
Health Systems Determinants of Delivery and Uptake of Maternal Vaccines in Low- and Middle-Income Countries: A Qualitative Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
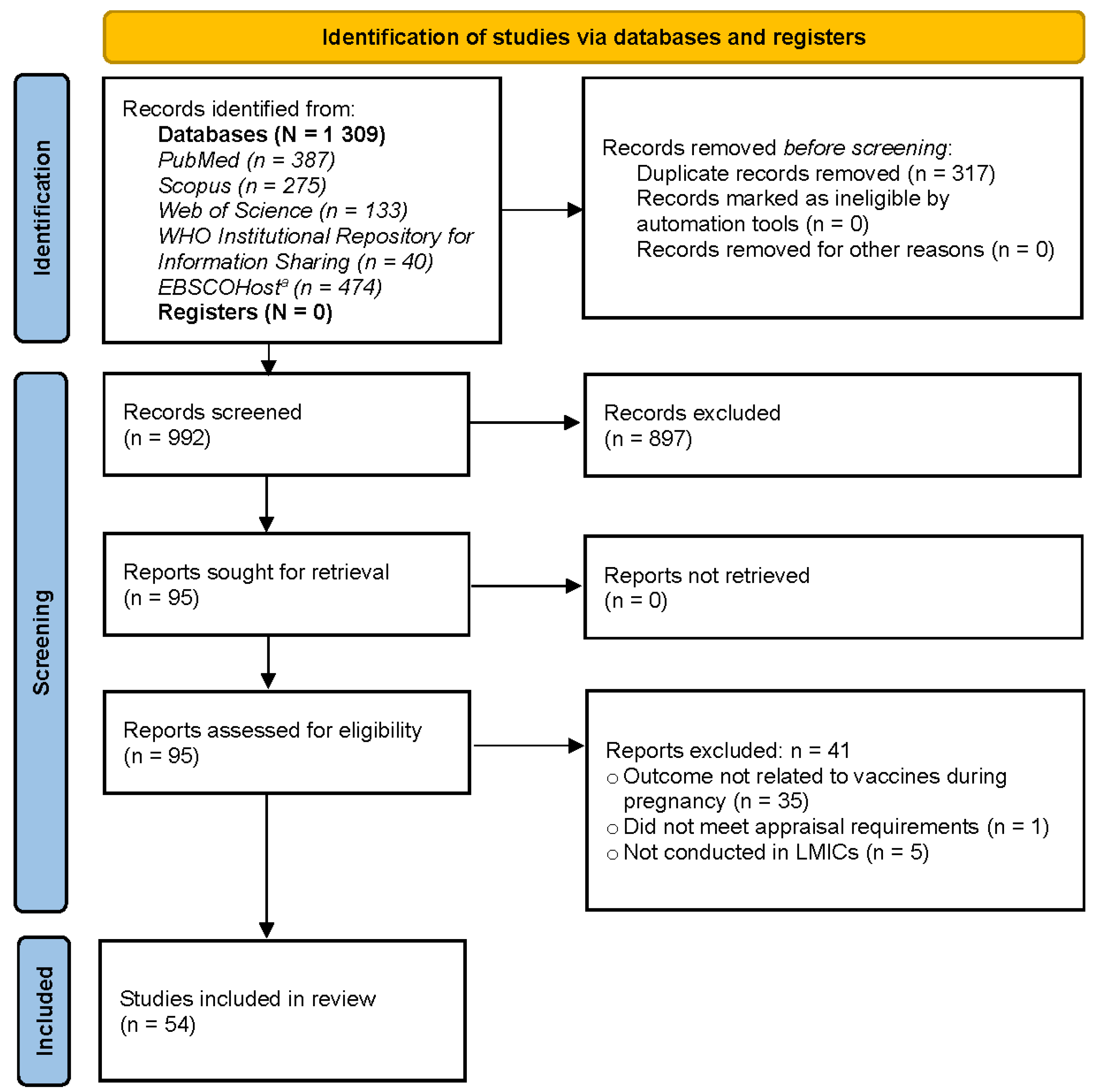
2.1. Search Strategy
2.2. Eligibility Criteria and Study Selection
2.3. Study Appraisal
2.4. Data Extraction
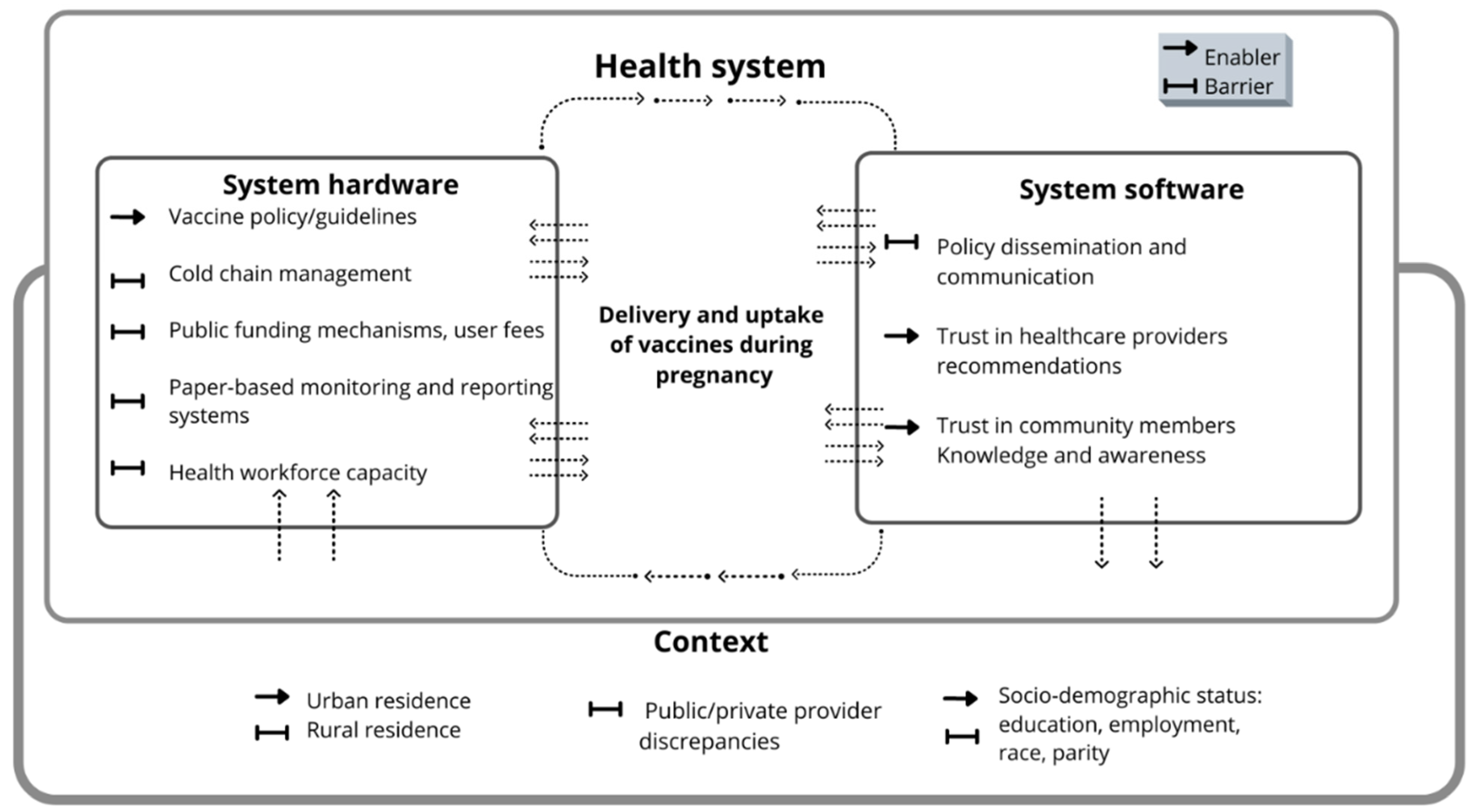
2.5. Conceptual Framework
2.6. Data Synthesis
3. Results
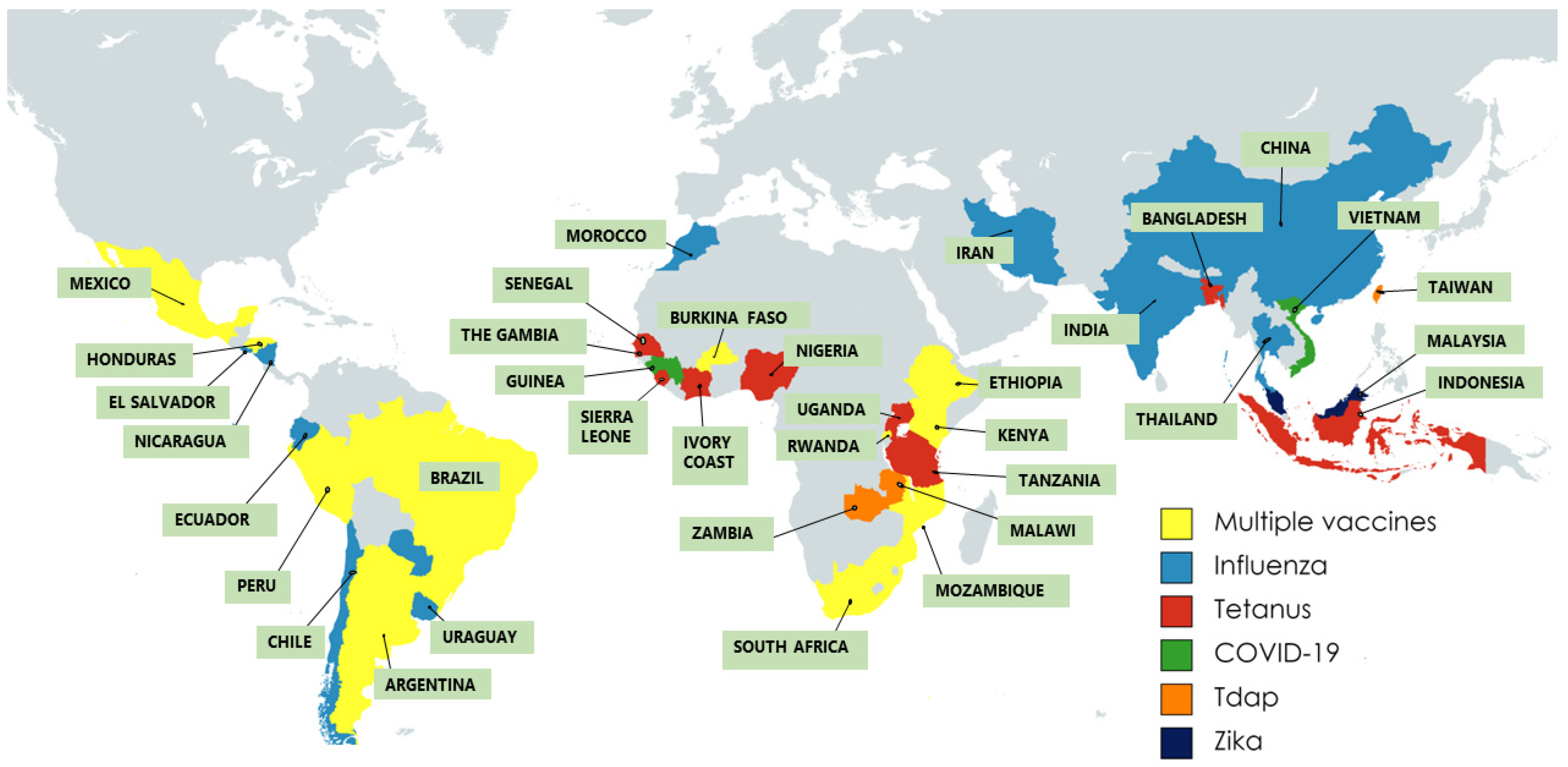
3.1. Characteristics of Included Studies and Participants
3.2. Health Systems Determinants of Maternal Vaccine Delivery
3.3. Health Systems Determinants of Maternal Vaccine Uptake
4. Discussion
4.1. Findings and Recommendations for Vaccine Decision- and Policy-Makers
4.2. Findings and Recommendations for Health Systems and Maternal Vaccination Research Agenda
4.3. Strengths and Limitations of this Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alkema, L.; Chou, D.; Hogan, D.; Zhang, S.; Moller, A.-B.; Gemmill, A.; Fat, D.M.; Boerma, T.; Temmerman, M.; Mathers, C.; et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: A systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet 2016, 387, 462–474. [Google Scholar] [CrossRef] [PubMed]
- Marshall, H.; McMillan, M.; Andrews, R.M.; Macartney, K.; Edwards, K. Vaccines in pregnancy: The dual benefit for pregnant women and infants. Hum. Vaccines Immunother. 2016, 12, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Saso, A.; Kampmann, B. Maternal Immunization: Nature Meets Nurture. Front. Microbiol. 2020, 11, 1499. [Google Scholar] [CrossRef]
- Maitra, C.; Hodge, A.; Jimenez Soto, E. A scoping review of cost benefit analysis in reproductive, maternal, newborn and child health: What we know and what are the gaps? Health Policy Plan. 2016, 31, 1530–1547. [Google Scholar] [CrossRef] [PubMed]
- Regan, A.K. The safety of maternal immunization. Hum. Vaccines Immunother. 2016, 12, 3132–3136. [Google Scholar] [CrossRef]
- Greenwood, B. Maternal immunisation in developing countries. Vaccine 2003, 21, 3436–3441. [Google Scholar] [CrossRef]
- Ortiz, J.R.; Englund, J.A.; Neuzil, K.M. Influenza vaccine for pregnant women in resource-constrained countries: A review of the evidence to inform policy decisions. Vaccine 2011, 29, 4439–4452. [Google Scholar] [CrossRef]
- Ortiz, J.R.; Neuzil, K.M.; Ahonkhai, V.I.; Gellin, B.G.; Salisbury, D.M.; Read, J.S.; Adegbola, R.A.; Abramson, J.S. Translating vaccine policy into action: A report from the Bill & Melinda Gates Foundation Consultation on the prevention of maternal and early infant influenza in resource-limited settings. Vaccine 2012, 30, 7134–7140. [Google Scholar]
- Kachikis, A.; Eckert, L.O.; Englund, J.A. Chapter 1—The History of Maternal Immunization. In Maternal Immunization; Leuridan, E.E., Nunes, M.C., Jones, C.E., Eds.; Academic Press: London, UK, 2020; Available online: https://www.sciencedirect.com/science/article/pii/B9780128145821000012 (accessed on 2 March 2021).
- Swamy, G.K.; Beigi, R.H. Maternal benefits of immunization during pregnancy. Vaccine 2015, 33, 6436–6440. [Google Scholar] [CrossRef]
- Swamy, G.K.; Metz, T.D.; Edwards, K.M.; Soper, D.E.; Beigi, R.H.; Campbell, J.D.; Grassano, L.; Buffi, G.; Dreisbach, A.; Margarit, I.; et al. Safety and immunogenicity of an investigational maternal trivalent group B streptococcus vaccine in pregnant women and their infants: Results from a randomized placebo-controlled phase II trial. Vaccine 2020, 38, 6930–6940. [Google Scholar] [CrossRef]
- Saso, A.; Kampmann, B. Vaccination against respiratory syncytial virus in pregnancy: A suitable tool to combat global infant morbidity and mortality? Lancet Infect. Dis. 2016, 16, e153–e163. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef] [PubMed]
- Zavala, E.; Krubiner, C.B.; Jaffe, E.F.; Nicklin, A.; Gur-Arie, R.; Wonodi, C.; Faden, R.R.; Karron, R.A. Global disparities in public health guidance for the use of COVID-19 vaccines in pregnancy. BMJ Glob. Health 2022, 7, e007730. [Google Scholar] [CrossRef] [PubMed]
- Berman Institute of Bioethics & Center for Immunization Research, Johns Hopkins University. COVID-19 Maternal Immunization Tracker (COMIT). Available online: https://www.comitglobal.org (accessed on 4 September 2022).
- Sedgh, G.; Singh, S.; Hussain, R. Intended and Unintended Pregnancies Worldwide in 2012 and Recent Trends. Stud. Fam. Plann. 2014, 45, 301–314. [Google Scholar] [CrossRef]
- Shen, A.K.; Fields, R.; McQuestion, M. The future of routine immunization in the developing world: Challenges and opportunities. Glob. Health Sci. Pract. 2014, 2, 381–394. [Google Scholar] [CrossRef]
- Bishop, K.; McMorrow, M.; Meiring, S.; Walaza, S.; Rossi, L.; Mhlanga, S.; Tempia, S.; Mathunjwa, A.; Kleynhans, J.; Appiah, G.D.; et al. An evaluation of an influenza vaccination campaign targeting pregnant women in 27 clinics in two provinces of South Africa, 2015–2018. BMC Health Serv. Res. 2021, 21, 941. [Google Scholar] [CrossRef]
- DiTosto, J.D.; Weiss, R.E.; Yee, L.M.; Badreldin, N. Association of Tdap vaccine guidelines with vaccine uptake during pregnancy. PLoS ONE 2021, 16, e0254863. [Google Scholar] [CrossRef]
- Hug, L.; Alexander, M.; You, D.; Alkema, L. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: A systematic analysis. Lancet Glob. Health 2019, 7, e710–e720. [Google Scholar] [CrossRef]
- Choudhary, M.; Solomon, R.; Awale, J.; Dey, R. Demand-side determinants of timely vaccination of oral polio vaccine in social mobilization network areas of CORE Group polio project in Uttar Pradesh, India. BMC Infect. Dis. 2018, 18, 222. [Google Scholar] [CrossRef]
- Ritchie, L.M.P.; Khan, S.; Moore, J.E.; Timmings, C.; van Lettow, M.; Vogel, J.P.; Khan, D.N.; Mbaruku, G.; Mrisho, M.; Mugerwa, K.; et al. Low-and middle-income countries face many common barriers to implementation of maternal health evidence products. J. Clin. Epidemiol. 2016, 76, 229–237. [Google Scholar] [CrossRef]
- Hardt, K.; Bonanni, P.; King, S.; Santos, J.I.; El-Hodhod, M.; Zimet, G.D.; Preiss, S. Vaccine strategies: Optimising outcomes. Vaccine 2016, 34, 6691–6699. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Pluye, P.; Robert, E.; Cargo, M.; Bartlett, G.; O’cathain, A.; Griffiths, F.; Boardman, F.; Gagnon, M.-P.; Rousseau, M.C. Proposal: A mixed methods appraisal tool for systematic mixed studies reviews. Montr. McGill Univ. 2011, 2, 1–8. [Google Scholar]
- Shakarishvili, G.; Atun, R.; Berman, P.; Hsiao, W.; Burgess, C.; Lansang, M.A. Converging Health Systems Frameworks: Towards A Concepts-to-Actions Roadmap for Health Systems Strengthening in Low and Middle Income Countries. Glob. Health Gov. 2010, 3, 2. [Google Scholar]
- De Savigny, D.; Adam, T. Systems Thinking for Health Systems Strengthening; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Agyepong, I.A.; Kwamie, A.; Frimpong, E.; Defor, S.; Ibrahim, A.; Aryeetey, G.C.; Lokossou, V.; Sombie, I. Spanning maternal, newborn and child health (MNCH) and health systems research boundaries: Conducive and limiting health systems factors to improving MNCH outcomes in West Africa. Health Res. Policy Syst. 2017, 15, 54. [Google Scholar] [CrossRef]
- Van Olmen, J.; Criel, B.; Van Damme, W.; Marchal, B.; Van Belle, S.; Van Dormael, M.; Hoeree, T.; Pirard, M.; Kegels, G. Analysing Health Systems to Make Them Stronger; ITGPress: Antwerp, Belgium, 2010. [Google Scholar]
- Amponsah-Dacosta, E.; Kagina, B.M.; Olivier, J. Health systems constraints and facilitators of human papillomavirus immunization programmes in sub-Saharan Africa: A systematic review. Health Policy Plan. 2020, 35, czaa017. [Google Scholar] [CrossRef]
- Engmann, C.; Fleming, J.A.; Khan, S.; Innis, B.L.; Smith, J.M.; Hombach, J.; Sobanjo-ter Meulen, A. Closer and closer? Maternal immunization: Current promise, future horizons. J. Perinatol. 2020, 40, 844–857. [Google Scholar] [CrossRef]
- World Health Organization. Strategies toward Ending Preventable Maternal Mortality (EPMM). 2015. Available online: http://www.who.int/reproductivehealth/topics/maternal_perinatal/epmm/en/ (accessed on 15 September 2021).
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Snelgrove, S. Theme in Qualitative Content Analysis and Thematic Analysis. Forum Qual. Sozialforschung Forum Qual. Soc. Res. 2019, 20, 3. [Google Scholar] [CrossRef]
- Nagata, J.M.; Hernández-Ramos, I.; Kurup, A.S.; Albrecht, D.; Vivas-Torrealba, C.; Franco-Paredes, C. Social determinants of health and seasonal influenza vaccination in adults ≥65 years: A systematic review of qualitative and quantitative data. BMC Public Health 2013, 13, 388. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, H.B.; Trotter, C.; Hickman, M.; Audrey, S. Barriers and facilitators to HPV vaccination of young women in high-income countries: A qualitative systematic review and evidence synthesis. BMC Public Health 2014, 14, 700. [Google Scholar] [CrossRef] [PubMed]
- Giles, M.; Mantel, C.; Muñoz, F.; Moran, A.; Roos, N.; Yusuf, N.; Diaz, T.; Ahun, M.; Lochlainn, L.N.; Wootton, E. Vaccine implementation factors affecting maternal tetanus immunization in low-and middle-income countries: Results of the Maternal Immunization and Antenatal Care Situational Analysis (MIACSA) project. Vaccine 2020, 38, 5268–5277. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, A.M.R.; Vilajeliu, A.; Magariños, M.; Jauregui, B.; Guzmán, L.; Whittembury, A.; Cain, E.; Garcia, O.; Montesanos, R.; Matus, C.R.; et al. Enablers and barriers of maternal and neonatal immunization programs in Latin America. Vaccine 2020, 39, B34–B43. [Google Scholar] [CrossRef] [PubMed]
- Otieno, N.A.; Malik, F.A.; Nganga, S.W.; Wairimu, W.N.; Ouma, D.O.; Bigogo, G.M.; Chaves, S.S.; Verani, J.R.; Widdowson, M.-A.; Wilson, A.D.; et al. Decision-making process for introduction of maternal vaccines in Kenya, 2017–2018. Implement. Sci. 2021, 16, 39. [Google Scholar] [CrossRef]
- Praphasiri, P.; Ditsungneon, D.; Greenbaum, A.; Dawood, F.S.; Yoocharoen, P.; Stone, D.M.; Olsen, S.J.; Lindblade, K.A.; Muangchana, C. Do Thai Physicians Recommend Seasonal Influenza Vaccines to Pregnant Women? A Cross-Sectional Survey of Physicians’ Perspectives and Practices in Thailand. PLoS ONE 2017, 12, e0169221. [Google Scholar] [CrossRef]
- Li, R.; Xie, R.; Yang, C.; Rainey, J.; Song, Y.; Greene, C. Identifying ways to increase seasonal influenza vaccine uptake among pregnant women in China: A qualitative investigation of pregnant women and their obstetricians. Vaccine 2018, 36, 3315–3322. [Google Scholar] [CrossRef]
- Chimukuche, R.S.; Ngwenya, N.; Seeley, J.; Nxumalo, P.S.; Nxumalo, Z.P.; Godongwana, M.; Radebe, N.; Myburgh, N.; Adedini, S.A.; Cutland, C. Assessing Community Acceptance of Maternal Immunisation in Rural KwaZulu-Natal, South Africa: A Qualitative Investigation. Vaccines 2022, 10, 415. [Google Scholar] [CrossRef]
- Li, W.F.; Huang, S.Y.; Peng, H.H.; Chang, Y.L.; Chang, S.D.; Cheng, P.J.; Hsiao, C.-H.; Su, Y.-N.; Lin, T.-H.; Cheng, C.-C.; et al. Factors affecting pregnant women’s decisions regarding prenatal pertussis vaccination: A decision-making study in the nationwide Prenatal Pertussis Immunization Program in Taiwan. Taiwan. J. Obstet. Gynecol. 2020, 59, 200–206. [Google Scholar] [CrossRef]
- Malik, F.A.; Alonso, J.P.; Sanclemente, L.N.; Vilajeliu, A.; Gutierrez, M.; Gonzalez-Casanova, I.; Jones, D.; Omer, S.; Ropero, A.-M.; Belizán, M. Health care providers perspectives about maternal immunization in Latin America. Vaccine 2021, 39, B50–B54. [Google Scholar] [CrossRef] [PubMed]
- Giles, M.L.; Mason, E.; Muñoz, F.M.; Moran, A.C.; Lambach, P.; Merten, S.; Diaz, T.; Baye, M.; Mathai, M.; Pathirana, J.; et al. Antenatal care service delivery and factors affecting effective tetanus vaccine coverage in low-and middle-income countries: Results of the Maternal Immunisation and Antenatal Care Situational analysis (MIACSA) project. Vaccine 2020, 38, 5278–5285. [Google Scholar] [CrossRef] [PubMed]
- Bergenfeld, I.; Nganga, S.W.; Andrews, C.A.; Fenimore, V.L.; Otieno, N.A.; Wilson, A.D.; Chaves, S.S.; Verani, J.R.; Widdowson, M.-A.; Wairimu, W.N.; et al. Provider perspectives on demand creation for maternal vaccines in Kenya. Gates Open Res. 2018, 2, 34. [Google Scholar] [CrossRef]
- Giduthuri, J.G.; Purohit, V.; Maire, N.; Kudale, A.; Utzinger, J.; Schindler, C.; Weiss, M.G. Influenza vaccination of pregnant women: Engaging clinicians to reduce missed opportunities for vaccination. Vaccine 2019, 37, 1910–1917. [Google Scholar] [CrossRef] [PubMed]
- Laizer, S.N.; Hemed, A.; Cyril, P.M. Challenges Experienced by Healthcare Workers on Maternal Tetanus Toxoid Vaccination in Kilimanjaro Region Tanzania. Clin. Immunol. Res. 2021, 5, 1–8. [Google Scholar] [CrossRef]
- Gonzalez-Casanova, I.; Chander, S.; Chaves, S.S.; Otieno, N.A.; Widdowson, M.A.; Verani, J.; Frew, P.; Wilson, A.; Omer, S.B.; Malik, F. Antenatal care providers’ attitudes and beliefs towards maternal vaccination in Kenya. Gates Open Res. 2021, 4, 19. [Google Scholar]
- Malik, A.F.; Belizan, M.; Gutierrez, M.; Vilajeliu, A.; Sanclemente, L.N.; Casanova, I.G.; Jones, D.; Omer, S.; Ropero, A.M.; Alonso, J.P. Pregnant women’s perspectives about maternal immunization in Latin America. Vaccine 2021, 39, B44–B49. [Google Scholar] [CrossRef]
- Simas, C.; Larson, H.J.; Paterson, P. “Saint Google, now we have information!”: A qualitative study on narratives of trust and attitudes towards maternal vaccination in Mexico City and Toluca. BMC Public Health 2021, 21, 1170. [Google Scholar] [CrossRef]
- Giduthuri, J.G.; Purohit, V.; Kudale, A.; Utzinger, J.; Schindler, C.; Weiss, M.G. Antenatal influenza vaccination in urban Pune, India: Clinician and community stakeholders’ awareness, priorities, and practices. Hum. Vaccines Immunother. 2021, 17, 1211–1222. [Google Scholar] [CrossRef]
- Kfouri, R.d.Á.; Richtmann, R. Influenza vaccine in pregnant women: Immunization coverage and associated factors. Einstein Sao Paulo Braz. 2013, 11, 53–57. [Google Scholar] [CrossRef]
- Anatea, M.D.; Mekonnen, T.H.; Dachew, B.A. Determinants and perceptions of the utilization of tetanus toxoid immunization among reproductive-age women in Dukem Town, Eastern Ethiopia: A community-based cross-sectional study. BMC Int. Health Hum. Rights 2018, 18, 27. [Google Scholar] [CrossRef] [PubMed]
- Fleming, J.A.; Baltrons, R.; Rowley, E.; Quintanilla, I.; Crespin, E.; Ropero, A.M.; Ortiz, J.R.; Lambach, P.; Neuzil, K.M.; Stepanchak, M. Implementation of maternal influenza immunization in El Salvador: Experiences and lessons learned from a mixed-methods study. Vaccine 2018, 36, 4054–4061. [Google Scholar] [CrossRef] [PubMed]
- Arriola, C.S.; Suntarattiwong, P.; Dawood, F.S.; Soto, G.; Das, P.; Hunt, D.R.; Sinthuwattanawibool, C.; Kurhe, K.; Thompson, M.G.; Wesley, M.G.; et al. What do pregnant women think about influenza disease and vaccination practices in selected countries. Hum. Vaccines Immunother. 2021, 17, 2176–2184. [Google Scholar] [CrossRef] [PubMed]
- Nyiro, J.U.; Bukusi, E.; Mwaengo, D.; Walumbe, D.; Nyaguara, A.; Nyawanda, B.; Otieno, N.; Berkley, J.A.; Munywoki, P.; Nokes, D.J. Implications of gestational age at antenatal care attendance on the successful implementation of a maternal respiratory syncytial virus (RSV) vaccine program in coastal Kenya. BMC Public Health 2020, 20, 1723. [Google Scholar] [CrossRef]
- Yaya, S.; Kota, K.; Buh, A.; Bishwajit, G. Prevalence and predictors of taking tetanus toxoid vaccine in pregnancy: A cross-sectional study of 8722 women in Sierra Leone. BMC Public Health 2020, 20, 855. [Google Scholar] [CrossRef]
- Erazo, C.E.; Erazo, C.V.; Grijalva, M.J.; Moncayo, A.L. Knowledge, attitudes and practices on influenza vaccination during pregnancy in Quito, Ecuador. BMC Public Health 2021, 21, 72. [Google Scholar] [CrossRef]
- Kaoiean, S.; Kittikraisak, W.; Suntarattiwong, P.; Ditsungnoen, D.; Phadungkiatwatana, P.; Srisantiroj, N.; Asavapiriyanont, S.; Chotpitayasunondh, T.; Dawood, F.S.; Lindblade, K.A. Predictors for influenza vaccination among Thai pregnant woman: The role of physicians in increasing vaccine uptake. Influenza Other Respir. Viruses 2019, 13, 582–592. [Google Scholar] [CrossRef]
- Otieno, N.A.; Otiato, F.; Nyawanda, B.; Adero, M.; Wairimu, W.N.; Ouma, D.; Atito, R.; Wilson, A.; Gonzalez-Casanova, I.; Malik, F.A.; et al. CDrivers and barriers of vaccine acceptance among pregnant women in Kenya. Hum. Vaccines Immunother. 2020, 16, 2429–2437. [Google Scholar] [CrossRef]
- Fleming, J.A.; Munthali, A.; Ngwira, B.; Kadzandira, J.; Jamili-Phiri, M.; Ortiz, J.R.; Lambach, P.; Hombach, J.; Neuzil, K.M.; Stepanchak, M.; et al. CMaternal immunization in Malawi: A mixed methods study of community perceptions, programmatic considerations, and recommendations for future planning. Vaccine 2019, 37, 4568–4575. [Google Scholar] [CrossRef]
- Garcia, P.J.; George, P.E.; Romero, C.; Soto, G.; Carcamo, C.; Bayer, A.M. “The flu is a little more complicated than a cold”: Knowledge, beliefs, and practices related to influenza and influenza vaccination among at-risk populations and health professionals in Peru. Vaccine 2020, 38, 7688–7695. [Google Scholar] [CrossRef]
- Johm, P.; Nkoum, N.; Ceesay, A.; Larson, H.; Kampmann, B. Factors influencing acceptance of vaccination during pregnancy in The Gambia and Senegal. Vaccine 2021, 39920, 3926–3934. [Google Scholar] [CrossRef] [PubMed]
- Madubueze, U.C.; Una, A.F.; Okedo-Alex, I.N.; Agha, V.M.; Umeokonkwo, C.D.; Eze, I.I.; Utulu, R.; Okeke, K.C.; Agbo, U.N.; Nwobashi, L.N.; et al. Awareness, knowledge, risk perception and uptake of maternal vaccination in rural communities of Ebonyi State, Nigeria. Afr. Health Sci. 2022, 4, 306–317. [Google Scholar] [CrossRef]
- Wang, J.; Sun, D.; Abudusaimaiti, X.; Vermund, S.H.; Li, D.; Hu, Y. Low awareness of influenza vaccination among pregnant women and their obstetricians: A population-based survey in Beijing, China. Hum. Vaccines Immunother. 2019, 15, 2637–2643. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Tao, L.; Han, N.; Liu, J.; Yuan, C.; Deng, L.; Han, C.; Sun, F.; Chi, L.; Liu, M.; et al. Acceptance of seasonal influenza vaccination and associated factors among pregnant women in the context of COVID-19 pandemic in China: A multi-center cross-sectional study based on health belief model. BMC Pregnancy Childbirth 2021, 21, 745. [Google Scholar] [CrossRef] [PubMed]
- Simas, C.; Paterson, P.; Lees, S.; Larson, H.J. “From my phone, I could rule the world”: Critical engagement with maternal vaccine information, vaccine confidence builders and post-Zika outbreak rumours in Brazil. Vaccine 2021, 39, 4700–4704. [Google Scholar] [CrossRef] [PubMed]
- Belizán, M.; Rodriguez Cairoli, F.; Mazzoni, A.; Goucher, E.; Zaraa, S.; Matthews, S.; Pingray, V.; Stergachis, A.; Xiong, X.; Berrueta, M.; et al. Data collection systems for active safety surveillance of vaccines during pregnancy in low-and middle-income countries: Developing and piloting an assessment tool (VPASS). BMC Pregnancy Childbirth 2023, 23, 1. [Google Scholar] [CrossRef]
- Nganga, S.W.; Otieno, N.A.; Adero, M.; Ouma, D.; Chaves, S.S.; Verani, J.R.; Widdowson, M.-A.; Wilson, A.; Bergenfeld, I.; Andrews, C.; et al. Patient and provider perspectives on how trust influences maternal vaccine acceptance among pregnant women in Kenya. BMC Health Serv. Res. 2019, 19, 747. [Google Scholar] [CrossRef]
- Kajungu, D.; Muhoozi, M.; Stark, J.; Weibel, D.; Sturkenboom, M.C.J.M. Vaccines safety and maternal knowledge for enhanced maternal immunization acceptability in rural Uganda: A qualitative study approach. PLoS ONE 2020, 15, e0243834. [Google Scholar] [CrossRef]
- Lohiniva, A.-L.; Barakat, A.; Dueger, E.; Restrepo, S.; El Aouad, R. A Qualitative Study of Vaccine Acceptability and Decision Making among Pregnant Women in Morocco during the A (H1N1) pdm09 Pandemic. PLoS ONE 2014, 9, e96244. [Google Scholar] [CrossRef]
- Wong, V.W.Y.; Fong, D.Y.T.; Lok, K.Y.W.; Wong, J.Y.H.; Sing, C.; Choi, A.Y.Y.; Yuen, C.Y.S.; Tarrant, M. Brief education to promote maternal influenza vaccine uptake: A randomized controlled trial. Vaccine 2016, 34, 5243–5250. [Google Scholar] [CrossRef]
- Otieno, N.A.; Nyawanda, B.; Otiato, F.; Adero, M.; Wairimu, W.N.; Atito, R.; Wilson, A.D.; Gonzalez-Casanova, I.; Malik, F.A.; Verani, J.R.; et al. Knowledge and attitudes towards influenza and influenza vaccination among pregnant women in Kenya. Vaccine 2020, 38, 6832–6838. [Google Scholar] [CrossRef] [PubMed]
- González-Block, M.Á.; Gutiérrez-Calderón, E.; Pelcastre-Villafuerte, B.E.; Arroyo-Laguna, J.; Comes, Y.; Crocco, P.; Fachel-Leal, A.; Noboa, L.; Riva-Knauth, D.; Rodríguez-Zea, B.; et al. Influenza vaccination hesitancy in five countries of South America. Confidence, complacency and convenience as determinants of immunization rates. PLoS ONE 2020, 15, e0243833. [Google Scholar] [CrossRef] [PubMed]
- Varan, A.K.; Esteves-Jaramillo, A.; Richardson, V.; Esparza-Aguilar, M.; Cervantes-Powell, P.; Omer, S.B. Intention to accept Bordetella pertussis booster vaccine during pregnancy in Mexico City. Vaccine 2014, 32, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Hassan, J.; AbuBakar, S. Attitudes towards Zika screening and vaccination acceptability among pregnant women in Malaysia. Vaccine 2017, 35, 5912–5917. [Google Scholar] [CrossRef] [PubMed]
- Carcelen, A.; Vilajeliu, A.; Malik, F.; Gilman, R.; Omer, S. Perceptions and attitudes towards vaccination during pregnancy in a peri urban area of Lima, Peru. Vaccine 2021, 39, B27–B33. [Google Scholar] [CrossRef]
- Arriola, C.S.; Vasconez, N.; Thompson, M.; Mirza, S.; Moen, A.C.; Bresee, J.; Talavera, I.; Ropero, A.M. Factors associated with a successful expansion of influenza vaccination among pregnant women in Nicaragua. Vaccine 2016, 34, 1086–1090. [Google Scholar] [CrossRef]
- Arriola, C.S.; Vasconez, N.; Bresee, J.; Ropero, A.M. Knowledge, attitudes and practices about influenza vaccination among pregnant women and healthcare providers serving pregnant women in Managua, Nicaragua. Vaccine 2018, 36, 3686–3693. [Google Scholar] [CrossRef]
- Toure, A.A.; Traore, F.A.; Camara, G.; Magassouba, A.S.; Barry, I.; Kourouma, M.L.; Sylla, Y.; Conte, N.Y.; Cisse, D.; Dioubaté, N.; et al. CoFacilitators and barriers to COVID-19 vaccination among healthcare workers and the general population in Guinea. BMC Infect. Dis. 2022, 22, 1–8. [Google Scholar] [CrossRef]
- Mendoza-Sassi, R.A.; Linhares, A.O.; Schroeder, F.M.M.; Maas, N.M.; Nomiyama, S.; César, J.A. Vaccination against influenza among pregnant women in southern Brazil and associated factors. Cienc. E Saude Coletiva 2019, 24, 4655–4664. [Google Scholar] [CrossRef]
- Larson Williams, A.; Mitrovich, R.; Mwananyanda, L.; Gill, C. Maternal vaccine knowledge in low-and middle-income countries—And why it matters. Hum. Vaccines Immunother. 2019, 15, 283–286. [Google Scholar] [CrossRef]
- Amin, M.B.; Roy, N.; Meem, A.E.; Hossain, E.; Aktarujjaman, M. Trends and determinants of taking tetanus toxoid vaccine among women during last pregnancy in Bangladesh: Country representative survey from 2006 to 2019. PLoS ONE 2022, 17, e0276417. [Google Scholar] [CrossRef] [PubMed]
- Asratie, M.H.; Kassie, B.A.; Belay, D.G.; Endalew, M.; Gashaw, M.; Assegie, G.M. Perception of risk regarding the use of COVID-19 vaccine among pregnant women in Motta town and Hulet Eji Enese district, northwest Ethiopia. PLoS ONE 2022, 17, e0269591. [Google Scholar] [CrossRef] [PubMed]
- Arifin, H.; Widiasih, R.; Pradipta, R.O.; Kurniawati, Y. Regional disparities and their contribution to the coverage of the tetanus toxoid vaccine among women aged 15-49 years in Indonesia. F1000Research 2021, 10, 437. [Google Scholar] [CrossRef] [PubMed]
- Aynalem, Z.B.; Bogale, T.W.; Bantie, G.M.; Ayalew, A.F.; Tamir, W.; Feleke, D.G.; Yazew, B.G. Factors associated with willingness to take COVID-19 vaccine among pregnant women at Gondar town, Northwest Ethiopia: A multicenter institution-based cross-sectional study. PLoS ONE 2022, 17, e0276763. [Google Scholar] [CrossRef] [PubMed]
- Gebremedhin, T.S.; Welay, F.T.; Mengesha, M.B.; Assefa, N.E.; Werid, W.M. Tetanus Toxoid Vaccination Uptake and Associated Factors among Mothers Who Gave Birth in the Last 12 Months in Errer District, Somali Regional State, Eastern Ethiopia. BioMed Res. Int. 2020, 2020, 4023031. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Hoang, M.T.; Nguyen, L.D.; Ninh, L.T.; Nguyen, H.T.T.; Nguyen, A.D.; Vu, L.G.; Vu, G.T.; Doan, L.P.; Latkin, C.A.; et al. Acceptance and willingness to pay for COVID-19 vaccines among pregnant women in Vietnam. Trop. Med. Int. Health TM IH 2021, 26, 1303–1313. [Google Scholar] [CrossRef]
- Yaya, S.; Kota, K.; Buh, A.; Bishwajit, G. Antenatal visits are positively associated with uptake of tetanus toxoid and intermittent preventive treatment in pregnancy in Ivory Coast. BMC Public Health 2019, 19, 1467. [Google Scholar] [CrossRef]
- Honarvar, B.; Odoomi, N.; Mahmoodi, M.; Kashkoli, G.S.; Khavandegaran, F.; Bagheri Lankarani, K.; Moghadami, M. Acceptance and rejection of influenza vaccination by pregnant women in southern Iran: Physicians’ role and barriers. Hum. Vaccines Immunother. 2012, 8, 1860–1866. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. 2019. Available online: https://apps.who.int/iris/handle/10665/327595 (accessed on 15 September 2021).
- Elmusharaf, K.; Byrne, E.; O’Donovan, D. Strategies to increase demand for maternal health services in resource-limited settings: Challenges to be addressed. BMC Public Health 2015, 15, 870. [Google Scholar] [CrossRef]
- Wang, S.A.; Hyde, T.B.; Mounier-Jack, S.; Brenzel, L.; Favin, M.; Gordon, W.S.; Shearer, J.C.; Mantel, C.F.; Arora, N.; Durrheim, D. New vaccine introductions: Assessing the impact and the opportunities for immunization and health systems strengthening. Vaccine 2013, 31, B122–B128. [Google Scholar] [CrossRef]
- Saso, A.; Skirrow, H.; Kampmann, B. Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint-The Immunising Pregnant Women and Infants Network. Vaccines 2020, 8, 556. [Google Scholar] [CrossRef] [PubMed]
- Gauld, N.; Martin, S.; Sinclair, O.; Petousis-Harris, H.; Dumble, F.; Grant, C.C. A qualitative study of views and experiences of women and health care professionals about free maternal vaccinations administered at community pharmacies. Vaccines 2020, 8, 152. [Google Scholar] [CrossRef] [PubMed]
- Bisset, K.A.; Paterson, P. Strategies for increasing uptake of vaccination in pregnancy in high-income countries: A systematic review. Vaccine 2018, 36, 2751–2759. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Vaccine Action Plan 2011–2020. 2013. Available online: https://www.who.int/publications-detail-redirect/global-vaccine-action-plan-2011-2020 (accessed on 13 March 2022).
- Sheikh, K.; Ranson, M.K.; Gilson, L. Explorations on people centredness in health systems. Health Policy Plan. 2014, 29, ii1–ii5. [Google Scholar] [CrossRef]
- Morales, K.F.; Menning, L.; Lambach, P. The faces of influenza vaccine recommendation: A Literature review of the determinants and barriers to health providers’ recommendation of influenza vaccine in pregnancy. Vaccine 2020, 38, 4805–4815. [Google Scholar] [CrossRef] [PubMed]
- Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016.
- Divala, T.H.; Mungwira, R.G.; Laufer, M.K. Moving targets: The challenges of studying infectious diseases among pregnant women in resource limited settings. Vaccine 2015, 33, 6401–6405. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Population Group | Description | Total Studies (n = 54) | Total Participants (n) | |
|---|---|---|---|---|
| Pregnant women | Women pregnant at time of study | 34 | 80,814 | |
| Community members | Women of childbearing age, partners of pregnant women, family, broader community | 17 | 85,566 | |
| Healthcare providers | Obstetricians, physicians, nurses, community health workers | 13 | 1326 | |
| Policymakers and health leadership | National technical advisory group members, health ministry, facility managers, researchers | 4 | 153 | |
| Health Systems Determinant | Descriptive Themes Relating to Maternal Vaccine Delivery (Supply-Side) | |
|---|---|---|
| Enablers of Vaccine Delivery | Barriers to Vaccine Delivery | |
| Policy, leadership and governance | Top-down policy formulation and implementation omits key stakeholder engagement (Brazil, Kenya, Thailand). Lack of coordinated national approach to vaccine policy formulation leads to reliance on international guidelines without consideration for local contexts (Taiwan, Argentina, Brazil, Honduras, Mexico, Peru). Lack of communication from leadership to facility-based healthcare providers on maternal vaccination guidelines (China, Thailand, Kenya). | |
| Financing | Pooled procurement funding for vaccine delivery services (Brazil, Mexico, Honduras, Peru). Reliance on donor funding informs feasibility of vaccine policy recommendations at national level (Kenya). | Reliance on out-of-pocket payments negatively affects pregnant women’s access to lifesaving vaccines. Low facility-level budgets compromise vaccine education and awareness efforts (Kenya). |
| Implementation: vaccine products and service delivery | Increased ANC visits are associated with higher coverage of influenza and tetanus vaccines among pregnant women (Sierra Leone, Ethiopia, India)/ | Guideline discrepancies for vaccine administration and timing during pregnancy between public and private providers (Brazil, Mexico, Honduras, Peru). Vaccine stock-outs (South Africa, Kenya, Brazil). Lack of fuel, electrical power and transport lead to vaccine shortages and impact cold-chain management (Taiwan, Kenya). |
| Health workforce | Training of nurses supports maternal vaccine delivery (Honduras, Brazil, Peru). | Staff shortages due to strikes or high turnover (Kenya, El Salvador). Heavy staff workloads (Nicaragua, India). Lack of clinician training and professional development (Honduras, Brazil, Peru). |
| Information systems | Reliance on ANC booklets/vaccine cards and paper-based systems (Burkina Faso, Mozambique, Kenya, Sierra Leone). | Lack of formal monitoring and reporting structures (Malawi, South Africa). Lack of public/private provider co-ordination (Thailand, Kenya). Lack of electronic health records and/or effective integration thereof (Uganda). |
| Context | Strong political will for maternal vaccines (Brazil). Lack of political interference at the facility level (Kenya). | Gangsterism and crime limit pregnant women’s access to facilities (El Salvador). |
| Health Systems Determinant | Descriptive Themes Relating to Maternal Vaccine Delivery (Demand-Side) | |
|---|---|---|
| Enablers of Vaccine Uptake | Barriers to Vaccine Uptake | |
| Policy, leadership and governance | High level of trust in political governance (Kenya, Ethiopia). | Low level of trust in political governance (Morocco). |
| Decision-making | Healthcare provider recommendations. High level of trust in healthcare providers. | Media sources fuel mistrust (Brazil). |
| Financing | Out-of-pocket payments associated with social standing by spouses (Malawi). | Out-of-pocket payments. User fees for ANC services. |
| Implementation: access | Punitive approach to missed ANC appointments (Malawi). | |
| Health workforce | Education and awareness of maternal vaccines provided by healthcare providers. | Low level of trust in healthcare providers due to previous negative experience (Ethiopia, Brazil). |
| Information systems | Reliance on maternal recall in place of patient records. | |
| Context | Higher education level of pregnant women. Rural residency (Indonesia). Urban residency (Kenya, Bangladesh). | Higher education level of pregnant women (Kenya). Rural residence. Increased travel distance to facilities. Belonging to a religious group (Ethiopia, Senegal). Maternal employment—employers do not grant time off work to access ANC, including vaccination (El Salvador). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davies, B.; Olivier, J.; Amponsah-Dacosta, E. Health Systems Determinants of Delivery and Uptake of Maternal Vaccines in Low- and Middle-Income Countries: A Qualitative Systematic Review. Vaccines 2023, 11, 869. https://doi.org/10.3390/vaccines11040869
Davies B, Olivier J, Amponsah-Dacosta E. Health Systems Determinants of Delivery and Uptake of Maternal Vaccines in Low- and Middle-Income Countries: A Qualitative Systematic Review. Vaccines. 2023; 11(4):869. https://doi.org/10.3390/vaccines11040869
Chicago/Turabian StyleDavies, Bronte, Jill Olivier, and Edina Amponsah-Dacosta. 2023. "Health Systems Determinants of Delivery and Uptake of Maternal Vaccines in Low- and Middle-Income Countries: A Qualitative Systematic Review" Vaccines 11, no. 4: 869. https://doi.org/10.3390/vaccines11040869