
Dutch Healthcare Professionals’ Opinion on the Allocation of Responsibilities concerning Prescribing and Administering Medically Indicated Vaccines to Immunocompromised Patients
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection and Analysis
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. Directorship of Vaccine Recommendations
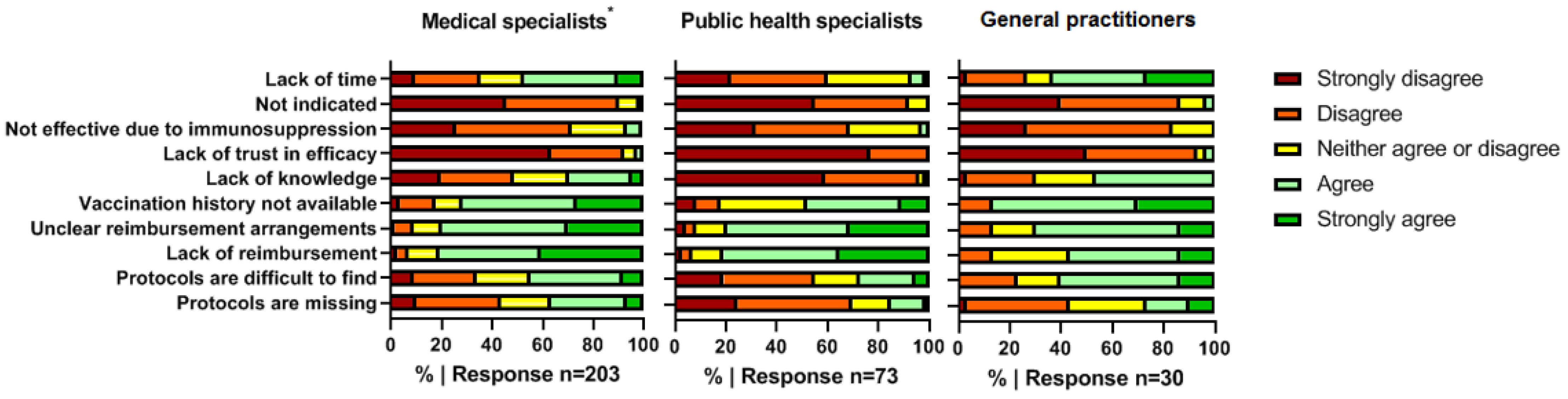
3.2. Barriers to Recommending Medically Indicated Vaccines
3.3. Responsibility for Vaccine Administration
3.4. Barriers and Facilitators to Vaccine Administration
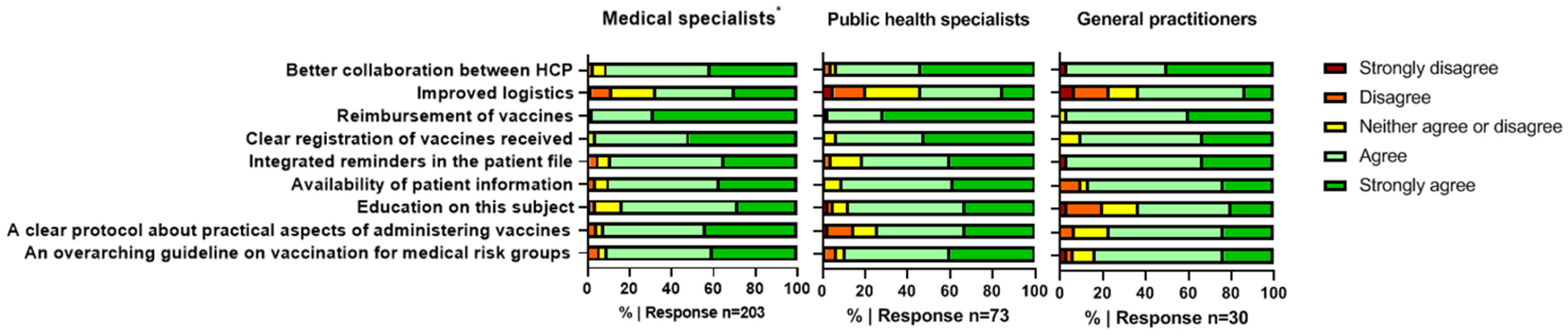
3.5. Solutions to Improve Vaccination Practices
4. Discussion
4.1. Responsibility to Prescribe and Administer Vaccines
4.2. Barriers
4.3. Recommendations for Improvements
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bonten, M.J.; Huijts, S.M.; Bolkenbaas, M.; Webber, C.; Patterson, S.; Gault, S.; van Werkhoven, C.H.; van Deursen, A.M.; Sanders, E.A.; Verheij, T.J.; et al. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N. Engl. J. Med. 2015, 372, 1114–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, A.L.; Heineman, T.C.; Lal, H.; Godeaux, O.; Chlibek, R.; Hwang, S.J.; McElhaney, J.E.; Vesikari, T.; Andrews, C.; Choi, W.S.; et al. Immune Responses to a Recombinant Glycoprotein E Herpes Zoster Vaccine in Adults Aged 50 Years or Older. J. Infect. Dis. 2018, 217, 1750–1760. [Google Scholar] [CrossRef]
- Chilson, E.; Scott, D.A.; Schmoele-Thoma, B.; Watson, W.; Moran, M.M.; Isturiz, R. Immunogenicity and safety of the 13-valent pneumococcal conjugate vaccine in patients with immunocompromising conditions: A review of available evidence. Hum. Vaccines Immunother. 2020, 16, 2758–2772. [Google Scholar] [CrossRef]
- Dagnew, A.F.; Ilhan, O.; Lee, W.S.; Woszczyk, D.; Kwak, J.Y.; Bowcock, S.; Sohn, S.K.; Rodriguez Macias, G.; Chiou, T.J.; Quiel, D.; et al. Immunogenicity and safety of the adjuvanted recombinant zoster vaccine in adults with haematological malignancies: A phase 3, randomised, clinical trial and post-hoc efficacy analysis. Lancet Infect. Dis. 2019, 19, 988–1000. [Google Scholar] [CrossRef]
- Lee, A.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.; Mariette, X.; Bachelez, H.; Belot, A.; Bonnotte, B.; Hachulla, E.; Lahfa, M.; Lortholary, O.; Loulergue, P.; Paul, S.; et al. Vaccination recommendations for the adult immunosuppressed patient: A systematic review and comprehensive field synopsis. J. Autoimmun. 2017, 80, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Struijk, G.H.; Lammers, A.J.; Brinkman, R.J.; Lombarts, M.J.; van Vugt, M.; van der Pant, K.A.; Ten Berge, I.J.; Bemelman, F.J. Immunization after renal transplantation: Current clinical practice. Transpl. Infect. Dis. 2015, 17, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Aberumand, B.; Dyck, B.A.; Towheed, T. Identifying perceptions and barriers regarding vaccination in patients with rheumatoid arthritis: A Canadian perspective. Int. J. Rheum. Dis. 2020, 23, 1526–1533. [Google Scholar] [CrossRef]
- Doornekamp, L.; de Jong, W.; Wagener, M.N.; Goeijenbier, M.; van Gorp, E.C.M. Dutch healthcare professionals’ opinion on vaccination and education to prevent infections in immunocompromised patients: A mixed-method study with recommendations for daily practice. Vaccine 2019, 37, 1476–1483. [Google Scholar] [CrossRef]
- Doornekamp, L.; van Leeuwen, L.; van Gorp, E.; Voeten, H.; Goeijenbier, M. Determinants of Vaccination Uptake in Risk Populations: A Comprehensive Literature Review. Vaccines 2020, 8, 480. [Google Scholar] [CrossRef]
- Lin, C.; Mullen, J.; Smith, D.; Kotarba, M.; Kaplan, S.J.; Tu, P. Healthcare Providers’ Vaccine Perceptions, Hesitancy, and Recommendation to Patients: A Systematic Review. Vaccines 2021, 9, 713. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, I.; Duarte, A.C.; Ferreira, J.F.; Goncalves, M.J.; Meirinhos, T.; Rocha, T.M.; Romao, V.C.; Sousa, S.; Guedes, M.; Conde, M.; et al. Recommendations for Vaccination in Adult Patients with Systemic Inflammatory Rheumatic Diseases from the Portuguese Society of Rheumatology. Acta Reumatol. Port. 2016, 41, 112–130. [Google Scholar] [PubMed]
- Papp, K.A.; Haraoui, B.; Kumar, D.; Marshall, J.K.; Bissonnette, R.; Bitton, A.; Bressler, B.; Gooderham, M.; Ho, V.; Jamal, S.; et al. Vaccination Guidelines for Patients with Immune-mediated Disorders Taking Immunosuppressive Therapies: Executive Summary. J. Rheumatol. 2019, 46, 751–754. [Google Scholar] [CrossRef]
- Saslow, D.; Andrews, K.S.; Manassaram-Baptiste, D.; Smith, R.A.; Fontham, E.T.H.; American Cancer Society Guideline Development, G. Human papillomavirus vaccination 2020 guideline update: American Cancer Society guideline adaptation. CA Cancer J. Clin. 2020, 70, 274–280. [Google Scholar] [CrossRef]
- LCI.RIVM. Vaccinatie Bij Chronisch Inflammatoire Aandoeningen 2019. Available online: https://lci.rivm.nl/richtlijnen/vaccinatie-bij-chronisch-inflammatoire-aandoeningen (accessed on 3 March 2023).
- Medicines Reimbursement Policies in Europe: World Health Organization. Available online: https://www.euro.who.int/__data/assets/pdf_file/0011/376625/pharmaceutical-reimbursement-eng.pdf (accessed on 3 March 2023).
- The Organization and Delivery of Vaccination Services in the European Union: European Observatory on Health Systems and Policies. Available online: https://health.ec.europa.eu/system/files/2018-11/2018_vaccine_services_en_0.pdf (accessed on 3 March 2023).
- Tharmaraj, D.; Dendle, C.; Polkinghorne, K.R.; Mulley, W.R. Kidney transplant recipients’ attitudes toward COVID-19 vaccination and barriers and enablers to vaccine acceptance. Transpl. Infect. Dis. 2022, 24, e13749. [Google Scholar] [CrossRef]
- Philip, R.K.; Di Pasquale, A. Health Care Professionals’ Perspectives on Life-Course Immunization: A Qualitative Survey from a European Conference. Vaccines 2020, 8, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qendro, T.; de la Torre, M.L.; Panopalis, P.; Hazel, E.; Ward, B.J.; Colmegna, I.; Hudson, M. Suboptimal Immunization Coverage among Canadian Rheumatology Patients in Routine Clinical Care. J. Rheumatol. 2020, 47, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Zorginstituut Nederland. Vaccinatiezorg Voor Medische Risicogroepen: Wie Neemt de Regie? 2021. Available online: https://www.rijksoverheid.nl/documenten/rapporten/2021/06/11/adviesrapport-vaccinatiezorg-voor-medische-risicogroepen-wie-neemt-de-regie (accessed on 3 March 2023).
- Wet Medisch-Wetenschappelijk Onderzoek Met Mensen. Available online: https://wetten.overheid.nl/BWBR0009408/2022-07-01#Paragraaf8 (accessed on 3 March 2023).
- The Netherlands Code of Conduct for Academic Practice. 2014. Available online: https://www.universiteitenvannederland.nl/files/documenten/Domeinen/Onderzoek/The_Netherlands_Code%20of_Conduct_for_Academic_Practice_2004_(version2014).pdf (accessed on 3 March 2023).
- Lammers, A.J.; Hoekstra, J.B.; Speelman, P.; Lombarts, K.M. Physicians report barriers to deliver best practice care for asplenic patients: A cross-sectional survey. PLoS ONE 2011, 6, e17302. [Google Scholar] [CrossRef]
- Colmegna, I.; Valerio, V.; Gosselin-Boucher, V.; Lacoste, G.; Labbe, S.; Lavoie, K.L.; Hazel, E.; Ward, B.; Hudson, M.; Pelaez, S. Barriers and facilitators to influenza and pneumococcal vaccine hesitancy in rheumatoid arthritis: A qualitative study. Rheumatology 2021, 60, 5257–5270. [Google Scholar] [CrossRef]
- Gurvits, G.E.; Lan, G.; Tan, A.; Weissman, A. Vaccination practices in patients with inflammatory bowel disease among general internal medicine physicians in the USA. Postgrad. Med. J. 2017, 93, 333–337. [Google Scholar] [CrossRef]
- Wasan, S.K.; Coukos, J.A.; Farraye, F.A. Vaccinating the inflammatory bowel disease patient: Deficiencies in gastroenterologists knowledge. Inflamm. Bowel. Dis. 2011, 17, 2536–2540. [Google Scholar] [CrossRef] [PubMed]
- Yeung, J.H.; Goodman, K.J.; Fedorak, R.N. Inadequate knowledge of immunization guidelines: A missed opportunity for preventing infection in immunocompromised IBD patients. Inflamm. Bowel. Dis. 2012, 18, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Hurley, L.P.; O’Leary, S.T.; Dooling, K.; Anderson, T.C.; Crane, L.A.; Cataldi, J.R.; Brtnikova, M.; Beaty, B.L.; Gorman, C.; Guo, A.; et al. Survey of Physician Practices, Attitudes, and Knowledge Regarding Recombinant Zoster Vaccine. J. Gen. Intern. Med. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.; Lopalco, P.L.; Giesecke, J. Immunisation registers—important for vaccinated individuals, vaccinators and public health. Euro Surveill. 2012, 17, 20151. [Google Scholar] [CrossRef] [PubMed]
- Wehbi, N.K.; Wani, R.J.; Klepser, D.G.; Murry, J.; Khan, A.S. Impact of implementing a technology platform in community pharmacies to increase adult immunizations rates. Vaccine 2019, 37, 56–60. [Google Scholar] [CrossRef]
- Shapiro Ben David, S.; Goren, I.; Mourad, V.; Cahan, A. Vaccination Coverage among Immunocompromised Patients in a Large Health Maintenance Organization: Findings from a Novel Computerized Registry. Vaccines 2022, 10, 1654. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Total | Medical Specialists | Nurse Practitioners/Physician Assistants | Public Health Specialists | General Practitioners |
|---|---|---|---|---|---|
| Number (% of total participants) | 306 (100) | 165 (53.9) | 38 (12.4) | 73 (23.9) | 30 (9.8) |
| Age (median (IQR)) | 44.0 (37.8–52.0) | 44.0 (39.0–51.0) | 40.0 (33.8–48.0) | 49.0 (38.0–57.5) | 40.0 (34.8–47.0) |
| Female (n (%)) | 217 (70.9) | 107 (64.8) | 35 (92.1) | 55 (75.3) | 20 (66.7) |
| Years working in current position (%) | |||||
| <5 | 84 (27.5) | 46 (27.9) | 13 (34.2) | 17 (23.3) | 8 (26.7) |
| 5–10 | 74 (24.2) | 40 (24.2) | 13 (34.2) | 11 (15.1) | 10 (33.3) |
| 10–15 | 56 (18.3) | 33 (20.0) | 7 (18.4) | 14 (19.2) | 2 (6.7) |
| 15–20 | 36 (11.8) | 16 (9.7) | 2 (5.3) | 13 (17.8) | 5 (16.7) |
| >20 | 56 (18.3) | 30 (18.2) | 3 (7.9) | 18 (24.7) | 5 (16.7) |
| Specialty | MSs (n = 203) | |
|---|---|---|
| Non-Academic (n = 104) | Academic (n = 99) | |
| Infectiology (n, %) | 29 (27.9) | 22 (22.2) |
| Gastro-enterology (n, %) | 19 (18.3) | 20 (20.2) |
| Rheumatology (n, %) | 28 (26.9) | 4 (4.0) |
| Hematology (n, %) | 20 (19.2) | 11 (11.1) |
| Nephrology (n, %) | 2 (1.9) | 16 (16.2) |
| Ophthalmology (n, %) | 0 (0) | 8 (8.1) |
| Clinical immunology (n, %) | 1 (1.0) | 6 (6.1) |
| Pulmonology (n, %) | 1 (1.0) | 6 (6.1) |
| Dermatology (n, %) | 0 (0) | 4 (4.0) |
| Cardiology (n, %) | 0 (0) | 1 (1.0) |
| Unknown (n, %) | 4 (3.8) | 1 (1.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
te Linde, E.; Doornekamp, L.; Daenen, K.C.P.; van Gorp, E.C.M.; Bruns, A.H.W. Dutch Healthcare Professionals’ Opinion on the Allocation of Responsibilities concerning Prescribing and Administering Medically Indicated Vaccines to Immunocompromised Patients. Vaccines 2023, 11, 686. https://doi.org/10.3390/vaccines11030686
te Linde E, Doornekamp L, Daenen KCP, van Gorp ECM, Bruns AHW. Dutch Healthcare Professionals’ Opinion on the Allocation of Responsibilities concerning Prescribing and Administering Medically Indicated Vaccines to Immunocompromised Patients. Vaccines. 2023; 11(3):686. https://doi.org/10.3390/vaccines11030686
Chicago/Turabian Stylete Linde, Elsemieke, Laura Doornekamp, Katrijn C. P. Daenen, Eric C. M. van Gorp, and Anke H. W. Bruns. 2023. "Dutch Healthcare Professionals’ Opinion on the Allocation of Responsibilities concerning Prescribing and Administering Medically Indicated Vaccines to Immunocompromised Patients" Vaccines 11, no. 3: 686. https://doi.org/10.3390/vaccines11030686