
Humoral Response after SARS-CoV-2 Vaccination in Prostate Cancer Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Collection
2.3. Detection of SARS-CoV-2 Antibody
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Characteristics of the Studied Population
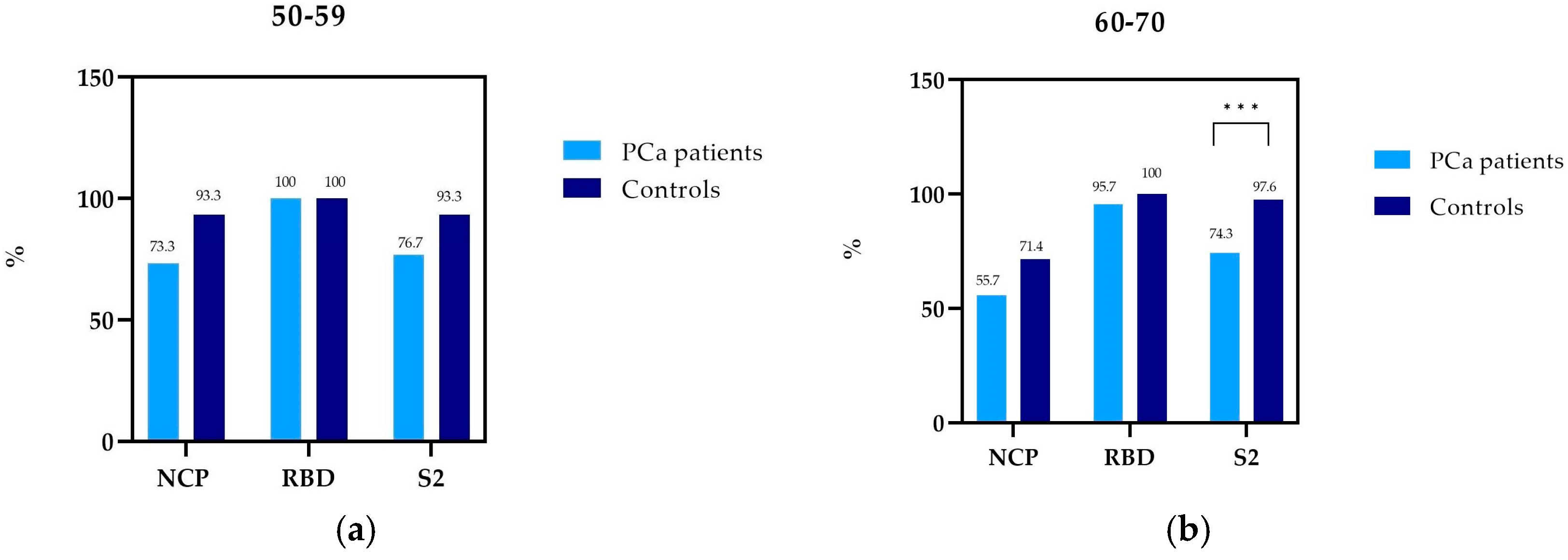
3.2. Prevalence of NCP, RBD, and S2 IgG Antibody in PCa Patients and Controls by Age
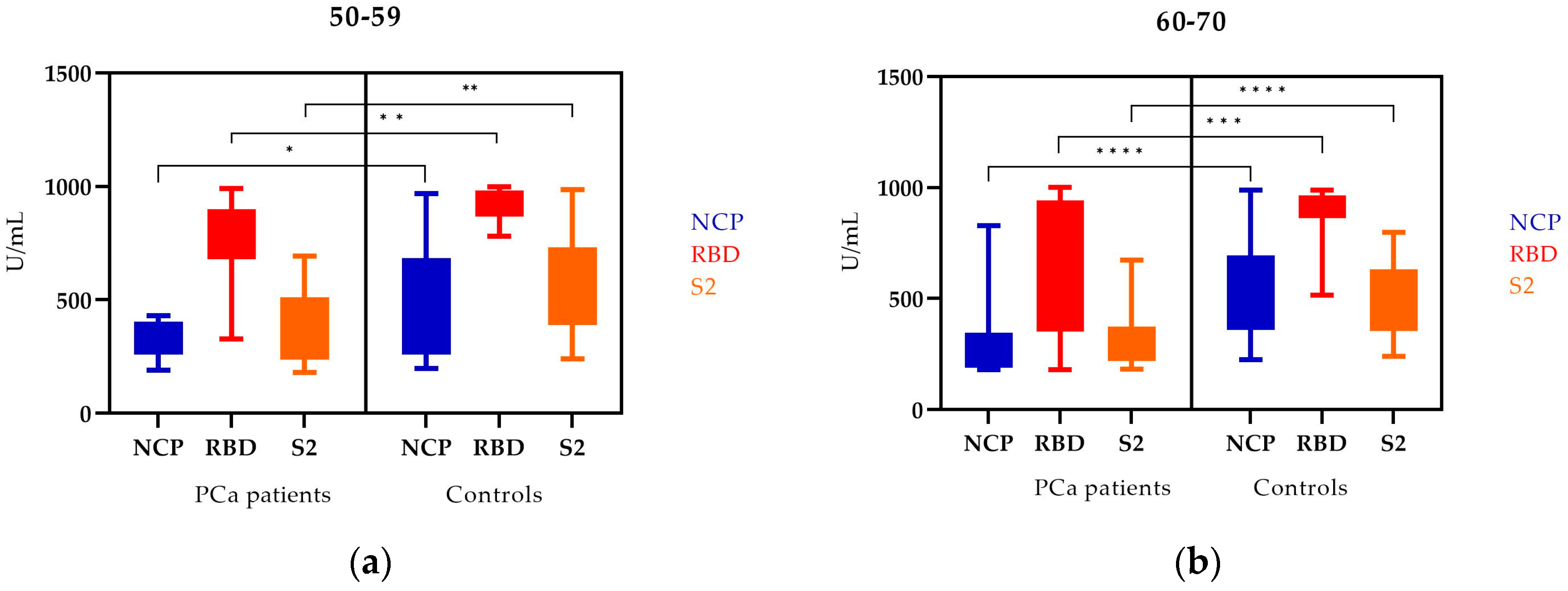
3.3. The NCP, RBD, and S2 IgG Antibody Levels in PCa Patients and Controls by Age
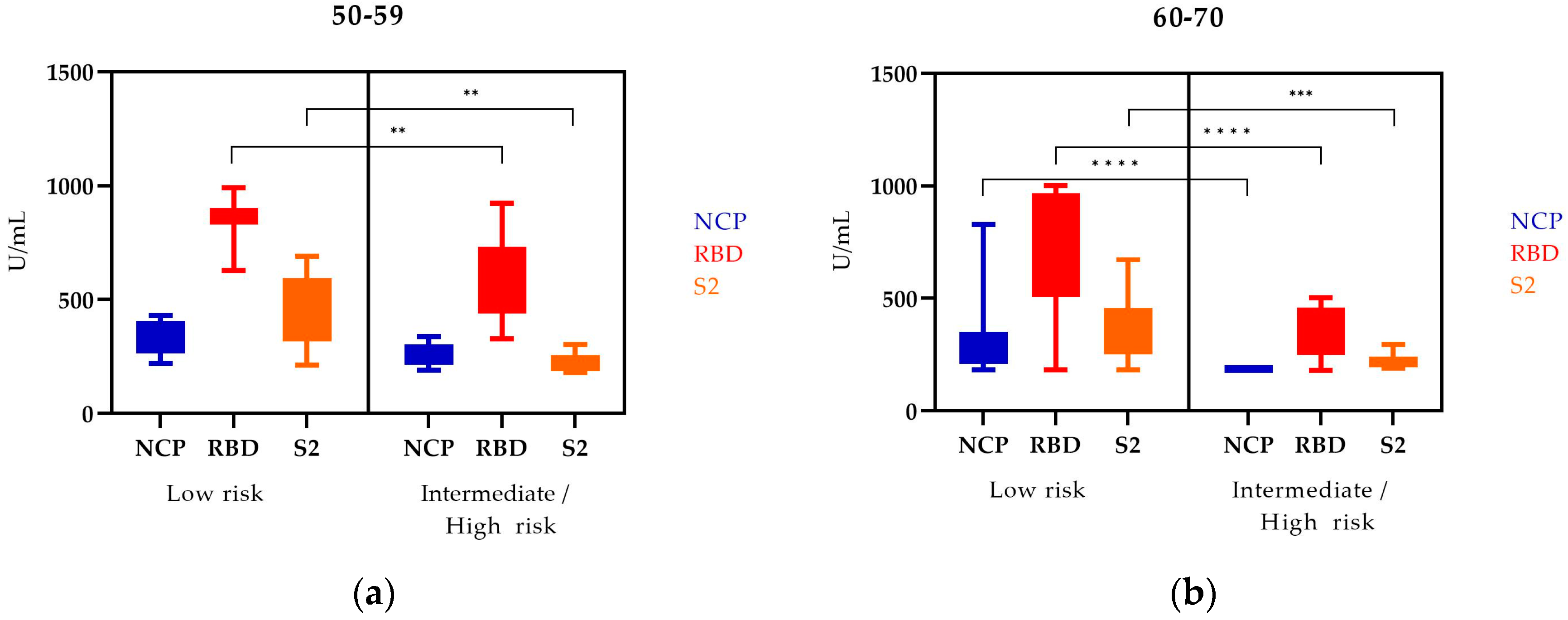
3.4. NCP, RBD, and S2 IgG Antibody Levels in PCa Patients Depending on Age in Two Risk Groups (the EAU Risk Group Classification of PCa)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update on COVID-19—22 February 2023. Edition 131. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---22-february-2023 (accessed on 28 February 2023).
- Mou, R.; Jin, X.; Li, W.; Wu, M.; Liu, X.; Liu, Z.; Guo, S.; Li, X.; Jia, Y. Prostate cancer: A risk factor for COVID-19 in males? A protocol for systematic review and meta analysis. Medicine 2020, 99, e22591. [Google Scholar] [CrossRef]
- Zong, Z.; Wei, Y.; Ren, J.; Zhang, L.; Zhou, F. The intersection of COVID-19 and cancer: Signaling pathways and treatment implications. Mol. Cancer 2021, 20, 76. [Google Scholar] [CrossRef]
- Prostate Cancer: Statistics. Available online: https://www.cancer.net/cancer-types/prostate-cancer/statistics (accessed on 28 February 2023).
- Prostate Cancer—Is It Worth Getting Tested? Available online: https://pacjent.gov.pl (accessed on 28 February 2023).
- Malik, S.S.; Batool, R.; Masood, N.; Yasmin, A. Risk factors for prostate cancer: A multifactorial case-control study. Curr. Probl. Cancer 2018, 42, 337–343. [Google Scholar] [CrossRef]
- Stultz, J.; Fong, L. How to turn up the heat on the cold immune microenvironment of metastatic prostate cancer. Prostate Cancer Prostatic Dis. 2021, 24, 697–717. [Google Scholar] [CrossRef]
- Kwon, J.T.W.; Bryant, R.J.; Parkes, E.E. The tumor microenvironment and immune responses in prostate cancer patients. Endocr. Relat. Cancer 2021, 28, T95–T107. [Google Scholar] [CrossRef] [PubMed]
- Hinshaw, D.C. Shevde LA. 2019. The tumor microenvironment innately modulates cancer progression. Cancer Res. 2019, 79, 4557–4566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messex, J.K.; Liou, G.-Y. Impact of Immune Cells in the Tumor Microenvironment of Prostate Cancer Metastasis. Life 2023, 13, 333. [Google Scholar] [CrossRef]
- Dai, J.; Lu, Y.; Roca, H.; Keller, J.M.; Zhang, J.; McCauley, L.K.; Keller, E.T. Immune mediators in the tumor microenvironment of prostate cancer. Chin. J. Cancer 2017, 36, 29. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, H.; Hagerling, C.; Werb, Z. Roles of the immune system in cancer: From tumor initiation to metastatic progression. Genes Dev. 2018, 32, 1267–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.I.; Soki, F.N.; McCauley, L.K. Roles of bone marrow cells in skeletal metastases: No longer bystanders. Cancer Microenviron. 2011, 4, 237–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabrilovich, D.I.; Nagaraj, S. Myeloid-derived suppressor cells as regulators of the immune system. Nat. Rev. Immunol. 2009, 9, 162–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R.H.; Vanaparthy, R.; Greene, J.N. COVID-19 in Immunocompromised Cancer Patients: A Case Series and Review of the Literature. Cancer Control 2021, 28, 1–7. [Google Scholar] [CrossRef]
- Esperança-Martins, M.; Gonçalves, L.; Soares-Pinho, I.; Gomes, A.; Serrano, M.; Blankenhaus, B.; Figueiredo-Campos, P.; Catarina-Marques, A.; Castro-Barbosa, A.; Cardoso, A.; et al. Humoral Immune Response of SARS-CoV-2–Infected Patients with Cancer: Influencing Factors and Mechanisms. Oncologist 2021, 26, e1619–e1632. [Google Scholar] [CrossRef]
- Steele, R.W. Managing Infection in Cancer Patients and Other Immunocompromised Children. Ochsner J. 2012, 12, 202–210. [Google Scholar] [PubMed]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading Committee. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2016, 9–10, 339–341. [Google Scholar] [CrossRef]
- Epstein, J.I.; Zelefsky, M.J.; Sjoberg, D.D.; Nelson, J.B.; Egevad, L.; Magi-Galluzzi, C.; Vickers, A.J.; Parwani, A.V.; Reuter, V.E.; Fine, S.W. A Contemporary Prostate Cancer Grading System: A Validated Alternative to the Gleason Score. Eur. Urol. 2016, 69, 428–435. [Google Scholar] [CrossRef] [Green Version]
- EAU Guidelines for Prostate Cancer. Available online: https://uroweb.org/guidelines/prostate-cancer/chapter/classification-and-staging-systems (accessed on 28 February 2023).
- Błaszczuk, A.; Michalski, A.; Malm, M.; Drop, B.; Polz-Dacewicz, M. Antibodies to NCP, RBD and S2 SARS-CoV-2 in Vaccinated and Unvaccinated Healthcare Workers. Vaccines 2022, 10, 1169. [Google Scholar] [CrossRef]
- Heudel, P.; Favier, B.; Assaad, S.; Zrounba, P.; Blay, J.-Y. Reduced SARS-CoV-2 infection and death after two doses of COVID-19 vaccines in a series of 1503 cancer patients. Ann. Oncol. 2021, 32, 1443–1444. [Google Scholar] [CrossRef]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.S.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N. Engl. J. Med. 2022, 386, 2201–2212. [Google Scholar] [CrossRef]
- Becerril-Gaitan, A.; Vaca-Cartagena, B.F.; Ferrigno, A.S.; Mesa-Chavez, F.; Barrientos-Gutiérrez, T.; Tagliamento, M.; Lambertini, M.; Villarreal-Garza, C. Immunogenicity and risk of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection after Coronavirus Disease 2019 (COVID-19) vaccination in patients with cancer: A systematic review and meta-analysis. Eur. J. Cancer 2022, 160, 243–260. [Google Scholar] [CrossRef]
- Ferrara, P.; Ponticelli, D.; Magliuolo, R.; Borrelli, M.; Schiavone, B.; Mantovani, L.G. Time-Varying Effect of Hybrid Immunity on the Risk of Breakthrough Infection after Booster Dose of mRNA COVID-19 Vaccine: The MOSAICO Study. Vaccines 2022, 10, 1353. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ierullo, M.; Ku, T.; Marinelli, T.; Majchrzak-Kita, B.; Yousuf, A.; Kulasingam, V.; Humar, A.; Kumar, D. Humoral and cellular immune response and safety of two-dose SARS- CoV-2 mRNA-1273 vaccine in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3980–3989. [Google Scholar] [CrossRef]
- Mehrabi Nejad, M.-M.; Moosaie, F.; Dehghanbanadaki, H.; Haji Ghadery, A.; Shabani, M.; Tabary, M.; Aryannejad, A.; SeyedAlinaghi, S.; Rezaei, N. Immunogenicity of COVID-19 mRNA vaccines in immunocompromised patients: A systematic review and meta-analysis. Eur. J. Med. Res. 2021, 27, 23. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, B.U.; Drabe, C.H.; Barnkob, M.B.; Johansen, I.S.; Hansen, A.K.K.; Nilsson, A.C.; Rasmussen, L.D. Antibody response following the third and fourth SARS-CoV-2 vaccine dose in individuals with common variable immunodeficiency. Front. Immunol. 2022, 13, 934476. [Google Scholar] [CrossRef] [PubMed]
- Overheu, O.; Quast, D.R.; Schmidt, W.E.; Sakinç-Güler, T.; Reinacher-Schick, A. Low Serological Prevalence of SARS-CoV-2 Antibodies in Cancer Patients at a German University Oncology Center. Oncol. Res. Treat. 2022, 45, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Cavanna, L.; Citterio, C.; Toscani, I. COVID-19 Vaccines in Cancer Patients. Seropositivity and Safety. Systematic Review and Meta-Analysis. Vaccines 2021, 9, 1048. [Google Scholar] [CrossRef]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef]
- Martins-Branco, D.; Nader-Marta, G.; Tecic Vuger, A.; Debien, V.; Ameye, L.; Brandão, M.; Punie, K.; Loizidou, A.; Willard-Gallo, K.; Spilleboudt, C. Immune response to anti-SARS-CoV-2 prime-vaccination in patients with cancer: A systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 2022. [Google Scholar] [CrossRef]
- Chen, J.; Deng, J.C.; Goldstein, D.R. How aging impacts vaccine efficacy: Known molecular and cellular mechanisms and future directions. Trends Mol. Med. 2022, 28, 1100–1111. [Google Scholar] [CrossRef] [PubMed]
- Pinti, M.; Appay, V.; Campisi, J.; Frasca, D.; Fülöp, T.; Sauce, D.; Larbi, A.; Weinberger, B.; Cossarizza, A. Aging of the immune system: Focus on inflammation and vaccination. Eur. J. Immunol. 2016, 46, 2286–2301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel, A.; Ben-Zvi, H.; Moskovits, N.; Brenner, B.; et al. Evaluation of Seropositivity Following BNT162b2 Messenger RNA Vaccination for SARS-CoV-2 in Patients Undergoing Treatment for Cancer. JAMA Oncol. 2021, 7, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv, T.; Shorer Arbel, Y.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef] [PubMed]
- Monin, L.; Laing, A.G.; Muñoz-Ruiz, M.; McKenzie, D.R.; Del Molino Del Barrio, I.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: Interim analysis of a prospective observational study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef] [PubMed]
- van Dam, P.A.; Debie, Y.; Teuwen, L.; Verbruggen, L.; Vanhoutte, G.; Peeters, B.; Croes, L.; Vulsteke, C.; Anguille, S.; Vandamme, T.; et al. Comparison of S1 antibody titers between BNT162b2 and ChAdOx1 COVID-19 vaccination in cancer patients. ESMO Open 2022, 7, 100414. [Google Scholar] [CrossRef] [PubMed]
- Debie, Y.; Van Audenaerde, J.R.M.; Vandamme, T.; Croes, L.; Teuwen, L.-A.; Verbruggen, L.; Vanhoutte, G.; Marcq, E.; Verheggen, L.; Le Blon, D.; et al. Humoral and Cellular Immune Responses against SARS-CoV-2 after Third Dose BNT162b2 following Double-Dose Vaccination with BNT162b2 versus ChAdOx1 in Patients with Cancer. Clin. Cancer Res. 2023, 29, 635–646. [Google Scholar] [CrossRef]
- Chen, J.; Kelley, W.J.; Goldstein, D.R. Role of Aging and the Immune Response to Respiratory Viral Infections: Potential Implications for COVID-19. J. Immunol. 2020, 205, 313–320. [Google Scholar] [CrossRef]
- Shaw, A.C.; Joshi, S.; Greenwood, H.; Panda, A.; Lord, J. Aging of the Innate Immune System. Curr. Opin. Immunol. 2010, 22, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Panda, A.; Arjona, A.; Sapey, E.; Bai, F.; Fikrig, E.; Montgomery, R.R.; Lord, J.M.; Shaw, A.C. Human innate immunosenescence: Causes and consequences for immunity in old age. Trends Immunol. 2009, 30, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Macrae, K.; Martinez-Cajas, J.; Bessai, K.; Abdulhamed, A.; Gong, Y. Quantitative Analysis of SARS-CoV-2 Antibody Levels in Cancer Patients Post Three Doses of Immunization and Prior to Breakthrough COVID-19 Infections. Curr. Oncol. 2022, 29, 7059–7071. [Google Scholar] [CrossRef] [PubMed]
- Barrière, J.; Carles, M.; Audigier-Valette, C.; Re, D.; Adjtoutah, Z.; Seitz-Polski, B.; Gounant, V.; Descamps, D.; Zalcman, G. Third dose of anti-SARS-CoV-2 vaccine for patients with cancer: Should humoral responses be monitored? A position article. Eur. J. Cancer 2022, 162, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Haggenburg, S.; Hofsink, Q.; Lissenberg-Witte, B.I.; Broers, A.E.C.; van Doesum, J.A.; van Binnendijk, R.S.; den Hartog, G.; Bhoekhan, M.S.; Haverkate, N.J.E.; Burger, J.A.; et al. Antibody Response in Immunocompromised Patients With Hematologic Cancers Who Received a 3-Dose mRNA-1273 Vaccination Schedule for COVID-19. JAMA Oncol. 2022, 8, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- Fendler, A.; de Vries, E.G.E.; GeurtsvanKessel, C.H.; Haanen, J.B.; Wörmann, B.; Turajlic, S.; von Lilienfeld-Toal, M. COVID-19 vaccines in patients with cancer: Immunogenicity, efficacy and safety. Nat. Rev. Clin. Oncol. 2022, 19, 385–401. [Google Scholar] [CrossRef] [PubMed]
- Mehrabi Nejad, M.-M.; Shobeiri, P.; Dehghanbanadaki, H.; Tabary, M.; Aryannejad, A.; Haji Ghadery, A.; Shabani, M.; Moosaie, F.; SeyedAlinaghi, S.; Rezaei, N. Seroconversion following the first, second, and third dose of SARS-CoV-2 vaccines in immunocompromised population: A systematic review and meta-analysis. Virol. J. 2022, 19, 132. [Google Scholar] [CrossRef]
- Schmidt, T.; Klemis, V.; Schub, D.; Schneitler, S.; Reichert, M.C.; Wilkens, H.; Sester, U.; Sester, M.; Mihm, J. Cellular immunity predominates over humoral immunity after homologous and heterologous mRNA and vector-based COVID-19 vaccine regimens in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3990–4002. [Google Scholar] [CrossRef]
- Pulliam, J.R.C.; van Schalkwyk, C.; Govender, N.; von Gottberg, A.; Cohen, C.; Groome, M.J.; Dushoff, J.; Mlisana, K.; Moultrie, H. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 2022, 376, eabn4947. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Benslimane, F.M.; et al. Protection against the Omicron variant from previous SARS-CoV-2 infection. N. Engl. J. Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef]
- Accorsi, E.K.; Britton, A.; Fleming-Dutra, K.E.; Smith, Z.R.; Shang, N.; Derado, G.; Miller, J.; Schrag, S.J.; Verani, J.R. Association between 3 doses of mRNA COVID-19 vaccine and symptomatic infection caused by the SARS-CoV-2 Omicron and Delta variants. JAMA 2022, 327, 639–651. [Google Scholar] [CrossRef]
- Tan, S.T.; Kwan, A.T.; Rodríguez-Barraquer, I.; Singer, B.J.; Park, H.J.; Lewnard, J.A.; Sears, D.; Lo, N.C. Infectiousness of SARS-CoV-2 breakthrough infections and reinfections during the Omicron wave. Nat. Med. 2023, 29, 358–365. [Google Scholar] [CrossRef]
- Cohen, I.; Campisi-Pfinto, S.; Rozenberg, O.; Colodner, R.; Bar-Sela, G. The Humoral Response of Patients With Cancer to Breakthrough COVID-19 Infection or the Fourth BNT162b2 Vaccine Dose. Oncologist 2023, oyad003. [Google Scholar] [CrossRef] [PubMed]
- Amodeo, G.; Bugada, D.; Franchi, S.; Moschetti, G.; Grimaldi, S.; Panerai, A.; Allegri, M.; Sacerdote, P. Immune function after major surgical intervention: The effect of postoperative pain treatment. J. Pain Res. 2018, 11, 1297–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameters | PCa Patients | Controls | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age | 50–59 | 30 | 30.0 | 30 | 41.7 |
| 60–70 | 70 | 70.0 | 42 | 58.3 | |
| Risk | Low | 67 | 67.0 | - | - |
| Intermediate/high | 33 | 33.0 | - | - | |
| NCP | RBD | S2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PCa Patients | Controls | PCa Patients | Controls | PCa Patients | Controls | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| 50–59 | 22 | 73.3 | 28 | 93.3 | 30 | 100.0 | 30 | 100.0 | 23 | 76.7 | 28 | 93.3 |
| p | 0.0797 | 0.1455 | ||||||||||
| 60–70 | 39 | 55.7 | 30 | 71.4 | 67 | 95.7 | 42 | 100.0 | 52 | 74.3 | 41 | 97.6 |
| p | 0.1119 | 0.2905 | 0.0013 * | |||||||||
| NCP | RBD | S2 | ||||
|---|---|---|---|---|---|---|
| PCa Patients | Controls | PCa Patients | Controls | PCa Patients | Controls | |
| 50–59 | 298.0 | 461.3 | 877.8 | 962.7 | 335.6 | 501.8 |
| (190.1–430.5) | (196.3–969.1) | (326.3–990.8) | (780.0–999.9) | (180.7–691.6) | (239.9–986.5) | |
| p | 0.0157 * | 0.0018 * | 0.0023 * | |||
| 60–70 | 217.1 | 545.1 | 696.1 | 917.4 | 266.1 | 476.1 |
| (179.6–827.9) | (225.6–989.2) | (180.0–1000.0) | (515.1–989.9) | (182.1–672.2) | (239.9–797.5) | |
| p | <0.0001 * | 0.0005 * | <0.0001 * | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Błaszczuk, A.; Sikora, D.; Kiś, J.; Stępień, E.; Drop, B.; Polz-Dacewicz, M. Humoral Response after SARS-CoV-2 Vaccination in Prostate Cancer Patients. Vaccines 2023, 11, 770. https://doi.org/10.3390/vaccines11040770
Błaszczuk A, Sikora D, Kiś J, Stępień E, Drop B, Polz-Dacewicz M. Humoral Response after SARS-CoV-2 Vaccination in Prostate Cancer Patients. Vaccines. 2023; 11(4):770. https://doi.org/10.3390/vaccines11040770
Chicago/Turabian StyleBłaszczuk, Agata, Dominika Sikora, Jacek Kiś, Ewa Stępień, Bartłomiej Drop, and Małgorzata Polz-Dacewicz. 2023. "Humoral Response after SARS-CoV-2 Vaccination in Prostate Cancer Patients" Vaccines 11, no. 4: 770. https://doi.org/10.3390/vaccines11040770