
Impact of BNT162b2 Booster Dose on SARS-CoV-2 Anti-Trimeric Spike Antibody Dynamics in a Large Cohort of Italian Health Care Workers
 ,
,  , , , , ,
, , , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
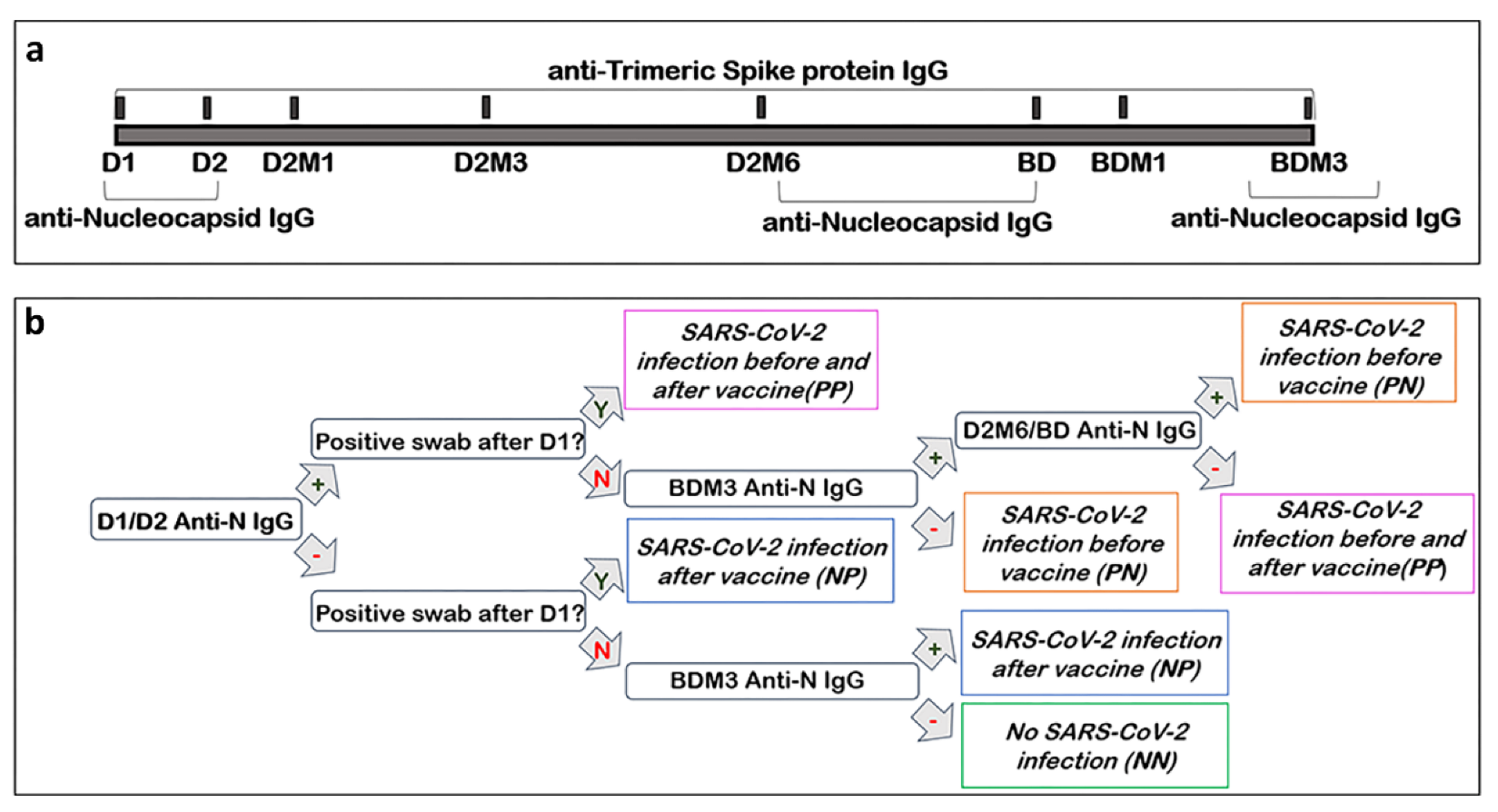
2.1. Study Design
2.2. Specimens Collection and Biobanking
2.3. Quantitative Analysis of Anti-Trimeric Spike IgG antibodies
2.4. Qualitative Assessment of Anti-Nucleocapsid IgG Antibodies
2.5. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Anti-Trimeric Spike IgG Titer Dynamic throughout Vaccination Campaign
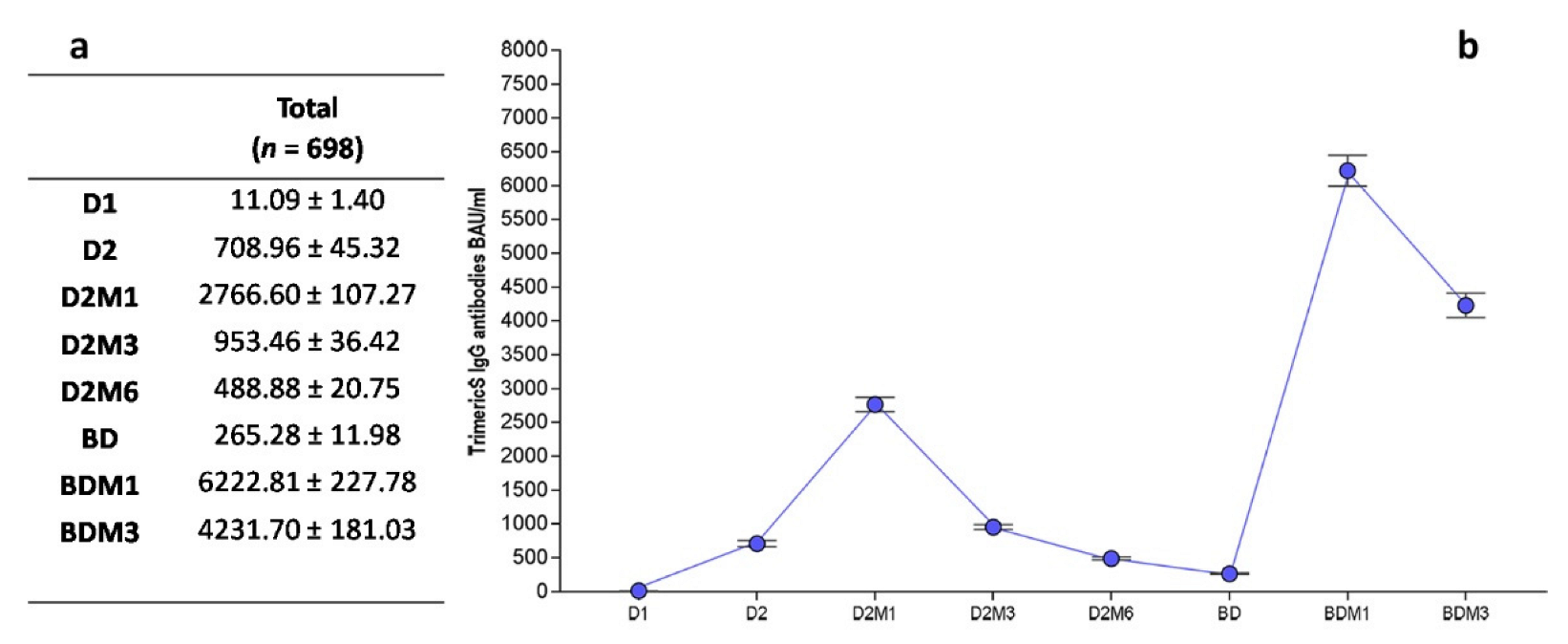
3.2.1. Overall Dynamic of Anti-Trimeric Spike IgG
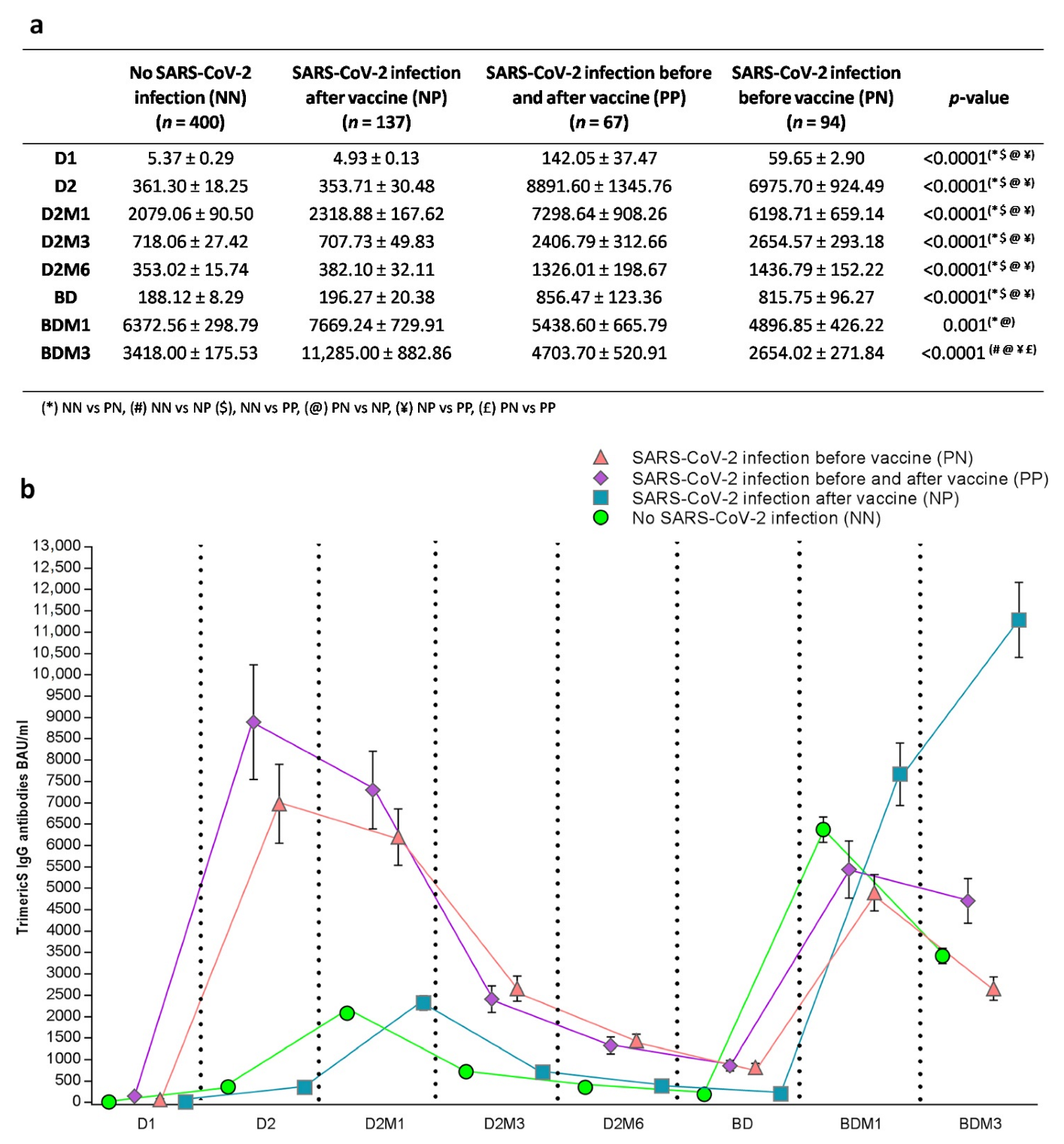
3.2.2. Anti-Trimeric Spike IgG Titer Dynamic According to SARS-CoV-2 Infection Status
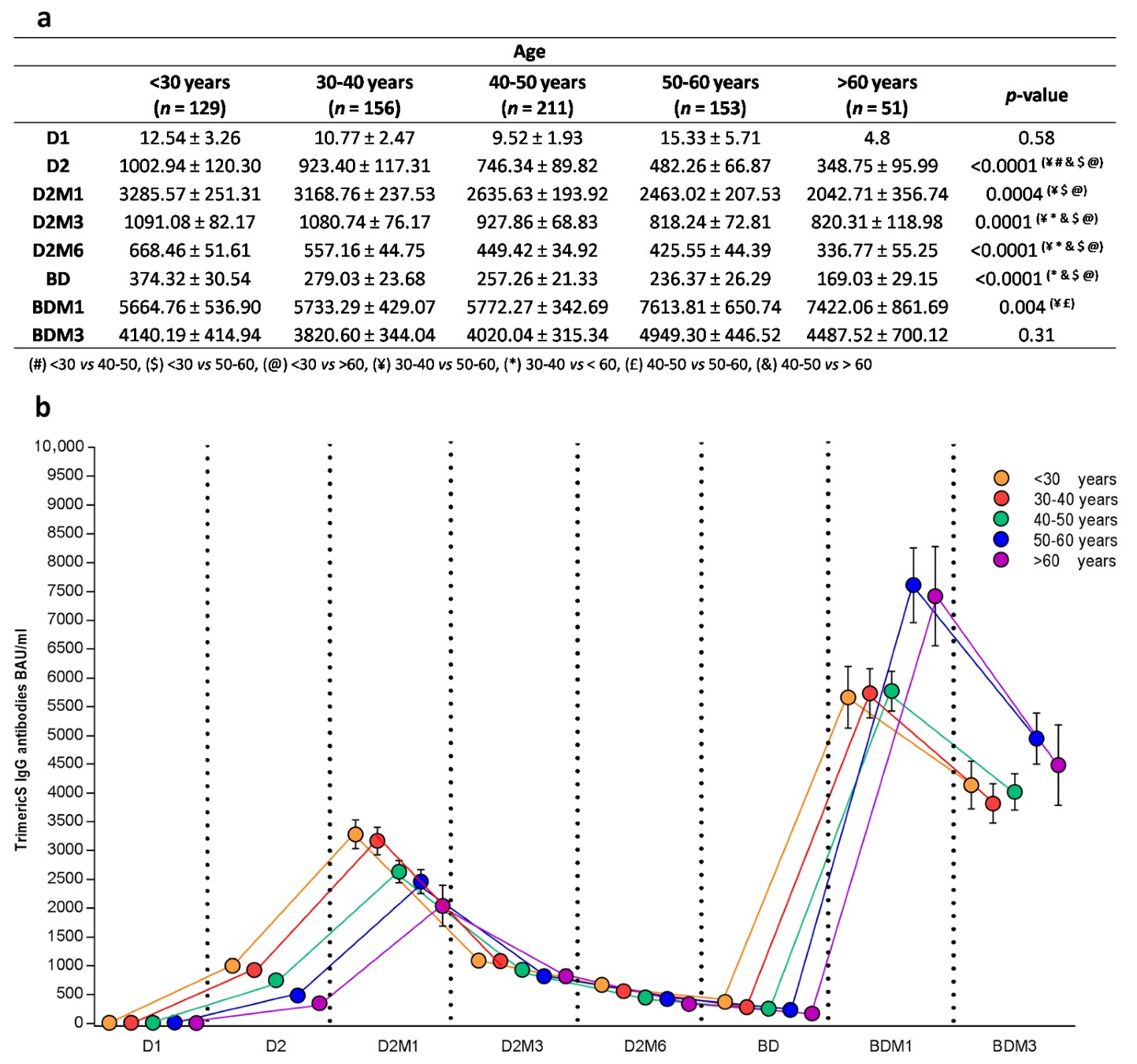
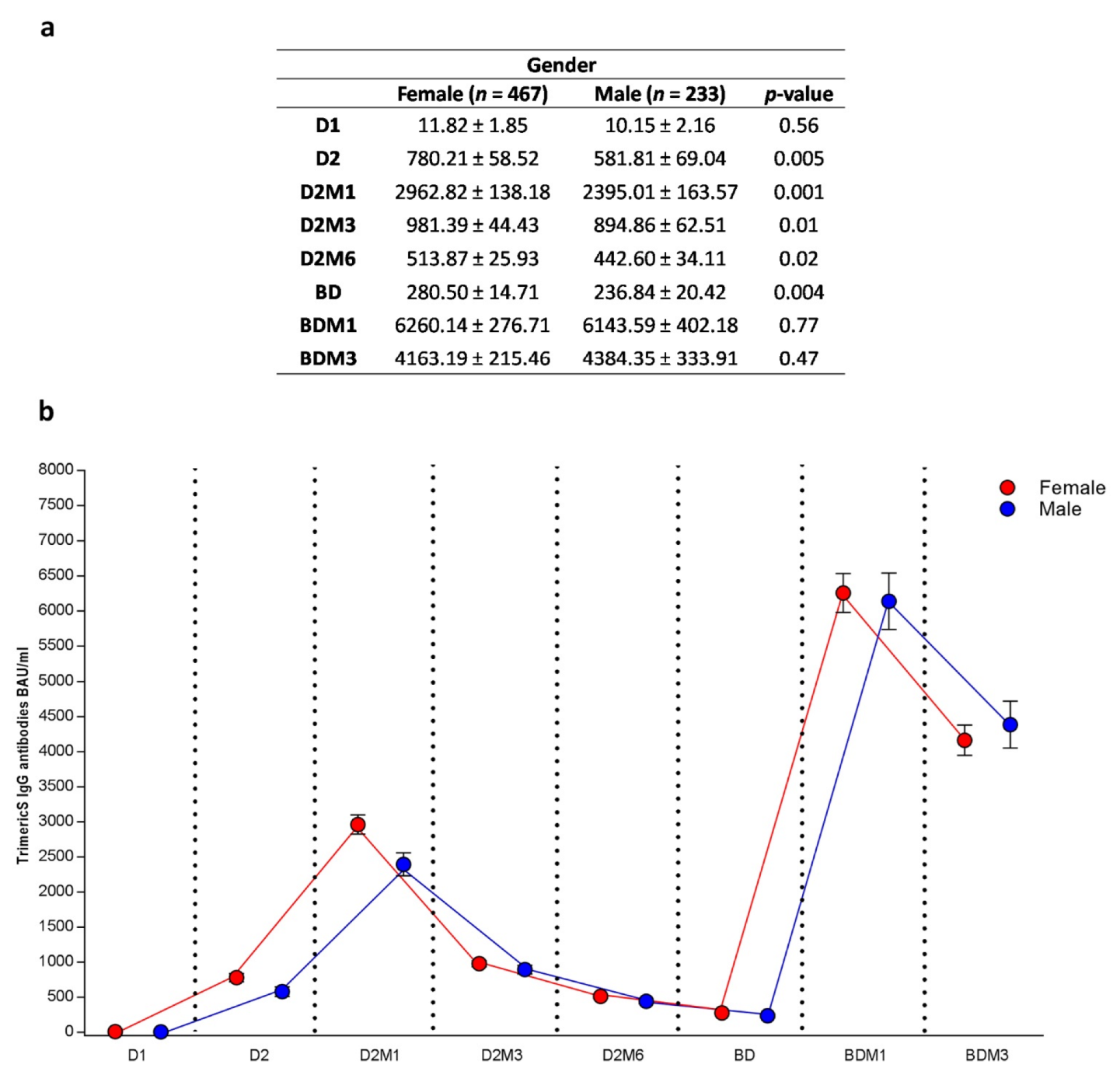
3.2.3. Anti-Trimeric Spike IgG Titer Dynamic According to Age and Sex
3.3. Effects of Variables in Antibody Titer Waning after Dose 2 and after Booster Dose
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ludwig, S.; Zarbock, A. Coronaviruses and SARS-CoV-2: A Brief Overview. Anesth. Analg. 2020, 131, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Lamb, Y.N. BNT162b2 mRNA COVID-19 Vaccine: First Approval. Drugs 2021, 81, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Pardi, N.; Tuyishime, S.; Muramatsu, H.; Kariko, K.; Mui, B.L.; Tam, Y.K.; Madden, T.D.; Hope, M.J.; Weissman, D. Expression kinetics of nucleoside-modified mRNA delivered in lipid nanoparticles to mice by various routes. J. Control. Release. 2015, 217, 345–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.-L.; Abiona, O.; Graham, B.S.; McLellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabiani, M.; Ramigni, M.; Gobbetto, V.; Mateo-Urdiales, A.; Pezzotti, P.; Piovesan, C. Effectiveness of the comirnaty (BNT162b2, BioNTech/Pfizer) vaccine in preventing SARS-CoV-2 infection among healthcare workers, Treviso province, Veneto region, Italy, 27 December 2020 to 24 March 2021. Eurosurveillance 2021, 26, 2100420. [Google Scholar] [CrossRef]
- Mascellino, M.T.; di Timoteo, F.; de Angelis, M.; Oliva, A. Overview of the main anti-sars-cov-2 vaccines: Mechanism of action, efficacy and safety. Infect. Drug Resist. 2021, 14, 3459–3476. [Google Scholar] [CrossRef]
- Paterlini, M. Covid-19: Italy makes vaccination mandatory for healthcare workers. BMJ 2021, 373, n905. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. Covid-19 Vaccine Effectiveness in New York State. N. Engl. J. Med. 2022, 386, 116–127. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Naioti, E.A.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; et al. Sustained Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Associated Hos-pitalizations Among Adults—United States, March–July 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 1156–1162. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.; Alterki, A.; Sindhu, S.; Alahmad, B.; Hammad, M.; Al-Sabah, S.; Alghounaim, M.; Jamal, M.H.; Aldei, A.; Mairza, M.J.; et al. Robust Antibody Levels in Both Diabetic and Non-Diabetic Individuals After BNT162b2 mRNA COVID-19 Vac-cination. Front. Immunol. 2021, 12, 752233. [Google Scholar] [CrossRef] [PubMed]
- Gudbjartsson, D.F.; Norddahl, G.L.; Melsted, P.; Gunnarsdottir, K.; Holm, H.; Eythorsson, E.; Arnthorsson, A.O.; Helgason, D.; Bjarnadottir, K.; Ingvarsson, R.F.; et al. Humoral Immune Response to SARS-CoV-2 in Iceland. N. Engl. J. Med. 2020, 383, 18. [Google Scholar] [CrossRef] [PubMed]
- Jeyanathan, M.; Afkhami, S.; Smaill, F.; Miller, M.S.; Lichty, B.D.; Xing, Z. Immunological considerations for COVID-19 vaccine strategies. Nat. Rev. Immunol. 2020, 20, 615–632. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC) Grading of Recommendations, Assessment, Development, and Evaluation (GRADE): COVID-19 Vaccine Additional and Booster Doses. 2021. Available online: https://www.cdc.gov/vaccines/acip/recs/grade/covid-19-booster-doses.html (accessed on 12 January 2023).
- ECDC Press Release ECDC and EMA Highlight Considerations for Additional and Booster Doses of COVID-19 Vaccines. (2 September 2021). Available online: https://www.ecdc.europa.eu/en/news-events/ecdc-and-ema-considerations-additional-and-booster-doses-covid-19-vaccines (accessed on 12 January 2023).
- Ali, H.; Alahmad, B.; Al-Shammari, A.A.; Alterki, A.; Hammad, M.; Cherian, P.; Alkhairi, I.; Sindhu, S.; Thanaraj, T.A.; Mohammad, A.; et al. Previous COVID-19 Infection and Antibody Levels After Vaccination. Front. Public Heal. 2021, 9, 778243. [Google Scholar] [CrossRef] [PubMed]
- Sano, K.; Bhavsar, D.; Singh, G.; Floda, D.; Srivastava, K.; Gleason, C.; PARIS Study Group; Carreño, J.M.; Simon, V.; Krammer, F. SARS-CoV-2 vaccination induces mucosal antibody responses in previously infected individuals. Nat. Commun. 2022, 13, 5135. [Google Scholar] [CrossRef]
- Trombetta, C.M.; Piccini, G.; Pierleoni, G.; Leonardi, M.; Dapporto, F.; Marchi, S.; Andreano, E.; Paciello, I.; Benincasa, L.; Lovreglio, P.; et al. Immune response to SARS-CoV-2 Omicron variant in patients and vaccinees following homologous and heterologous vaccinations. Commun. Biol. 2022, 5, 903. [Google Scholar] [CrossRef]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccina-tion against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef]
- Hoffmann, M.; Krüger, N.; Schulz, S.; Cossmann, A.; Rocha, C.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.-S.; Winkler, M.S.; et al. The Omicron variant is highly resistant against antibody-mediated neutralization: Implications for control of the COVID-19 pandemic. Cell 2021, 185, 447–456.e11. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Malavazos, A.E.; Basilico, S.; Iacobellis, G.; Milani, V.; Cardani, R.; Boniardi, F.; Dubini, C.; Prandoni, I.; Capitanio, G.; Renna, L.V.; et al. Antibody responses to BNT162b2 mRNA vaccine: Infection-naïve individuals with abdominal obesity warrant attention. Obesity 2021, 30, 606–613. [Google Scholar] [CrossRef]
- Wang, C.; Li, W.; Drabek, D.; Okba, N.M.A.; van Haperen, R.; Osterhaus, A.D.M.E.; van Kuppeveld, F.J.M.; Haagmans, B.L.; Grosveld, F.; Bosch, B.J. A human monoclonal antibody blocking SARS-CoV-2 infection. Nat. Commun. 2020, 11, 2251. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, P.; Nair, M.S.; Yu, J.; Rapp, M.; Wang, Q.; Luo, Y.; Chan, J.F.; Sahi, V.; Figueroa, A.; et al. Potent neutralizing antibodies against multiple epitopes on SARS-CoV-2 spike. Nature 2020, 584, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, S.A.; Ganesan, S.; Naik, S.; Bissar, S.; Zamel, I.A.; Warren, K.N.; Khan, G. Serological Assays for Assessing Postvaccination SARS-CoV-2 Antibody Response. Microbiol. Spectr. 2021, 9, e0073321. [Google Scholar] [CrossRef] [PubMed]
- Salvagno, G.L.; Henry, B.M.; Pighi, L.; De Nitto, S.; Gianfilippi, G.; Lippi, G. The pronounced decline of anti-SARS-CoV-2 spike trimeric IgG and RBD IgG in baseline seronegative individuals six months after BNT162b2 vaccination is consistent with the need for vaccine boosters. Clin. Chem. Lab. Medicine 2022, 60, e29–e31. [Google Scholar] [CrossRef]
- Xiong, X.; Qu, K.; Ciazynska, K.A.; Hosmillo, M.; Carter, A.P.; Ebrahimi, S.; Ke, Z.; Scheres, S.H.W.; Bergamaschi, L.; Grice, G.L.; et al. A thermostable, closed SARS-CoV-2 spike protein trimer. Nat. Struct. Mol. Biol. 2020, 27, 934–941. [Google Scholar] [CrossRef]
- Eyre, D.W.; Lumley, S.F.; Wei, J.; Cox, S.; James, T.; Justice, A.; Jesuthasan, G.; O’Donnell, D.; Howarth, A.; Hatch, S.B.; et al. Quantitative SARS-CoV-2 anti-spike responses to Pfizer–BioNTech and Oxford–AstraZeneca vaccines by previous infection status. Clin. Microbiol. Infect. 2021, 27, 1516.e7–1516.e14. [Google Scholar] [CrossRef]
- Ishizaki, A.; Bi, X.; Nguyen, Q.T.; Maeno, T.; Hara, A.; Nakamura, H.; Kuramoto, S.; Nishi, K.; Ooe, H.; Ichimura, H. Neutralizing-antibody response to SARS-CoV- 2 for 12 months after the COVID-19 workplace outbreaks in Japan. PLoS ONE 2022, 17, e0273712. [Google Scholar] [CrossRef]
- Takahashi, M.; Ai, T.; Sinozuka, K.; Baba, Y.; Igawa, G.; Nojiri, S.; Yamamoto, T.; Yuri, M.; Takei, S.; Saito, K.; et al. Activation of SARS-CoV-2 neutralizing antibody is slower than elevation of spike-specific IgG, IgM, and nucleocapsid-specific IgG antibodies. Sci. Rep. 2022, 12, 14909. [Google Scholar] [CrossRef]
- Gallais, F.; Gantner, P.; Bruel, T.; Velay, A.; Planas, D.; Wendling, M.J.; Bayer, S.; Solis, M.; Laugel, E.; Reix, N.; et al. Evolution of antibody responses up to 13 months after SARS-CoV-2 infection and risk of reinfection. EBioMe-Dicine 2021, 71, 103561. [Google Scholar] [CrossRef]
- Krutikov, M.; Palmer, T.; Tut, G.; Fuller, C.; Azmi, B.; Giddings, R.; Shrotri, M.; Kaur, N.; Sylla, P.; Lancaster, T.; et al. Prevalence and duration of detectable SARS-CoV-2 nucleocapsid antibodies in staff and residents of long-term care facilities over the first year of the pandemic (VIVALDI study): Prospective cohort study in England. Lancet Healthy Longev. 2022, 3, e13–e21. [Google Scholar] [CrossRef]
- Nakagama, Y.; Komase, Y.; Kaku, N.; Nitahara, Y.; Tshibangu-Kabamba, E.; Tominaga, T.; Tanaka, H.; Yokoya, T.; Hosokawa, M.; Kido, Y. Detecting Waning Serological Response with Commercial Immunoassays: 18-Month Longitudinal Fol-low-up of Anti-SARS-CoV-2 Nucleocapsid Antibodies. Microbiol. Spectr. 2022, 10, e0098622. [Google Scholar] [CrossRef] [PubMed]
- Navaratnam, A.M.D.; Shrotri, M.; Nguyen, V.; Braithwaite, I.; Beale, S.; Byrne, T.E.; Fong, W.L.E.; Fragaszy, E.; Geismar, C.; Hoskins, S.; et al. Nucleocapsid and spike antibody responses following virologically confirmed SARS-CoV-2 infec-tion: An observational analysis in the Virus Watch community cohort. Int. J. Infect. Dis. 2022, 123, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Teyssou, E.; Zafilaza, K.; Sayon, S.; Marot, S.; Dropy, M.; Soulie, C.; Abdi, B.; Tubach, F.; Hausfater, P.; Marcelin, A.G.; et al. Long-term evolution of humoral immune response after SARS-CoV-2 infection. Clin. Microbiol. -Fection. 2022, 28, 1027.e1–1027.e4. [Google Scholar] [CrossRef] [PubMed]
- Van Elslande, J.; Oyaert, M.; Ailliet, S.; Van Ranst, M.; Lorent, N.; Vande Weygaerde, Y.; André, E.; Lagrou, K.; Vandendriessche, S.; Vermeersch, P. Longitudinal follow-up of IgG anti-nucleocapsid antibodies in SARS-CoV-2 infected patients up to eight months after infection. J. Clin. Virology 2021, 136, 104765. [Google Scholar] [CrossRef]
- Casado, J.L.; Haemmerle, J.; Vizcarra, P.; Ramirez-Alonso, G.; Salazar-Tosco, A.; Romero-Hernandez, B.; Blasco, M.; Rodriguez-Dominguez, M.; Mirabella, I.G.; Vallejo, A.; et al. Risk of SARS-CoV-2 Reinfections in a Prospective Inception Cohort Study: Impact of COVID-19 Vaccination. J. Clin. Med. 2022, 11, 3352. [Google Scholar] [CrossRef] [PubMed]
- Lan, F.-Y.; Sidossis, A.; Iliaki, E.; Buley, J.; Nathan, N.; Bruno-Murtha, L.A.; Kales, S.N. Continued effectiveness of COVID-19 vaccination among urban healthcare workers during delta variant predominance. BMC Infect. Dis. 2022, 22, 1–4. [Google Scholar] [CrossRef]
- Ntziora, F.; Kostaki, E.G.; Karapanou, A.; Mylona, M.; Tseti, I.; Sipsas, N.V.; Paraskevis, D.; Sfikakis, P.P. Protection of vaccination versus hybrid immunity against infection with COVID-19 Omicron variants among Health-Care Workers. Vaccine 2022, 40, 7195–7200. [Google Scholar] [CrossRef]
- Murchu, O.E.; Byrne, P.; Carty, P.G.; De Gascun, C.; Keogan, M.; O’Neill, M.; Harrington, P.; Ryan, M. Quantifying the risk of SARS-CoV-2 reinfection over time. Rev. Med. Virology 2022, 32, e2260. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità (ISS) Prevalence and Distribution of SARS-CoV-2 Variants of Concern for Public Health in Italy (Re-portn. 18–25 March 2022). Available online: https://www.epicentro.iss.it/coronavirus/pdf/sars-cov-2-monitoraggio-varianti-rapporti-periodici-25-marzo-2022.pdf (accessed on 12 January 2023).
- Vicentini, C.; Zotti, C.M.; Cornio, A.R.; Garlasco, J.; Marengo, N.; Meddis, D.; Ditommaso, S.; Giacomuzzi, M.; Memoli, G.; Bordino, V.; et al. Serological Responses up to 9 Months following COVID-19 mRNA Vaccination in Residents and Health-Care Workers of Long-Term Care Facilities: A Multicenter Prospective Cohort Study in Northern Italy. Vaccines 2022, 10, 2183. [Google Scholar] [CrossRef]
- Faas, M.R.; Mak, W.A.; Markus, H.Y.; van der Zwan, E.M.; van der Vliet, M.; Koeleman, J.G.M.; Ong, D.S.Y. Dynamics of Antibody and T Cell Immunity against SARS-CoV-2 Variants of Concern and the Impact of Booster Vaccinations in Previously Infected and Infection-Naïve Individuals. Vaccines 2022, 10, 2132. [Google Scholar] [CrossRef] [PubMed]
- Gilboa, M.; Regev-Yochay, G.; Mandelboim, M.; Indenbaum, V.; Asraf, K.; Fluss, R.; Amit, S.; Mendelson, E.; Doolman, R.; Afek, A.; et al. Durability of Immune Response After COVID-19 Booster Vaccination and Association With COVID-19 Omicron Infection. JAMA Netw. Open 2022, 5, e2231778. [Google Scholar] [CrossRef] [PubMed]
- Blain, H.; Tuaillon, E.; Gamon, L.; Pisoni, A.; Miot, S.; Picot, M.C. Strong Decay of SARS-CoV-2 Spike Antibodies after 2 BNT162b2 Vaccine Doses and High Antibody Response to a Third Dose in Nursing Home Residents. J. Am. Med. Dir. Assoc. 2022, 23, 750–753. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Frenck, R.W., Jr.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 Neutralization with BNT162b2 Vaccine Dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Rahman, M.M.; Miah, M.; Begum, M.N.; Sarmin, M.; Mahfuz, M.; Hossain, M.E.; Chisti, M.J.; Ahmed, T.; El Arifeen, S. COVID-19 reinfections among naturally infected and vaccinated individuals. Sci. Rep. 2022, 12, 1–10. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.S.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and waning of natural and hybrid COVID-19 immunity to SARS-CoV-2. N. Engl. J. Med. 2022, 386, 2201–2212. [Google Scholar] [CrossRef]
- Hussein, K.; Dabaja-Younis, H.; Szwarcwort-Cohen, M.; Almog, R.; Leiba, R.; Weissman, A.; Mekel, M.; Hyams, G.; Horowitz, N.A.; Gepstein, V.; et al. Third BNT162b2 Vaccine Booster Dose against SARS-CoV-2-Induced Antibody Response among Healthcare Workers. Vaccines 2022, 10, 1741. [Google Scholar] [CrossRef]
- Pérez-Alós, L.; Armenteros, J.J.A.; Madsen, J.R.; Hansen, C.B.; Jarlhelt, I.; Hamm, S.R.; Heftdal, L.D.; Pries-Heje, M.M.; Møller, D.L.; Fogh, K.; et al. Modeling of waning immunity after SARS-CoV-2 vaccination and influencing factors. Nat. Commun. 2022, 13, 1614. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G. Efficacy of COVID-19 vaccine booster doses in older people. Eur. Geriatr. Med. 2022, 13, 275–278. [Google Scholar] [CrossRef]
- Xia, H.; Zou, J.; Kurhade, C.; Cai, H.; Yang, Q.; Cutler, M.; Cooper, D.; Muik, A.; Jansen, K.U.; Xie, X.; et al. Neutralization and durability of 2 or 3 doses of the BNT162b2 vaccine against Omicron SARS-CoV-2. Cell. Host. Microbe. 2022, 30, 485–488.e3. [Google Scholar] [CrossRef]
- Abdollahi, A.; Afsharyzad, Y.; Vaezi, A.; Meysamie, A. Importance of the COVID-19 Vaccine Booster Dose in Protection and Immunity. Vaccines 2022, 10, 1708. [Google Scholar] [CrossRef] [PubMed]
- Alidjinou, E.K.; Demaret, J.; Corroyer-Simovic, B.; Labreuche, J.; Goffard, A.; Trauet, J.; Lupau, D.; Miczek, S.; Vuotto, F.; Dendooven, A.; et al. Immunogenicity of BNT162b2 vaccine booster against SARS-CoV-2 Delta and Omicron variants in nursing home residents: A prospective observational study in older adults aged from 68 to 98 years. Lancet Reg. Health Europe 2022, 17, 100385. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No SARS-CoV-2 Infection (NN) (n = 400) | SARS-CoV-2 Infection after vaccine (NP) (n = 137) | SARS-CoV-2 Infection before and after Vaccine (PP) (n = 67) | SARS-CoV-2 Infection before Vaccine (PN) (n = 94) | Total (n = 698) | p-Value | |
|---|---|---|---|---|---|---|
| Age. Median (percentile) | 44.04 ± 12.18; 45.00 (35.00–53.00) | 41.79 ± 11.61; 42.00 (33.00–50.00) | 41.87 ± 9.56; 42.00 (35.00–50.00) | 43.16 ± 11.77; 43.00 (32.00–52.00) | 43.27 ± 11.80; 44.00 (34.00–52.00) | 0.20 |
| Female. n (%) | 276 (69.0) | 82 (59.9) | 45 (67.2) | 63 (67.0) | 466 (66.8) | 0.27 |
| Age n (%) | ||||||
| (19–30) | 69 (17.3) | 31 (22.6) | 10 (14.9) | 18 (19.2) | 128 (18.3) | 0.38 |
| (30–40) | 84 (21.0) | 32 (23.4) | 19 (28.4) | 21 (22.3) | 156 (22.4) | |
| (40–50) | 114 (28.5) | 43 (31.4) | 24 (35.8) | 29 (30.9) | 210 (30.1) | |
| (50–60) | 99 (24.8) | 23 (16.8) | 13 (19.4) | 18 (19.2) | 153 (21.9) | |
| (>60) | 34 (8.5) | 8 (5.8) | 1 (1.5) | 8 (8.5) | 51 (7.3) | |
| Occupation Status | ||||||
| Administrative Staff Members | 76 (19.1) | 20 (14.6) | 5 (7.5) | 13 (13.8) | 114 (16.4) | 0.09 |
| Auxiliary Health Workers | 20 (5.0) | 9 (6.6) | 4 (6.0) | 4 (4.3) | 37 (5.3) | |
| Medical Doctors | 78 (19.6) | 38 (27.7) | 11 (16.4) | 17 (18.1) | 144 (20.7) | |
| Non Medical Doctors | 74 (18.6) | 26 (19.0) | 10 (14.9) | 13 (13.8) | 123 (17.7) | |
| Nurses and Social Health Workers | 126 (31.6) | 39 (28.5) | 33 (49.3) | 39 (41.5) | 237 (34.0) | |
| Non-Health Care Workers | 25 (6.3) | 5 (3.7) | 4 (6.0) | 8 (8.5) | 42 (6.0) |
| After Second Dose | After Booster Dose | |||
|---|---|---|---|---|
| Univariate | Multivariable | Univariate | Multivariable | |
| p-Value | p-Value | p-Value | p-Value | |
| Sex | 0.07 | 0.084 | 0.705 | 0.613 |
| Age | 0.73 | 0.632 | 0.476 | 0.174 |
| IgG antibody level 1 month after dose | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| SARS CoV-2 infection groups | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| SARS-CoV-2 NP | 0.76 | <0.0001 | ||
| SARS-CoV-2 PP | 0.003 | 0.004 | ||
| SARS-CoV-2 PN | <0.0001 | 0.99 | ||
| SARS-CoV-2 NN | -- | -- | ||
| SARS-CoV-2 Infection Group | Fold after Second Dose (CI 95%) | Fold after Booster Dose (CI 95%) | p-Value |
|---|---|---|---|
| SARS-CoV-2 NN | 0.35 (0.31–0.39) | 0.54 (0.46–0.61) | <0.0001 |
| SARS-CoV-2 NP | 0.30 (0.25–0.37) | 1.47 (1.15–1.88) | 0.057 |
| SARS-CoV-2 PP | 0.33 (0.23–0.47) | 0.86 (0.62–1.20) | <0.0001 |
| SARS-CoV-2 PN | 0.42 (0.31–0.58) | 0.54 (0.42–0.71) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renna, L.V.; Bertani, F.; Podio, A.; Boveri, S.; Carrara, M.; Pinton, A.; Milani, V.; Spuria, G.; Nizza, A.F.; Basilico, S.; et al. Impact of BNT162b2 Booster Dose on SARS-CoV-2 Anti-Trimeric Spike Antibody Dynamics in a Large Cohort of Italian Health Care Workers. Vaccines 2023, 11, 463. https://doi.org/10.3390/vaccines11020463
Renna LV, Bertani F, Podio A, Boveri S, Carrara M, Pinton A, Milani V, Spuria G, Nizza AF, Basilico S, et al. Impact of BNT162b2 Booster Dose on SARS-CoV-2 Anti-Trimeric Spike Antibody Dynamics in a Large Cohort of Italian Health Care Workers. Vaccines. 2023; 11(2):463. https://doi.org/10.3390/vaccines11020463
Chicago/Turabian StyleRenna, Laura V., Fabio Bertani, Alessandro Podio, Sara Boveri, Matteo Carrara, Arianna Pinton, Valentina Milani, Giovanni Spuria, Angelica F. Nizza, Sara Basilico, and et al. 2023. "Impact of BNT162b2 Booster Dose on SARS-CoV-2 Anti-Trimeric Spike Antibody Dynamics in a Large Cohort of Italian Health Care Workers" Vaccines 11, no. 2: 463. https://doi.org/10.3390/vaccines11020463