
COVID-19 in a Pre-Omicron Era: A Cross-Sectional Immuno-Epidemical and Genomic Evaluation
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Methodology
3. Results and Discussion
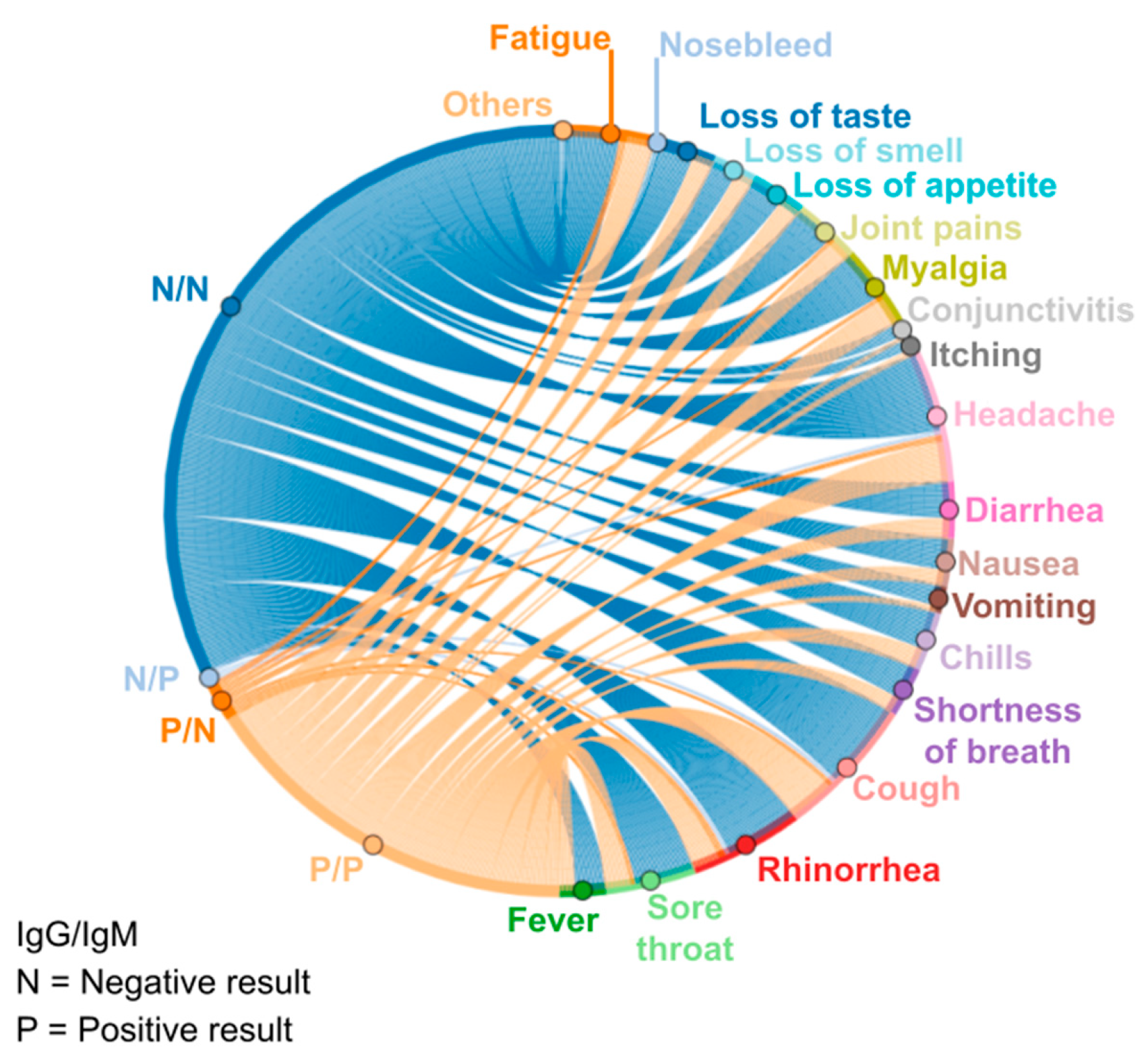
3.1. Frequent Symptoms of the Analyzed Volunteers
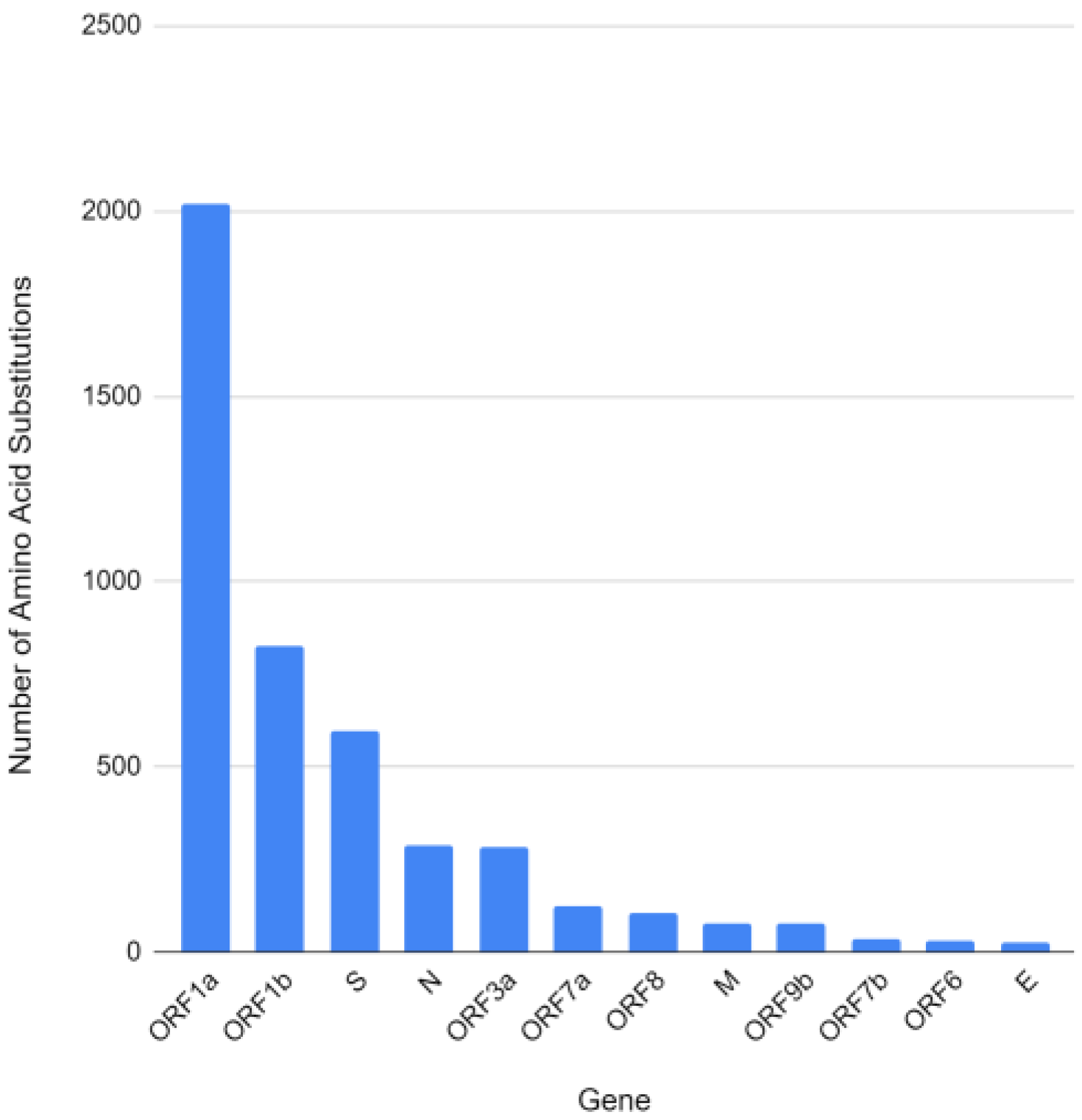
3.2. Genome Evaluation
3.3. Immunological Factors
3.4. Humanistic Perspective
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Director—General’s Opening Remarks at the Media Briefing on COVID-19; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Ciotti, M.; Ciccozzi, M.; Terrinoni, A.; Jiang, W.C.; Wang, C.B.; Bernardini, S. The COVID-19 pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Ponce, D. The impact of coronavirus in Brazil: Politics and the pandemic. Nat. Rev. Nephrol. 2020, 16, 483. [Google Scholar] [CrossRef]
- Boschiero, M.N.; Palamim, C.V.C.; Ortega, M.M.; Mauch, R.M.; Marson, F.A.L. One Year of Coronavirus Disease 2019 (COVID-19) in Brazil: A Political and Social Overview. Ann. Glob. Health 2021, 87, 44. [Google Scholar] [CrossRef]
- Silva, H.M. The danger of denialism: Lessons from the Brazilian pandemic. Bull. Natl. Res. Cent. 2021, 45, 55. [Google Scholar] [CrossRef]
- de Sousa, F.C.B.; Silva, L.C.N.T.; de Sousa, M.A.A.; de Santana, M.A.A.; da Silva, R.B. Protocolos utilizados para diagnóstico de COVID-19. Rev. FAESF 2020, 4. Available online: https://www.faesfpi.com.br/revista/index.php/faesf/article/view/113 (accessed on 15 November 2022). [CrossRef]
- Kopel, J.; Goyal, H.; Perisetti, A. Antibody tests for COVID-19. In Baylor University Medical Center Proceedings; Taylor & Francis: Abingdon, UK, 2021; Volume 34, pp. 63–72. [Google Scholar]
- Haldane, V.; De Foo, C.; Abdalla, S.M.; Jung, A.S.; Tan, M.; Wu, S.; Chua, A.; Verma, M.; Shrestha, P.; Singh, S.; et al. Health systems resilience in managing the COVID-19 pandemic: Lessons from 28 countries. Nat. Med. 2021, 27, 964–980. [Google Scholar] [CrossRef] [PubMed]
- Utku, A.C.; Budak, G.; Karabay, O.; Güçlü, E.; Okan, H.D.; Vatan, A. Main symptoms in patients presenting in the COVID-19 period. Scott. Med. J. 2020, 65, 127–132. [Google Scholar] [CrossRef]
- IBGE, Instituto Brasileiro de Geografia e Estatística. Censo Demográfico: Resultados Preliminares. Cruzeiro-SP. Rio de Janeiro, 2020. Available online: https://cidades.ibge.gov.br/brasil/sp/cruzeiro/panorama (accessed on 28 October 2022).
- Elibol, E. Otolaryngological symptoms in COVID-19. Eur. Arch. Otorhinolaryngol. 2021, 278, 1233–1236. [Google Scholar] [CrossRef]
- Quer, G.; Radin, J.M.; Gadaleta, M.; Baca-Motes, K.; Ariniello, L.; Ramos, E.; Kheterpal, V.; Topol, E.J.; Steinhubl, S.R. Wearable sensor data and self-reported symptoms for COVID-19 detection. Nat. Med. 2021, 27, 73–77. [Google Scholar] [CrossRef]
- Considerations for Implementing and Adjusting Public Health and Social Measures in the Context of COVID-19. Available online: https://www.who.int/publications-detail-redirect/considerations-in-adjusting-public-health-and-social-measures-in-the-context-of-covid-19-interim-guidance (accessed on 29 October 2022).
- Decreto no 65.897, de 30 de Julho de 2021. Available online: https://www.al.sp.gov.br/leis/legislacao-do-estado/ (accessed on 29 October 2022).
- Cortis, D. On determining the age distribution of COVID-19 pandemic. Front. Public Health 2020, 8, 202. [Google Scholar] [CrossRef]
- Werneck, G.L.; Carvalho, M.S. The COVID-19 pandemic in Brazil: Chronicle of a health crisis foretold. Cad. Saude Pública 2020, 36, e00068820. [Google Scholar] [CrossRef]
- Dellière, S.; Salmona, M.; Minier, M.; Gabassi, A.; Alanio, A.; Le Goff, J.; Delaugerre, C.; Chaix, M.-L. Evaluation of the COVID-19 IgG/IgM rapid test from orient gene biotech. J. Clin. Microbiol. 2020, 58, e01233-20. [Google Scholar] [CrossRef] [PubMed]
- Sabatello, M.; Burke, T.B.; McDonald, K.E.; Appelbaum, P.S. Disability, ethics, and health care in the COVID-19 pandemic. Am. J. Public Health 2020, 110, 1523–1527. [Google Scholar] [CrossRef]
- Nunes, R.S.C.; Santa Brígida, M.M.; de Barros, Y.M.R.; Assumpção, R.; da Silva, J.C. Perspectivas da população brasileira sobre as vacinas COVID-19 como método de prevenção. Conjecturas 2021, 21, 246–255. [Google Scholar] [CrossRef]
- Borghetti, A.; Ciccullo, A.; Visconti, E.; Tamburrini, E.; Di Giambenedetto, S. COVID-19 diagnosis does not rule out other concomitant diseases. Eur. J. Clin. Investig. 2020, 50, e13241. [Google Scholar] [CrossRef]
- Salian, V.S.; Wright, J.A.; Vedell, P.T.; Nair, S.; Li, C.; Kandimalla, M.; Tang, X.; Porquera, E.M.C.; Kalari, K.R.; Kandimalla, K.K. COVID-19 transmission, current treatment, and future therapeutic strategies. Mol. Pharm. 2021, 18, 754–771. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, S.; Sreenivasulu, K.; Mitra, P.; Misra, S.; Sharma, P. Role of Genetic Variants and Gene Expression in the Susceptibility and Severity of COVID-19. Ann. Lab. Med. 2021, 41, 129–138. [Google Scholar] [CrossRef]
- Expósito Lara, A.; Feria Díaz, G.E.; González Benítez, S.N.; Soca, P.E.M. Variantes genéticas del SARS-CoV-2 y sus implicaciones clínicas. Medisan 2021, 25, 1424–1446. [Google Scholar]
- Biswas, S.K.; Mudi, S.R. Spike protein D614G and RdRp P323L: The SARS-CoV-2 mutations associated with severity of COVID-19. Genom. Inform. 2020, 18, e44. [Google Scholar] [CrossRef]
- Sharawy, L.; Tantawy, M.; Ahmed, Y.; Taha, A.; Soliman, O.; Ibrahim, T.M.; El-hadidi, M. In-Silico Comparative Analysis of Egyptian SARS CoV-2 with Other Populations: A Phylogeny and Mutation Analysis. In Proceedings of the IEEE 2020 2nd Novel Intelligent and Leading Emerging Sciences Conference (NILES), Giza, Egypt, 24–26 October 2020; pp. 618–622. [Google Scholar]
- Zhang, J.; Cai, Y.; Xiao, T.; Lu, J.; Peng, H.; Sterling, S.M.; Walsh, R.M., Jr.; Rits-Volloch, S.; Zhu, H.; Chen, B. Structural impact on SARS-CoV-2 spike protein by D614G substitution. Science 2021, 372, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Arya, R.; Kumari, S.; Pandey, B.; Mistry, H.; Bihani, S.C.; Das, A.; Prashar, V.; Gupta, G.D.; Panicker, L.; Kumar, M. Structural insights into SARS-CoV-2 proteins. J. Mol. Biol. 2021, 433, 166725. [Google Scholar] [CrossRef]
- Miyata, T.; Miyazawa, S.; Yasunaga, T. Two types of amino acid substitutions in protein evolution. J. Mol. Evol. 1979, 12, 219–236. [Google Scholar] [CrossRef] [PubMed]
- Subissi, L.; Imbert, I.; Ferron, F.; Collet, A.; Coutard, B.; Decroly, E.; Canard, B. SARS-CoV ORF1b-encoded nonstructural proteins 12–16: Replicative enzymes as antiviral targets. Antivir. Res. 2014, 101, 122–130. [Google Scholar] [CrossRef]
- Nawaz, M.S.; Fournier-Viger, P.; Shojaee, A.; Fujita, H. Using artificial intelligence techniques for COVID-19 genome analysis. Appl. Intell. 2021, 51, 3086–3103. [Google Scholar] [CrossRef]
- Sarti, T.D.; Lazarini, W.S.; Fontenelle, L.F.; Almeida, A.P.S.C. Qual o papel da Atenção Primária à Saúde diante da pandemia provocada pela COVID-19? Epidemiol. Serviços Saúde 2020, 29, e2020166. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Li, X.; Zhang, L.; Wan, S.; Zhang, L.; Zhou, F. SARS-CoV-2 Omicron variant: Recent progress and future perspectives. Signal Transduct. Target. Ther. 2022, 7, 141. [Google Scholar] [CrossRef] [PubMed]
- Grudlewska-Buda, K.; Wiktorczyk-Kapischke, N.; Wałecka-Zacharska, E.; Kwiecińska-Piróg, J.; Buszko, K.; Leis, K.; Juszczuk, K.; Gospodarek-Komkowska, E.; Skowron, K. SARS-CoV-2, morphology, transmission and diagnosis during pandemic, review with element of meta-analysis. J. Clin. Med. 2021, 10, 1962. [Google Scholar] [CrossRef] [PubMed]
- Güner, H.R.; Hasanoğlu, İ.; Aktaş, F. COVID-19: Prevention and control measures in community. Turk. J. Med. Sci. 2021, 50, 571–577. [Google Scholar] [CrossRef]
- Xiao, Y.; Torok, M.E. Taking the right measures to control COVID-19. Lancet Infect. Dis. 2020, 20, 523–524. [Google Scholar] [CrossRef] [Green Version]
- Qu, P.; Faraone, J.; Evanus, J.P.; Zou, X.; Zheng, Y.-M.; Carlin, C.; Bednash, J.S.; Lozanski, G.; Mallampali, R.K.; Saif, L.J.; et al. Neutralization of the SARS-CoV-2 omicron BA. 4/5 and BA. 2.12. 1 subvariants. N. Engl. J. Med. 2022, 386, 2526–2528. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.M.A.D.O. Informações sobre o novo coronavírus (COVID-19). Radiol. Bras. 2020, 53, V–VI. [Google Scholar] [CrossRef] [Green Version]
- de Sousa, A.R.; de Carvalho, A.R.B.; de Olivia, E.M.N.; de Lima Brito Magalhães, R.; Moura, M.E.B.; de Freitas, D.R.J. Manifestações sintomáticas da doença causada por coronavírus (COVID-19) em adultos: Revisão sistemática. Rev. Gaúcha Enferm. 2021, 42. [Google Scholar] [CrossRef]
- Escobar, A.L.; Rodriguez, T.D.M.; Monteiro, J.C. Letalidade e características dos óbitos por COVID-19 em Rondônia: Estudo observacional. Epidemiol. Serv. 2021, 30, e2020763. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Pathirana, P.N.; Nguyen, T.; Nguyen, Q.V.H.; Bhatti, A.; Nguyen, D.C.; Abdelrazek, M. Genomic mutations and changes in protein secondary structure and solvent accessibility of SARS-CoV-2 (COVID-19 virus). Sci. Rep. 2021, 11, 3487. [Google Scholar] [CrossRef]
- Marhoon, A.A.; AL-Obaidi, Z.F. Article Review: Molecular Study for Mutation of N-gene and S-gene COVID-19 Virus. Int. J. Res. Appl. Sci. Biotechnol. 2022, 9, 34–44. [Google Scholar]
- Michelon, C.M. Principais variantes do SARS-CoV-2 notificadas no Brasil. RBAC 2021, 53, 109–116. [Google Scholar] [CrossRef]
- Pascoal, D.B.; Carvalho, A.C.S.; Mata, L.E.L.F.S.; Lopes, T.P.; Lopes, L.P.; da Cruz, C.M. Síndrome Respiratória Aguda: Uma resposta imunológica exacerbada ao COVID19 / Acute Respiratory Syndrome: An exacerbated immune response to COVID-19. Braz. J. Health Rev. 2020, 3, 2978–2994. [Google Scholar] [CrossRef]
- Carvalho, V.; Dias, H.; Carneiro, M.; Michelin, L.; Fernanda, C.; Vidal, L.A.T.J.C.; Ferrerira, C.E.S. Serological tests for COVID-19: Interpretation and practical applications. J. Infect. 2020, 9, 1–41. [Google Scholar]
- Agondi, R.C.; Rizzo, L.V.; Kalil, J.; Barros, M. Imunossenescência. Rev. Bras. Alerg. Imunopatol. 2012, 35, 169–176. [Google Scholar]
- Kontou, P.I.; Braliou, G.G.; Dimou, N.L.; Nikolopoulos, G.; Bagos, P.G. Antibody Tests in Detecting SARS-CoV-2 Infection: A Meta-Analysis. Diagnostics 2020, 10, 319. [Google Scholar] [CrossRef]
- Ndwandwe, D.; Wiysonge, C.S. COVID-19 vaccines. Curr. Opin. Immunol. 2021, 71, 111–116. [Google Scholar] [CrossRef]
- Jeyanathan, M.; Afkhami, S.; Smaill, F.; Miller, M.S.; Lichty, B.D.; Xing, Z. Immunological considerations for COVID-19 vaccine strategies. Nat. Rev. Immunol. 2020, 20, 615–632. [Google Scholar] [CrossRef] [PubMed]
- Creech, C.B.; Walker, S.C.; Samuels, R.J. SARS-CoV-2 Vaccines. JAMA 2021, 325, 1318–1320. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Tomlinson, A.C.; Wong, A.H.; Zhou, D.; Desforges, M.; Talbot, P.J.; Benlekbir, B.; Rubinstein, J.L.; Rini, J.M. The human coronavirus HCoV-229E S-protein structure and receptor binding. Elife 2019, 8, e51230. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wang, J.; Xu, X.; Liao, G.; Chen, Y.; Hu, C.H. Patterns of IgG and IgM antibody response in COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 1269–1274. [Google Scholar] [CrossRef]
- Qu, J.; Wu, C.; Li, X.; Zhang, G.; Jiang, Z.; Li, X.; Zhu, Q.; Liu, L. Profile of Immunoglobulin G and IgM Antibodies Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 71, 2255–2258. [Google Scholar] [CrossRef] [PubMed]
- Van Elslande, J.; Houben, E.; Depypere, M.; Brackenier, A.; Desmet, S.; André, E.; Ranst, M.V.; Lagrou, K.; Vermeersch, P. Diagnostic performance of seven rapid IgG/IgM antibody tests and the Euroimmun IgA/IgG ELISA in COVID-19 patients. Clin. Microbiol. Infect. 2020, 26, 1082–1087. [Google Scholar] [CrossRef]
- Olivieri, B.; Betterle, C.; Zanoni, G. Vaccinations and Autoimmune Diseases. Vaccines 2021, 9, 815. [Google Scholar] [CrossRef]
- Vasireddy, D.; Vanaparthy, R.; Mohan, G.; Malayala, S.V.; Atluri, P. Review of COVID-19 variants and COVID-19 vaccine efficacy: What the clinician should know? J. Clin. Med. Res. 2021, 13, 317. [Google Scholar] [CrossRef]
- Barouch, D.H. Covid-19 Vaccines, Immunity, Variants, Boosters. N. Engl. J. Med. 2022, 387, 1011–1020. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Bernal, J.L. Covid-19 vaccine effectiveness against the Omicron (B. 1.1. 529) variant. N. Engl. J. Med. 2021, 386, 1532–1546. [Google Scholar] [CrossRef]
- do Prado, M.F.; de Paula Antunes, B.B.; dos Santos Lourenço Bastos, L.; Peres, I.T.; de Araújo Batista da Silva, A.; Dantas, L.F.; Baião, F.A.; Maçaira, P.; Hamacher, S.; Bozza, F.A. Análise da subnotificação de COVID-19 no Brasil. Rev. Bras. Ter. Intensiva. 2020, 32, 224–228. [Google Scholar]
- Melo, C.M.D.; Silva, G.A.; Melo, A.R.; Freitas, A.C. COVID-19 pandemic outbreak: The Brazilian reality from the first case to the collapse of health services. An. Acad. Bras. Ciências 2020, 92, e20200709. [Google Scholar] [CrossRef] [PubMed]
- e Silva, A.C.S.; Oliveira, E.A.; Martelli, H., Jr. Coronavirus disease pandemic is a real challenge for Brazil. Front. Public Health 2020, 8, 268. [Google Scholar] [CrossRef]
- Caponi, S. Covid-19 no Brasil: Entre o negacionismo e a razão neoliberal. Estud. Av. 2020, 34, 209–224. [Google Scholar] [CrossRef]
- Urban, R.C.; Nakada, L.Y.K. COVID-19 pandemic: Solid waste and environmental impacts in Brazil. Sci. Total Environ. 2021, 755, 142471. [Google Scholar] [CrossRef]
- Abers, R.N.; Rossi, F.M.; von Bülow, M. State–society relations in uncertain times: Social movement strategies, ideational contestation and the pandemic in Brazil and Argentina. Int. Political Sci. Rev. 2021, 42, 333–349. [Google Scholar] [CrossRef]
- Silva, G.A.e.; Jardim, B.C.; dos Santos, C.V.B. Excesso de mortalidade no Brasil em tempos de COVID-19. Ciênc Saúde Coletiva 2020, 25, 3345–3354. [Google Scholar]
- Santos, J.L.G.D.; Balsanelli, A.P.; Freitas, E.D.O.; Menegon, F.H.A.; Carneiro, I.A.; Lazzari, D.D.; Camponogara, S. Work environment of hospital nurses during the COVID-19 pandemic in Brazil. Int. Nurs. Rev. 2021, 68, 228–237. [Google Scholar] [CrossRef]
- Noronha, K.V.M.D.S.; Guedes, G.R.; Turra, C.M.; Andrade, M.V.; Botega, L.; Nogueira, D.; Ferreira, M.F. The COVID-19 pandemic in Brazil: Analysis of supply and demand of hospital and ICU beds and mechanical ventilators under different scenarios. Cad. Saúde Pública 2020, 36, e00115320. [Google Scholar] [CrossRef]
- Dantas, E.S.O. Saúde mental dos profissionais de saúde no Brasil no contexto da pandemia por Covid-19. Interface Comun. Saúde Educ. 2021, 25. [Google Scholar] [CrossRef]
- Ruckert, A.; Zinszer, K.; Zarowsky, C.; Labonté, R.; Carabin, H. What role for One Health in the COVID-19 pandemic? Can. J. Public Health 2020, 111, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.; de Oliveira, G.F.; Franco, J.C.; de Assis, I.B.; Banwo, K.; Pagnossa, J.P. One Health and a Computational Biology approach. Res. Soc. Dev. 2022, 11, e02111437105–e02111437105. [Google Scholar] [CrossRef]
- Mushi, V. The holistic way of tackling the COVID-19 pandemic: The one health approach. Trop. Med. Health 2020, 48, 69. [Google Scholar] [CrossRef] [PubMed]
- Trilla, A. One world, one health: The novel coronavirus COVID-19 epidemic. Med. Clin. 2020, 154, 175. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Viral Agents | Bacterial Agents | ||
|---|---|---|---|
| Adenovirus | Enterovirus | Parainfluenza virus | Chlamydophila pneumoniae |
| Bocavirus | Influenza | Rhinovirus | Mycoplasma pneumoniae |
| Coronavirus (except SARS-CoV-2) | Metapneumovirus | Respiratory Syncytial virus (RSV) | Mycobacterium tuberculosis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pagnossa, J.P.; Rodrigues, S.d.O.; Oliveira, G.F.d.; Adnan, M.; Aljaid, M.S.; Assis, I.B.d.; Lima, A.S.G.; Patel, M.; Ogaly, H.A.; Batiha, G.E.-S. COVID-19 in a Pre-Omicron Era: A Cross-Sectional Immuno-Epidemical and Genomic Evaluation. Vaccines 2023, 11, 272. https://doi.org/10.3390/vaccines11020272
Pagnossa JP, Rodrigues SdO, Oliveira GFd, Adnan M, Aljaid MS, Assis IBd, Lima ASG, Patel M, Ogaly HA, Batiha GE-S. COVID-19 in a Pre-Omicron Era: A Cross-Sectional Immuno-Epidemical and Genomic Evaluation. Vaccines. 2023; 11(2):272. https://doi.org/10.3390/vaccines11020272
Chicago/Turabian StylePagnossa, Jorge Pamplona, Sarah de Oliveira Rodrigues, Gabriel Ferrari de Oliveira, Mohd Adnan, Maryam Saud Aljaid, Isabela Bacelar de Assis, Alex Sandro Gomes Lima, Mitesh Patel, Hanan A. Ogaly, and Gaber El-Saber Batiha. 2023. "COVID-19 in a Pre-Omicron Era: A Cross-Sectional Immuno-Epidemical and Genomic Evaluation" Vaccines 11, no. 2: 272. https://doi.org/10.3390/vaccines11020272