
COVID-19 Vaccination in the WHO African Region: Progress Made in 2022 and Factors Associated

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Sources and Measurement
2.3. Data Analysis
- (a)
- Vaccine uptake and coverage cumulatively and during the years 2021 and 2022.
- Percentage of doses administered over received: The cumulative doses administered was divided by the cumulative doses received and multiplied by 100.
- Percentage of doses expired over received: The cumulative doses expired was divided by the cumulative doses received and multiplied by 100.
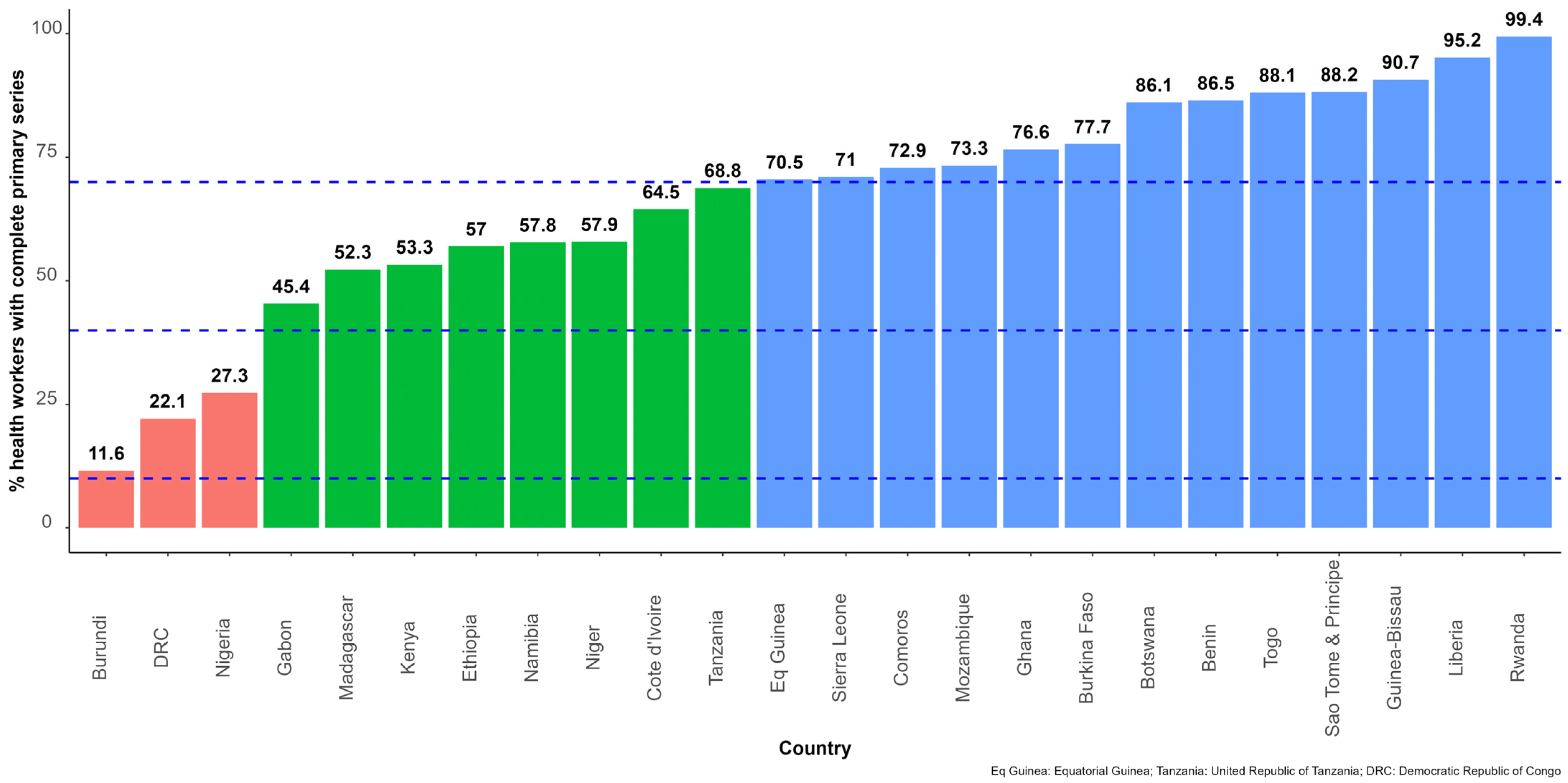
- Percentage of people who had completed the primary vaccination series ((initial number of doses of a particular vaccine that a person needs), i.e., one dose of the Janssen vaccine or two doses of other vaccines [11]) in the general population and in high-priority risk groups (using healthcare workers as a tracer): The cumulative number of people having completed the primary series was divided by the general population or the population size of the related high-risk group, and multiplied by 100. Booster doses were not included in the primary series definition [11].
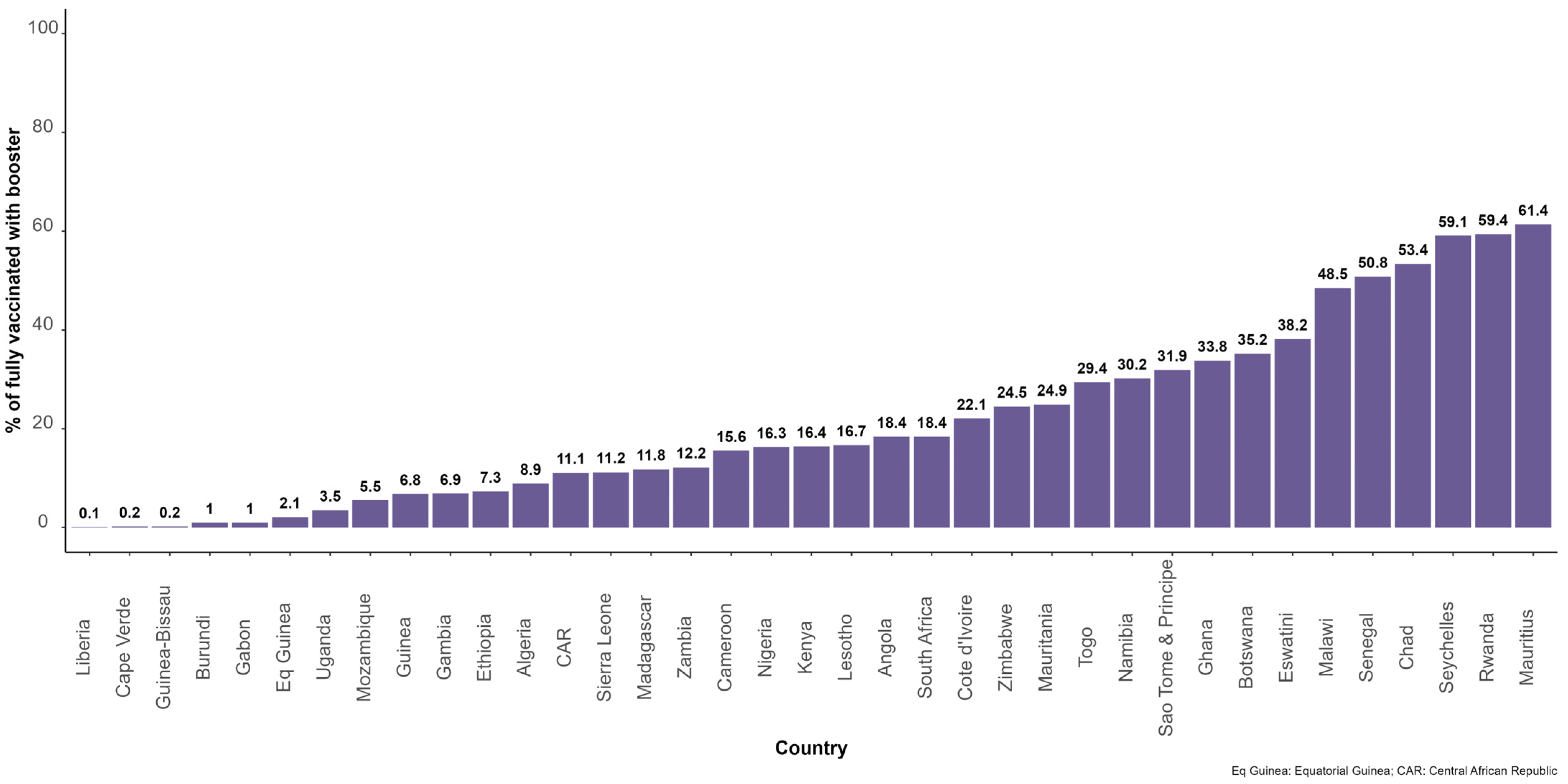
- Percentage of people who have completed the primary series and received at least one booster dose: The cumulative number of people who received the first dose of booster was divided by the number of people who have completed the primary series and multiplied by 100.
- (b)
- Multivariable analysis of factors associated with COVID-19 vaccination coverage in 2022.
3. Results
3.1. COVID-19 Vaccines Doses Received and Administered
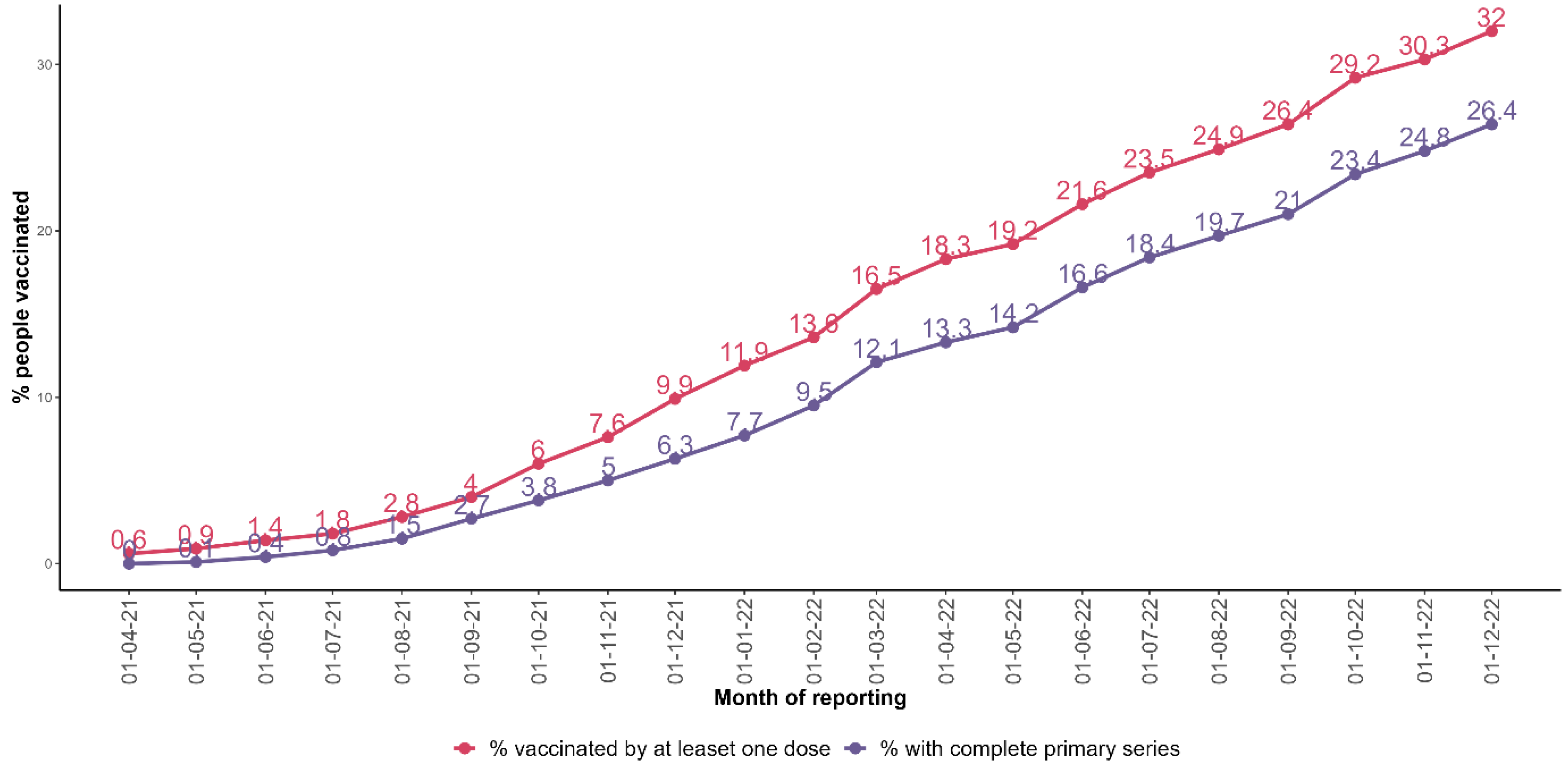
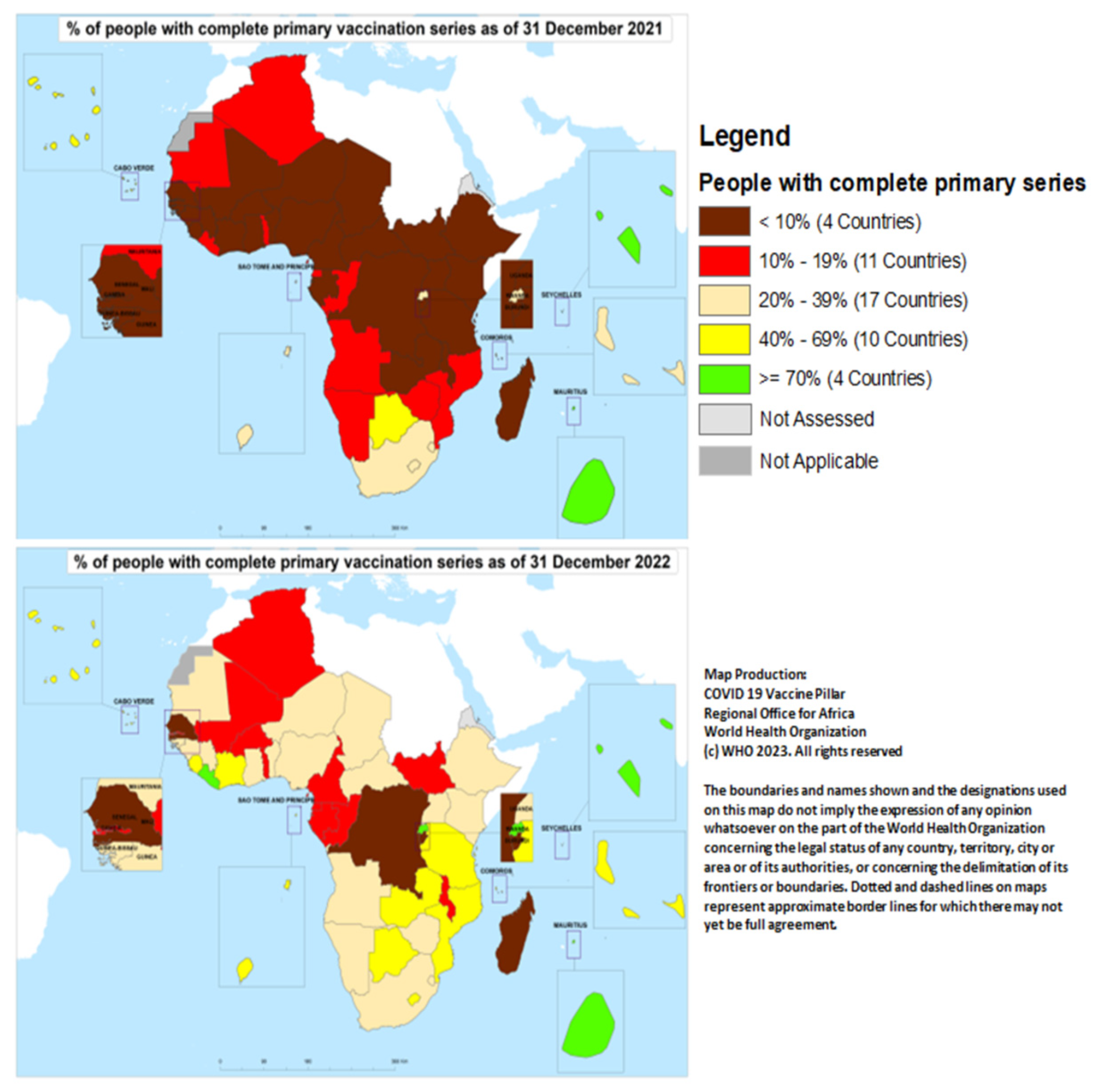
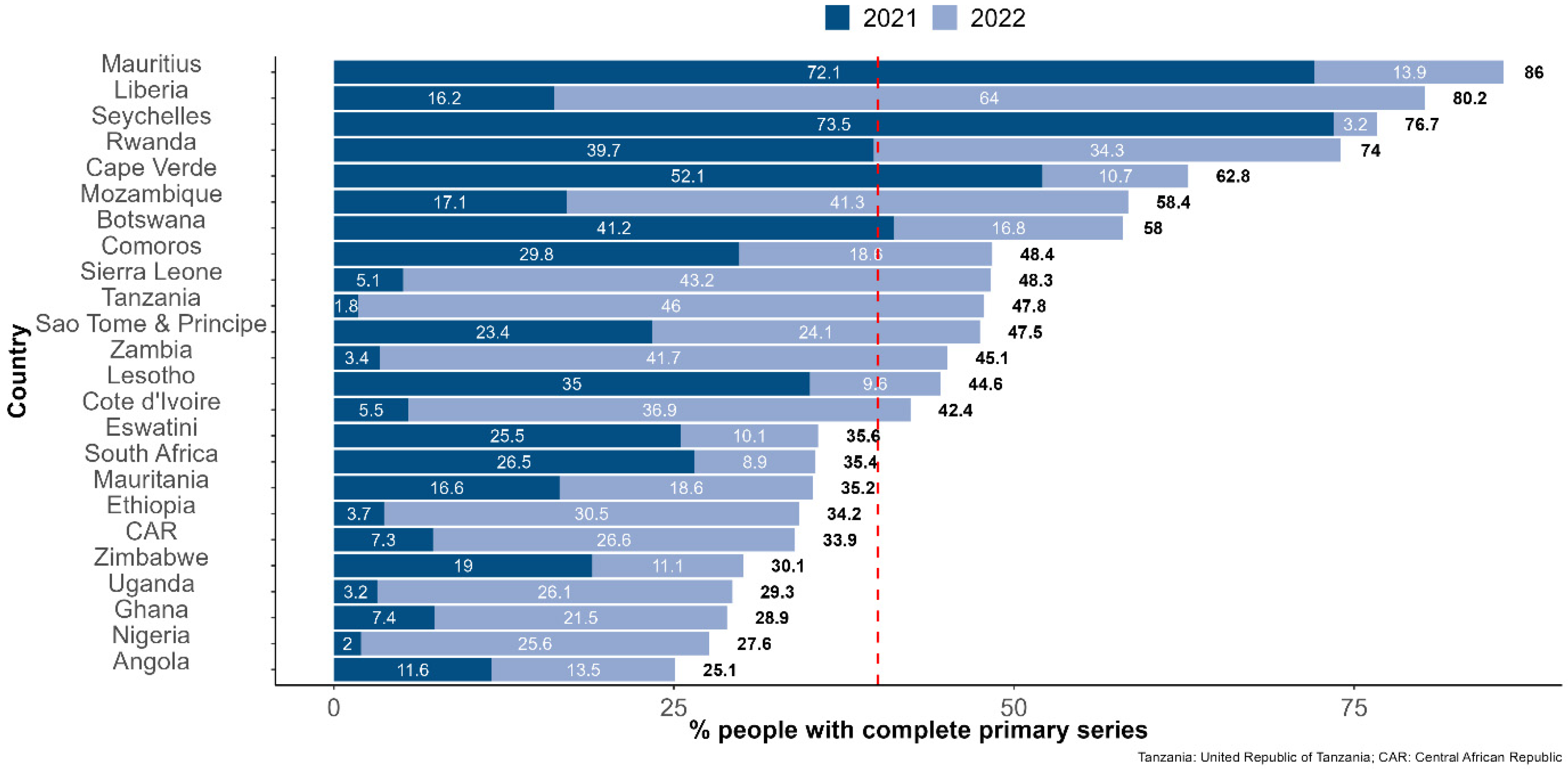
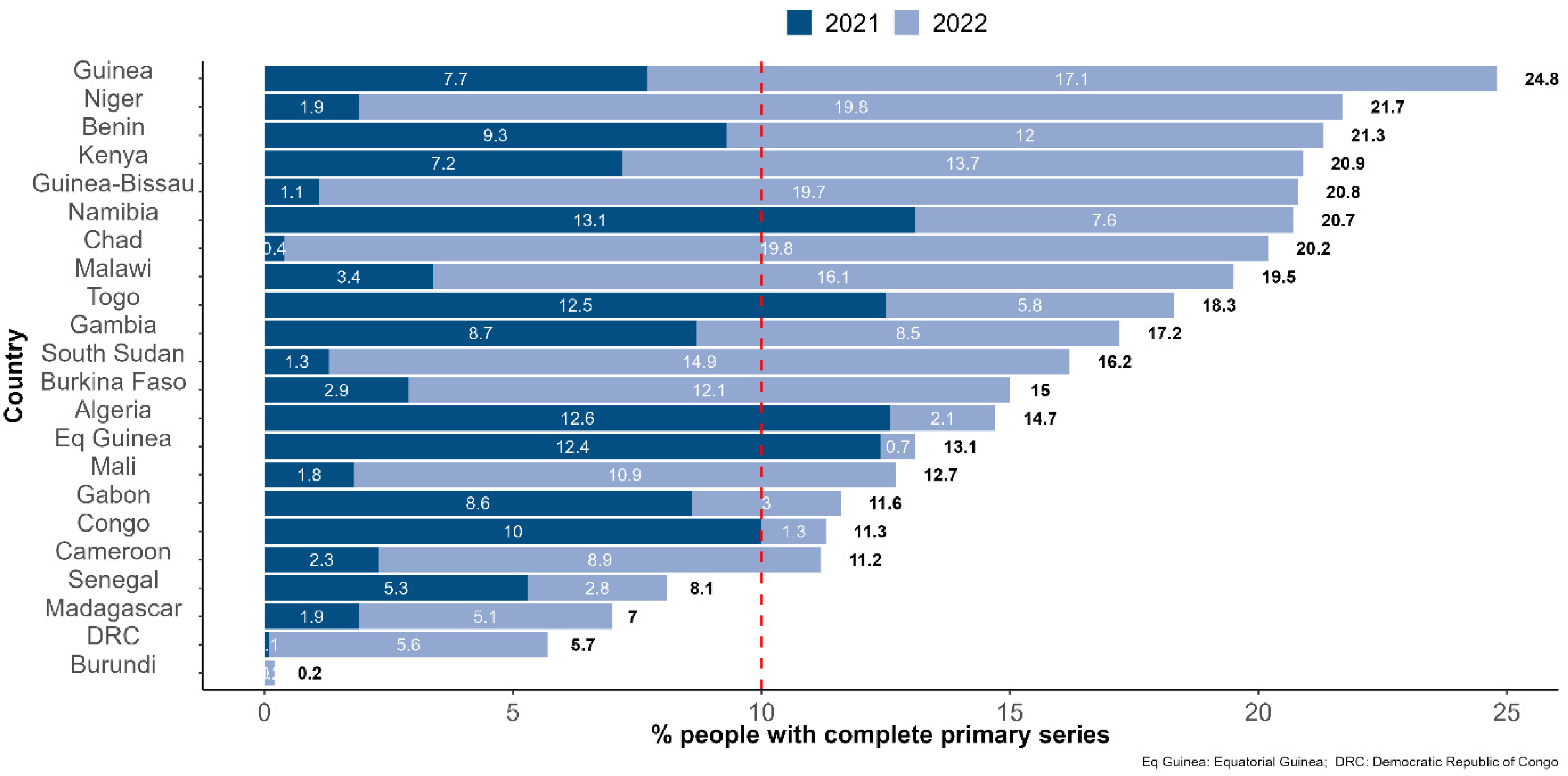
3.2. COVID-19 Vaccination Coverage
3.3. Factors Associated with Vaccine Coverage in 2022
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The American Journal of Managed Care. A Timeline of COVID-19 Developments in 2020. AJMC, 2021. Available online: https://www.ajmc.com/view/a-timeline-of-covid19-developments-in-2020 (accessed on 1 February 2023).
- World Health Organization. Strategic Preparedness, Readiness and Response Plan to End the Global COVID-19 Emergency in 2022. Available online: https://www.who.int/publications/i/item/WHO-WHE-SPP-2022.1 (accessed on 15 January 2023).
- World Health Organization. WHO Issues Its First Emergency Use Validation for a COVID-19 Vaccine and Emphasizes Need for Equitable Global Access. Available online: https://www.who.int/news/item/31-12-2020-who-issues-its-first-emergency-use-validation-for-a-covid-19-vaccine-and-emphasizes-need-for-equitable-global-access (accessed on 1 February 2022).
- Verbele, R.; Lentacker, I.; De Smedt, S.C.; Dewitte, H. The dawn of mRNA vaccines: The COVID-19 case. J. Control. Release 2021, 333, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst. Rev. 2022, 12, CD015477. [Google Scholar] [CrossRef]
- World Health Organization. WHO SAGE Roadmap for Prioritizing Uses of COVID-19 Vaccine. Available online: https://apps.who.int/iris/handle/10665/351138 (accessed on 1 February 2023).
- World Health Organization. About WHO: Regional Office for Africa. Available online: https://www.afro.who.int/countries (accessed on 1 February 2023).
- Vilches, T.N.; SAH, P.; Abdollahi, E.; Moghadas, S.M.; Galvani, A.P. Importance of non-pharmaceutical interventions in the COVID-19 vaccination era: A case study of the Seychelles. J. Glob. Health 2021, 11, 03104. [Google Scholar] [CrossRef]
- Impouma, B.; Mboussou, F.; Farham, B.; Makubalo, L.; Mwinga, K.; Onyango, A.; Sthreshley, L.; Akpaka, K.; Balde, T.; Atuhebwe, P.; et al. COVID-19 vaccination rollout in the World Health Organization African region: Status at end June 2022 and way forward. Epidemiol. Infect. 2022, 150, e143. [Google Scholar] [CrossRef]
- World Health Organization. Strategy to Achieve Global COVID-29 Vaccination by Mid-2022. Available online: https://www.who.int/publications/m/item/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022 (accessed on 1 February 2023).
- Rosen, B.; Waitzberg, R.; Israeli, A. Israel’s rapid rollout of vaccinations for COVID-19. Isr. J. Health Policy Res. 2021, 10, 6. [Google Scholar] [CrossRef]
- Antonini, M.; Eid, M.A.; Falkenbach, M.; Rosenbluth, S.T.; Prieto, P.A.; Brammli-Greenberg, S.; McMeekin, P.; Paolucci, F. An analysis of the COVID-19 vaccination campaigns in France, Israel, Italy and Spain and their impact on health and economic outcomes. Health Policy Technol. 2022, 11, 100594. [Google Scholar] [CrossRef]
- Falkenbach, M.; Willison, C. Resources or trust: What matters more in the vaccination strategies of high-income liberal democracies? Health Policy Technol. 2022, 11, 100618. [Google Scholar] [CrossRef]
- World Health Organization. The International Health Regulation. Available online: https://www.who.int/publications/i/item/9789241580496 (accessed on 1 February 2023).
- Kasolo, F.; Zabulon, Y.; Bakyaita, M.; Guturuku, P.; Katz, R.; Fischer, J.E.; Perry, H.N. IDSR as a platform for implementing IHR in African countries. Biosecur. Bioterror. 2013, 11, 163–169. [Google Scholar] [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, W.D. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. Available online: https://scfbm.biomedcentral.com/articles/10.1186/1751-0473-3-17 (accessed on 1 February 2023). [CrossRef]
- R Core Team. The R Project for Statistical Computing. Available online: https://www.r-project.org (accessed on 1 February 2023).
- ESRI. ArcGIS: The Mapping and Analytics Platform. Available online: https://www.esri.com/en-us/arcgis/about-arcgis/overview (accessed on 1 February 2023).
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 1 February 2023).
- Hassan, M.A.; Bala, A.A.; Jatau, A.I. Low rate of COVID-19 vaccination in Africa: A cause for concern. Ther. Adv. Vaccines Immunother. 2022, 10, 25151355221088159. [Google Scholar] [CrossRef]
- Al Hasan, S.M.; Saulam, J.; Mikami, F.; Kanda, K.; Yokoi, H.; Hirao, T. COVID-19 outbreak trends in South Africa: A comparison of Omicron (B.1.1.529), Delta (B.1.617.2), and Beta (B.1.351) variants outbreak periods. J. Infect. Public Health 2022, 15, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Lawal, L.; Bello, M.A.; Murwira, T.; Avoka, C.; Ma’Aruf, S.Y.; Omonhinmin, I.H.; Maluleke, P.; Tsagkaris, C.; Onyeaka, H. Low coverage of COVID-19 vaccines in Africa: Current evidence and the way forward. Hum. Vaccin Immunother. 2022, 18, 2034457. [Google Scholar] [CrossRef]
- Tagoe, E.T.; Sheikh, N.; Morton, A.; Nonvignon, J.; Sarker, A.R.; Williams, L.; Megiddo, I. COVID-19 vaccination in Lower Middle income countries: National stakeholders views on challenges. Public Health 2021, 9, 709127. [Google Scholar] [CrossRef]
- Grabenstein, J.D.; Nevin, R.L. Mass Immunization Programs: Principles and Standards. Curr. Top. Microbiol. Immunol. 2006, 304, 31–51. [Google Scholar] [CrossRef]
- Olu-Abiodun, O.; AbiodunID, O.; Okafor, N. COVID-19 vaccination in Nigeria: A rapid review of vaccine acceptance rate and the associated factors. PLoS ONE 2022, 11, e0267691. [Google Scholar] [CrossRef]
- Msuya, S.E.; Manongi, R.N.; Jonas, N.; Mtei, M.; Amour, C.; Mgongo, M.B.; Bilakwate, J.S.; Amour, M.; Kalolo, A.; Kapologwe, N.; et al. COVID-19 Vaccine Uptake and Associated Factors in Sub-Saharan Africa: Evidence from a Community-Based Survey in Tanzania. Vaccines 2023, 11, 465. [Google Scholar] [CrossRef]
- Njoga, E.O.; Awoyomi, O.J.; Onwumere-Idolor, O.S.; Awoyomi, P.O.; Ugochukwu, I.C.I.; Ozioko, S.N. Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out—COVID-19 Vaccination Acceptance Rates as Case-in-Point. Vaccines 2022, 10, 1934. [Google Scholar] [CrossRef]
- Kabakama, S.; Konje, E.T.; Dinga, J.N.; Kishamawe, C.; Morhason-Bello, I.; Hayombe, P.; Adeyemi, O.; Chimuka, E.; Lumu, I.; Amuasi, J.; et al. Commentary on COVID-19 Vaccine Hesitancy in sub-Saharan Africa. Trop. Med. Infect. Dis. 2022, 7, 130. [Google Scholar] [CrossRef]
- The Humanitarian Data Exchange. World Bank and Gavi Vaccine Financing. Available online: https://data.humdata.org/dataset/world-bank-and-gavi-vaccine-financing? (accessed on 5 February 2023).
- Idris, I.O.; Ayeni, G.O.; Adebisi, Y.A. Why Many African countries may not achieve the 2022 COVID-19 vaccination coverage target. Trop. Med. Health 2022, 50, 15. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Karim, S.S.A.; van Selm, L.; Doran, J.; Batista, C.; Ben Amor, Y.; Hellard, M.; Kim, B.; Kopka, C.J.; Yadav, P. COVID-19 vaccine wastage in the midst of vaccine inequity: Causes, types and practical steps. BMJ Glob. Health 2022, 7, e009010. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Joint Statement on Dose Donations of COVID-19 Vaccines to African Countries. Available online: https://www.who.int/news/item/29-11-2021-joint-statement-on-dose-donations-of-covid-19-vaccines-to-african-countries (accessed on 1 March 2023).
- Fall, A.; Eldesouki, R.E.; Sachithanandham, J.; Morris, C.P.; Norton, J.M.; Gaston, D.C.; Forman, M.; Abdullah, O.; Gallagher, N.; Li, M.; et al. A Quick Displacement of the SARS-CoV-2 variant Delta with Omicron: Unprecedented Spike in COVID-19 Cases Associated with Fewer Admissions and Comparable Upper Respiratory Viral Loads. medRxiv, 2022; preprint. [Google Scholar] [CrossRef]
- Hamimes, A.; Aouissi, H.A.; Ababsa, M.; Lounis, M.; Jayarajah, U.; Napoli, C.; Kasemy, Z.A. The Effect of Preventive Measures and Vaccination against SARS-CoV-2 on the Infection Risk, Treatment, and Hospitalization: A Cross-Sectional Study of Algeria. Viruses 2022, 14, 2771. [Google Scholar] [CrossRef]
- Makomi, M. Tanzania refuses COVID-19 vaccines. Lancet 2021, 397, 566. [Google Scholar] [CrossRef]
- World Bank. Learning from Burundi’s Political Pivot on COVID-19 Vaccines. Available online: https://blogs.worldbank.org/nasikiliza/learning-burundis-political-pivot-covid-19-vaccines (accessed on 1 February 2023).
- Olayinka, F.; Sauer, M.; Menning, L.; Summers, D.; Wonodi, C.; Mackay, S.; MacDonald, N.E.; Figueroa, J.P.; Andriamitantsoa, B.; Bonsu, G.; et al. Building and sustaining public and political commitment to the value of vaccination: Recommendations for the Immunization Agenda 2030 (Strategic Priority Area 2). Vaccine, 2022; in press. [Google Scholar] [CrossRef]
- Wells, C.R.; Galvani, A.P. The global impact of disproportionate vaccination coverage on COVID-19 mortality. Lancet Infect. Dis. 2022, 22, 1254–1255. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Weekly Epidemiological Update on COVID-19—28 December 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---28-december-2021 (accessed on 1 February 2023).
- Owen, D. COVID-19: Winter surge feared as China lurches away from zero covid. BMJ 2022, 379, o2983. [Google Scholar] [CrossRef]
- Chisale, M.R.O.; Ramazanu, S.; Mwale, S.E.; Kumwenda, P.; Chipeta, M.; Kaminga, A.C.; Nkhata, O.; Nyambalo, B.; Chavura, E.; Mbakaya, B.C. Seroprevalence of anti-SARS-CoV-2 antibodies in Africa: A systematic review and meta-analysis. Rev. Med. Virol. 2022, 32, e2271. [Google Scholar] [CrossRef]
- World Health Organization: Global COVID-19 Vaccination Strategy in a Changing World: July 2022 Update. Available online: https://www.who.int/publications/m/item/global-covid-19-vaccination-strategy-in-a-changing-world--july-2022-update (accessed on 1 February 2023).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Explanatory Variables | Mean ± sd or n (%) | Crude Beta Coefficient | Adjusted Beta Coefficient (Final Model) | ||||
|---|---|---|---|---|---|---|---|
| Value | 95% CI | p | Value | 95% CI | p | ||
| Population (million) | 264.5 ± 390.7 | 0.0002 | [−0.0003; 0.0009] | 0.50 | |||
| Income classification (Middle income) | 24 (54.5%) | −0.32 | [−0.80; −0.15] | 0.18 | −0.0026 | [−0.039; 0.34] | 0.89 |
| UHC service coverage index | 46.5 ± 10.0 | −0.015 | [−0.04; 0.012] | 0.23 | |||
| Number of cases per million population in 2022 | 3745 ± 9125 | −9.14 × 10−6 | [−3.25 × 10−5; 2.04 × 10−5] | 0.50 | |||
| Number of deaths per million population in 2022 | 231.0 ± 414.1 | −0.0005 | [−0.001; 0.0001] | 0.11 | −0.00042 | [−0.00054; 0.00048] | 0.86 |
| % of people with complete primary series who received Janssen vaccine | 51.63 ± 33.16 | 0.004 | [−0.004; 0.011] | 0.32 | |||
| MP–CST country (Yes) | 19 (43.18%) | 0.47 | [0.004; 0.94] | 0.049 | −0.0078 | [−0.47; 0.314] | 0.69 |
| Days of expertise provided by WHO AFRO | 263 ± 376 | 0.0002 | [−0.0005; 0.0009] | 0.57 | |||
| Implemented at least one high volume mass vaccination campaign (Yes) | 18 (40.91%) | 1.03 | [0.66; 1.41] | <0.001 | 0.91 | [0.52; 1.31] | <0.0001 |
| WHO funding spent per people vaccinated (complete primary series) in USD | 0.88 ± 2.08 | −0.35 | [−0.59; −0.16] | 0.001 | −0.26 | [−0.46; −0.11] | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mboussou, F.; Farham, B.; Nsasiirwe, S.; Atagbaza, A.; Oyaole, D.; Atuhebwe, P.L.; Alegana, V.; Osei-sarpong, F.; Bwaka, A.; Paluku, G.; et al. COVID-19 Vaccination in the WHO African Region: Progress Made in 2022 and Factors Associated. Vaccines 2023, 11, 1010. https://doi.org/10.3390/vaccines11051010
Mboussou F, Farham B, Nsasiirwe S, Atagbaza A, Oyaole D, Atuhebwe PL, Alegana V, Osei-sarpong F, Bwaka A, Paluku G, et al. COVID-19 Vaccination in the WHO African Region: Progress Made in 2022 and Factors Associated. Vaccines. 2023; 11(5):1010. https://doi.org/10.3390/vaccines11051010
Chicago/Turabian StyleMboussou, Franck, Bridget Farham, Sheillah Nsasiirwe, Ajiri Atagbaza, Daniel Oyaole, Phionah Lynn Atuhebwe, Victor Alegana, Fred Osei-sarpong, Ado Bwaka, Gilson Paluku, and et al. 2023. "COVID-19 Vaccination in the WHO African Region: Progress Made in 2022 and Factors Associated" Vaccines 11, no. 5: 1010. https://doi.org/10.3390/vaccines11051010