

Estimating the Global Spread of Epidemic Human Monkeypox with Bayesian Directed Acyclic Graphic Model

Abstract
:1. Introduction
2. Materials and Methods
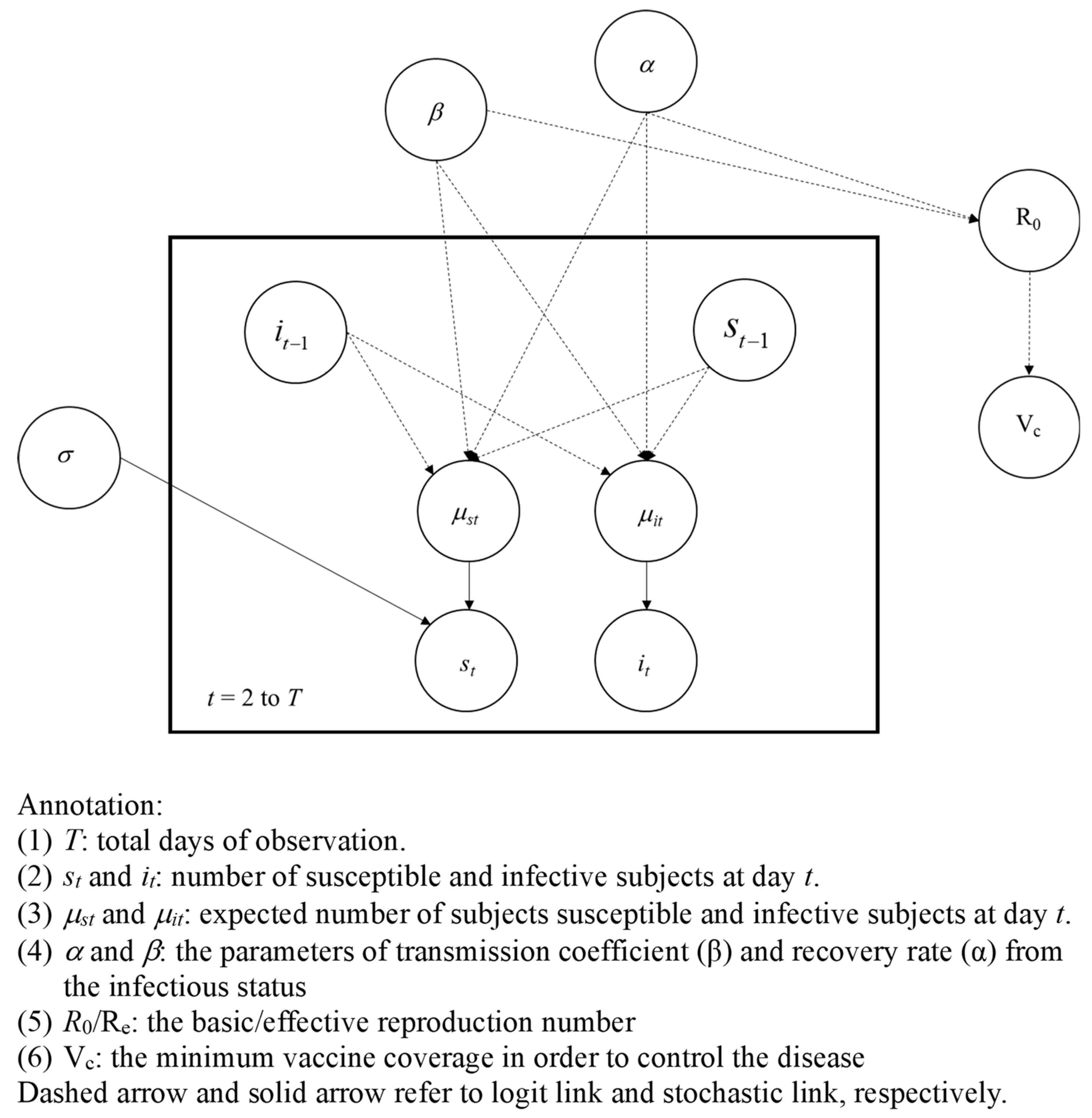
Bayesian SIR Model
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Magnus, P.V.; Andersen, E.K.; Petersen, K.B.; Birch-Andersen, A. A pox-like disease in cynomolgus monkeys. Acta Path Microbiol. Scand. 1959, 46, 156–176. [Google Scholar] [CrossRef]
- Breman, J.G.; Kalisa, R.; Steniowski, M.V.; Zanotto, E.; Gromyko, A.I.; Arita, I. Human monkeypox, 1970–1979. Bull. World Health Organ. 1980, 58, 165–182. [Google Scholar] [PubMed]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox-A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- Jezek, Z.; Grab, B.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M. Clinico-epidemiological features of monkeypox patients with an animal or human source of infection. Bull. World Health Organ. 1988, 66, 459–464. [Google Scholar] [PubMed]
- Aplogan, A.; Szczeniowski, M. Human monkeypox—Kasai Oriental, Democratic Republic of Congo, February 1996–October 1997. MMWR Morb. Mortal. Wkly. Rep. 1997, 46, 1168–1171. [Google Scholar]
- WHO. Multi-Country Monkeypox Outbreak: Situation Update. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396 (accessed on 7 August 2022).
- CDC. 2022 U.S. Map & Case Count. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/us-map.html (accessed on 7 August 2022).
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Suarez Rodriguez, B.; Guzman Herrador, B.R.; Diaz Franco, A.; Sanchez-Seco Farinas, M.P.; Del Amo Valero, J.; Aginagalde Llorente, A.H.; de Agreda, J.; Malonda, R.C.; Castrillejo, D.; Chirlaque Lopez, M.D.; et al. Epidemiologic Features and Control Measures during Monkeypox Outbreak, Spain, June 2022. Emerg. Infect. Dis. 2022, 28, 1847–1851. [Google Scholar] [CrossRef] [PubMed]
- Farahat, R.A.; Abdelaal, A.; Shah, J.; Ghozy, S.; Sah, R.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J.; McHugh, T.D.; Leblebicioglu, H. Monkeypox outbreaks during COVID-19 pandemic: Are we looking at an independent phenomenon or an overlapping pandemic? Ann. Clin. Microbiol. Antimicrob. 2022, 21, 26. [Google Scholar] [CrossRef] [PubMed]
- Loconsole, D.; Sallustio, A.; Centrone, F.; Casulli, D.; Accogli, M.; Saracino, A.; Foti, C.; Grandolfo, M.; Buccoliero, G.B.; Vitale, V.; et al. Monkeypox Virus Infections in Southern Italy: Is There a Risk for Community Spread? Int. J. Environ. Res. Public Health 2022, 19, 11719. [Google Scholar] [CrossRef] [PubMed]
- The Global Health Team. Monkeypox 2022 Global Epidemiology; Report 2022-08-05. Available online: https://www.monkeypox.global.health/ (accessed on 7 August 2022).
- Kraemer, M.U.G.; Tegally, H.; Pigott, D.M.; Dasgupta, A.; Sheldon, J.; Wilkinson, E.; Schultheiss, M.; Han, A.; Oglia, M.; Marks, S.; et al. Tracking the 2022 monkeypox outbreak with epidemiological data in real-time. Lancet Infect. Dis. 2022, 22, 941–942. [Google Scholar] [CrossRef] [PubMed]
- Kermack, W.O.; McKendrick, A.G. A Contribution to the Mathematical Theory of Epidemics. Proc. R. Soc. London Ser. A Math. Phys. Eng. Sci. 1927, 115, 700–721. [Google Scholar]
- Plans-Rubio, P. Percentages of Vaccination Coverage Required to Establish Herd Immunity against SARS-CoV-2. Vaccines 2022, 10, 736. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Hsu, C.Y.; Jen, H.H.; Yen, A.M.; Chan, C.C.; Chen, H.H. The Bayesian Susceptible-Exposed-Infected-Recovered model for the outbreak of COVID-19 on the Diamond Princess Cruise Ship. Stoch. Environ. Res. Risk Assess. 2021, 35, 1319–1333. [Google Scholar] [CrossRef] [PubMed]
- Miura, F.; van Ewijk, C.E.; Backer, J.A.; Xiridou, M.; Franz, E.; Op de Coul, E.; Brandwagt, D.; van Cleef, B.; van Rijckevorsel, G.; Swaan, C.; et al. Estimated incubation period for monkeypox cases confirmed in the Netherlands, May 2022. Eurosurveillance 2022, 27, 2200448. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Shao, Z.; Bai, Y.; Wang, L.; Herrera-Diestra, J.L.; Fox, S.J.; Ertem, Z.; Lau, E.H.Y.; Cowling, B.J. Reproduction number of monkeypox in the early stage of the 2022 multi-country outbreak. J. Travel Med. 2022, 29, taac099. [Google Scholar] [CrossRef] [PubMed]
- Gani, R.; Leach, S. Transmission potential of smallpox in contemporary populations. Nature 2001, 414, 748–751. [Google Scholar] [CrossRef] [PubMed]
- Rimoin, A.W.; Mulembakani, P.M.; Johnston, S.C.; Lloyd Smith, J.O.; Kisalu, N.K.; Kinkela, T.L.; Blumberg, S.; Thomassen, H.A.; Pike, B.L.; Fair, J.N.; et al. Major increase in human monkeypox incidence 30 years after smallpox vaccination campaigns cease in the Democratic Republic of Congo. Proc. Natl. Acad. Sci. USA 2010, 107, 16262–16267. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Country/Areas | The Periods | The Deterministic SIR Model | ||
|---|---|---|---|---|
| β | R0/Re | Vc(%) | ||
| The Globe | 31 January~30 April | 0.132 | 1.119 | 11 |
| 1 May~31 May | 0.265 | 2.251 | 56 | |
| 1 June~30 June | 0.180 | 1.532 | 35 | |
| 1 July~31 July | 0.149 | 1.271 | 21 | |
| 1 August~31 August | 0.136 | 1.153 | 13 | |
| 1 September~23 September | 0.096 | 0.817 | - | |
| United States | 18 May~30 June | 0.245 | 2.086 | 52 |
| 1 July~30 July | 0.184 | 1.568 | 36 | |
| 1 August~31 August | 0.145 | 1.229 | 19 | |
| 1 September~23 September | 0.080 | 0.677 | - | |
| Spain | 18 May~16 June | 0.242 | 2.057 | 51 |
| 17 June~16 July | 0.15318 | 1.302 | 23 | |
| 17 July~31 August | 0.11767 | 1.000 | - | |
| 1 September~23 September | 0.0523 | 0.445 | - | |
| Brazil | 8 June~7 July | 0.276 | 2.346 | 57 |
| 8 July~6 August | 0.1882 | 1.600 | 38 | |
| 7 August~31 August | 0.1271 | 1.080 | 7 | |
| 1 September~23 September | 0.1077 | 0.915 | ||
| United Kingdom | 8 June~7 July | 0.286 | 2.432 | 59 |
| 8 July~6 August | 0.154 | 1.312 | 24 | |
| 7 August~31 August | 0.113 | 0.964 | ||
| 1 September~23 September | 0.055 | 0.470 | ||
| Democratic Republic of the Congo | 8 May~5 June | 0.118 | 1.407 | 29 |
| 6 June~28 July | 0.067 | 0.568 | ||
| 28 July~7 August | 0.329 | 2.797 | 64 | |
| Data | Total Cases | Estimated by the Bayesian SIR Model | ||||
|---|---|---|---|---|---|---|
| The Periods | β (95% CI) | α (95% CI); Reciprocal α (95% CI) | R0/Re (95% CI) | Vc (%) (95% CI) | ||
| The Globe | 65,215 | 31 January~30 April | 0.374 (0.368–0.384) | 0.373 (0.373–0.374); | 1.001 (0.986–1.150) | - |
| 1 May~31 May | 0.545 (0.511–0.563) | 1.459 (1.370–1.507) | 31.4 (27.0–33.6) | |||
| 1 June~31 July | 0.420 (0.419–0.421) | 1.125 (1.123–1.127) | 11.1 (10.9–11.3) | |||
| 1 August~23 September | 0.383 (0.383–0.384) | 2.678 (2.677–2.680) | 1.027 (1.026–1.028) | 2.6 (2.5–2.7) | ||
| United States | 24,403 | 17 May~30 June | 0.583 (0.581–0.589) | 0.487 (0.485–0.490); | 1.198 (1.197–1.201) | 16.5 (16.4–16.7) |
| 1 July~30 July | 0.567 (0.563–0.569) | 1.164 (1.149–1.169) | 14.1 (13.0–14.5) | |||
| 31 July~31 August | 0.499 (0.493–0.516) | 1.024 (1.016–1.052) | 2.3 (1.6–4.9) | |||
| 1 September~23 September | 0.407 (0.192–0.452) | 2.054 (2.039–2.061) | 0.837 (−0.391–0.929) | - | ||
| Spain | 7083 | 18 May~16 June | 0.480 (0.478–0.483) | 0.403 (0.400–0.405); | 1.191(1.189–1.194) | 16.0 (15.9–16.2) |
| 17 June~16 July | 0.454 (0.451–0.457) | 1.126 (1.124–1.129) | 11.2 (11.0–11.4) | |||
| 17 July~31 August | 0.389 (0.386–0.391) | 0.963 (0.961–0.966) | - | |||
| 1 September~23 September | 0.298 (0.278–0.316) | 2.479 (2.467–2.498) | 0.739 (0.690–0.784) | - | ||
| Brazil | 7300 | 8 June~7 July | 0.489 (0.487–0.492) | 0.365 (0.363–0.368); | 1.341 (1.337–1.345) | 25.4 (25.2–25.6) |
| 8 July~6 August | 0.435 (0.433–0.439) | 1.193 (1.189–1.197) | 16.2 (15.9–14.4) | |||
| 7 August~23 September | 0.362 (0.359–0.365) | 2.740 (2.717–2.758) | 0.992 (0.990–0.994) | - | ||
| United Kingdom | 3585 | 8 June~7 July | 0.542 (0.539–0.545) | 0.408 (0.405–0.411); | 1.330 (1.326–1.334) | 24.8 (24.7–25.0) |
| 8 July~6 August | 0.437 (0.433–0.440) | 1.071 (1.067–1.074) | 6.6 (6.3–6.9) | |||
| 7 August~31 August | 0.395 (0.392–0.398) | 0.969 (0.966–0.972) | - | |||
| 1 September~23 September | 0.181 (0.115–0.280) | 2.453 (2.436–2.472) | 0.443 (0.284–0.687) | - | ||
| Democratic Republic of the Congo | 195 | 8 May~5 June | 0.482 (0.463–0.497) | 0.397 (0.376–0.415) | 1.216 (1.199–1.235) | 17.8 (16.6–19.0) |
| 6 June~28 July | 0.334 (0.313–0.358) | 0.841 (0.816–0.864) | ||||
| 29 July~7 August | 0.847 (0.794–0.903) | 2.136 (2.011–2.284) | 53.2 (56.2–78.3) | |||
| After 8 August | 0.005 (0.000–0.033) | 2.524 (2.412–2.662) | 0.013 (0.000–0.083) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, L.-C.; Hsu, C.-Y.; Chen, H.-H.; Lai, C.-C. Estimating the Global Spread of Epidemic Human Monkeypox with Bayesian Directed Acyclic Graphic Model. Vaccines 2023, 11, 468. https://doi.org/10.3390/vaccines11020468
Liao L-C, Hsu C-Y, Chen H-H, Lai C-C. Estimating the Global Spread of Epidemic Human Monkeypox with Bayesian Directed Acyclic Graphic Model. Vaccines. 2023; 11(2):468. https://doi.org/10.3390/vaccines11020468
Chicago/Turabian StyleLiao, Ling-Chun, Chen-Yang Hsu, Hsiu-Hsi Chen, and Chao-Chih Lai. 2023. "Estimating the Global Spread of Epidemic Human Monkeypox with Bayesian Directed Acyclic Graphic Model" Vaccines 11, no. 2: 468. https://doi.org/10.3390/vaccines11020468