

Real-World Efficacy of COVID-19 Pre-Exposure Prophylaxis with Tixagevimab/Cilgavimab in People with Multiple Sclerosis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
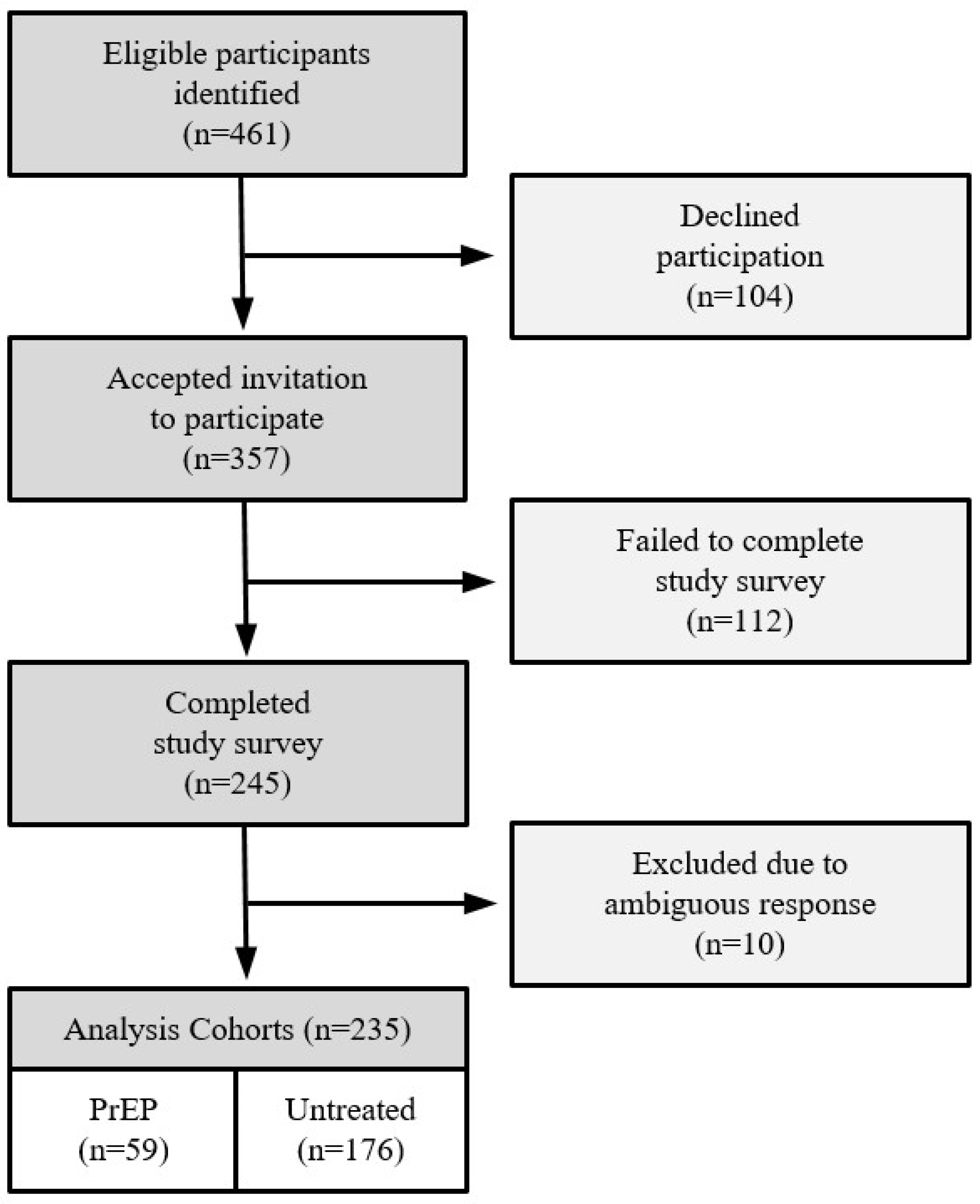
2.2. Study Participants
2.3. Data Analysis
2.4. Ethics
3. Results
3.1. Baseline Demographics
3.2. COVID-19 Infections
3.3. Post Hoc Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 1 April 2022).
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Jaber, A.; Patel, M.; Sylvester, A.; Yarussi, M.; Kalina, J.T.; Mendoza, J.P.; Avila, R.L.; Tremblay, M.A. COVID-19 Vaccine Response in People with Multiple Sclerosis Treated with Dimethyl Fumarate, Diroximel Fumarate, Natalizumab, Ocrelizumab, or Interferon Beta Therapy. Neurol Ther. 2023, 12, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Achiron, A.; Mandel, M.; Dreyer-Alster, S.; Harari, G.; Magalashvili, D.; Sonis, P.; Dolev, M.; Menascu, S.; Flechter, S.; Falb, R.; et al. Humoral immune response to COVID-19 mRNA vaccine in patients with multiple sclerosis treated with high-efficacy disease-modifying therapies. Ther. Adv. Neurol. Disord. 2021, 14, 17562864211012835. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, J.J., Jr.; Mittl, K.; Rowles, W.M.; McPolin, K.; Rajan, J.V.; Laurie, M.T.; Zamecnik, C.R.; Dandekar, R.; Alvarenga, B.D.; Loudermilk, R.P.; et al. Multiple sclerosis therapies differentially affect SARS-CoV-2 vaccine-induced antibody and T cell immunity and function. JCI Insight 2022, 7, e156978. [Google Scholar] [CrossRef] [PubMed]
- Bar-Or, A.; Calkwood, J.C.; Chognot, C.; Evershed, J.; Fox, E.J.; Herman, A.; Manfrini, M.; McNamara, J.; Robertson, D.S.; Stokmaier, D.; et al. Effect of ocrelizumab on vaccine responses in patients with multiple sclerosis: The VELOCE study. Neurology 2020, 95, e1999–e2008. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.J.; Ustianowski, A.; De Wit, S.; Launay, O.; Avila, M.; Templeton, A.; Yuan, Y.; Seegobin, S.; Ellery, A.; Levinson, D.J.; et al. Intramuscular AZD7442 (Tixagevimab-Cilgavimab) for Prevention of COVID-19. N. Engl. J. Med. 2022, 386, 2188–2200. [Google Scholar] [CrossRef]
- VanBlargan, L.A.; Errico, J.M.; Halfmann, P.J.; Zost, S.J.; Crowe, J.E., Jr.; Purcell, L.A.; Kawaoka, Y.; Corti, D.; Fremont, D.H.; Diamond, M.S. An infectious SARS-CoV-2 B.1.1.529 Omicron virus escapes neutralization by therapeutic monoclonal antibodies. Nat. Med. 2022, 28, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Dejnirattisai, W.; Huo, J.; Zhou, D.; Zahradník, J.; Supasa, P.; Liu, C.; Duyvesteyn, H.M.E.; Ginn, H.M.; Mentzer, A.J.; Tuekprakhon, A.; et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell 2022, 185, 467–484.e15. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Velay, A.; Gautier-Vargas, G.; Olagne, J.; Obrecht, A.; Cognard, N.; Heibel, F.; Braun-Parvez, L.; Keller, N.; Martzloff, J.; et al. Breakthrough COVID-19 cases despite prophylaxis with 150 mg of tixagevimab and 150 mg of cilgavimab in kidney transplant recipients. Am. J. Transplant. 2022, 22, 2675–2681. [Google Scholar] [CrossRef]
- Ma, K.C.; Shirk, P.; Lambrou, A.S.; Hassell, N.; Zheng, X.-Y.; Payne, A.B.; Ali, A.R.; Batra, D.; Caravas, J.; Chau, R.; et al. Genomic Surveillance for SARS-CoV-2 Variants: Circulation of Omicron Lineages—United States, January 2022–May 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 651–656. [Google Scholar] [CrossRef]
- Soeroto, A.Y.; Yanto, T.A.; Kurniawan, A.; Hariyanto, T.I. Efficacy and safety of tixagevimab-cilgavimab as pre-exposure prophylaxis for COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2023, 33, e2420. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zheng, J.; Zhu, K.; Xu, C.; Wang, D.; Hou, M. The effect of tixagevimab-cilgavimab on clinical outcomes in patients with COVID-19: A systematic review with meta-analysis. J. Infect. 2023, 86, e15–e17. [Google Scholar] [CrossRef] [PubMed]
- Jondreville, L.; D’Aveni, M.; Labussière-Wallet, H.; Le Bourgeois, A.; Villate, A.; Berceanu, A.; Bezsera, S.-M.; Thiebaut, A.; Boissard-Simonet, M.; Legrand, M.; et al. Pre-exposure prophylaxis with tixagevimab/cilgavimab (AZD7442) prevents severe SARS-CoV-2 infection in recipients of allogeneic hematopoietic stem cell transplantation during the Omicron wave: A multicentric retrospective study of SFGM-TC. J. Hematol. Oncol. 2022, 15, 169. [Google Scholar] [CrossRef] [PubMed]
- Ocon, A.J.; Mustafa, S.S. Real-World Experience of Tixagevimab and Cilgavimab (Evusheld) in Rheumatologic Patients on Rituximab. J. Clin. Rheumatol. 2022, 29, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Planas, D.; Bruel, T.; Staropoli, I.; Guivel-Benhassine, F.; Porrot, F.; Maes, P.; Grzelak, L.; Prot, M.; Mougari, S.; Planchais, C.; et al. Resistance of Omicron subvariants BA.2.75.2, BA.4.6 and BQ.1.1 to neutralizing antibodies. bioRxiv 2022. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administation. FDA Announces Evusheld Is Not Currently Authorized for Emergency Use in the U.S. 26 January 2023. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-announces-evusheld-not-currently-authorized-emergency-use-us (accessed on 5 June 2023).
- Evans, R.A.; Dube, S.; Lu, Y.; Yates, M.; Arnetorp, S.; Barnes, E.; Bell, S.; Carty, L.; Evans, K.; Graham, S.; et al. Impact of COVID-19 on immunocompromised populations during the Omicron Era: Insights from the observational population-based INFORM study. Lancet Reg. Health Eur. 2023, 35, 100747. [Google Scholar] [CrossRef]
- ClinicalTrials.gov NCT05648110. Available online: https://clinicaltrials.gov/study/NCT05648110 (accessed on 9 December 2023).


{kind=link}
| Demographics | |||
|---|---|---|---|
| PrEP | Untreated | p-Value | |
| n | 59 | 176 | |
| Age, mean (SD) | 56.4 (11.0) | 49.1 (12.1) | <0.0001 |
| Female, n (%) | 42 (71.2%) | 124 (70.5%) | >0.9999 |
| MS Subtype *, n (%) | |||
| Relapsing | 36 (66.7%) | 116 (75.8%) | 0.2116 |
| Progressive | 18 (33.3%) | 37 (24.2%) | |
| DMT, n (%) | |||
| Ocrelizumab | 30 (50.8%) | 120 (68.2%) | 0.053 |
| Ofatumumab | 2 (3.4%) | 5 (2.8%) | |
| Rituximab | 27 (45.8%) | 51 (29.0%) | |
| Vaccination Status, n (%) | |||
| Vaccinated | 57 (96.6%) | 151 (85.8%) | 0.0312 |
| Unvaccinated | 2 (3.4%) | 25 (14.2%) | |
| COVID-19 History, n (%) | |||
| Prior COVID-19 | 12 (20.3%) | 72 (40.9%) | 0.0046 |
| Uninfected | 47 (79.7%) | 104 (59.1%) | |
| PrEP (n = 59) | Untreated (n = 176) | p-Value OR (95% CI) | |
|---|---|---|---|
| COVID-19 Infection | 9 (15.3%) | 50 (28.4%) | 0.0557 |
| No Infection | 50 (84.7%) | 126 (71.6%) | OR = 0.4536 (0.2046 to 0.9599) |
| Hospitalization | 0 (0%) | 2 (4%) | NA |
| ICU Admission | 0 (0%) | 1 (2%) | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elias, L.B.; Jaber, A.; Manzano, M.; Leekoff, M.; Sylvester, A.; Tremblay, M.A. Real-World Efficacy of COVID-19 Pre-Exposure Prophylaxis with Tixagevimab/Cilgavimab in People with Multiple Sclerosis. Vaccines 2023, 11, 1855. https://doi.org/10.3390/vaccines11121855
Elias LB, Jaber A, Manzano M, Leekoff M, Sylvester A, Tremblay MA. Real-World Efficacy of COVID-19 Pre-Exposure Prophylaxis with Tixagevimab/Cilgavimab in People with Multiple Sclerosis. Vaccines. 2023; 11(12):1855. https://doi.org/10.3390/vaccines11121855
Chicago/Turabian StyleElias, Luke B., Aliya Jaber, Margarita Manzano, Mark Leekoff, Andrew Sylvester, and Matthew A. Tremblay. 2023. "Real-World Efficacy of COVID-19 Pre-Exposure Prophylaxis with Tixagevimab/Cilgavimab in People with Multiple Sclerosis" Vaccines 11, no. 12: 1855. https://doi.org/10.3390/vaccines11121855