
Prevalence, Risk Factors and Vaccine Response against Hepatitis B in People Aged 50 Years or Older


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cross-Sectional Study
- Exposure to HBV: positivity for markers of exposure or infection by HBV: HBsAg or anti-HBc;
- Serological profile of vaccination: isolated positivity for the anti-HBs marker;
- Reported on the vaccination card: three doses of vaccine against hepatitis B on the vaccination card;
- Serological profile of vaccination or vaccine reported on the vaccination card: positivity for the isolated anti-HBs marker or three vaccine doses against hepatitis B via vaccination card.
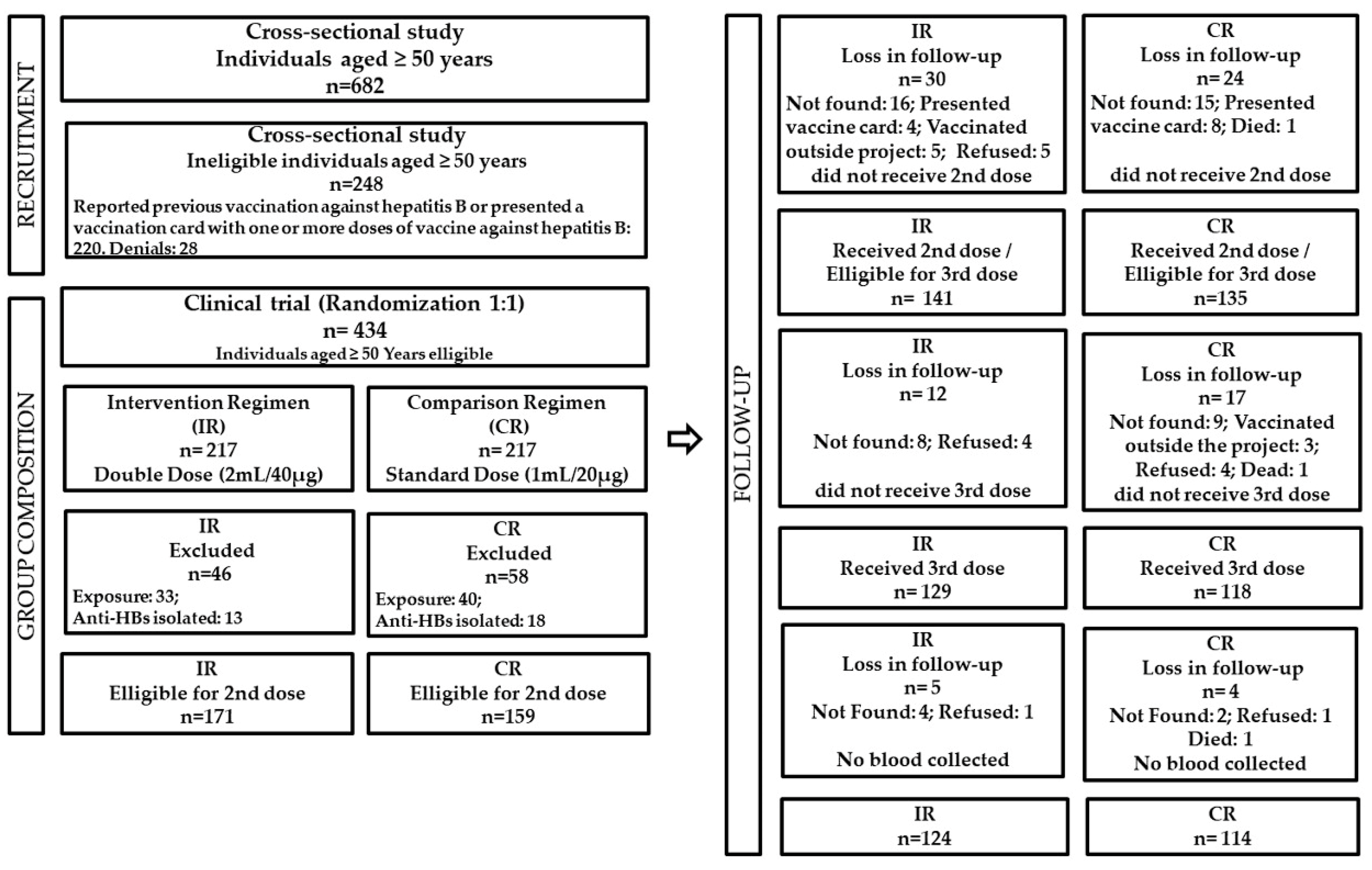
2.2. Randomized and Controlled Clinical Trial
- Having participated in the cross-sectional study;
- Not having a vaccination record or report of previous vaccination against hepatitis B;
- Having presented a negative result for HBsAg in the rapid test performed in the cross-sectional study.
3. Results
3.1. Cross-Sectional Study
3.2. Randomized and Controlled Clinical Trial
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Hepatitis Report 2017; World Health Organization: Geneva, Switzerland, 2017; Available online: https://www.who.int/publications/i/item/9789241565455 (accessed on 27 January 2023).
- Sheena, B.S.; Hiebert, L.; Han, H.; Ippolito, H.; Abbasi-Kangevari, M.; Abbasi-Kangevari, Z.; Abbastabar, H.; Abdoli, A.; Ali, H.A.; Adane, M.M.; et al. Global, regional, and national burden of hepatitis B, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol. Hepatol. 2022, 7, 796–829. [Google Scholar] [CrossRef]
- Szmuness, W.; Stevens, C.E.; Harley, E.J.; Zang, E.A.; Oleszko, W.R.; William, D.C.; Sadovsky, R.; Morrison, J.M.; Kellner, A. Hepatitis B vaccine: Demonstration of efficacy in a controlled clinical trial in a high-risk population in the United States. N. Engl. J. Med. 1980, 303, 833–841. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/bitstream/handle/10665/246177/WHO-HIV-2016.06-eng.pdf (accessed on 27 January 2023).
- Liu, Z.; Yang, Q.; Shi, O.; Ye, W.; Chen, X.; Zhang, T. The epidemiology of hepatitis B and hepatitis C infections in China from 2004 to 2014: An observational population-based study. J. Viral Hepat. 2018, 25, 1543–1554. [Google Scholar] [CrossRef]
- Ministério da Saúde. Nota técnica Conjunta N° 02/2013. Ampliação da Oferta da Vacina Contra a Hepatite B Para a Faixa Etária de 30 a 49 anos em 2013; Ministério da Saúde: Brasília, Brazil, 2013. Available online: http://antigo.aids.gov.br/pt-br/legislacao/nota-tecnica-conjunta-no-022013cgpnidevep-e-cgdhrvdst-aidssvsems (accessed on 27 January 2023).
- Pattyn, J.; Hendrickx, G.; Vorsters, A.; Van Damme, P. Hepatitis B Vaccines. J. Infect. Dis. 2021, 224, S343–S351. [Google Scholar] [CrossRef]
- Ministério da Saúde. Boletim Epidemiológico das Hepatites Virais 2021; Ministério da Saúde: Brasília, Brazil, 2021. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2021/boletim-epidemiologico-de-hepatite-2021.pdf (accessed on 27 January 2023).
- Vermeulen, M.; Swanevelder, R.; Van Zyl, G.; Lelie, N.; Murphy, E.L. An assessment of hepatitis B virus prevalence in South African young blood donors born after the implementation of the infant hepatitis B virus immunization program: Implications for transfusion safety. Transfusion 2021, 61, 2688–2700. [Google Scholar] [CrossRef]
- Lewis, R.; Mitchell, K.R.; Mercer, C.H.; Datta, J.; Jones, K.G.; Wellings, K. Navigating new sexual partnerships in midlife: A socioecological perspective on factors shaping STI risk perceptions and practices. Sex. Transm. Infect. 2020, 96, 238–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minichiello, V.; Rahman, S.; Hawkes, G.; Pitts, M. STI epidemiology in the global older population: Emerging challenges. Perspect Public Health 2012, 132, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. . Nota Técnica Conjunta n. 149 de 2015. Informa as Mudanças no Calendário Vacinal de Vacinação para o ano de 2016; Ministério da Saúde: Brasília, Brazil, 2015; Available online: https://www.cvpvacinas.com.br/pdf/nota_informativa_149.pdf (accessed on 27 January 2023).
- Lima, L.A.; Lago, B.V.D.; Weis-Torres, S.M.D.S.; Martins, R.M.B.; Cesar, G.A.; Bandeira, L.M.; Rezende, G.R.; Lindenberg, A.S.C.; Gomes, S.A.; Motta-Castro, A.R.C. Hepatitis B: Changes in epidemiological features of Afro-descendant communities in Central Brazil. Sci. Rep. 2020, 10, 6708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezende, G.R.; Lago, B.V.; Puga, M.A.; Bandeira, L.M.; Pompilio, M.A.; Castro, V.; Tanaka, T.S.; Cesar, G.A.; Oliveira, S.; Yassuda, R.; et al. Prevalence, incidence and associated factors for HBV infection among male and female prisoners in Central Brazil: A multicenter study. Int. J. Infect. Dis. 2020, 96, 298–307. [Google Scholar] [CrossRef]
- Caetano, K.A.; Del-Rios, N.H.; Pinheiro, R.S.; Bergamaschi, F.P.; Carneiro, M.A.; Teles, S.A. Low Immunogenicity of Recombinant Hepatitis B Vaccine Derived from Hansenula polymorpha in Adults Aged Over 40 Years. Am. J. Trop. Med. Hyg. 2017, 96, 118–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, C.L.; Klopfer, S.O.; Martin, J.C.; Schödel, F.P.; Bhuyan, P.K. Safety and immunogenicity of a modified process hepatitis B vaccine in healthy adults >/=50 years. Hum. Vaccines 2011, 7, 1336–1342. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Hong, S.; Im, J.H.; Lee, J.S.; Baek, J.H.; Kwon, H.Y. Systematic review and meta-analysis of immune response of double dose of hepatitis B vaccination in HIV-infected patients. Vaccine 2020, 38, 3995–4000. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Menchen, L.; Garcia-Sanchez, V.; Marin, I.; Villagrasa, J.R.; Chaparro, M. Comparison of the effectiveness of two protocols for vaccination (standard and double dosage) against hepatitis B virus in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2012, 35, 1379–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food and Drug Administration. Hepatitis B Vaccine (Recombinant); Food and Drug Administration: Washington, USA, 2018. Available online: https://www.fda.gov/vaccines-blood-biologics/hepatitis-b-vaccine-recombinant (accessed on 27 January 2023).
- Abramowicz, M.; Zuccotti, G.; Pflomm, J. The Medical Letter on Drugs and Therapeutics. A Two-Dose Hepatitis B Vaccine for Adults (Heplisav-B). JAMA 2018, 319, 822–823. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística. Censo Demográfico 2010; Instituto Brasileiro de Geografia e Estatística: Rio de Janeiro, Brazil, 2010. Available online: https://biblioteca.ibge.gov.br/visualizacao/periodicos/93/cd_2010_caracteristicas_populacao_domicilios.pdf (accessed on 27 January 2023).
- Pereira, L.; Ximenes, R.A.A.; Braga, M.C.; Moreira, R.C. Estudo de Prevalência de Base Populacional das Infecções Pelos Vírus das Hepatites A, B e C nas Capitais do Brasil. Recife Ministério da Saúde—Organização Pan-Americana de Saúde: Parnamirim, Brazil, 2010; pp. 1–295. [Google Scholar]
- Ponde, R.A.A. Expression and detection of anti-HBs antibodies after hepatitis B virus infection or vaccination in the context of protective immunity. Arch. Virol. 2019, 164, 2645–2658. [Google Scholar] [CrossRef]
- Saco, T.V.; Strauss, A.T.; Ledford, D.K. Hepatitis B vaccine nonresponders: Possible mechanisms and solutions. Ann. Allergy Asthma Immunol. 2018, 121, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Junior, A.P.; de-Oliveira, E.C.; Martin, T.O.G.; Rodrigues Alves-Junior, E.; Silva, L.J.D.; Mello, F.C.D.A.; Fontes, C.J.F.; Souto, F.J.D. Prevalence of hepatitis B and D virus infection in a district of Mato Grosso, bordering Amazonas and Rondonia states. Rev. Soc. Bras. Med. Trop. 2020, 53, e20190559. [Google Scholar] [CrossRef]
- Villar, L.M.; Milagres, F.A.P.; Lampe, E.; Cruz, H.M.; Scalioni, L.P.; Magalhães, M.A.F.M.; Romão, A.R.; Gracie, R.; de Paula, V.S. Determination of hepatitis B, C and D prevalence among urban and Amerindian populations from the Eastern Brazilian Amazon: A cross sectional study. BMC Infect. Dis. 2018, 18, 411. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.D.S.U.; Morais, I.O.; Gonçalves, D.M.; De Matos, I.S.; Da Rocha, F.F.; Torres, G.M.D.N.; Da Costa, M.L.A.; Da Silva, S.S.; Da Silva, P.A.M.; Souza, R. Prevalência da infecção pelo vírus da hepatite B em um município do interior do estado do Acre, Amazônia Ocidental, Brasil. Rev. Pan-Amaz Saude 2017, 8, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Melardo, C.; Foglia, F.; Della Rocca, M.T.; Zaino, A.; Morone, M.V.; De Filippis, A.; Finamore, E.; Galdiero, M. Hepatitis B Virus prevalence and serological profiles in a hospital in Southern Italy. New Microbiol. 2022, 10, 45. [Google Scholar]
- Shadaker, S.; Sood, A.; Averhoff, F.; Suryaprasad, A.; Kanchi, S.; Midha, V.; Kamili, S.; Nasrullah, M.; Trickey, A.; Garg, R.; et al. Hepatitis B Prevalence and Risk Factors in Punjab, India: A Population-Based Serosurvey. J. Clin. Exp. Hepatol. 2022, 12, 1310–1319. [Google Scholar] [CrossRef]
- Daka, D.; Hailemeskel, G.; Fenta, D.A. Prevalence of Hepatitis B Virus infection and associated factors among female sex workers using respondent-driven sampling in Hawassa City, Southern Ethiopia. BMC Microbiol. 2022, 22, 37. [Google Scholar] [CrossRef] [PubMed]
- Rostam-Abadi, Y.; Rafiemanesh, H.; Gholami, J.; Shadloo, B.; Amin-Esmaeili, M.; Rahimi-Movaghar, A. Hepatitis B virus infection among people who use drugs in Iran: A systematic review, meta-analysis, and trend analysis. Harm Reduct. J. 2020, 17, 81. [Google Scholar] [CrossRef]
- Jeele, M.O.O.; Addow, R.O.B.; Adan, F.N.; Jimale, L.H. Prevalence and Risk Factors Associated with Hepatitis B and Hepatitis C Infections among Patients Undergoing Hemodialysis: A Single-Centre Study in Somalia. Int. J. Nephrol. 2021, 2021, 1555775. [Google Scholar] [CrossRef] [PubMed]
- Kasradze, A.; Shadaker, S.; Kuchuloria, T.; Gamkrelidze, A.; Nasrullah, M.; Gvinjilia, L.; Baliashvili, D.; Chitadze, N.; Kodani, M.; Tejada-Strop, A.; et al. The burden and epidemiology of hepatitis B and hepatitis D in Georgia: Findings from the national seroprevalence survey. Public Health 2020, 185, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Lian, D.S.; Yin, Y.Q.; Hu, D.; Wang, N.; Chen, L.S.; Wang, B. HIV prevalence and correlated factors among male clients of female sex workers in a border region of China. PLoS ONE 2019, 14, e0225072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hongjaisee, S.; Khamduang, W.; Sripan, P.; Choyrum, S.; Thepbundit, V.; Ngo-Giang-Huong, N.; Tangmunkongvorakul, A. Prevalence and factors associated with hepatitis B and D virus infections among migrant sex workers in Chiangmai, Thailand: A cross-sectional study in 2019. Int. J. Infect. Dis. 2020, 100, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Adeyemi, O.A.; Mitchell, A.; Shutt, A.; Crowell, T.A.; Ndembi, N.; Kokogho, A.; Ramadhani, H.O.; Robb, M.L.; Baral, S.D.; Ake, J.; et al. Hepatitis B virus infection among men who have sex with men and transgender women living with or at risk for HIV: A cross sectional study in Abuja and Lagos, Nigeria. BMC Infect. Dis. 2021, 21, 1–654. [Google Scholar] [CrossRef] [PubMed]
- Duric, P.; Rajcevic, S.; Ilic, S.; Milosevic, V.; Hintringer, K.; Fabri, M.; Ruzic, M.; Petrovic, V.; Petrovic, M.; Dragovac, G.; et al. Hepatitis B Outbreak Among Men Who Have Sex with Men in the Autonomous Province of Vojvodina, Serbia. LGBT Health 2018, 5, 91–93. [Google Scholar] [CrossRef]
- Persson, K.I.; Berglund, T.; Bergstrom, J.; Tikkanen, R.; Thorson, A.; Forsberg, B. Place and practice: Sexual risk behaviour while travelling abroad among Swedish men who have sex with men. Travel Med. Infect. Dis. 2018, 25, 58–64. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, C.; Silva, S.S.; Viera, J.J.S.; Barbosa, K.M.V.; Freitas, P.E.B.; Sarmento, V.P.; Soares, M.C.P.; Nunes, H.M. Soroprevalência das infecções pelos vírus das hepatites B e C e situação vacinal para o vírus da hepatite B em servidores da Polícia Rodoviária Federal, Estado do Pará, Brasil, 2013-2014. Rev. Pan-Amaz Saude 2017, 8, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde, Gabinete do Ministro. Portaria SAS/MS nº 249, de 16 de Abril de 2002. Aprova a Política Nacional de Saúde da Pessoa Idosa; Ministério da Saúde, Gabinete do Ministro: Brasília, Brazil, 2002. Available online: https://www.coffito.gov.br/nsite/?p=3372 (accessed on 27 January 2023).
- Bruce, M.G.; Bruden, D.; Hurlburt, D.; Zanis, C.; Thompson, G.; Rea, L.; Toomey, M.; Townshend-Bulson, L.; Rudolph, K.; Bulkow, L.; et al. Antibody Levels and Protection After Hepatitis B Vaccine: Results of a 30-Year Follow-up Study and Response to a Booster Dose. J. Infect. Dis. 2016, 214, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Cocchio, S.; Baldo, V.; Volpin, A.; Fonzo, M.; Floreani, A.; Furlan, P.; Mason, P.; Trevisan, A.; Scapellato, M.L. Persistence of Anti-Hbs after up to 30 Years in Health Care Workers Vaccinated against Hepatitis B Virus. Vaccines 2021, 9, 323. [Google Scholar] [CrossRef]
- Drummond, G.R.; Vinh, A.; Guzik, T.J.; Sobey, C.G. Immune mechanisms of hypertension. Nat. Rev. Immunol. 2019, 19, 517–532. [Google Scholar] [CrossRef] [PubMed]
- Kwetkat, A.; Heppner, H.J. Comorbidities in the Elderly and Their Possible Influence on Vaccine Response. Interdiscip. Top Gerontol. Geriatr. 2020, 43, 73–85. [Google Scholar] [CrossRef]
- Van Der Meeren, O.; Crasta, P.; Cheuvart, B.; De Ridder, M. Characterization of an age-response relationship to GSK’s recombinant hepatitis B vaccine in healthy adults: An integrated analysis. Hum. Vaccines Immunother. 2015, 11, 1726–1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, J.K.; Jeevan-Raj, B.; Netter, H.J. Hepatitis B Virus (HBV) Subviral Particles as Protective Vaccines and Vaccine Platforms. Viruses 2020, 12, 126. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Zhou, X.; Zhou, Y.H. Hepatitis B vaccine development and implementation. Hum. Vaccines Immunother. 2020, 16, 1533–1544. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, J.; Chen, X.; Yu, M.; Yu, S.; Sun, Y.; Duan, J.; Sun, H.; Yuan, P. Short-term immunogenicity of standard and accelerated hepatitis B virus vaccination schedules in healthy adults: A comparative field study in China. Biosci. Rep. 2018, 38, BSR20180846. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Bivariate Analysis | Multiple Analysis **** | ||||||
|---|---|---|---|---|---|---|---|---|
| HBV (n = 682) | ||||||||
| Total | Positive | Negative | p | OR * (CI 95% **) | p | OR * (CI 95% **) | ||
| n= 682 (%) | n =113 (%) | n = 569 (%) | ||||||
| Sex | 0.094 | 0.094 | ||||||
| Male | 214 (31.4) | 43 (20.0) | 171 (80.0) | 1 | ||||
| Female | 468 (68.6) | 70 (15.0) | 398 (85.0) | 0.69 (0.46−1.06) | ||||
| Age | 0.135 | |||||||
| 50–59 years old | 266 (39.0) | 37 (86.1) | 229 (13.9) | 1 | ||||
| ≥60 years | 416 (61.0) | 76 (18.3) | 340 (81.7) | 1.38 (0.90−2.12) | ||||
| City of Origin | 0.514 | |||||||
| Capital | 339 (49.7) | 53 (15.6) | 286 (84.4) | 1 | ||||
| Interior | 343 (50.3) | 60 (17.5) | 283 (82.5) | 1.14 (0.76−1.71) | ||||
| Education/(NI = 5) *** | 0.168 | |||||||
| > 9 years | 184 (27.2) | 24 (12.5) | 161 (87.5) | 1 | ||||
| 5–9 years | 183 (27.0) | 30 (18.4) | 153 (81.6) | 1.37 (0.76−2.47) | ||||
| <5 years | 310 (45.8) | 59 (19.0) | 251 (81.0) | 1.65 (0.98−2.77) | ||||
| Internet | 0.104 | |||||||
| No | 369 (54.1) | 69 (18.7) | 300 (81.3) | 1 | ||||
| Yes | 313 (45.9) | 44 (14.1) | 269 (85.9) | 0.71 (0.47−1.1) | ||||
| Religion/(NI = 2) *** | 0.092 | |||||||
| Without religion | 33 (4.9) | 9 (27.3) | 24 (72.7) | 1 | ||||
| Religious | 647 (95.1) | 104 (16.1) | 543 (83.9) | 0.51 (0.23−1.13) | ||||
| Self-declared color | 0.795 | |||||||
| White | 236 (34.6) | 39 (16.5) | 197 (83.5) | 1 | ||||
| Brown and Black | 135 (63.8) | 73 (16.8) | 362 (83.2) | 1.02 (0.67−1.56) | ||||
| Yellow (Eastern) and Red (Indigenous) | 11 (1.6) | 1 (9.1) | 10 (90.9) | 0.51 (0.63−4.06) | ||||
| Marital Status/(NI = 1) *** | 0.982 | |||||||
| Married/Stable union | 373 (54.8) | 62 (16.6) | 311 (83.4) | 1 | ||||
| Single/Separated/Widowed | 308 (45.2) | 51 (16.6) | 257 (83.4) | 0.99 (0.66−1.49) | ||||
| Use of illicit drugs in life/(NI = 6) *** | 0.518 | |||||||
| No | 658 (97.3) | 111 (16.9) | 547 (83.1) | 1 | ||||
| Yes | 18 (2.7) | 2 (11.1) | 16 (88.9) | 0.62 (0.14−2.72) | ||||
| Use of alcohol in the last 12 months/(NI = 6) *** | 0.225 | |||||||
| No | 492 (72.8) | 77 (15.7) | 415 (84.3) | 1 | ||||
| Yes | 184 (27.2) | 36 (19.6) | 148 (80.4) | 1.31 (0.85−2.03) | ||||
| History of incarceration/(NI = 7) *** | 0.141 | |||||||
| No | 635 (94.1) | 102 (16.1) | 533 (83.9) | 1 | ||||
| Yes | 40 (5.9) | 10 (25.0) | 30 (75.0) | 1.74 (0.83−3.67) | ||||
| Age of first sexual intercourse/(NI = 17) *** | 0.087 | |||||||
| >=16 years | 491 (73.8) | 74 (15.1) | 417 (84.9) | 1 | ||||
| <15 years | 174 (26.2) | 36 (20.7) | 138 (79.3) | 1.47 (0.94−2.29) | ||||
| Number of sexual partners in the last 12 months/(NI = 8) *** | 0.627 | |||||||
| Did not have sexual intercourse | 244 (36.2) | 36 (14.8) | 208 (85.2) | 1 | ||||
| One partner | 361 (53.6) | 62 (17.2) | 299 (82.8) | 1.20 (0.77−1.87) | ||||
| Two or more partners | 69 (10.2) | 13 (18.8) | 56 (81.2) | 1.34 (0.66–2.70) | ||||
| Condom use at last sexual intercourse/(NI = 25) *** | 0.571 | |||||||
| Yes | 71 (10.8) | 10 (14.1) | 61 (85.9) | 1 | ||||
| No | 586 (89.2) | 98 (16.7) | 488 (83.3) | 1.23 (0.61−2.47) | ||||
| Use of lubricant/NI (n = 78) *** | 0.235 | |||||||
| Yes | 154 (25.5) | 21 (13.6) | 133 (86.4) | 1 | ||||
| No | 450 (74.5) | 80 (17.8) | 370 (82.2) | 1.37 (0.81−2.30) | ||||
| Received money or paid in exchange for sex/(NI = 9) *** | 0.046 | |||||||
| No | 585 (86.9) | 90 (15.4) | 495 (84.6) | 1 | ||||
| Yes | 88 (13.1) | 21 (23.9) | 67 (76.1) | 1.72 (1.01−2.96) | ||||
| Sexual intercourse with a person of the same sex/(NI = 11) *** | 0.017 | 0.059 | ||||||
| No | 659 (98.2) | 105 (15.9) | 554 (84.1) | 1 | 1 | |||
| Yes | 12 (1.8) | 5 (41.7) | 7 (58.3) | 3.77 (1.17−12.10) | 3.15 (0.96−10.35) | |||
| History of sexual intercourse with a sex worker/(NI = 10) *** | 0.006 | 0.013 | ||||||
| No | 572 (85.1) | 85 (14.9) | 487 (85.1) | 1 | 1 | |||
| Yes | 100 (14.9) | 26 (26.0) | 74 (74.0) | 2.01 (1.22−3.33) | 1.94 (1.15−3.28) | |||
| History of genital sores/(NI = 5) *** | 0.038 | |||||||
| No | 611 (90.3) | 96 (15.7) | 515 (84.3) | 1 | ||||
| Yes | 66 (9.7) | 17 (25.8) | 49 (74.2) | 1.86 (1.03−3.37) | ||||
| History of blisters on genitalia/(NI = 5) *** | 0.169 | |||||||
| No | 641 (94.7) | 104 (16.2) | 537 (83.8) | 1 | ||||
| Yes | 36 (5.3) | 9 (25.0) | 27 (75.0) | 1.72 (0.79−3.77) | ||||
| History of genital warts/(NI = 6) *** | 0.103 | |||||||
| No | 628 (92.9) | 100 (15.9) | 528 (84.1) | 1 | ||||
| Yes | 48 (7.1) | 12 (25.0) | 36 (75.0) | 1.76 (0.89−3.50) | ||||
| Victim of sexual violence/(NI = 4) *** | 0.311 | |||||||
| No | 644 (94.8) | 105 (16.3) | 539 (83.7) | 1 | ||||
| Yes | 35 (5.2) | 8 (22.9) | 27 (77.1) | 1.52 (0.67−3.44) | ||||
| Hospitalization history/(NI = 2) *** | 0.777 | |||||||
| No | 62 (9.1) | 11 (17.7) | 51 (82.3) | 1 | ||||
| Yes | 618 (90.9) | 101 (16.3) | 517 (83.7) | 0.91 (0.46−1.80) | ||||
| Seen a dentist/(NI = 11) *** | 0.851 | |||||||
| No | 344 (51.3) | 56 (16.3) | 288 (83.7) | 1 | ||||
| Yes | 327 (48.7) | 55 (16.8) | 272 (83.2) | 1.03 (0.69−1.56) | ||||
| History of hemodialysis/(NI = 7) *** | 0.650 | |||||||
| No | 671 (99.4) | 111 (16.5) | 560 (83.5) | 1 | ||||
| Yes | 4 (0.6) | 1 (25.0) | 3 (75.0) | 1.68 (0.17−16.32) | ||||
| History of blood transfusion/(NI = 7) *** | 0.176 | |||||||
| No | 560 (83.0) | 88 (15.7) | 472 (84.3) | 1 | ||||
| Yes | 115 (17.0) | 24 (20.9) | 91 (79.1) | 1.41 (0.85−2.34) | ||||
| Shared sharp personal hygiene object/(NI = 2) *** | 0.671 | |||||||
| No | 316 (46.5) | 50 (15.8) | 266 (84.2) | 1 | ||||
| Yes | 364 (53.5) | 62 (17.9) | 302 (82.1) | 1.09 (0.73−1.64) | ||||
| Variables | Isolated anti-HBs Titers | p | ||
|---|---|---|---|---|
| Total n = 147 (%) | <10 mUI/mL n = 101 (%) | ≥10 mUI/mL n = 46 (%) | ||
| Sex | 0.092 | |||
| Male | 46 (31.3) | 36 (78.3) | 10 (21.7) | |
| Female | 101 (68.7) | 65 (64.4) | 36 (35.6) | |
| Age | 0.002 | |||
| 50–59 years old | 59 (40.1) | 32 (54.2) | 27 (45.8) | |
| ≥60 years | 88 (59.9) | 69 (78.4) | 19 (21.6) | |
| Self-declared color | 0.067 | |||
| White | 61 (41.5) | 37 (60.7) | 24 (39.3) | |
| Brown and Black | 85 (57.8) | 63 (74.1) | 22 (25.9) | |
| Yellow (Eastern) and Red (Indigenous) | 1 (0.7) | 1 (100.0) | 0 | |
| Body Mass Index (kg/m2) (NI = 43) * | 0.464 | |||
| Malnutrition (<22) | 14 (13.4) | 9 (64.3) | 5 (35.7) | |
| Eutrophy (22–26) | 48 (46.2) | 30 (62.5) | 18 (37.5) | |
| Obesity (>27) | 42 (40.4) | 30 (71.4) | 12 (28.6) | |
| Systemic Arterial Hypertension (NI = 1) * | 0.007 | |||
| No/Don’t know | 62 (42.5) | 35 (56.5) | 27 (43.5) | |
| Yes | 84 (57.5) | 65 (77.4) | 19 (22.6) | |
| Diabetes Mellitus | 0.760 | |||
| No/Don’t know | 116 (78.9) | 79 (68.1) | 37 (31.9) | |
| Yes | 31 (21.1) | 22 (71.0) | 9 (29.0) | |
| Never smoked a cigarette/tobacco (NI = 2) | 0.072 | |||
| No | 111 (76.6) | 74 (66.7) | 37 (33.3) | |
| Yes | 34 (23.4) | 25 (73.5) | 9 (26.5) | |
| Currently smokes cigarettes/tobacco (NI = 2) | 0.452 | |||
| No | 111 (76.6) | 74 (66.7) | 37 (33.3) | |
| Yes | 34 (23.4) | 25 (73.5) | 9 (26.5) | |
| Time after last vaccine dose (years) | 0.783 | |||
| 147 | 101 (68.7) | 46 (31.3) | ||
| Mean (standard deviation) | 5.93 (5.003) | 5.74 (4.915) | ||
| Variables | Total n = 434 (%) | Intervention Regimen (40 mg/mL) n = 217 (%) | Comparison Regimen (20 mg/mL) n = 217 (%) | p |
|---|---|---|---|---|
| Sex | 0.466 | |||
| Male | 133 (30.6) | 63 (47.4) | 70 (52.6) | |
| Female | 301 (69.4) | 154 (51.2) | 147 (48.8) | |
| Age 63.9 (8.8) * | 0.920 | |||
| 50–59 years old | 157 (36.2) | 78 (49.7) | 79 (50.3) | |
| 60–97 years old | 277 (63.8) | 139 (50.2) | 138 (49.8) | |
| Marital status/(NI = 1) ** | 0.965 | |||
| Married/Stable Union | 239 (55.2) | 119 (49.8) | 120 (50.2) | |
| Single/Separated/Widowed | 194 (44.8) | 97 (50.0) | 97 (50.0) | |
| Education 6.1 (4.6) */(NI= 5) ** | 0.607 | |||
| <5 years | 207 (48.3) | 102 (50.7) | 102 (49.3) | |
| 5–9 years | 116 (27.0) | 56 (48.3) | 60 (51.7) | |
| >9 years | 106 (24.7) | 56 (52.8) | 50 (47.2) | |
| Self-declared race | 0.181 | |||
| White | 139 (32.0) | 76 (54.7) | 63 (45.3) | |
| Brown and black | 286 (65.9) | 137 (47.9) | 149 (52.1) | |
| Yellow (Eastern) and Red (Indigenous) | 9 (2.1) | 4 (44.4) | 5 (55.6) | |
| Systemic Arterial Hypertension/(NI = 2) ** | 0.568 | |||
| No | 163 (37.7) | 84 (51.5) | 79 (48.5) | |
| Yes | 269 (62.3) | 131 (48.7) | 138 (51.3) | |
| Diabetes Mellitus/(NI = 3) ** | 0.375 | |||
| No | 331 (76.8) | 169 (51.1) | 162 (48.9) | |
| Yes | 100 (23.2) | 46 (46.0) | 54 (54.0) | |
| Body Mass Index (kg/m2)/(NI = 17) * | 0.854 | |||
| Malnutrition (< 22) | 69 (16.6) | 35 (50.7) | 34 (49.3) | |
| Eutrophy (22–27) | 166 (39.8) | 83 (50.0) | 83 (50.0) | |
| Obesity (>27) | 182 (43.6) | 90 (50.5) | 92 (49.5) | |
| Ever smoked cigarette/tobacco in life/(NI = 43) * | 0.277 | |||
| No | 219 (56.0) | 105 (47.9) | 114 (52.1) | |
| Yes | 172 (44.0) | 92 (53.5) | 80 (46.5) | |
| Current smoker/tobacco/(NI = 11) * | 0.683 | |||
| No | 366 (86.5) | 182 (49.7) | 184 (50.3) | |
| Yes | 57 (13.5) | 30 (52.6) | 27 (47.4) |
| Parameter | Intervention Regimen (40 mg/mL) n = 124 | Comparison Regimen(20 mg/mL)n = 114 | p | ||
|---|---|---|---|---|---|
| n (%) | IC 95% * | n (%) | IC 95% * | ||
| Seroconversion | 0.952 | ||||
| 0 mUl/mL | 1 (0.8) | (0.0−3.0) | 1 (0.9) | (0.2−4.1) | |
| ≥1 mUl/mL | 123 (99.2) | (95.6−99.9) | 113 (99.1) | (95.2−99.8) | |
| Seroprotection | 0.007 | ||||
| <10 mUl/mL | 5 (4.0) | (1.7−9.1) | 16 (14.0) | (8.8−21.6) | |
| ≥10 mUl/mL | 119 (96.0) | (90.9−98.3) | 98 (86.0) | (78.4−91.2) | |
| GMT ** | 0.007 | ||||
| 518.2 | (456.0–580.4) | 260.2 | (183.5−336.9) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Cunha Rosa, L.R.; Brandão, L.G.V.A.; Moura, W.É.A.; Campos, L.R.; Pessoni, G.C.; de Oliveira Roque e Lima, J.; de Moraes, J.C.; dos Santos Carneiro, M.A.; Teles, S.A.; Caetano, K.A.A. Prevalence, Risk Factors and Vaccine Response against Hepatitis B in People Aged 50 Years or Older. Vaccines 2023, 11, 597. https://doi.org/10.3390/vaccines11030597
da Cunha Rosa LR, Brandão LGVA, Moura WÉA, Campos LR, Pessoni GC, de Oliveira Roque e Lima J, de Moraes JC, dos Santos Carneiro MA, Teles SA, Caetano KAA. Prevalence, Risk Factors and Vaccine Response against Hepatitis B in People Aged 50 Years or Older. Vaccines. 2023; 11(3):597. https://doi.org/10.3390/vaccines11030597
Chicago/Turabian Styleda Cunha Rosa, Luana Rocha, Leyla Gabriela Verner Amaral Brandão, Winny Éveny Alves Moura, Lays Rosa Campos, Grécia Carolina Pessoni, Juliana de Oliveira Roque e Lima, José Cássio de Moraes, Megmar Aparecida dos Santos Carneiro, Sheila Araújo Teles, and Karlla Antonieta Amorim Caetano. 2023. "Prevalence, Risk Factors and Vaccine Response against Hepatitis B in People Aged 50 Years or Older" Vaccines 11, no. 3: 597. https://doi.org/10.3390/vaccines11030597