
Effectiveness of the Air-Filled Technique to Reduce the Dead Space in Syringes and Needles during ChAdox1-n CoV Vaccine Administration
 and
and
Abstract
:1. Introduction
2. Materials and Methods
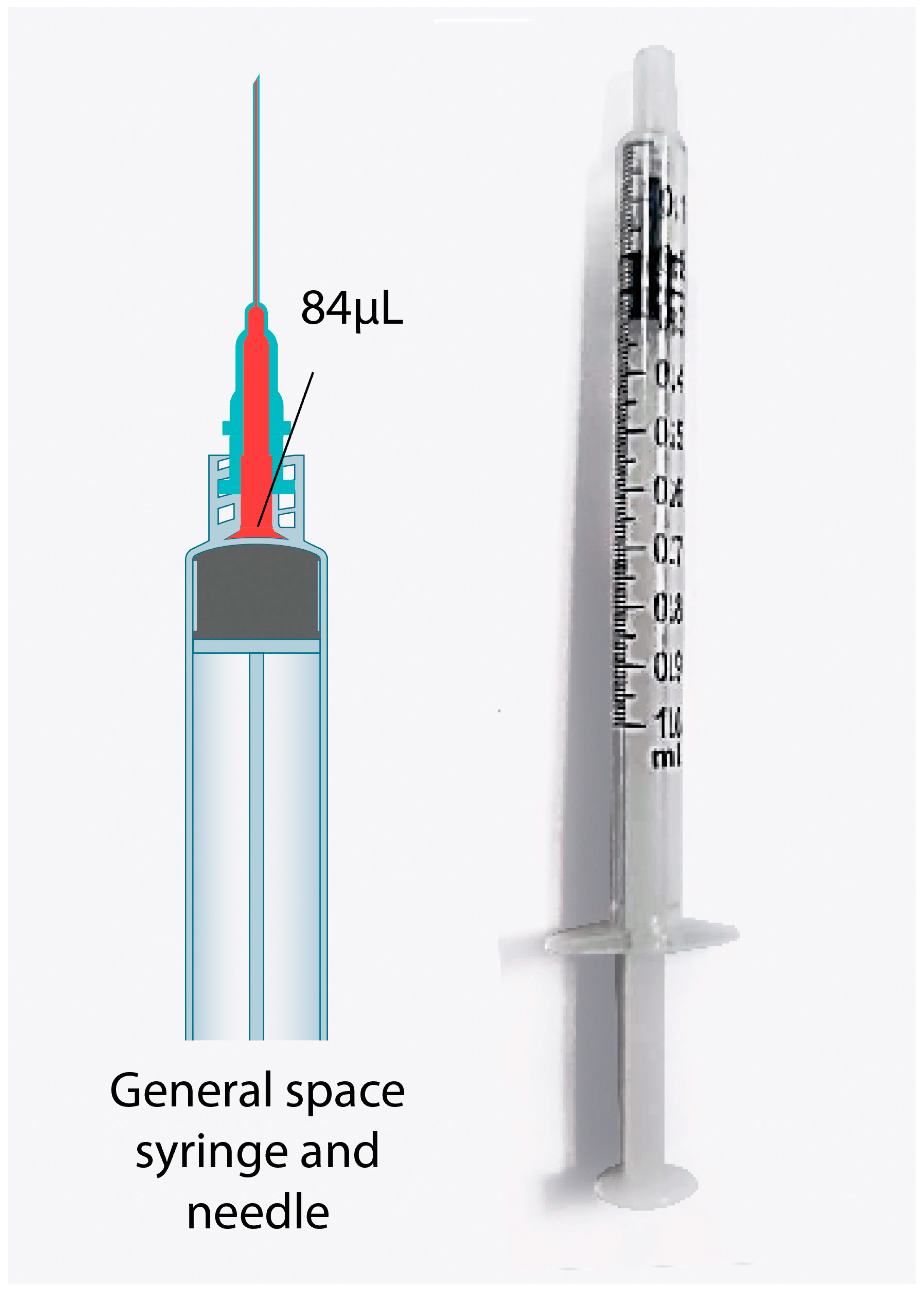
2.1. ChAdox1-n CoV Injection Technique
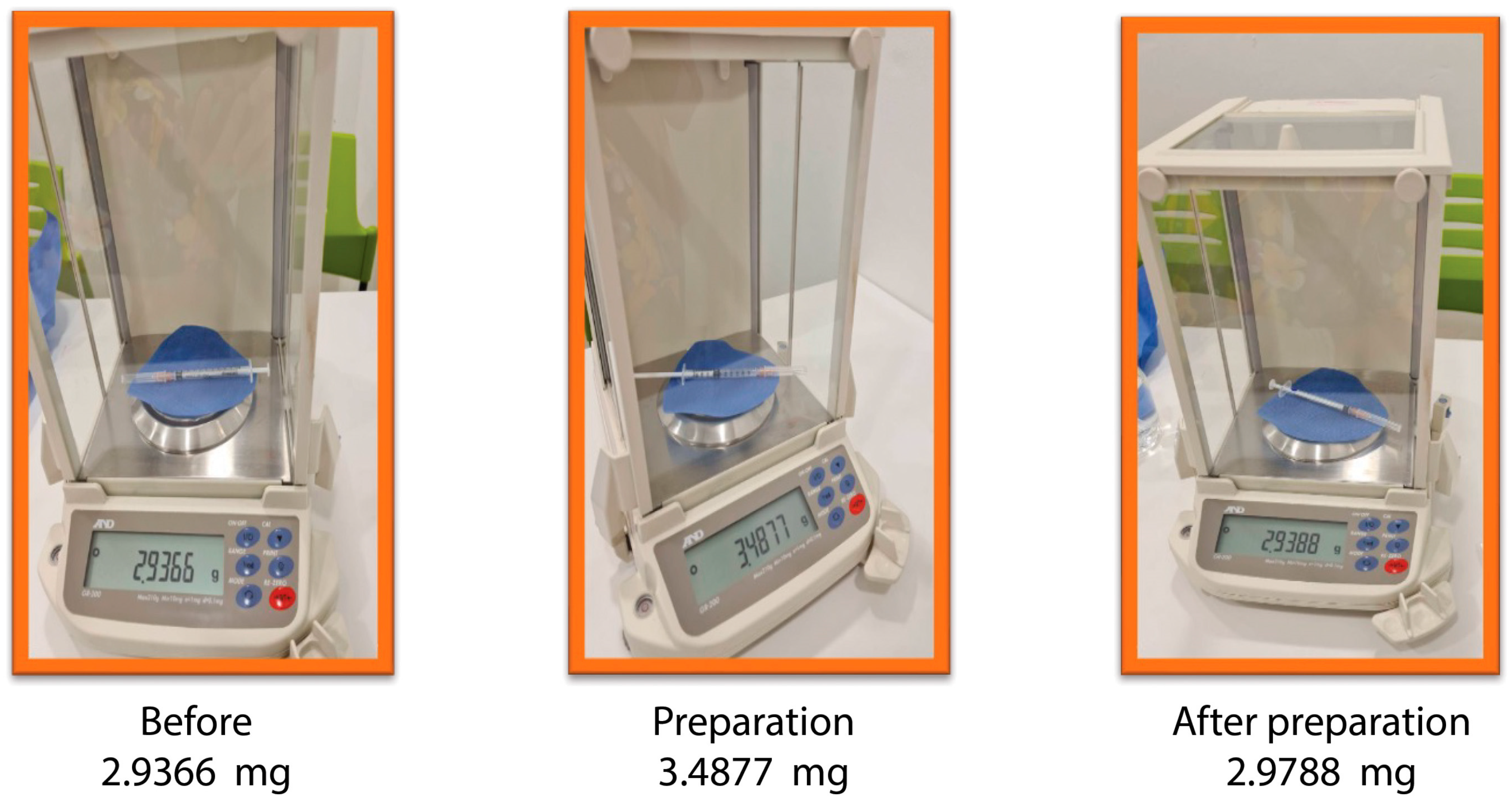
2.2. Outcome Measurement
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhattacharyya, A.; Seth, A.; Srivast, N.; Imeokparia, M.; Rai, S. Coronavirus (COVID-19): A systematic review and meta-analysis to evaluate the significance of demographics and comorbidities. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Chang, J.; Agliata, J.; Guarinieri, M. COVID-19-Enacting a ‘new normal’ for people who use drugs. Int. J. Drug Policy 2020, 83, 102832. [Google Scholar] [CrossRef] [PubMed]
- Garba, B.; Zakaria, Z.; Salihu, M.D.; Bande, F.; Saidu, B.; Bala, J.A. Breaking the cycle of the COVID-19 transmission: A challenge for Nigeria. J. Glob. Health 2020, 10, 020309. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccine Important Information about the AstraZeneca Vaccine Vaxzevria 29 April 2021. Available online: https://www.hse.ie/eng/services/news/newsfeatures/COVID19-updates/COVID-19-vaccine-materials/important-information-about-COVID19-vaccine-astrazeneca.pdf (accessed on 10 May 2022).
- Hancock, E.; Ward, Z.; Ayres, R.; Neale, J.; Hussey, D.; Kesten, J.M.; Hickman, M.; Vickerman, P. Detachable low dead space syringes for the prevention of hepatitis C among people who inject drugs in Bristol, UK: An economic evaluation. Addiction 2020, 115, 702–713. [Google Scholar] [CrossRef] [PubMed]
- Hasan, T.; Beardsley, J.; Marais, B.J.; Nguyen, T.A.; Fox, G.J. The implementation of mass-vaccination against SARS-CoV-2: A systematic review of existing strategies and guidelines. Vaccines 2021, 9, 326. [Google Scholar] [CrossRef] [PubMed]
- Kesten, J.M.; Ayres, R.; Neale, J.; Clark, J.; Vickerman, P.; Hickman, M.; Redwood, S. Acceptability of low dead space syringes and implications for their introduction: A qualitative study in the West of England. Int. J. Drug Policy 2017, 39, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Manomaipiboon, A.; Phumisantiphong, U.; Maneerit, J.; Chalearmchai, Y.; Jirawathin, W.; Prajongsai, A.; Phankavong, P.; Trakarnvanich, T. Immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2 with 12-dose vial: An interim analysis. Vaccine 2022, 40, 587–593. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Vial No. | Syringe Needle Weight | Syringe Needle Weight after Drawing the Distilled Water | Weight of Distilled Water in Syringe before Injection | Weight of Distilled Water in Syringe after Injection | Weight of the Dead Space of Distilled Water in Syringe | Volume of Distilled Water the Patient Received | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Vial 1 | 2.9408 | 0.0153 | 3.4560 | 0.0136 | 0.5151 | 0.0071 | 2.9549 | 0.0111 | 0.0141 | 0.0084 | 0.5011 | 0.0084 |
| Vial 2 | 2.9348 | 0.0175 | 3.4542 | 0.5194 | 0.5194 | 0.0074 | 2.9510 | 0.0172 | 0.0161 | 0.0024 | 0.5033 | 0.0078 |
| Vial 3 | 2.9330 | 0.0091 | 3.4516 | 0.0180 | 0.5186 | 0.0137 | 2.9428 | 0.0102 | 0.0098 | 0.0073 | 0.5089 | 0.0128 |
| Vial 4 | 2.9351 | 0.0083 | 3.4501 | 0.0155 | 0.5149 | 0.0137 | 2.9457 | 0.0115 | 0.0105 | 0.0094 | 0.5044 | 0.0122 |
| Vial 5 | 2.9359 | 0.0081 | 3.4516 | 0.0130 | 0.5157 | 0.0118 | 2.9462 | 0.0083 | 0.0103 | 0.0080 | 0.5054 | 0.0099 |
| Average | 2.9359 | 0.0122 | 3.4527 | 0.0148 | 0.5168 | 0.0109 | 2.9481 | 0.0124 | 0.0122 | 0.0077 | 0.5046 | 0.0104 |
| Vial No. | Syringe Needle Weight | Syringe Needle Weight after Drawing the Vaccine | Weight of Vaccine in Syringe before Injection | Weight of Vaccine in Syringe after Injection | Weight of the Dead Space of Vaccine in Syringe | Weight of Vaccine Injected out of the Syringe | Volume of Vaccine the Patient Received | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Vial 1 | 2.9326 | 0.0133 | 3.4804 | 0.0119 | 0.5478 | 0.0144 | 2.9566 | 0.0101 | 0.0240 | 0.0069 | 0.5238 | 0.0081 | 0.5086 | 0.0079 |
| Vial 2 | 2.9316 | 0.0310 | 3.4833 | 0.0184 | 0.5517 | 0.0213 | 2.9737 | 0.0219 | 0.0421 | 0.0244 | 0.5095 | 0.0134 | 0.4947 | 0.0130 |
| Vial 3 | 2.9436 | 0.0227 | 3.4861 | 0.0220 | 0.5425 | 0.0043 | 2.9654 | 0.0234 | 0.0218 | 0.0043 | 0.5207 | 0.0045 | 0.5055 | 0.0044 |
| Vial 4 | 2.9345 | 0.0112 | 3.4759 | 0.0124 | 0.5414 | 0.0048 | 2.9540 | 0.0114 | 0.0195 | 0.0055 | 0.5219 | 0.0050 | 0.5067 | 0.0048 |
| Vial 5 | 2.9337 | 0.0136 | 3.4819 | 0.0130 | 0.5482 | 0.0132 | 2.9576 | 0.0101 | 0.0239 | 0.0066 | 0.5243 | 0.0080 | 0.5090 | 0.0078 |
| Average | 2.9353 | 0.0205 | 3.4816 | 0.0165 | 0.5462 | 0.0137 | 2.9616 | 0.0182 | 0.0263 | 0.0148 | 0.5199 | 0.0100 | 0.5048 | 0.0097 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prueksaanantakal, N.; Manomaipiboon, A.; Phankavong, P.; Jirawathin, W.; Benjakul, N.; Maneerit, J.; Phumisantiphong, U.; Trakarnvanich, T. Effectiveness of the Air-Filled Technique to Reduce the Dead Space in Syringes and Needles during ChAdox1-n CoV Vaccine Administration. Vaccines 2023, 11, 741. https://doi.org/10.3390/vaccines11040741
Prueksaanantakal N, Manomaipiboon A, Phankavong P, Jirawathin W, Benjakul N, Maneerit J, Phumisantiphong U, Trakarnvanich T. Effectiveness of the Air-Filled Technique to Reduce the Dead Space in Syringes and Needles during ChAdox1-n CoV Vaccine Administration. Vaccines. 2023; 11(4):741. https://doi.org/10.3390/vaccines11040741
Chicago/Turabian StylePrueksaanantakal, Naphatthorn, Anan Manomaipiboon, Patchara Phankavong, Warissara Jirawathin, Nontawat Benjakul, Jakravoot Maneerit, Uraporn Phumisantiphong, and Thananda Trakarnvanich. 2023. "Effectiveness of the Air-Filled Technique to Reduce the Dead Space in Syringes and Needles during ChAdox1-n CoV Vaccine Administration" Vaccines 11, no. 4: 741. https://doi.org/10.3390/vaccines11040741