
Baseline Cytokine Profile Identifies a Favorable Outcome in a Subgroup of Colorectal Cancer Patients Treated with Regorafenib
 , , , , , ,
, , , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Blood Sample Collection
2.4. Analysis Methods
2.4.1. Plasma Levels of 18 Cytokines
2.4.2. IL-21
2.5. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Treatment Effect
3.3. Correlation between Baseline Cytokine Levels and PFS
3.4. Cluster Analysis
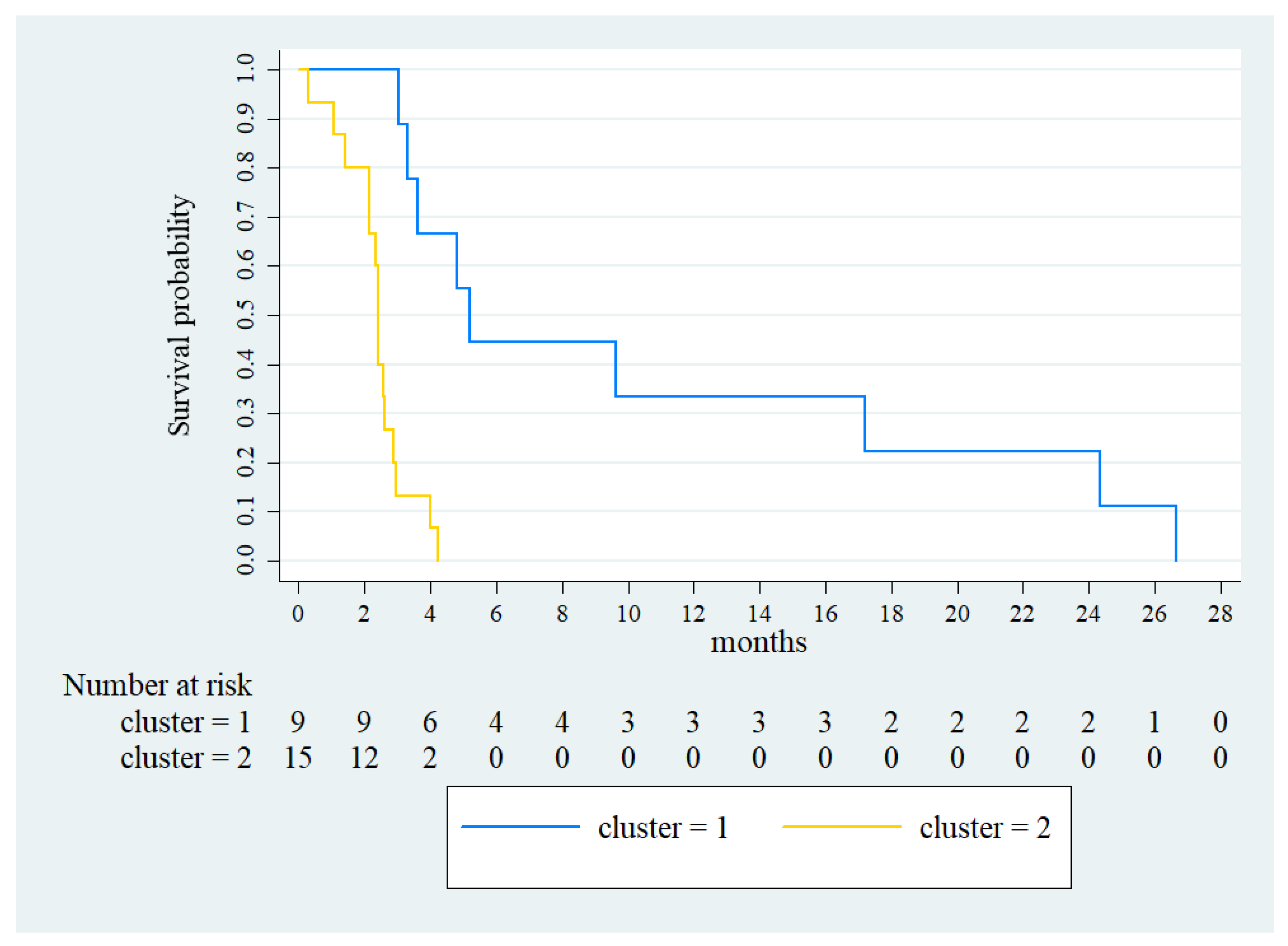
3.5. Kaplan–Meier Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baidoun, F.; Elshiwy, K.; Elkeraie, Y.; Merjaneh, Z.; Khoudari, G.; Sarmini, M.T.; Gad, M.; Al-Husseini, M.; Saad, A. Colorectal Cancer Epidemiology: Recent Trends and Impact on Outcomes. Curr. Drug Targets 2021, 22, 998–1009. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Sauer, A.G.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, T.; Pamoukdjian, F.; Quero, L.; Manfredi, S.; Wind, P.; Paillaud, E. Colorectal cancer care in elderly patients: Unsolved issues. Dig. Liver Dis. 2016, 48, 1112–1118. [Google Scholar] [CrossRef]
- Arai, H.; Battaglin, F.; Wang, J.; Lo, J.H.; Soni, S.; Zhang, W.; Lenz, H.-J. Molecular insight of regorafenib treatment for colorectal cancer. Cancer Treat. Rev. 2019, 81, 101912. [Google Scholar] [CrossRef] [PubMed]
- Ettrich, T.J.; Seufferlein, T. Regorafenib. Recent Results Cancer Res. 2018, 211, 45–56. [Google Scholar] [CrossRef]
- Li, J.; Qin, S.; Xu, R.; Yau, T.C.C.; Ma, B.; Pan, H.; Xu, J.; Bai, Y.; Chi, Y.; Wang, L.; et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2015, 16, 619–629. [Google Scholar] [CrossRef]
- Ducreux, M.; Petersen, L.N.; Öhler, L.; Bergamo, F.; Metges, J.-P.; de Groot, J.W.; Wang, J.-Y.; Paredes, B.G.; Dochy, E.; Fiala-Buskies, S.; et al. Safety and effectiveness of regorafenib in patients with metastatic colorectal cancer in routine clinical practice in the prospective, observational CORRELATE study. Eur. J. Cancer 2019, 123, 146–154. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Nordlinger, B.; Cervantes, A. Advanced colorectal cancer: ESMO Clinical Practice Guidelines for treatment. Ann. Oncol. 2010, 21 (Suppl. 5), v93–v97. [Google Scholar] [CrossRef]
- Grothey, A.; Van Cutsem, E.; Sobrero, A.F.; Siena, S.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouche, O.; Mineur, L.; Barone, C.; et al. Time course of regorafenib-associated adverse events in the phase III CORRECT study. J. Clin. Oncol. 2012, 30 (Suppl. 34), 467. [Google Scholar] [CrossRef]
- Bekaii-Saab, T.S.; Ou, F.-S.; Ahn, D.H.; Boland, P.M.; Ciombor, K.K.; Heying, E.N.; Dockter, T.J.; Jacobs, N.L.; Pasche, B.C.; Cleary, J.M.; et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): A randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019, 20, 1070–1082. [Google Scholar] [CrossRef]
- Goel, G. Evolution of regorafenib from bench to bedside in colorectal cancer: Is it an attractive option or merely a “me too” drug? Cancer Manag. Res. 2018, 10, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Kartikasari, A.E.R.; Huertas, C.S.; Mitchell, A.; Plebanski, M. Tumor-Induced Inflammatory Cytokines and the Emerging Diagnostic Devices for Cancer Detection and Prognosis. Front. Oncol. 2021, 11, 692142. [Google Scholar] [CrossRef] [PubMed]
- Ricci, V.; Granetto, C.; Falletta, A.; Paccagnella, M.; Abbona, A.; Fea, E.; Fabozzi, T.; Nigro, C.L.; Merlano, M.C. Circulating cytokines and outcome in metastatic colorectal cancer patients treated with regorafenib. World J. Gastrointest. Oncol. 2020, 12, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Kantola, T.; Klintrup, K.; Väyrynen, J.P.; Vornanen, J.; Bloigu, R.; Karhu, T.; Herzig, K.-H.; Näpänkangas, J.; Mäkelä, J.; Karttunen, T.J.; et al. Stage-dependent of the serumcytokine pattern in colorectal carcinoma. Br. J. Cancer 2012, 107, 1729–1736. [Google Scholar] [CrossRef]
- Wilkerson, J.; Fojo, T. Progression-free survival is simply a measure of a drug’s effect while administered and is not a surrogate for overall survival. Cancer J. 2009, 15, 379–385. [Google Scholar] [CrossRef]
- Haynes, W. Bonferroni Correction. In Encyclopedia of Systems Biology Components; Dubitzky, W., Wolkenhauer, O., Cho, K.H., Yokota, H., Eds.; Springer: New York, NY, USA, 2013; p. 154. [Google Scholar]
- Youngs, S.J.; Ali, S.A.; Taub, D.D.; Rees, R.C. Chemokines induce migrational responses in human breast carcinoma cell lines. Int. J. Cancer 1997, 71, 257–266. [Google Scholar] [CrossRef]
- Qian, B.-Z.; Li, J.; Zhang, H.; Kitamura, T.; Zhang, J.; Campion, L.R.; Kaiser, E.A.; Snyder, L.A.; Pollard, J.W. CCL2 recruits inflammatory monocytes to facilitate breast-tumour metastasis. Nature 2011, 475, 222–225. [Google Scholar] [CrossRef]
- Lança, T.; Costa, M.F.; Gonçalves-Sousa, N.; Rei, M.; Grosso, A.R.; Penido, C.; Silva-Santos, B. Protective Role of the Inflammatory CCR2/CCL2 Chemokine Pathway through Recruitment of Type 1 Cytotoxic γδ T Lymphocytes to Tumor Beds. J. Immunol. 2013, 190, 6673–6680. [Google Scholar] [CrossRef]
- Parrish-Novak, J.; Dillon, S.R.; Nelson, A.; Hammond, A.; Sprecher, C.A.; Gross, J.A.; Johnston, J.A.; Madden, K.; Xu, W.; West, J.; et al. Interleukin 21 and its receptor are involved in NK cell expansion and regulation of lymphocyte function. Nature 2000, 408, 57–63. [Google Scholar] [CrossRef]
- Zeng, R.; Spolski, R.; Finkelstein, S.E.; Oh, S.; Kovanen, P.E.; Hinrichs, C.S.; Pise-Masison, C.A.; Radonovich, M.F.; Brady, J.N.; Restifo, N.P.; et al. Synergy of IL-21 and IL-15 in regulating CD8+ T cell expansion and function. J. Exp. Med. 2005, 201, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Fantini, M.C.; Rizzo, A.; Fina, D.; Caruso, R.; Becker, C.; Neurath, M.F.; Macdonald, T.T.; Pallone, F.; Monteleone, G. IL-21 regulates experimental colitis by modulating the balance between Treg and Th17 cells. Eur. J. Immunol. 2007, 37, 3155–3163. [Google Scholar] [CrossRef] [PubMed]
- Barjon, C.; Michaud, H.-A.; Fages, A.; Dejou, C.; Zampieri, A.; They, L.; Gennetier, A.; Sanchez, F.; Gros, L.; Eliaou, J.-F.; et al. IL-21 promotes the development of a CD73-positive Vγ9Vδ2 T cell regulatory population. Oncoimmunology 2018, 7, e1379642. [Google Scholar] [CrossRef] [PubMed]
- Derynck, R.; Akhurst, R.J.; Balmain, A. TGF-beta signaling in tumor suppression and cancer progression. Nat. Genet. 2001, 29, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Baba, A.B.; Rah, B.; Bhat, G.R.; Mushtaq, I.; Parveen, S.; Hassan, R.; Zargar, M.H.; Afroze, D. Transforming growth-factor (TGF-β) signaling in cancer-A betrayal within. Front. Pharmacol. 2022, 13, 791272. [Google Scholar] [CrossRef]
- Sarris, A.H.; Kliche, K.-O.; Pethambaram, P.; Preti, A.; Tucker, S.; Jackow, C.; Messina, O.; Pugh, W.; Hagemeister, F.; McLaughlin, P.; et al. Interleukin-10 levels are often elevated in serum of adults with Hodgkin’s disease and are associated with inferior failure-free survival. Ann. Oncol. 1999, 10, 433–440. [Google Scholar] [CrossRef]
- Visco, C.; Vassilakopoulos, T.P.; Kliche, K.O.; Nadali, G.; Viviani, S.; Bonfante, V.; Medeiros, L.J.; Notti, P.; Rassidakis, G.Z.; Peethambaram, P.; et al. Elevated serum levels of IL-10 are associated with inferior progression-free survival in patients with Hodgkin’s disease treated with radiotherapy. Leuk. Lymphoma 2004, 45, 2085–2092. [Google Scholar] [CrossRef]
- Soria, J.-C.; Moon, C.; Kemp, B.L.; Liu, D.D.; Feng, L.; Tang, X.; Chang, Y.S.; Mao, L.; Khuri, F.R. Lack of interleukin-10 expression could predict poor outcome in patients with stage I non-small cell lung cancer. Clin. Cancer Res. 2003, 9, 1785–1791. [Google Scholar]
- Chang, J.; Zhang, W.; Lin, G.; Tong, D.; Zhu, D.; Zhao, J.; Yu, Q.; Huang, D.; Li, W. Tumor Response to Irinotecan is Associated with IL-10 Expression Level in Metastatic Colorectal Cancer-Results from mCRC Biomarker Study. OncoTargets Ther. 2020, 13, 11819–11826. [Google Scholar] [CrossRef]
- Xu, J.; Ye, Y.; Zhang, H.; Szmitkowski, M.; Mäkinen, M.J.; Li, P.; Xia, D.; Yang, J.; Wu, Y.; Wu, H. Diagnostic and Prognostic Value of Serum Interleukin-6 in Colorectal Cancer. Medicine 2016, 95, e2502. [Google Scholar] [CrossRef]
- Fisher, D.T.; Appenheimer, M.M.; Evans, S.S. The two faces of IL-6 in the tumor microenvironment. Semin. Immunol. 2014, 26, 38–47. [Google Scholar] [CrossRef]
- David, J.M.; Dominguez, C.; Hamilton, D.H.; Palena, C. The IL-8/IL-8R axis: A double agent in tumor immune resistance. Vaccines 2016, 4, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doll, D.; Keller, L.; Maak, M.; Boulesteix, A.-L.; Siewert, J.R.; Holzmann, B.; Janssen, K.-P. Differential expression of the chemokines GRO-2, GRO-3, and interleukin-8 in colon cancer and their impact on metastatic disease and survival. Int. J. Color. Dis. 2010, 25, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Terzić, J.; Grivennikov, S.; Karin, E.; Karin, M. Inflammation and colon cancer. Gastroenterology 2010, 138, 2101–2114. [Google Scholar] [CrossRef]
- Josephs, S.F.; Ichim, T.E.; Prince, S.M.; Kesari, S.; Marincola, F.M.; Escobedo, A.R.; Jafri, A. Unleashing endogenous TNF-α as a cancer immune therapy. J. Transl. Med. 2018, 16, 242. [Google Scholar] [CrossRef]
- Sinha, P.; Clements, V.K.; Ostrand-Rosenberg, S. Interleukin-13 regulated M2 macrophages in combination with myeloid suppressor cells block immune surveillance against metastasis. Cancer Res. 2005, 65, 11743–11751. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Zhang, J.; Liu, H.; Wan, L.; Zhang, H.; Huang, Q.; Xu, E.; Lai, M. IL13/STAT6 signaling plays a critical role in epithelial-mesenchymal transition of colorectal cancer cells. Oncotarget 2016, 7, 61183–61198. [Google Scholar] [CrossRef]
- Kantola, T.; Klintrup, K.; Väyrynen, J.P.; Vornanen, J.; Bloigu, R.; Karhu, T.; Herzig, K.-H.; Näpänkangas, J.; Mäkelä, J.; Karttunen, T.J.; et al. Reply: Comment on ‘Stage-dependent alterations of the serum cytokine pattern in colorectal carcinoma’. Br. J. Cancer 2013, 108, 1917–1918. [Google Scholar] [CrossRef]
- Chen, Z.-Y.; He, W.-Z.; Peng, L.-X.; Jia, W.-H.; Guo, R.-P.; Xia, L.-P.; Qian, C.-N. A prognostic classifier consisting of 17 circulating cytokines is a novel predictor of overall survival for metastatic colorectal cancer patients. Int. J. Cancer 2015, 136, 584–592. [Google Scholar] [CrossRef]
- Gunawardene, A.; Dennett, E.; Larsen, P. Prognostic value of multiple cytokine analysis in colorectal cancer: A systematic review. J. Gastrointest. Oncol. 2019, 10, 134–143. [Google Scholar] [CrossRef]
- Tuong, Z.K.; Lewandowski, A.; Bridge, J.A.; Cruz, J.L.G.; Yamada, M.; Lambie, D.; Lewandowski, R.; Steptoe, R.J.; Leggatt, G.R.; Simpson, F.; et al. Cytokine/chemokine profiles in squamous cell carcinoma correlate with precancerous and cancerous disease stage. Sci. Rep. 2019, 9, 17754. [Google Scholar] [CrossRef]
- Nistor, G.I.; Dillman, R.O. Cytokine network analysis of immune responses before and after autologous dendritic cell and tumor cell vaccine immunotherapies in a randomized trial. J. Transl. Med. 2020, 18, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellsworth, S.G.; Rabatic, B.M.; Chen, J.; Zhao, J.; Campbell, J.; Wang, W.; Pi, W.; Stanton, P.; Matuszak, M.; Jolly, S.; et al. Principal component analysis identifies patterns of cytokine expression in non-small cell lung cancer patients undergoing definitive radiation therapy. PLoS ONE 2017, 12, e0183239. [Google Scholar] [CrossRef]
- Merlano, M.; Abbona, A.; Paccagnella, M.; Falletta, A.; Granetto, C.; Ricci, V.; Fea, E.; Denaro, N.; Ruatta, F.; Merlotti, A.; et al. Cytokine profile of end stage cancer patients treated with immunotherapy. Vaccines 2021, 9, 235. [Google Scholar] [CrossRef] [PubMed]
- Paccagnella, M.; Abbona, A.; Michelotti, A.; Geuna, E.; Ruatta, F.; Landucci, E.; Denaro, N.; Vanella, P.; Lo Nigro, C.; Galizia, D.; et al. Circulating cytokines in metastatic breast cancer patients select different prognostic groups and patients who might benefit from treatment beyond progression. Vaccines 2022, 10, 78. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number 25 |
|---|---|
| Age (median, range) | 65 (48–80) |
| ECOG PS (median, range) | 0 (0–1) |
| Sex | |
| Male | 14 (56%) |
| Female | 11 (44 %) |
| Primary Tumor Site | rectum 10 (40%) |
| colon 15 (60%) | |
| Mutational RAS status | |
| Mutated | 20 (80%) |
| Wild type | 5 (20%) |
| Previous anticancer therapies in individual patients | |
| 2 | 4 (16%) |
| 3 | 11 (44 %) |
| 4 | 8 (32 %) |
| ≥5 | 2 (8 %) |
| Median n (range) | 3 (2–7) |
| Treatment Line | Treatment | Patients (# by Cluster) | Patients | ||||
|---|---|---|---|---|---|---|---|
| Cluster 1 | Cluster 2 | Cluster 3 | Cluster 1 | Cluster 2 | Cluster 3 | Total | |
| 1 | Folfiri 1 + beva 2 Xelox 3 + beva 2 Folfox 4 Folfoxiri 5 + beva 2 Folfox 4 + beva 2 Xelox 3 Cape 6 + beva 2 | Xelox 3 Folfoxiri 5 + beva 2 Folfox 4 Xelox 3 + RT Folfox 4 + beva 2 Folfoxiri 5 | Xelox 3 + beva 2 | 13 | 11 | 1 | 25 |
| 2 | Folfiri 1 (re-) 9 Xelox 3 Cape 6 Folfiri 1+ beva 2 Cape 6 + beva 2 Fu 10 + beva 2 Xeliri 7 Folfiri 1 | Folfiri 1 Cape 6 + beva 2 Folfiri 1 + beva 2 Xelox 3 + beva 2 Folfiri 1 + afli 12 | Folfiri 1 + beva 2 | 13 | 11 | 1 | 25 |
| 3 | Folfox 4 FU 10 + beva 2 Xelox 3 Cet 8 + Irino 11 Folfox 4 + beva 2 (re-) 9 Folfiri 1 + beva 2 Irino 11 + beva 2 Lons. 14 | Folfox 4 Folfiri 1 + beva 2 Folfox 4 (re-) 9 Cape 6 Lons. 14 | Lons. 14 | 12 | 8 | 1 | 21 |
| 4 | Folfiri 1 + Cet 8 Folfox 4 Folfox 4 + afli 12 Pani 13 Lons. 14 Folfox 4 + beva 2 | Pani 13 Xelox3 + beva 2 Cape 6 | 7 | 3 | - | 10 | |
| 5 | Folfox 4 (re-) 9 | Irino 11 + beva 2 | 2 | 1 | - | 3 | |
| 6 | Irino 11 + cet 8 | 1 | - | - | 1 | ||
| 7 | Lons. 14 | 1 | - | - | 1 | ||
| Variable | HR | 95% C.I. | p Value |
|---|---|---|---|
| Cluster 1 (ref Cluster 3) | 0.110 | 0.030–0.399 | 0.001 |
| Sex (ref male) | 0.867 | 0.428–2.737 | 0.867 |
| Primary site (ref rectum) | 0.555 | ||
| Right Colon | 0.528 | 0.127–2.195 | 0.380 |
| Left Colon | 1.481 | 0.390–5.630 | 0.564 |
| RAS status (ref wild type) | 0.670 | 0.173–2.595 | 0.562 |
| N° line of therapies (ref > 3 lines) | 2.067 | 0.606–7.056 | 0.246 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abbona, A.; Ricci, V.; Paccagnella, M.; Granetto, C.; Ruatta, F.; Cauchi, C.; Galizia, D.; Ghidini, M.; Denaro, N.; Merlano, M.C.; et al. Baseline Cytokine Profile Identifies a Favorable Outcome in a Subgroup of Colorectal Cancer Patients Treated with Regorafenib. Vaccines 2023, 11, 335. https://doi.org/10.3390/vaccines11020335
Abbona A, Ricci V, Paccagnella M, Granetto C, Ruatta F, Cauchi C, Galizia D, Ghidini M, Denaro N, Merlano MC, et al. Baseline Cytokine Profile Identifies a Favorable Outcome in a Subgroup of Colorectal Cancer Patients Treated with Regorafenib. Vaccines. 2023; 11(2):335. https://doi.org/10.3390/vaccines11020335
Chicago/Turabian StyleAbbona, Andrea, Vincenzo Ricci, Matteo Paccagnella, Cristina Granetto, Fiorella Ruatta, Carolina Cauchi, Danilo Galizia, Michele Ghidini, Nerina Denaro, Marco Carlo Merlano, and et al. 2023. "Baseline Cytokine Profile Identifies a Favorable Outcome in a Subgroup of Colorectal Cancer Patients Treated with Regorafenib" Vaccines 11, no. 2: 335. https://doi.org/10.3390/vaccines11020335