
Trends in Hospitalization and Mortality for Influenza and Other Respiratory Viruses during the COVID-19 Pandemic in the United States
 , , and
, , and 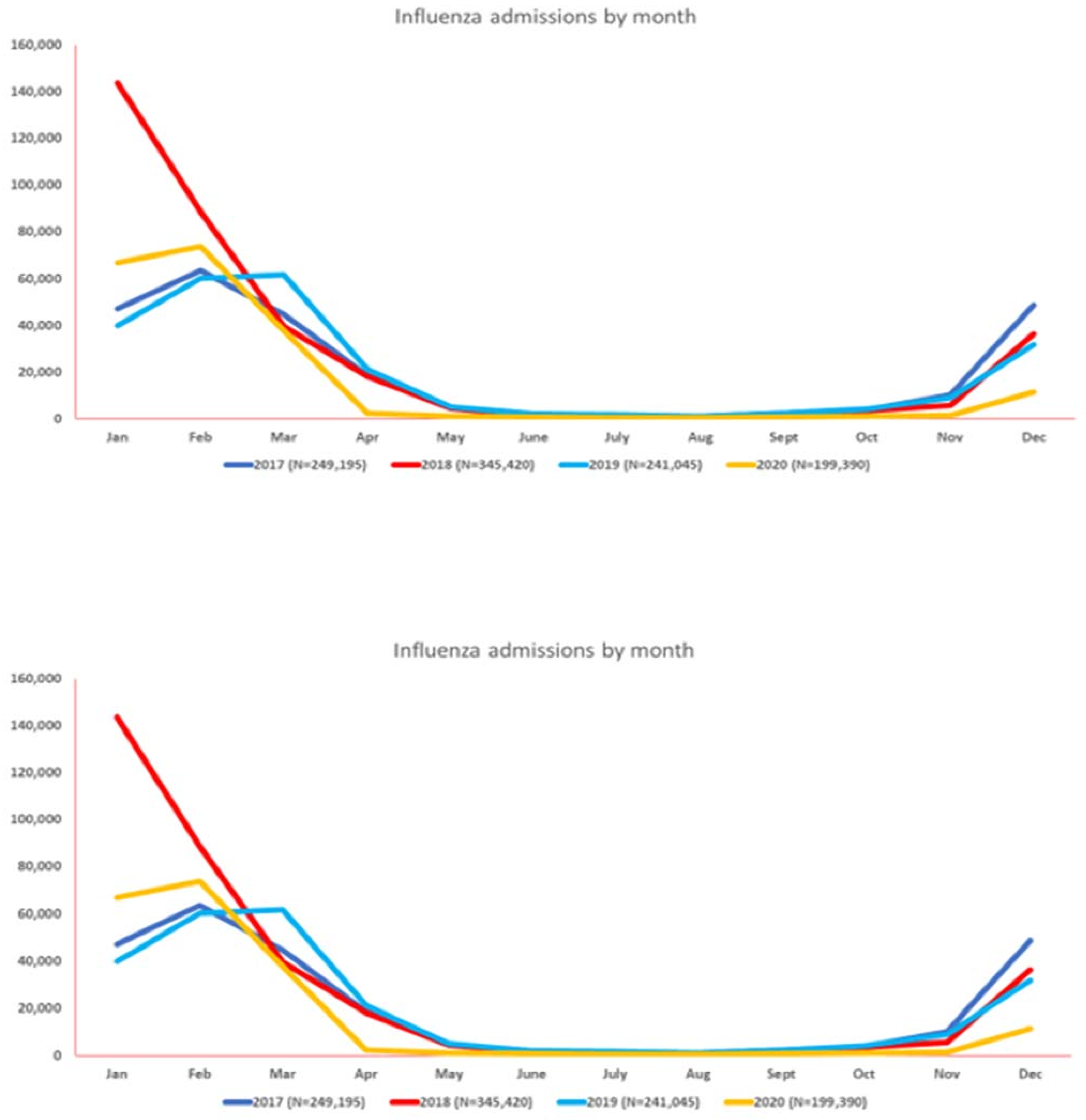{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Inclusion and Exclusion Criteria
2.3. Study Outcomes
2.4. Statistical Methods
3. Results
3.1. Influenza Virus
3.2. Respiratory Syncytial Virus (RSV)
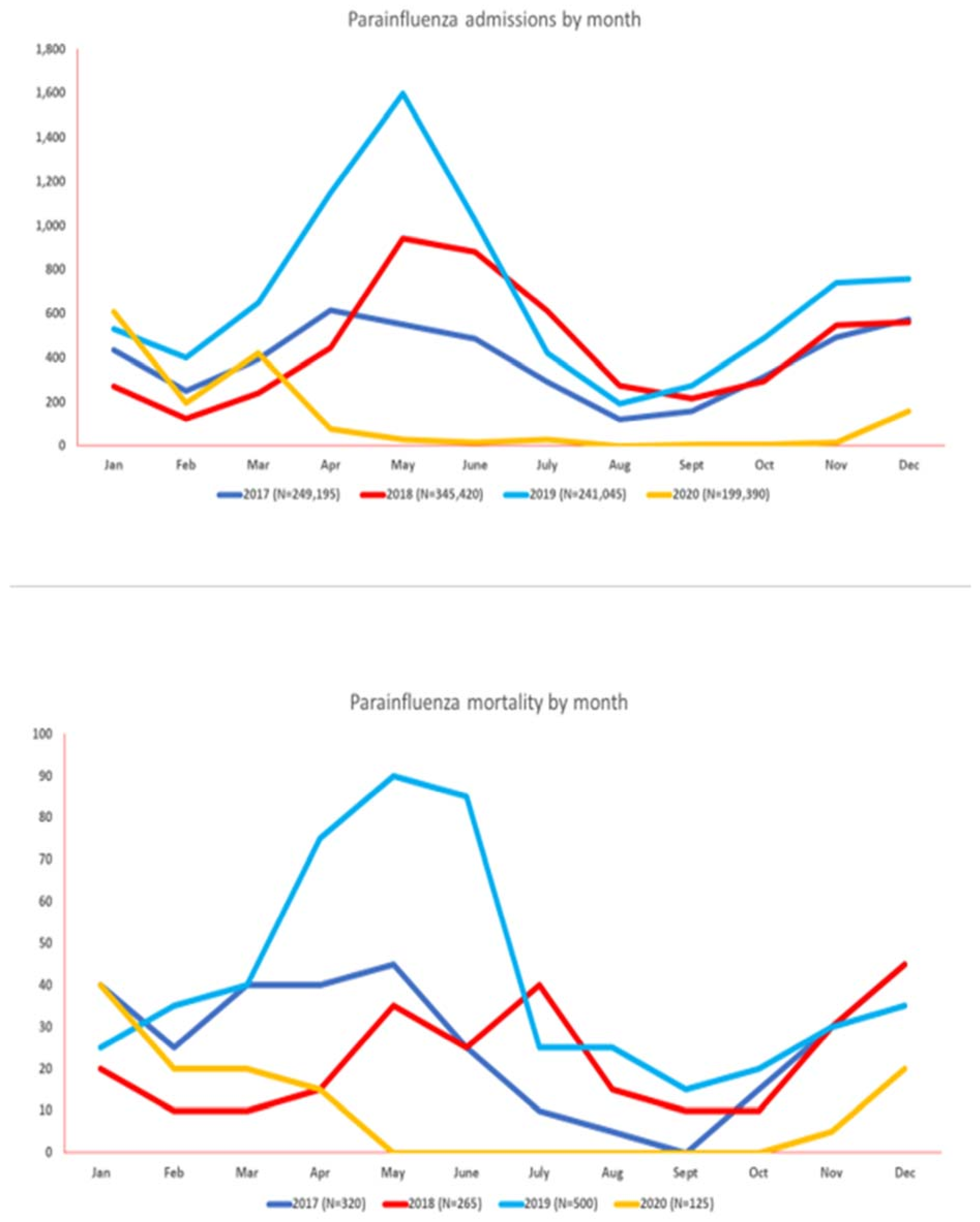
3.3. Parainfluenza Virus (PIV)
3.4. Human Metapneumovirus (MPV)
3.5. COVID-19 Infection
4. Discussion
4.1. Seasonality and Future Outbreaks
4.2. Public Health Interventions
4.3. Clinical and Diagnostic Tools
4.4. Research and Surveillance Tools
4.5. Potential Public Health Implications
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Itaya, T.; Furuse, Y.; Jindai, K. Does COVID-19 infection impact on the trend of seasonal influenza infection? 11 countries and regions, from 2014 to 2020. Int. J. Infect. Dis. 2020, 97, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef] [PubMed]
- CDC. CDC Museum COVID-19 Timeline | David J. Sencer CDC Museum. Available online: https://www.cdc.gov/museum/timeline/covid19.html (accessed on 7 January 2023).
- Garg, I.; Shekhar, R.; Sheikh, A.B.; Pal, S. Impact of COVID-19 on the Changing Patterns of Respiratory Syncytial Virus Infections. Infect. Dis. Rep. 2022, 14, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.J.; Winn, A.K.; Budd, A.P.; Prill, M.M.; Steel, J.; Midgley, C.M.; Kniss, K.; Burns, E.; Rowe, T.; Foust, A.; et al. Changes in Influenza and Other Respiratory Virus Activity During the COVID-19 Pandemic—United States, 2020–2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Ullrich, A.; Schranz, M.; Rexroth, U.; Hamouda, O.; Schaade, L.; Diercke, M.; Boender, T.S.; Robert Koch’s Infectious Disease Surveillance Group. Impact of the COVID-19 pandemic and associated non-pharmaceutical interventions on other notifiable infectious diseases in Germany: An analysis of national surveillance data during week 1–2016—Week 32–2020. Lancet Reg. Health-Eur. 2021, 6, 100103. [Google Scholar] [CrossRef]
- Solomon, D.A.; Sherman, A.C.; Kanjilal, S. Influenza in the COVID-19 Era. JAMA 2020, 324, 1342–1343. [Google Scholar] [CrossRef]
- McGovern, I.; Bogdanov, A.; Cappell, K.; Whipple, S.; Haag, M. Influenza Vaccine Uptake in the United States before and during the COVID-19 Pandemic. Vaccines 2022, 10, 1610. [Google Scholar] [CrossRef]
- NIS Database Documentation. Available online: https://hcup-us.ahrq.gov/db/nation/nis/nisdbdocumentation.jsp (accessed on 25 November 2022).
- NIS Database Documentation Archive. Available online: https://hcup-us.ahrq.gov/db/nation/nis/nisarchive.jsp (accessed on 7 January 2023).
- Leuchter, R.K.; Jackson, N.J.; Mafi, J.N.; Sarkisian, C.A. Association between Covid-19 Vaccination and Influenza Vaccination Rates. N. Engl. J. Med. 2022, 386, 2531–2532. [Google Scholar] [CrossRef]
- Chow, E.J.; Uyeki, T.M.; Chu, H.Y. The effects of the COVID-19 pandemic on community respiratory virus activity. Nat. Rev. Microbiol. 2022, 1–16. [Google Scholar] [CrossRef]
- Alshami, A.; Douedi, S.; Shenouda, D.; Nadhim, A.; Varon, J.; Patel, S. Incidence of influenza virus pneumonia during the time of coronovirus-2019 pandemic. Chest 2021, 160, A589. [Google Scholar] [CrossRef]
- Groves, H.E.; Papenburg, J.; Mehta, K.; Bettinger, J.A.; Sadarangani, M.; Halperin, S.A.; Morris, S.K.; Bancej, C.; Burton, C.; Embree, J.; et al. The effect of the COVID-19 pandemic on influenza-related hospitalization, intensive care admission and mortality in children in Canada: A population-based study. Lancet Reg. Health Am. 2022, 7, 100132. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Kim, H.I.; Kim, J.-H.; Park, S.; Hwang, Y.I.; Jang, S.H.; Kim, Y.K.; Jung, K.-S. Changes in respiratory virus infection trends during the COVID-19 pandemic in South Korea: The effectiveness of public health measures. Korean J. Intern. Med. 2021, 36, 1157–1168. [Google Scholar] [CrossRef] [PubMed]
- Suntronwong, N.; Thongpan, I.; Chuchaona, W.; Lestari, F.B.; Vichaiwattana, P.; Yorsaeng, R.; Pasittungkul, S.; Kitphati, R.; Vongpunsawad, S.; Poovorawan, Y. Impact of COVID-19 public health interventions on influenza incidence in Thailand. Pathog. Glob. Health 2020, 114, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Quandelacy, T.M.; Adams, L.E.; Munoz, J.; Santiago, G.A.; Kada, S.; Johansson, M.A.; Alvarado, L.I.; Rivera-Amill, V.; Paz–Bailey, G. Reduced spread of influenza and other respiratory viral infections during the COVID-19 pandemic in southern Puerto Rico. PLoS ONE 2022, 17, e0266095. [Google Scholar] [CrossRef]
- Sullivan, S.G.; Carlson, S.; Cheng, A.C.; Chilver, M.B.; Dwyer, D.E.; Irwin, M.; Kok, J.; Macartney, K.; MacLachlan, J.; Minney-Smith, C.; et al. Where has all the influenza gone? The impact of COVID-19 on the circulation of influenza and other respiratory viruses, Australia, March to September 2020. Eurosurveillance 2020, 25, 2001847. [Google Scholar] [CrossRef]
- Sovann, L.; Sar, B.; Kab, V.; Yann, S.; Kinzer, M.; Raftery, P.; Albalak, R.; Patel, S.; Hay, P.L.; Seng, H.; et al. An influenza A (H3N2) virus outbreak in the Kingdom of Cambodia during the COVID-19 pandemic of 2020. Int. J. Infect. Dis. 2021, 103, 352–357. [Google Scholar] [CrossRef]
- CDC. RSV-NET Interactive Dashboard. Available online: https://www.cdc.gov/rsv/research/rsv-net/dashboard.html (accessed on 7 January 2023).
- Ferrero, F.; Ossorio, M.F. Is there a place for bronchiolitis in the COVID-19 era? Lack of hospitalizations due to common respiratory viruses during the 2020 winter. Pediatr. Pulmonol. 2021, 56, 2372–2373. [Google Scholar] [CrossRef]
- Friedrich, F.; Ongaratto, R.; Scotta, M.C.; Veras, T.N.; Stein, R.T.; Lumertz, M.S.; Jones, M.H.; Comaru, T.; Pinto, L.A. Early Impact of Social Distancing in Response to Coronavirus Disease 2019 on Hospitalizations for Acute Bronchiolitis in Infants in Brazil. Clin. Infect. Dis. 2021, 72, 2071–2075. [Google Scholar] [CrossRef]
- Varela, F.H.; Scotta, M.C.; Polese-Bonatto, M.; Sartor, I.T.S.; Ferreira, C.F.; Fernandes, I.R.; Zavaglia, G.O.; Ferreira de Almeida, W.A.; Arakaki-Sanchez, D.; Pinto, L.A.; et al. Absence of detection of RSV and influenza during the COVID-19 pandemic in a Brazilian cohort: Likely role of lower transmission in the community. J. Glob. Health 2021, 11, 05007. [Google Scholar] [CrossRef]
- Tempia, S.; Walaza, S.; Bhiman, J.N.; McMorrow, M.L.; Moyes, J.; Mkhencele, T.; Meiring, S.; Quan, V.; Bishop, K.; McAnerney, J.M.; et al. Decline of influenza and respiratory syncytial virus detection in facility-based surveillance during the COVID-19 pandemic, South Africa, January to October 2020. Eurosurveillance 2021, 26, 2001600. [Google Scholar] [CrossRef]
- Agha, R.; Avner, J.R. Delayed Seasonal RSV Surge Observed During the COVID-19 Pandemic. Pediatrics 2021, 148, 2021052089. [Google Scholar] [CrossRef] [PubMed]
- Von Hammerstein, A.L.; Aebi, C.; Barbey, F.; Berger, C.; Buettcher, M.; Casaulta, C.; Egli, A.; Gebauer, M.; Guerra, B.; Kahlert, C.; et al. Interseasonal RSV infections in Switzerland—Rapid establishment of a clinician-led national reporting system (RSV EpiCH). Swiss Med. Wkly. 2021, 151, w30057. [Google Scholar] [CrossRef] [PubMed]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N. Resurgence of Respiratory Syncytial Virus Infections during COVID-19 Pandemic, Tokyo, Japan. Emerg. Infect. Dis. 2021, 27, 2969–2970. [Google Scholar] [CrossRef] [PubMed]
- Opek, M.W.; Yeshayahu, Y.; Glatman-Freedman, A.; Kaufman, Z.; Sorek, N.; Brosh-Nissimov, T. Delayed respiratory syncytial virus epidemic in children after relaxation of COVID-19 physical distancing measures, Ashdod, Israel, 2021. Eurosurveillance 2021, 26, 2100706. [Google Scholar] [CrossRef]
- CDC. Human Parainfluenza National Trends—NREVSS. Available online: https://www.cdc.gov/surveillance/nrevss/human-paraflu/natl-trend.html (accessed on 7 January 2023).
- Piroth, L.; Cottenet, J.; Mariet, A.-S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: A nationwide, population-based retrospective cohort study. Lancet Respir. Med. 2021, 9, 251–259. [Google Scholar] [CrossRef]
- Berencsi, G.; Kapusinszky, B.; Rigó, Z.; Szomor, K. Interference among viruses circulating and administered in Hungary from 1931 to 2008. Acta Microbiol. Immunol. Hung. 2010, 57, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Dental Group of Sherman Oaks; Chiappelli, F. Virus interference in CoViD-19. Bioinformation 2022, 18, 768–773. [Google Scholar] [CrossRef]
- Dhanasekaran, V.; Sullivan, S.; Edwards, K.M.; Xie, R.; Khvorov, A.; Valkenburg, S.A.; Cowling, B.J.; Barr, I.G. Human seasonal influenza under COVID-19 and the potential consequences of influenza lineage elimination. Nat. Commun. 2022, 13, 1721. [Google Scholar] [CrossRef]
- CDC. ACIP Influenza Vaccine Recommendations. Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/flu.html (accessed on 17 December 2022).
- Schlegtendal, A.; Eitner, L.; Falkenstein, M.; Hoffmann, A.; Lücke, T.; Sinningen, K.; Brinkmann, F. To Mask or Not to Mask—Evaluation of Cognitive Performance in Children Wearing Face Masks during School Lessons (MasKids). Children 2022, 9, 95. [Google Scholar] [CrossRef]
- Garg, I.; Shekhar, R.; Sheikh, A.; Pal, S. COVID-19 Vaccine in Pregnant and Lactating Women: A Review of Existing Evidence and Practice Guidelines. Infect. Dis. Rep. 2021, 13, 685–699. [Google Scholar] [CrossRef]
- Garg, I.; Hanif, H.; Javed, N.; Abbas, R.; Mirza, S.; Javaid, M.A.; Pal, S.; Shekhar, R.; Sheikh, A.B. COVID-19 Vaccine Hesitancy in the LGBTQ+ Population: A Systematic Review. Infect. Dis. Rep. 2021, 13, 872–887. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.-L.; Li, Y.-Q.; Chen, X.; Lin, H.; Jiang, Z.-C.; Gu, D.-L.; Chen, X.; Tang, C.-X.; Xie, Z.-Q. Co-Infection with Common Respiratory Pathogens and SARS-CoV-2 in Patients with COVID-19 Pneumonia and Laboratory Biochemistry Findings: A Retrospective Cross-Sectional Study of 78 Patients from a Single Center in China. Med. Sci. Monit. 2021, 27, e929783. [Google Scholar] [CrossRef] [PubMed]
- Leung, E.C.-M.; Chow, V.C.-Y.; Lee, M.K.-P.; Tang, K.P.-S.; Li, D.K.-C.; Lai, R.W.-M. Evaluation of the Xpert Xpress SARS-CoV-2/Flu/RSV Assay for Simultaneous Detection of SARS-CoV-2, Influenza A and B Viruses, and Respiratory Syncytial Virus in Nasopharyngeal Specimens. J. Clin. Microbiol. 2021, 59, e02965-20. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.Y.; Kim, J.-Y.; Shim, H.J.; Yun, S.A.; Jang, J.-H.; Huh, H.J.; Kim, J.-W.; Lee, N.Y. Comparison of the PowerChek SARS-CoV-2, Influenza A&B, RSV Multiplex Real-time PCR Kit and BioFire Respiratory Panel 2.1 for simultaneous detection of SARS-CoV-2, influenza A and B, and respiratory syncytial virus. J. Virol. Methods 2021, 298, 114304. [Google Scholar] [CrossRef]
- Wolters, F.; Grünberg, M.; Huber, M.; Kessler, H.H.; Prüller, F.; Saleh, L.; Fébreau, C.; Rahamat-Langendoen, J.; Thibault, V.; Melchers, W.J.G. European multicenter evaluation of Xpert® Xpress SARS-CoV-2/Flu/RSV test. J. Med. Virol. 2021, 93, 5798–5804. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasrullah, A.; Gangu, K.; Garg, I.; Javed, A.; Shuja, H.; Chourasia, P.; Shekhar, R.; Sheikh, A.B. Trends in Hospitalization and Mortality for Influenza and Other Respiratory Viruses during the COVID-19 Pandemic in the United States. Vaccines 2023, 11, 412. https://doi.org/10.3390/vaccines11020412
Nasrullah A, Gangu K, Garg I, Javed A, Shuja H, Chourasia P, Shekhar R, Sheikh AB. Trends in Hospitalization and Mortality for Influenza and Other Respiratory Viruses during the COVID-19 Pandemic in the United States. Vaccines. 2023; 11(2):412. https://doi.org/10.3390/vaccines11020412
Chicago/Turabian StyleNasrullah, Adeel, Karthik Gangu, Ishan Garg, Anam Javed, Hina Shuja, Prabal Chourasia, Rahul Shekhar, and Abu Baker Sheikh. 2023. "Trends in Hospitalization and Mortality for Influenza and Other Respiratory Viruses during the COVID-19 Pandemic in the United States" Vaccines 11, no. 2: 412. https://doi.org/10.3390/vaccines11020412