
Flattening the Curve after the Initial Outbreak of Coronavirus Disease 2019: A Data-Driven Modeling Analysis for the Omicron Pandemic in China

Abstract
:1. Introduction
2. Methods
2.1. SARS-CoV-2 Omicron Transmission, Vaccination Rate, and Disease Burden
2.2. Mitigation with Vaccination, Antiviral Therapies, and NPIs
3. Statistical Analysis
4. Data Availability and Code Availability
5. Results
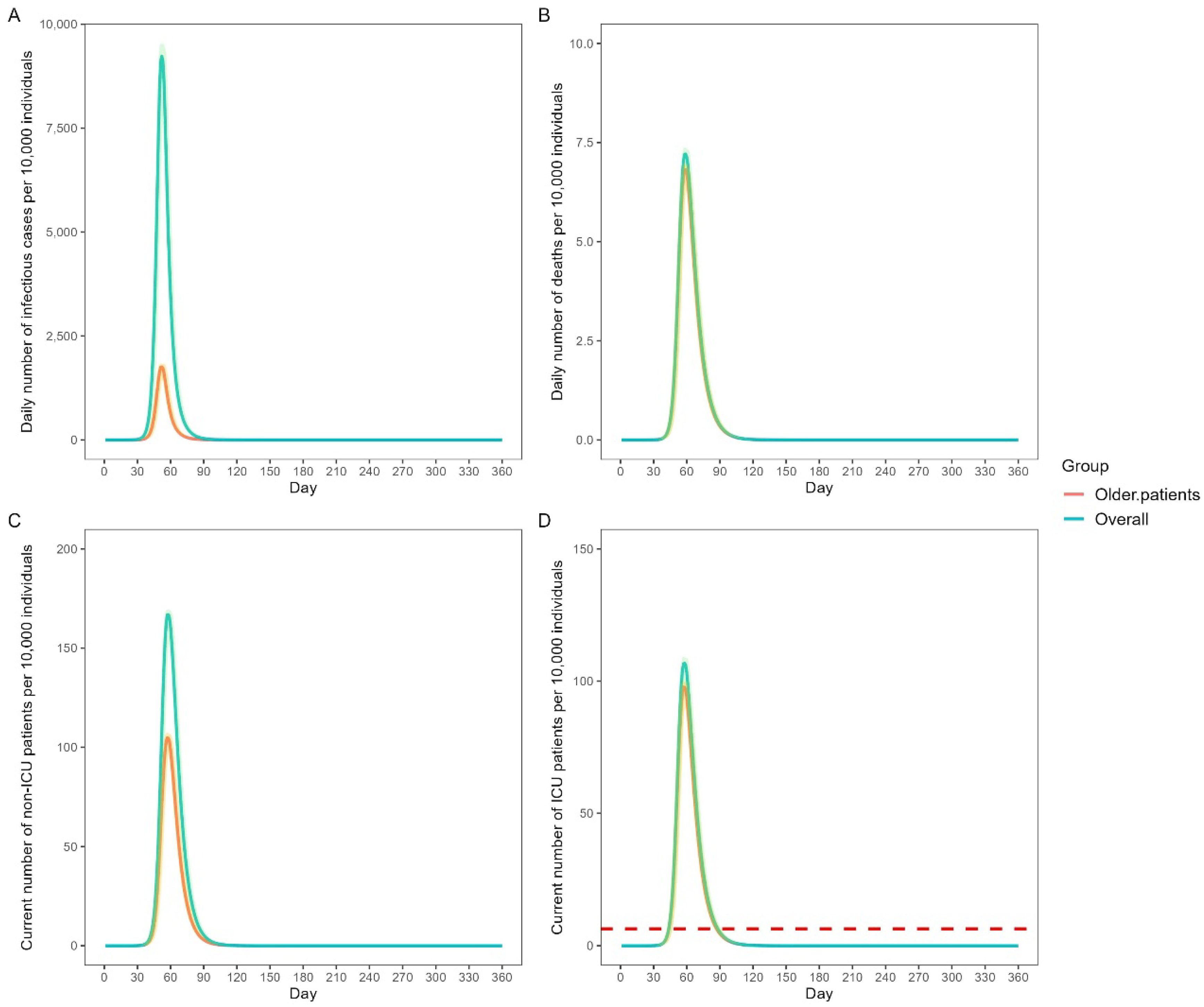
5.1. Baseline Scenario
5.2. Classification of the Stringency of NPIs
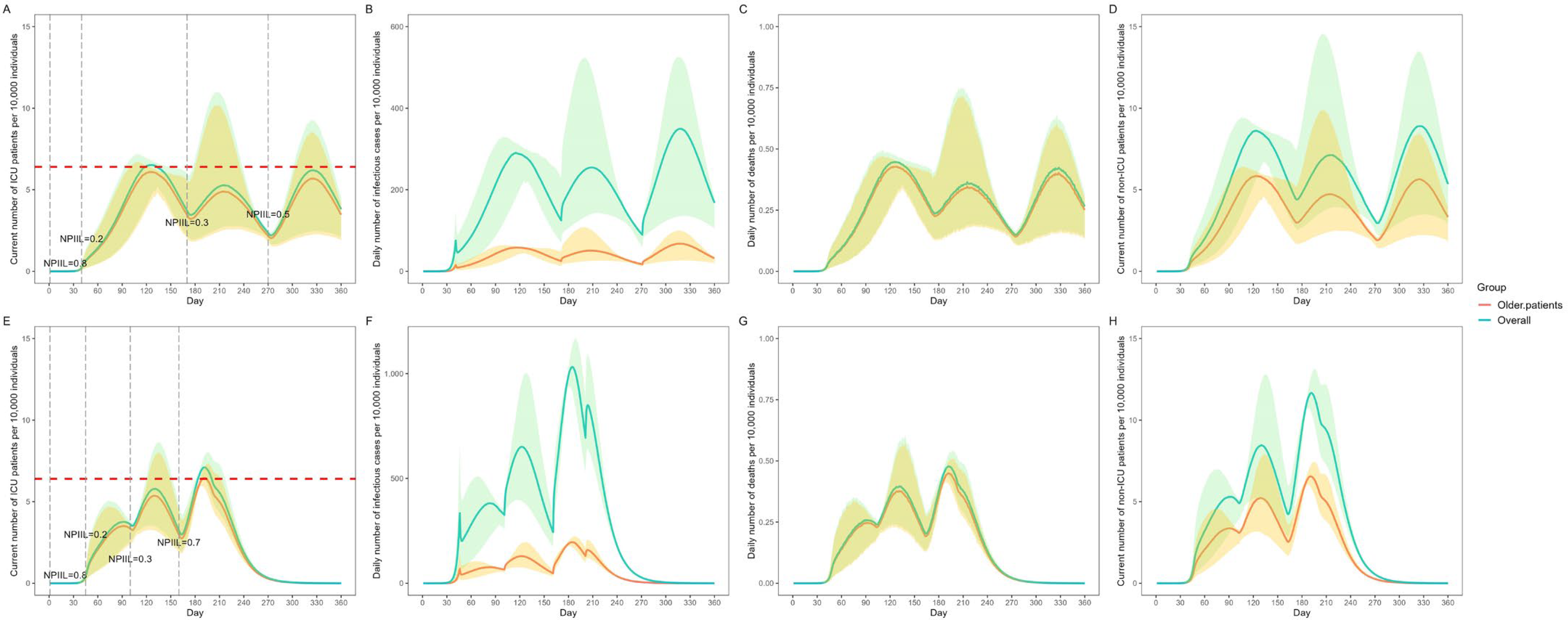
5.3. Impact of NPI Mitigation Strategies
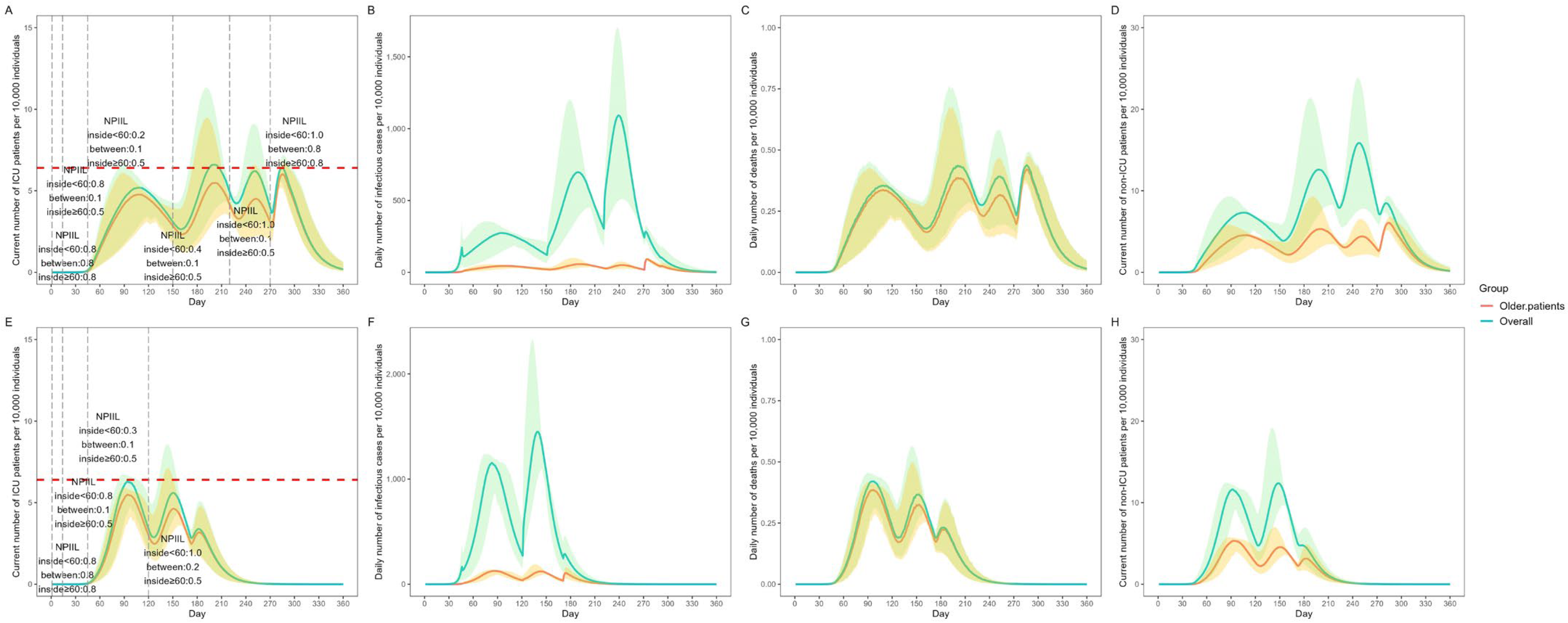
5.4. Impact of NPI Mitigation Strategies by Age
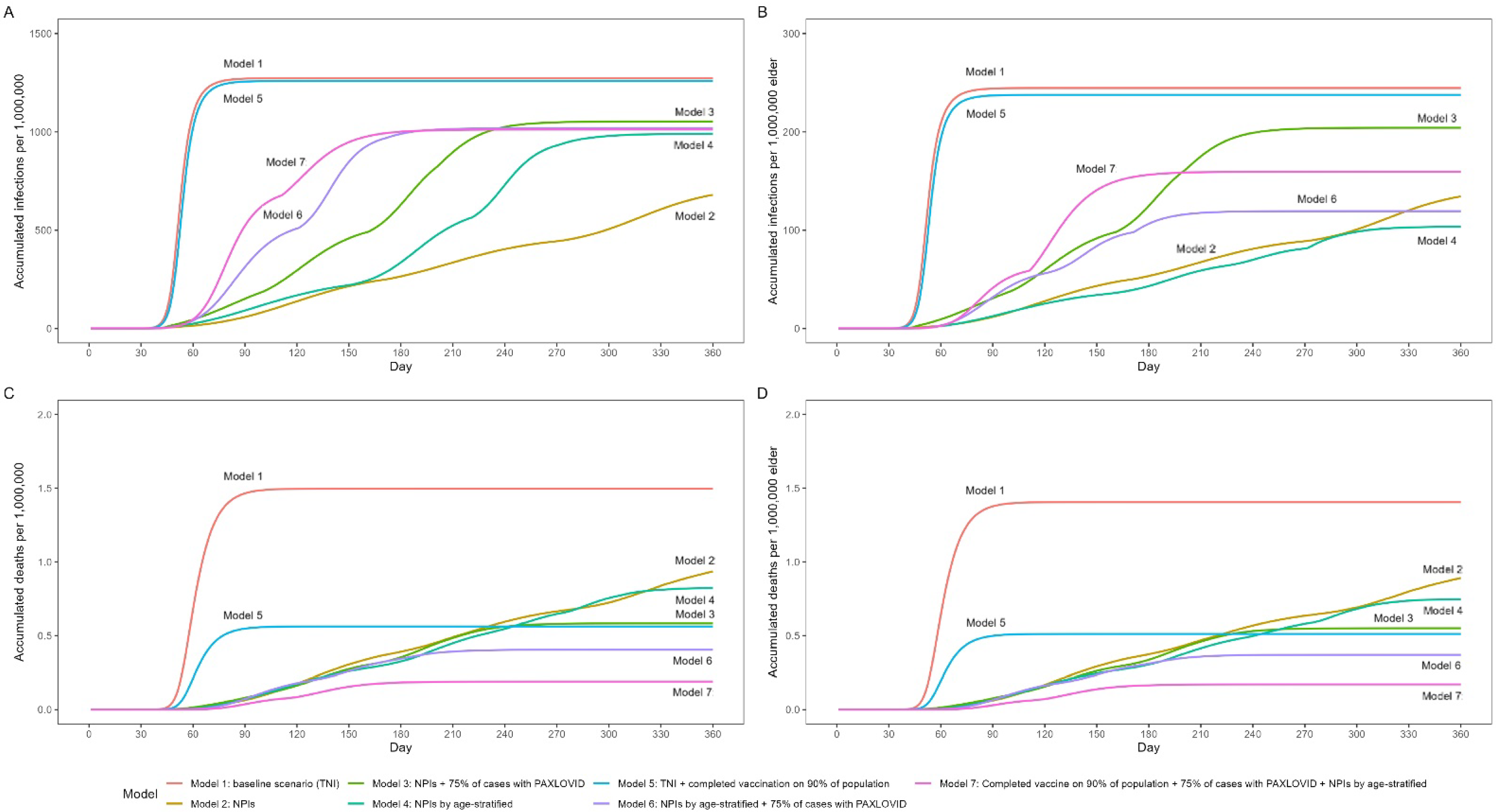
5.5. Comparison of the Outcomes of Different Strategies
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cosar, B.; Karagulleoglu, Z.Y.; Unal, S.; Ince, A.T.; Uncuoglu, D.B.; Tuncer, G.; Kilinc, B.R.; Ozkan, Y.E.; Ozkoc, H.C.; Demir, I.N.; et al. SARS-CoV-2 mutations and their viral variants. Cytokine Growth Factor Rev. 2022, 63, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef]
- Graham, F. Daily briefing: “Out of control” Omicron threatens China. Nature Briefing, 28 March 2022. [Google Scholar]
- Suzuki, R.; Yamasoba, D.; Kimura, I.; Wang, L.; Kishimoto, M.; Ito, J.; Morioka, Y.; Nao, N.; Nasser, H.; Uriu, K.; et al. Attenuated fusogenicity and pathogenicity of SARS-CoV-2 Omicron variant. Nature 2022, 603, 700–705. [Google Scholar] [CrossRef]
- Zhang, J.; Chen, N.; Zhao, D.; Zhang, J.; Hu, Z.; Tao, Z. Clinical characteristics of COVID-19 patients infected by the Omicron variant of SARS-CoV-2. Front. Med. 2022, 9, 912367. [Google Scholar] [CrossRef] [PubMed]
- Linas, B.P.; Xiao, J.; Dalgic, O.O.; Mueller, P.P.; Adee, M.; Aaron, A.; Ayer, T.; Chhatwal, J. Projecting COVID-19 Mortality as States Relax Nonpharmacologic Interventions. JAMA Health Forum 2022, 3, e220760. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.F.; Wu, X.; Li, Y.; Bian, J.; Li, K.; Jiang, Y.; Lu, Z.; Zhang, B.; Yang, C.; Sun, C.; et al. Impact of combination preventative interventions on hospitalization and death under the pandemic of SARS-CoV-2 Omicron variant in China. J. Med. Virol. 2022, 95, e28335. [Google Scholar] [CrossRef]
- Liu, J.; Liu, M.; Liang, W.N. Perspectives: The dynamic COVID-zero strategy in China. China CDC Wkly. 2022, 4, 74–75. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, K.; Feng, Z.; Yi, L.; Wu, Y.; Liu, H.; Wang, Q.; Ajelli, M.; Viboud, C.; Yu, H. Assessing the feasibility of sustaining SARS-CoV-2 local containment in China in the era of highly transmissible variants. BMC Med. 2022, 20, 442. [Google Scholar] [CrossRef]
- Cai, J.; Deng, X.; Yang, J.; Sun, K.; Liu, H.; Chen, Z.; Peng, C.; Chen, X.; Wu, Q.; Zou, J. Modeling transmission of SARS-CoV-2 Omicron in China. Nat. Med. 2022, 28, 1468–1475. [Google Scholar] [CrossRef]
- Kenyon, C. Flattening-the-curve associated with reduced COVID-19 case fatality rates- an ecological analysis of 65 countries. J. Infect. 2020, 81, e98–e99. [Google Scholar] [CrossRef]
- Strålin, K.; Wahlström, E.; Walther, S.; Bennet-Bark, A.M.; Heurgren, M.; Lindén, T.; Holm, J.; Hanberger, H. Mortality in hospitalized COVID-19 patients was associated with the COVID-19 admission rate during the first year of the pandemic in Sweden. Infect. Dis. 2022, 54, 145–151. [Google Scholar] [CrossRef]
- Dai, M.-Y.; Chen, Z.; Leng, Y.; Wu, M.; Liu, Y.; Zhou, F.; Ming, C.; Shao, N.; Liu, M.; Cai, H. Patients with Lung Cancer Have High Susceptibility of COVID-19: A Retrospective Study in Wuhan, China. Cancer Control 2020, 27, 1073274820960467. [Google Scholar] [CrossRef]
- Liu, M.; Chen, Z.; Dai, M.; Yang, J.; Chen, X.; Chen, D.; You, H.; Guo, X.; Leng, Y.; Yu, L.; et al. Lessons learned from early compassionate use of convalescent plasma on critically ill patients with COVID-19. Transfusion 2020, 60, 2210–2216. [Google Scholar] [CrossRef]
- Leng, Y.; Chen, M.; Dai, M.; Wu, Y.; Lei, S.; Yan, K.; Shao, N.; Xia, Z.; Liu, M. Minimized glycemic fluctuation decreases the risk of severe illness and death in patients with COVID-19. J. Med. Virol. 2021, 93, 4060–4062. [Google Scholar] [CrossRef]
- Zhao, L.; Li, Y.; Yi, W.; Yan, K.; Yang, C.; Radhakrishnan, S.; Li, R.; Tan, R.; Fan, G.; Dai, M.; et al. The clinical and bioinformatics analysis for the role of antihypertension drugs on mortality among patients with hypertension hospitalized with COVID-19. J. Med. Virol. 2022, 94, 4727–4734. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Li, X.; Zhang, L.; Wan, S.; Zhang, L.; Zhou, F. SARS-CoV-2 Omicron variant: Recent progress and future perspectives. Signal Transduct. Target. Ther. 2022, 7, 141. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Liu, S.; Cui, T.; Li, J.; Zhu, F.; Zhong, N.; Huang, W.; Zhao, Z.; Wang, Z. Heterologous booster with inhaled adenovirus vector COVID-19 vaccine generated more neutralizing antibodies against different SARS-CoV-2 variants. Emerg. Microbes Infect. 2022, 11, 2689–2697. [Google Scholar] [CrossRef] [PubMed]
- China Health Statistics Yearbook. Available online: http://www.stats.gov.cn/tjsj/ndsj/2021/indexeh.htm (accessed on 3 September 2021).
- Available online: http://www.nhc.gov.cn/yzygj/s7653p/202203/a354cb3151b74cfdbac6b2e909f311e6.shtml (accessed on 3 March 2022).
- Available online: https://www.moh.gov.sg/covid-19/statistics (accessed on 1 December 2022).
- Stuart, A.S.V.; Shaw, R.H.; Liu, X.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Immunogenicity, safety, and reactogenicity of heterologous COVID-19 primary vaccination incorporating mRNA, viral-vector, and protein-adjuvant vaccines in the UK (Com-COV2): A single-blind, randomised, phase 2, non-inferiority trial. Lancet 2022, 399, 36–49. [Google Scholar] [CrossRef]
- Chalkias, S.; Harper, C.; Vrbicky, K.; Walsh, S.R.; Essink, B.; Brosz, A.; McGhee, N.; Tomassini, J.E.; Chen, X.; Chang, Y.; et al. A Bivalent Omicron-Containing Booster Vaccine against COVID-19. N. Engl. J. Med. 2022, 387, 1279–1291. [Google Scholar] [CrossRef]
- Cheng, Z.J.; Zhan, Z.; Xue, M.; Zheng, P.; Lyu, J.; Ma, J.; Zhang, X.D.; Luo, W.; Huang, H.; Zhang, Y.; et al. Public Health Measures and the Control of COVID-19 in China. Clin. Rev. Allergy Immunol. 2021, 64, 1–16. [Google Scholar] [CrossRef]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Fang, Z.; Monteiro, V.S.; Hahn, A.M.; Grubaugh, N.D.; Lucas, C.; Chen, S. Bivalent mRNA vaccine booster induces robust antibody immunity against Omicron lineages BA.2, BA.2.12.1, BA.2.75 and BA.5. Cell Discov. 2022, 8, 108. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NPIIL | NPIs |
|---|---|
| 0.80 | Wearing a facemask |
| 0.30 | Banning dining in a restaurant and closing entertainment venues and other public places |
| 0.05 | Restrictions on going outdoors |
| 0.02 | Requirement for rapid antigen testing on a daily basis and quarantining of patients with confirmed cases |
| Model | Overall | Older Patients | ||
|---|---|---|---|---|
| Accumulated Number of Infectious Cases | Accumulated Number of Deaths | Accumulated Number of Infectious Cases | Accumulated Number of Deaths | |
| Model 1: baseline scenario (TNI) | 1273.27 (90.16%) | 1.49 (0.12%) | 244.60 (91.49%) | 1.40 (0.57%) |
| Model 2: NPIs | 680.40 (48.19%) | 0.94 (0.14%) | 134.45 (50.29%) | 0.89 (0.66%) |
| Model 3: NPIs + 75% of cases with Paxlovid | 1053.20 (74.59%) | 0.58 (0.06%) | 204.25 (76.40%) | 0.55 (0.27%) |
| Model 4: NPIs stratified by age | 990.67 (70.16%) | 0.81 (0.08%) | 103.59 (38.75%) | 0.73 (0.70%) |
| Model 5: TNI + completed vaccination on 90% of the population | 1259.43 (89.19%) | 0.56 (0.04%) | 237.69 (88.90%) | 0.51 (0.21%) |
| Model 6: NPIs stratified by age + 75% of cases with Paxlovid | 1019.30 (72.19%) | 0.40 (0.04%) | 119.39 (44.66%) | 0.37 (0.31%) |
| Model 7: completed vaccination on 90% of the population + 75% of cases with Paxlovid + NPIs stratified by age | 1011.87 (71.66%) | 0.19 (0.02%) | 159.53 (59.67%) | 0.17 (0.11%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, J.; Li, Y.; Xiao, L.-F.; Shao, N.-Y.; Liu, M. Flattening the Curve after the Initial Outbreak of Coronavirus Disease 2019: A Data-Driven Modeling Analysis for the Omicron Pandemic in China. Vaccines 2023, 11, 1009. https://doi.org/10.3390/vaccines11051009
Sun J, Li Y, Xiao L-F, Shao N-Y, Liu M. Flattening the Curve after the Initial Outbreak of Coronavirus Disease 2019: A Data-Driven Modeling Analysis for the Omicron Pandemic in China. Vaccines. 2023; 11(5):1009. https://doi.org/10.3390/vaccines11051009
Chicago/Turabian StyleSun, Jiaqi, Yusi Li, Lin-Fan Xiao, Ning-Yi Shao, and Miao Liu. 2023. "Flattening the Curve after the Initial Outbreak of Coronavirus Disease 2019: A Data-Driven Modeling Analysis for the Omicron Pandemic in China" Vaccines 11, no. 5: 1009. https://doi.org/10.3390/vaccines11051009