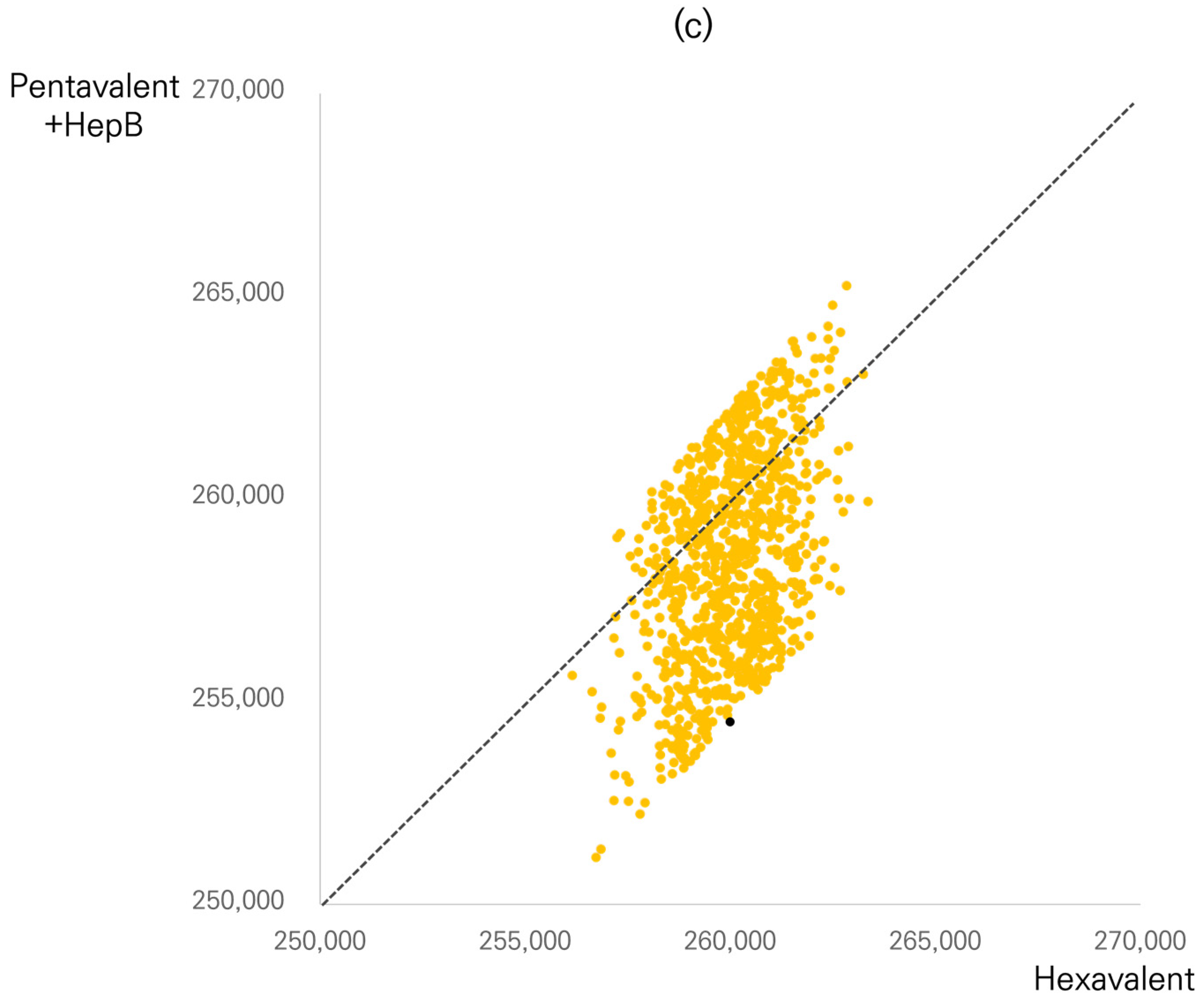
2.5. Probabilistic Simulation
2.6. Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kroger, A.B.L.; Hunter, P. General Best Practice Guidelines for Immunization. Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022.
- Skibinski, D.A.; Baudner, B.C.; Singh, M.; O’Hagan, D.T. Combination vaccines. J. Glob. Infect. Dis. 2011, 3, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Kalies, H.; Grote, V.; Verstraeten, T.; Hessel, L.; Schmitt, H.J.; von Kries, R. The use of combination vaccines has improved timeliness of vaccination in children. Pediatr. Infect. Dis. J. 2006, 25, 507–512. [Google Scholar] [CrossRef]
- Weston, W.M.; Klein, N.P. Kinrix: A new combination DTaP-IPV vaccine for children aged 4–6 years. Expert Rev. Vaccines 2008, 7, 1309–1320. [Google Scholar] [CrossRef]
- Dicko, M.; Oni, A.Q.; Ganivet, S.; Kone, S.; Pierre, L.; Jacquet, B. Safety of immunization injections in Africa: Not simply a problem of logistics. Bull. World Health Organ. 2000, 78, 163–169. [Google Scholar]
- Centers for Disease Control and Prevention. Combination vaccines for childhood immunization. Recommendations of the Advisory Committee on Immunization Practices (ACIP), the American Academy of Pediatrics (AAP), and the American Academy of Family Physicians (AAFP). Am. Fam. Physician 1999, 59, 2565–2574. [Google Scholar]
- Oliver, S.E.; Moore, K.L. Licensure of a Diphtheria and Tetanus Toxoids and Acellular Pertussis, Inactivated Poliovirus, Haemophilus influenzae Type b Conjugate, and Hepatitis B Vaccine, and Guidance for Use in Infants. Morb. Mortal. Wkly. Rep. 2020, 69, 136–139. [Google Scholar] [CrossRef]
- Obando-Pacheco, P.; Rivero-Calle, I.; Gómez-Rial, J.; Rodríguez-Tenreiro Sánchez, C.; Martinón-Torres, F. New perspectives for hexavalent vaccines. Vaccine 2018, 36, 5485–5494. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Infanrix Hexa: EPAR—Product Information; European Medicines Agency: Amsterdam, The Netherlands, 2022.
- European Medicines Agency. Hexyon: EPAR—Product Information; European Medicines Agency: Amsterdam, The Netherlands, 2022.
- European Medicines Agency. Vaxelis: EPAR—Product Information; European Medicines Agency: Amsterdam, The Netherlands, 2022.
- De Coster, I.; Fournie, X.; Faure, C.; Ziani, E.; Nicolas, L.; Soubeyrand, B.; Van Damme, P. Assessment of preparation time with fully-liquid versus non-fully liquid paediatric hexavalent vaccines. A time and motion study. Vaccine 2015, 33, 3976–3982. [Google Scholar] [CrossRef] [PubMed]
- Larmené-Beld, K.H.M.; Spronk, J.T.; Luttjeboer, J.; Taxis, K.; Postma, M. A Cost Minimization Analysis of Ready-to-Administer Prefilled Sterilized Syringes in a Dutch Hospital. Clin. Ther. 2019, 41, 1139–1150. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Harris, R.C.; Oh, H.W.; Oh, Y.; Vargas-Zambrano, J.C.; Choe, Y.J. Vaccine-Related Errors in Reconstitution in South Korea: A National Physicians’ and Nurses’ Survey. Vaccines 2021, 9, 117. [Google Scholar] [CrossRef] [PubMed]
- McDowell, S.E.; Mt-Isa, S.; Ashby, D.; Ferner, R. Where errors occur in the preparation and administration of intravenous medicines: A systematic review and Bayesian analysis. Qual. Saf. Health Care 2010, 19, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Macias, A.E.; Huertas, M.; de Leon, S.P.; Munoz, J.M.; Chavez, A.R.; Sifuentes-Osornio, J.; Romero, C.; Bobadilla, M. Contamination of intravenous fluids: A continuing cause of hospital bacteremia. Am. J. Infect. Control. 2010, 38, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Larmené-Beld, K.H.M.; Frijlink, H.W.; Taxis, K. A systematic review and meta-analysis of microbial contamination of parenteral medication prepared in a clinical versus pharmacy environment. Eur. J. Clin. Pharmacol. 2019, 75, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Olivera, I.; Grau, C.; Dibarboure, H.; Torres, J.P.; Mieres, G.; Lazarov, L.; Alvarez, F.P.; Yescas, J.G.L. Valuing the cost of improving Chilean primary vaccination: A cost minimization analysis of a hexavalent vaccine. BMC Health Serv. Res. 2020, 20, 295. [Google Scholar] [CrossRef] [PubMed]
- Mathijssen, D.A.R.; Heisen, M.; Clark-Wright, J.F.; Wolfson, L.J.; Lu, X.; Carrol, S.; van Dijk, B.C.P.; Klijn, S.L.; Alemayehu, B. Budget impact analysis of introducing a non-reconstituted, hexavalent vaccine for pediatric immunization in the United Kingdom. Expert Rev. Vaccines 2020, 19, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Romero, M.G.D.; Caicedo, M.L.; Benchabane, D.; Lopez, J.G. Cost-Minimization and Budget Impact Analysis of a Hexavalent Vaccine (Hexaxim®) in the Colombian Expanded Program on Immunization. Value Health Reg. Issues 2021, 26, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Seinfeld, J.; Rosales, M.L.; Sobrevilla, A.; Yescas, J.G.L. Economic assessment of incorporating the hexavalent vaccine as part of the National Immunization Program of Peru. BMC Health Serv. Res. 2022, 22, 651. [Google Scholar] [CrossRef] [PubMed]
- Higgins, A.M.; Harris, A. Health Economic Methods: Cost-Minimization, Cost-Effectiveness, Cost-Utility, and Cost-Benefit Evaluations. Crit. Care Clin. 2012, 28, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Health Insurance Review & Assessment Service. Healthcare Bigdata Hub. Available online: http://opendata.hira.or.kr/op/opc/olap4thDsInfo.do (accessed on 21 December 2022).
- Korean Statistical Information Service [KOSIS]. 2021 Population and Housing Census (Register-based Census). Available online: https://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1BPA004&conn_path=I3 (accessed on 15 November 2022).
- Briggs, A.; Sculpher, M.; Claxton, K. Decision Modelling for Health Economic Evaluation; Oup Oxford: Oxford, UK, 2006; pp. 85–93. [Google Scholar]
- Aljunid, S.M.; Al Bashir, L.; Ismail, A.B.; Aizuddin, A.N.; Rashid, S.A.; Nur, A.M. Economic impact of switching from partially combined vaccine “Pentaxim® and hepatitis B” to fully combined vaccine “Hexaxim®” in the Malaysian National Immunization Program. BMC Health Serv. Res. 2022, 22, 34. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Base-Case Value | Distribution for Probabilistic Simulation 1 | Source |
|---|---|---|---|
| Infection following immunization | |||
| Pentavalent | 0.001% 2 | Uniform (0.01–1%) | Base case: healthcare big data hub by HIRA (opendata.hira.or.kr) Range for probabilistic simulation: Larmené-Beld et al. (2019) [13] |
| Infection rate ratio | 0.01 3 | Uniform (0.008–0.0155) | Larmené-Beld et al. (2019) [13] |
| Ready-to-use Hexavalent | 0.00001% 4 | Infection rate of pentavalent × infection rate ratio | |
| Immunization error | |||
| Spillage risk | 1% | Beta | De Coster et al. (2015 [12]) |
| Risk to forget Hib | 1% | Beta | De Coster et al. (2015) [12] |
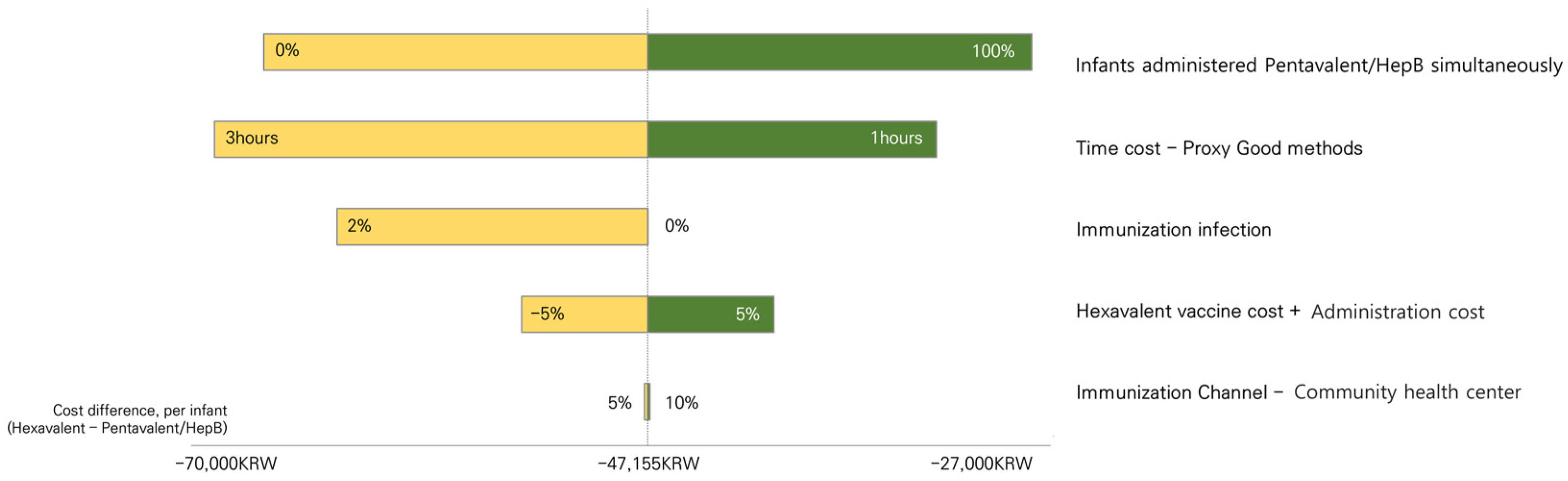
| Infants administered Pentavalent/HepB simultaneously at six months | 60% | Assumed | |
| Cost, KRW | |||
| Vaccine cost per dose | |||
| Ready-to-use Hexavalent | ₩ 42,000 | – | Assumed |
| Pentavalent | ₩ 34,990 | – | Unit cost announced by KDCA |
| HepB | ₩ 3300 | – | Unit cost announced by KDCA |
| Administration cost | |||
| Community health center 5 | ₩ 0 | ||
| Clinic/hospital | |||
| Ready-to-use Hexavalent | ₩ 48,550 | – | Assumed 6 |
| Pentavalent | ₩ 38,840 | – | Unit cost announced by KDCA |
| HepB | ₩ 19,420 | – | Unit cost announced by KDCA |
| Infection cost per case | ₩ 261,812 | Gamma | Healthcare big data hub by HIRA (opendata.hira.or.kr) |
| Immunization error cost | Gamma | Assumed one additional vaccine dose | |
| Ready-to-use Hexavalent | ₩ 42,000 | Same as a vaccine cost | |
| Pentavalent | ₩ 34,990 | Same as a vaccine cost | |
| HepB | ₩ 3300 | Same as a vaccine cost | |
| Transportation cost per visit | ₩ 8663 | Gamma | 2005 KNHANES report |
| Time cost per visit | ₩ 27,440 | – | KOSIS |
| Birth cohort (2021) | 260,500 | – | KOSIS |
| Inoculation completion rate | 97.90% | – | Unit cost announced by KDCA |
| Variable | Hexavalent | Pentavalent + HepB | Difference (Hexavalent- Pentavalent + HepB) |
|---|---|---|---|
| Cost items per infant, KRW | |||
| Vaccine cost + administration cost | ₩ 259,998 | ₩ 254,501 | ₩ 5497 |
| Infection cost following immunization | ₩ 0.084 | ₩ 8 | ₩ −8 |
| Immunization error cost | ₩ 0 | ₩ 2099 | ₩ −2099 |
| Transportation cost | ₩ 25,989 | ₩ 38,117 | ₩ −12,128 |
| Time cost | ₩ 82,320 | ₩ 120,736 | ₩ −38,416 |
| Total cost per infant, KRW | |||
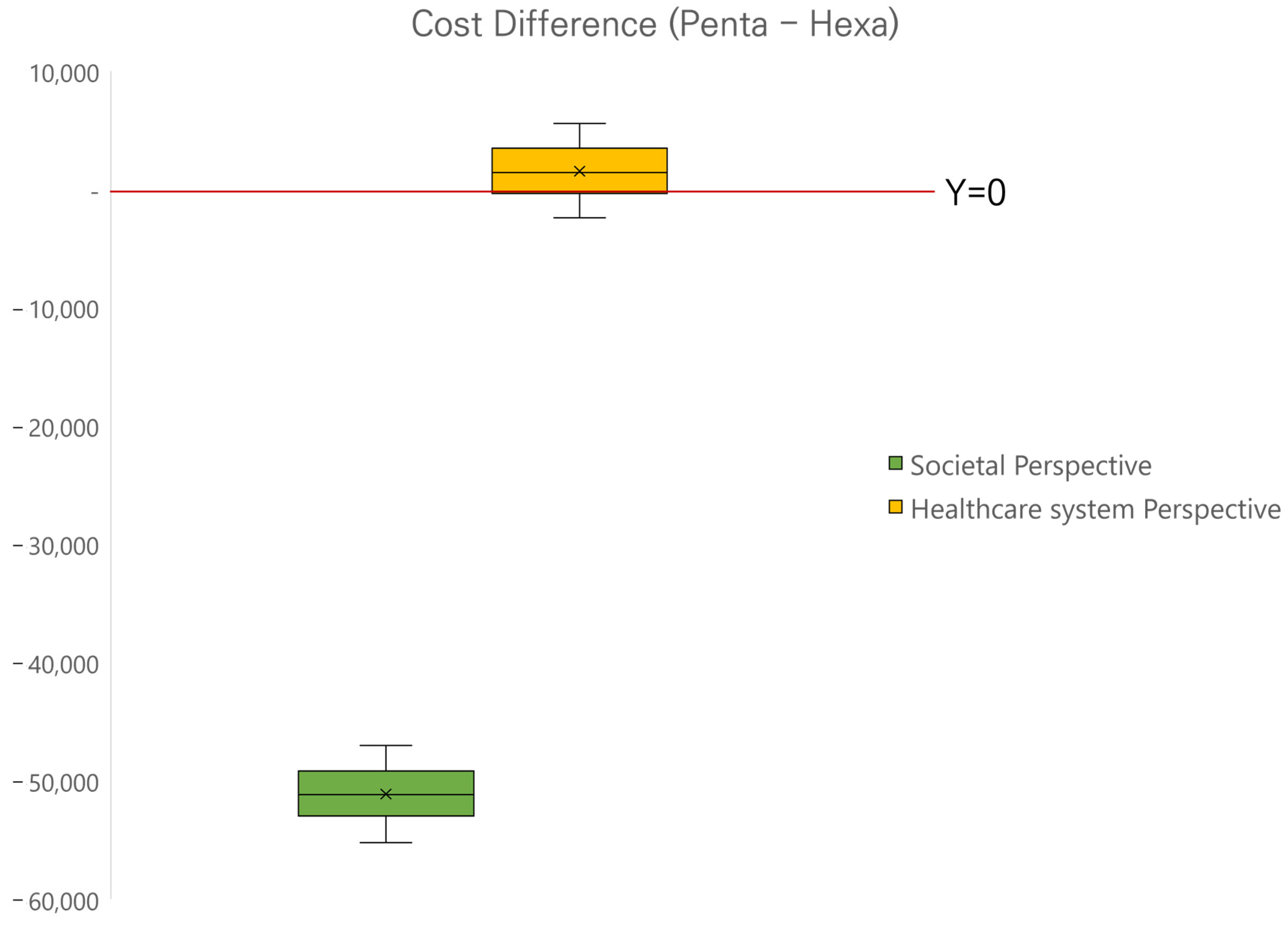
| Societal perspective | ₩ 368,307 | ₩ 415,462 | ₩ −47,155 |
| Healthcare system perspective | ₩ 259,998 | ₩ 254,509 | ₩ 5489 |
| Total cost of the birth cohort, 1 million KRW | |||
| Societal perspective | ₩ 93,929 | ₩ 105,955 | ₩ −12,026 |
| Healthcare system perspective | ₩ 66,307 | ₩ 64,907 | ₩ 1400 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Min, S.; Kwon, S.-H.; Lee, Y.-W.; Lee, J.-M.; Bae, E.J.; Lee, E.-K. Estimating the Total Societal Cost of a Hexavalent Vaccine versus a Pentavalent Vaccine with Hepatitis B in South Korea. Vaccines 2023, 11, 984. https://doi.org/10.3390/vaccines11050984
Min S, Kwon S-H, Lee Y-W, Lee J-M, Bae EJ, Lee E-K. Estimating the Total Societal Cost of a Hexavalent Vaccine versus a Pentavalent Vaccine with Hepatitis B in South Korea. Vaccines. 2023; 11(5):984. https://doi.org/10.3390/vaccines11050984
Chicago/Turabian StyleMin, Serim, Sun-Hong Kwon, Yeon-Woo Lee, Jung-Min Lee, Eun Jin Bae, and Eui-Kyung Lee. 2023. "Estimating the Total Societal Cost of a Hexavalent Vaccine versus a Pentavalent Vaccine with Hepatitis B in South Korea" Vaccines 11, no. 5: 984. https://doi.org/10.3390/vaccines11050984