
A Multi-Center Study Investigating Long COVID-19 in Healthcare Workers from North-Eastern Italy: Prevalence, Risk Factors and the Impact of Pre-Existing Humoral Immunity—ORCHESTRA Project
 , , , , ,
, , , , ,  , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- (a)
- Socio-demographic profile of the responder (including country of birth, ethnicity, marital status, educational level);
- (b)
- Smoking habit;
- (c)
- Any COVID-19 infection, including date of positive swab test, time between 1st and 2nd or 2nd and 3rd infection, days of viral shedding time (VST), eventual hospitalization, length of hospital stay, and admission to intensive care unit;
- (d)
- Date of COVID-19 vaccination, vaccine type, and vaccination status (0, 1, 2, 3, or 4 doses) before any SARS-CoV-2 infection;
- (e)
- Any symptoms developed during acute COVID-19 disease or after first negative swab test;
- (f)
- Post-COVID-19 symptoms persisting after acute disease (i.e., after first negative swab test);
- (g)
- Post-COVID-19 symptoms newly developed after first negative swab;
- (h)
- Long-COVID-19 syndrome (defined as the presence of any symptom) at 30–60 days or 61+ days since after first negative swab;
- (i)
- Any pre-existing condition (defined as morbidities with a medical diagnosis under treatment).
- (a)
- Diabetes therapy;
- (b)
- Cardio-vascular therapy;
- (c)
- Respiratory therapy;
- (d)
- Liver therapy;
- (e)
- Neurological therapy;
- (f)
- Rheumatologic therapy;
- (g)
- Immune-depression (sickle-cell disease, splenectomy, congenital immune-deficiency, HIV, other, none, unanswered)
2.1. Study Endpoints
- At 30–60 days: (yes vs. no);
- At 60+ days (yes vs. no).
- Overall symptoms present after first negative swab for COVID-19 (yes vs. no);
- Symptoms persisting since acute COVID-19 (yes vs. no);
- Symptoms newly developed after first negative swab for COVID-19, but not present during acute disease (yes. vs. no).
- General infectious symptoms (N = 7);
- Otolaryngological (earn–nose–throat; ENT) symptoms (N = 6);
- Pulmonary symptoms (N = 3);
- Gastro-enteric symptoms (N = 4);
- Psychological symptoms (N = 3);
- Neurological symptoms (N = 8).
2.2. Statistical Analysis
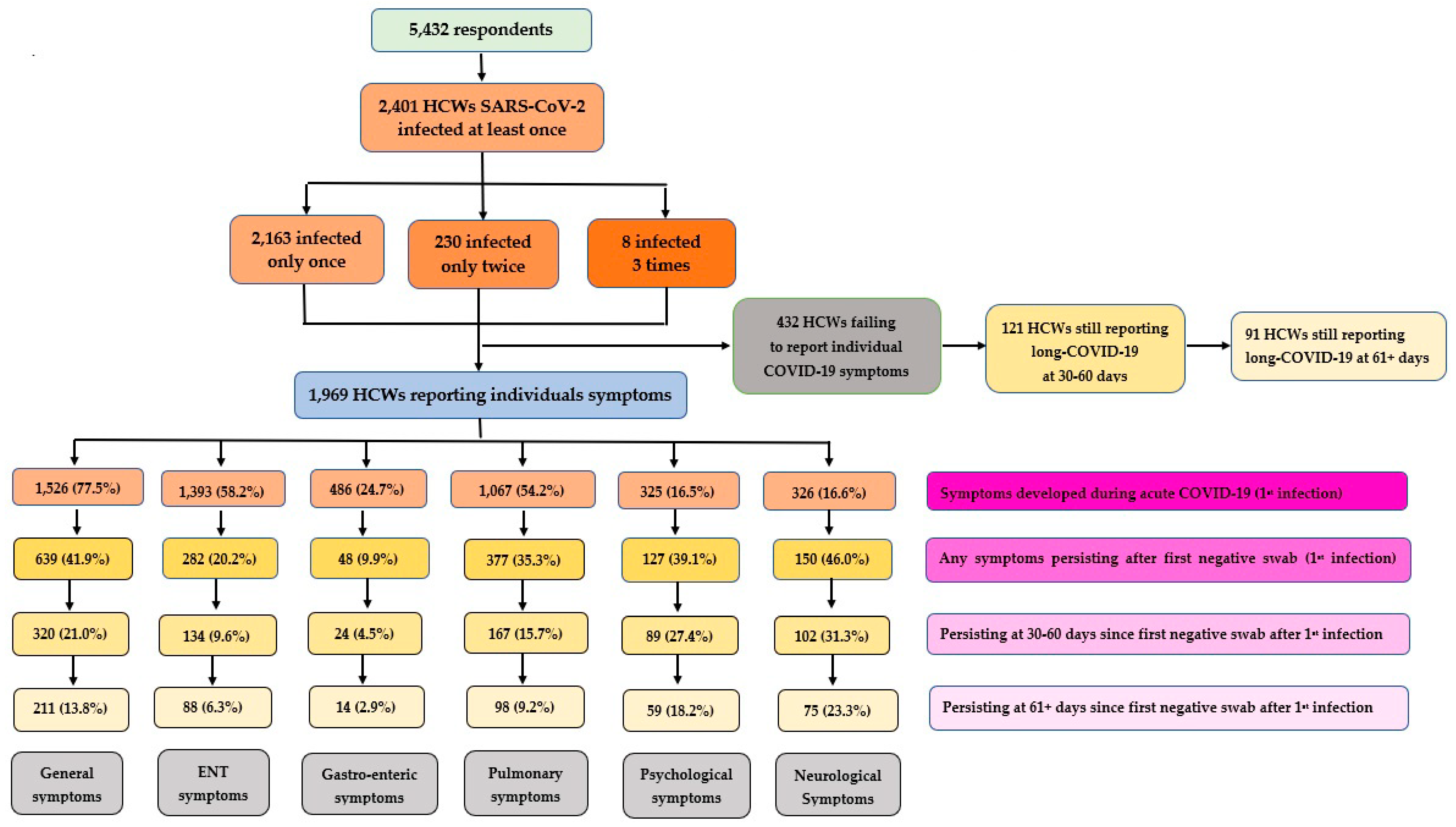
3. Results
3.1. Descriptive Analysis
3.1.1. Socio-Demographic Profile and Medical History of Interviewees
3.1.2. COVID-19 Vaccine Uptake
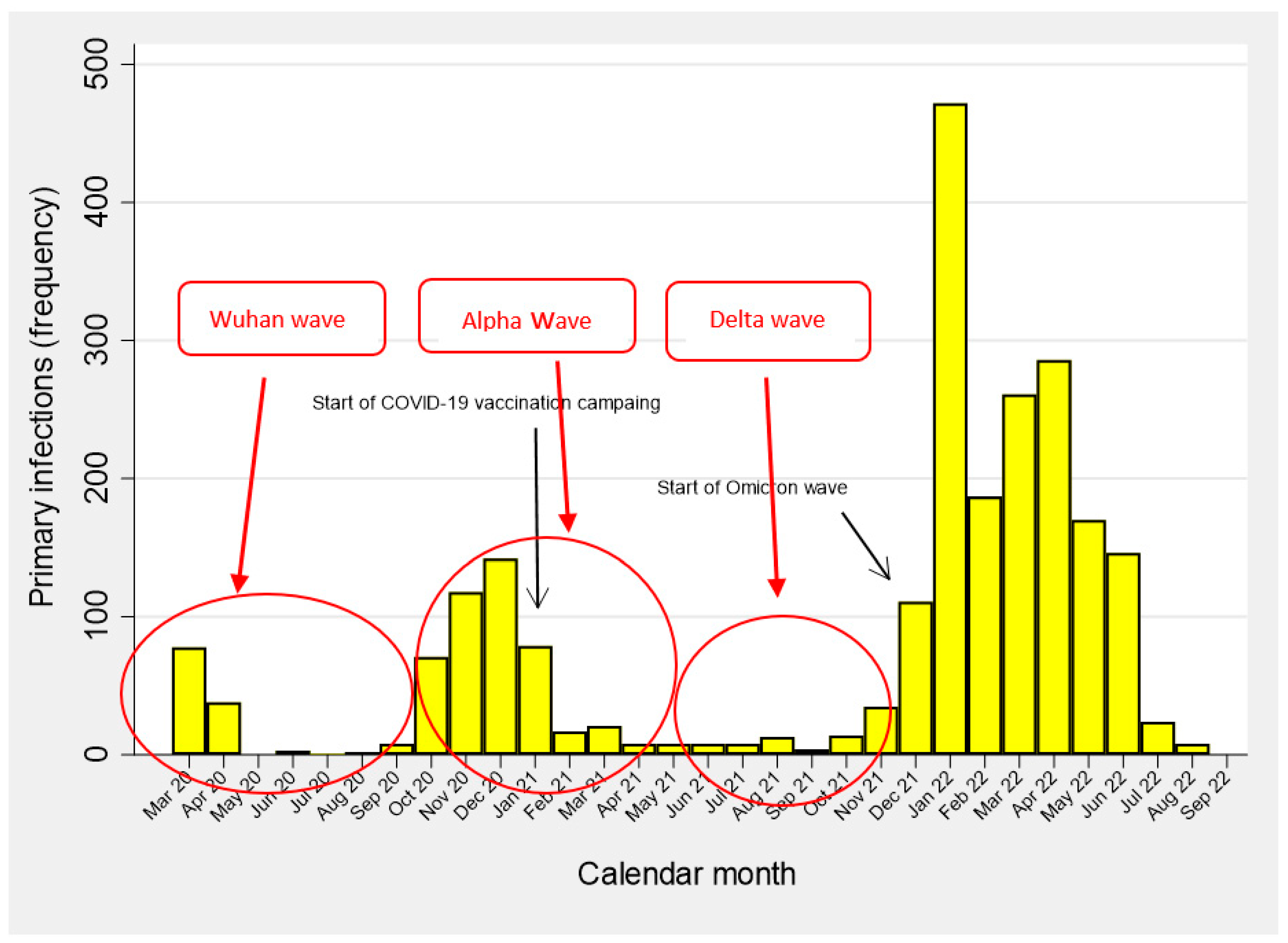
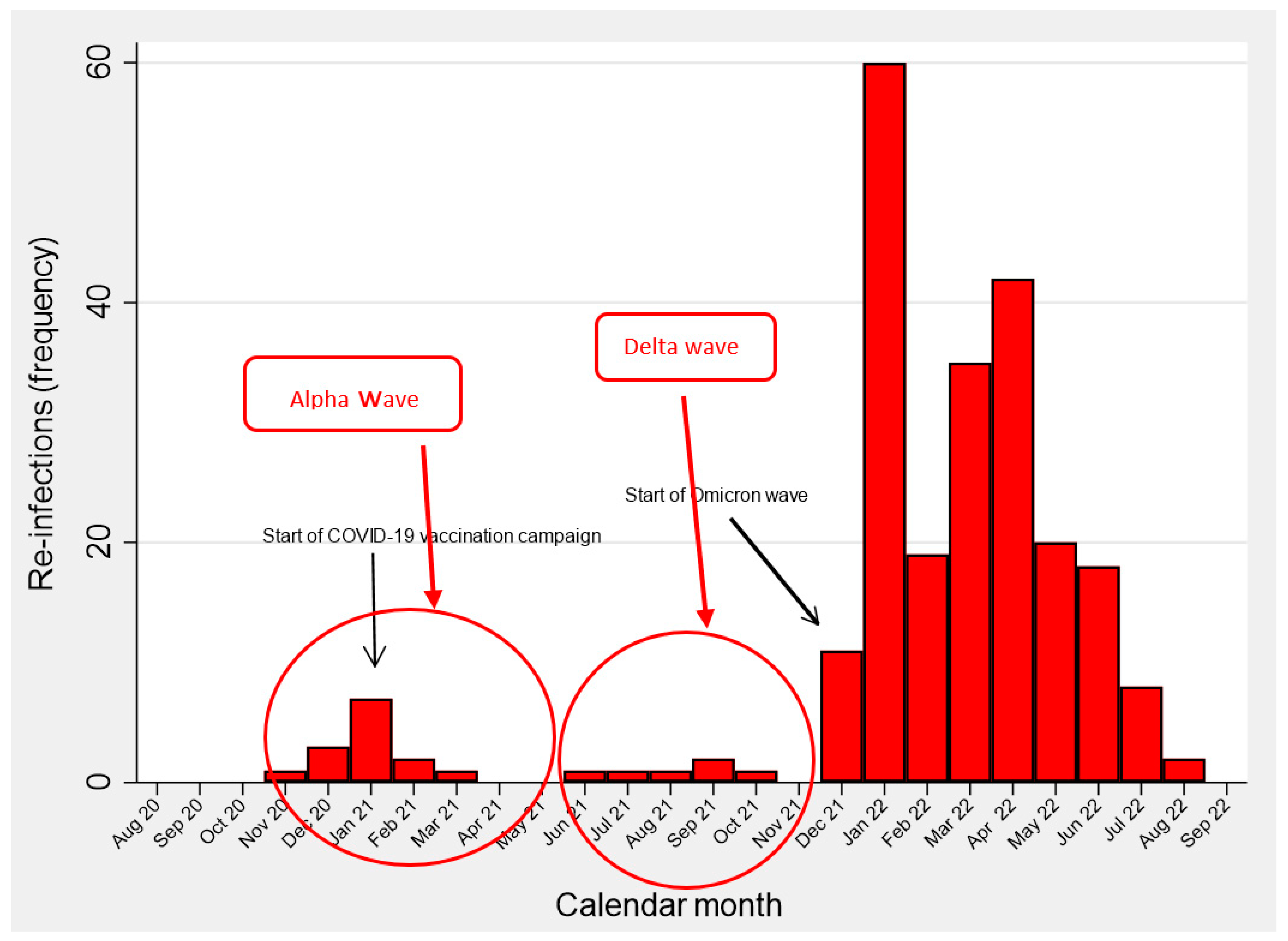
3.1.3. SARS-CoV-2 Infections
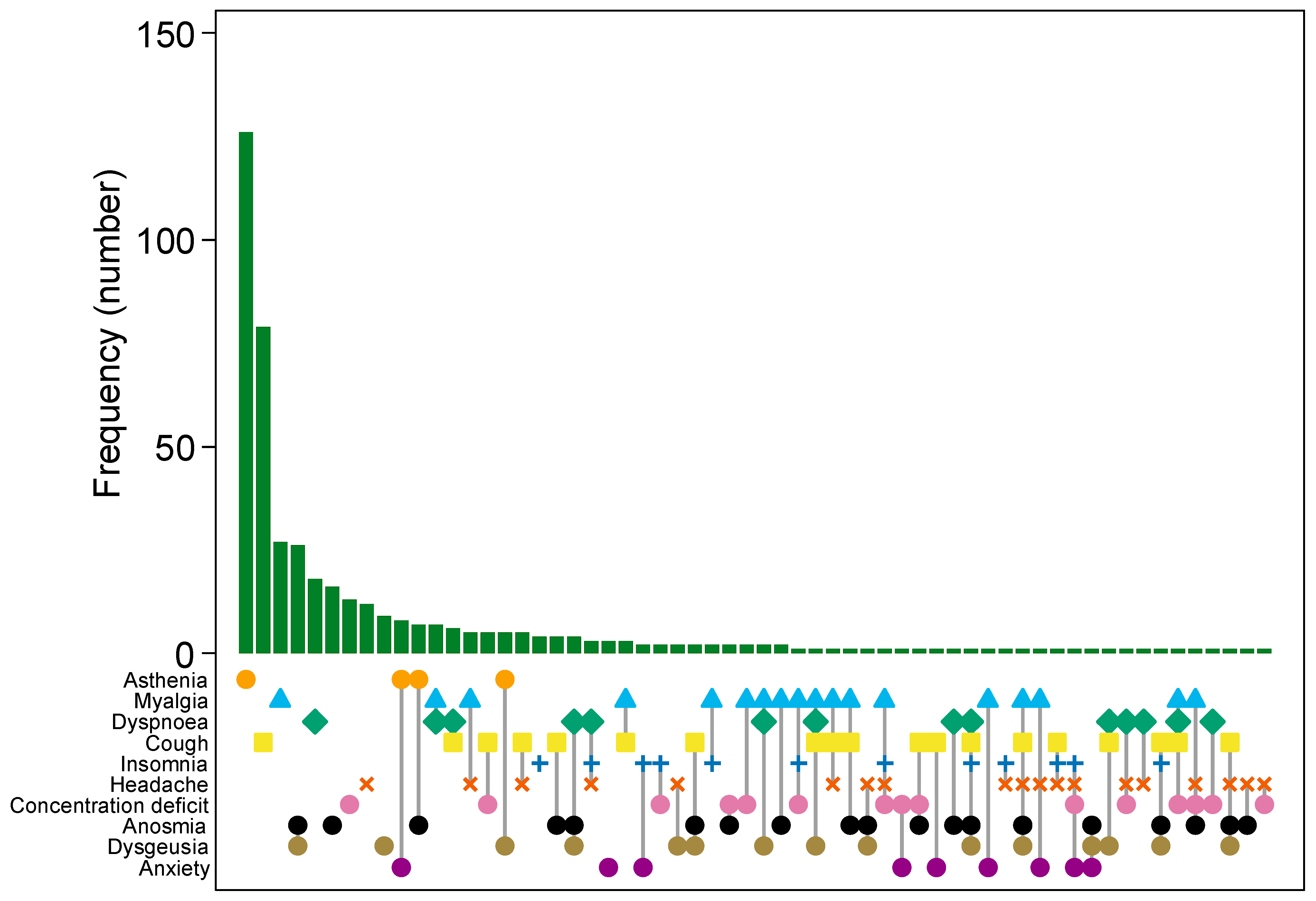
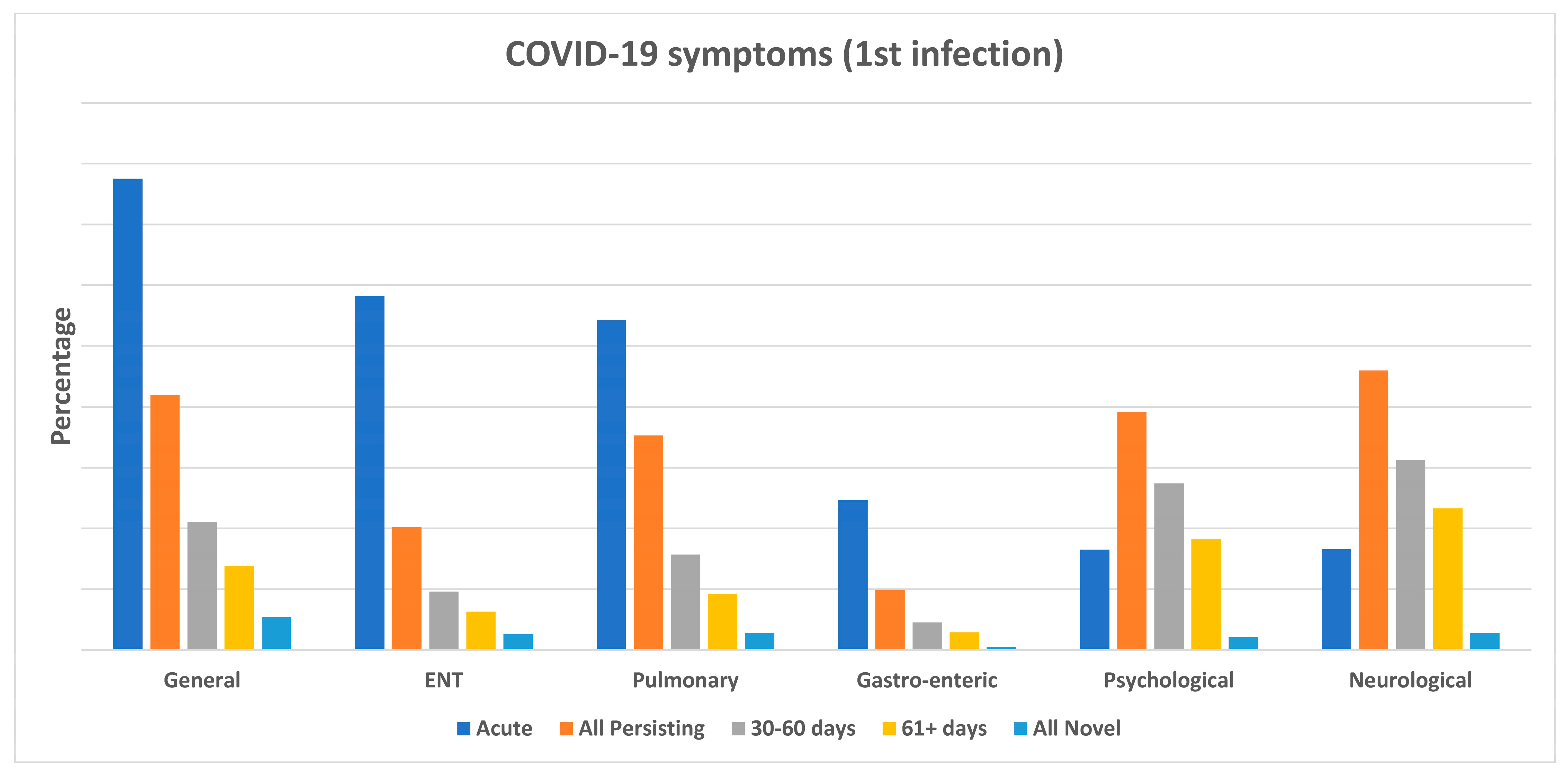
3.1.4. Acute and Post-COVID-19 Symptoms
3.2. Logistic Regression Analysis
4. Discussion
4.1. Key Findings
4.2. Prevalence of Long COVID-19
4.3. Post-COVID-19 Symptoms
- Is a chronic and dominant symptom;
- Is frequently combined with other symptoms;
- Impacts the majority of everyday life activities;
- Developed during acute COVID-19, persisting at least 30 days afterwards;
- Did not manifest during acute COVID-19, but newly developed shortly after the first negative swab, persisting at least 30 days afterwards.
4.4. Risk Factors for Long COVID-19
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garner, P. BMJ Opinion. Paul Garner: For 7 weeks I have Been through a Roller Coaster of Ill Health, Extreme Emotions, and Utter Exhaustion. 2020. Available online: https://blogs.bmj.com/bmj/2020/05/05/paul-garner-peoplewho-have-a-more-protracted-illness-need-help-to-understand-andcope-with-the-constantly-shifting-bizarre-symptoms/ (accessed on 5 November 2022).
- Perego, E.; Callard, F.; Stras, L.; Melville-Jóhannesson, B.; Pope, R.; Alwan, N.A. Why the patient-made term ‘long covid’ is needed. Wellcome Open Res. 2020, 5, 224. [Google Scholar] [CrossRef]
- Yongu, W.T. A Critical Review of Levels of Disease Development and Prevention in Epidemiology. Int. J. Hum. Kinet. Health Educ. 2022, 6. Available online: https://journals.aphriapub.com/index.php/IJoHKHE/article/view/1490 (accessed on 5 November 2022).
- Shukla, A.K.; Atal, S.; Banerjee, A.; Jhaj, R.; Balakrishnan, S.; Chugh, P.K.; Xavier, D.; Faruqui, A.; Singh, A.; Raveendran, R.; et al. An observational multi-centric COVID-19 sequelae study among health care workers. Lancet Reg. Health Southeast. Asia 2023, 10, 100129. [Google Scholar] [CrossRef]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition2021.1 (accessed on 5 November 2022).
- National Institute for Health and Care Excellence (NICE). COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. Available online: https://www.nice.org.uk/guidance/NG188 (accessed on 5 November 2022).
- Centers for Disease Control and Prevention (CDC). Post-COVID Conditions: Overview for Healthcare Providers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html# (accessed on 5 November 2022).
- US Department of Health & Human Services. Guidance on “Long COVID” as a Disability under the ADA, Section 504, and Section 1557. 2021. Available online: https://www.hhs.gov/civil-rights/for-providers/civil-rights-covid19/guidance-long-covid-disabil-dity/index.html (accessed on 23 October 2023).
- Haslam, A.; Olivier, T.; Prasad, V. The definition of long COVID used in interventional studies. Eur. J. Clin. Investig. 2023, 53, e13989. [Google Scholar] [CrossRef] [PubMed]
- Woodrow, M.; Carey, C.; Ziauddeen, N.; Thomas, R.; Akrami, A.; Lutje, V.; Greenwood, D.C.; Alwan, N.A. Systematic Review of the Prevalence of Long COVID. Open Forum Infect. Dis. 2023, 10, ofad233. [Google Scholar] [CrossRef] [PubMed]
- Lorettu, L.; Mastrangelo, G.; Stepien, J.; Grabowski, J.; Meloni, R.; Piu, D.; Michalski, T.; Waszak, P.M.; Bellizzi, S.; Cegolon, L. Attitudes and Perceptions of Health Protection Measures Against the Spread of COVID-19 in Italy and Poland. Front. Psychol. 2021, 12, 805790. [Google Scholar] [CrossRef]
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef]
- O’Mahoney, L.L.; Routen, A.; Gillies, C.; Ekezie, W.; Welford, A.; Zhang, A.; Karamchandani, U.; Simms-Williams, N.; Cassambai, S.; Ardavani, A.; et al. The prevalence and long-term health effects of Long Covid among hospitalised and non-hospitalised populations: A systematic review and meta-analysis. eClinicalMedicine 2023, 55, 101762. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long covid-mechanisms, risk factors, and management. BMJ 2021, 374, n1944. [Google Scholar] [CrossRef]
- Koc, H.C.; Xiao, J.; Liu, W.; Li, Y.; Chen, G. Long COVID and its Management. Int. J. Biol. Sci. 2022, 18, 4768–4780. [Google Scholar] [CrossRef]
- Sansone, D.; Tassinari, A.; Valentinotti, R.; Kontogiannis, D.; Ronchese, F.; Centonze, S.; Maggiore, A.; Cegolon, L.; Larese Filon, F. Persistence of Symptoms 15 Months since COVID-19 Diagnosis: Prevalence, Risk Factors and Residual Work Ability. Life 2022, 13, 97. [Google Scholar] [CrossRef] [PubMed]
- Cegolon, L.; Magnano, G.; Negro, C.; Larese Filon, F.; ORCHESTRA Working Group. SARS-CoV-2 Reinfections in Health-Care Workers, 1 March 2020–31 January 2023. Viruses 2023, 15, 1551. [Google Scholar] [CrossRef] [PubMed]
- Cegolon, L.; Ronchese, F.; Ricci, F.; Negro, C.; Larese-Filon, F. SARS-CoV-2 Infection in Health Care Workers of Trieste (North-Eastern Italy), 1 October 2020–7 February 2022: Occupational Risk and the Impact of the Omicron Variant. Viruses 2022, 28, 1663. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Excess Mortality Collaborators. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Kuppuswamy, A. The fatigue conundrum. Brain 2017, 140, 2240–2245. [Google Scholar] [CrossRef]
- Sandler, C.X.; Wyller, V.B.B.; Moss-Morris, R.; Buchwald, D.; Crawley, E.; Hautvast, J.; Katz, B.Z.; Knoop, H.; Little, P.; Taylor, R.; et al. Long COVID and Post-infective Fatigue Syndrome: A Review. Open Forum Infect. Dis. 2021, 8, ofab440. [Google Scholar] [CrossRef]
- Borges do Nascimento, I.J.; von Groote, T.C.; O’Mathuna, D.P.; Abdulazeem, H.M.; Henderson, C.; Jayarajah, U.; Weerasekara, I.; Poklepovic Pericic, T.; Klapproth, H.E.; Puljak, L.; et al. Clinical, laboratory and radiological characteristics and outcomes of novel coronavirus (SARSCoV-2) infection in humans: A systematic review and series of meta-analyses. PLoS ONE 2020, 15, e0239235. [Google Scholar] [CrossRef]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized COVID-19 “long haulers”. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef]
- Sykes, D.L.; Holdswoth, L.; Jawad, N. Post-COVID-19 Symptom Burden: What is Long-COVID and How Should We Manage It? Lung 2021, 199, 113–119. [Google Scholar] [CrossRef]
- Katz, B.Z.; Collin, S.M.; Murphy, G.; Katz, B.Z.; Collin, S.M.; Murphy, G.; Moss-Morris, R.; Wyller, V.B.; Wensaas, K.A.; Hautvast, J.L.; et al. The international Collaborative on Fatigue Following Infection (COFFI). Fatigue 2018, 6, 106–121. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A.; International Chronic Fatigue Syndrome Study Group. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Piraino, B.; Vollmer-Conna, U.; Lloyd, A.R. Genetic associations of fatigue and other symptom domains of the acute sickness response to infection. Brain Behav. Immun. 2012, 26, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Cvejic, E.; Li, H.; Hickie, I.B.; Wakefield, D.; Lloyd, A.R.; Vollmer-Conna, U. Contribution of individual psychological and psychosocial factors to symptom severity and time-to-recovery after naturally occurring acute infective illness: The Dubbo Infection Outcomes Study (DIOS). Brain Behav. Immun. 2019, 82, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Theorell, T.; Blomkvist, V.; Lindh, G.; Evengård, B. Critical life events, infections, and symptoms during the year preceding chronic fatigue syndrome (CFS): An examination of CFS patients and subjects with a nonspecific life crisis. Psychosom. Med. 1999, 61, 304–310. [Google Scholar] [CrossRef]
- Jackson, M.L.; Bruck, D. Sleep abnormalities in chronic fatigue syndrome/myalgic encephalomyelitis: A review. J. Clin. Sleep. Med. 2012, 8, 719–728. [Google Scholar] [CrossRef]
- Nelson, M.J.; Bahl, J.S.; Buckley, J.D.; Thomson, R.L.; Davison, K. Evidence of altered cardiac autonomic regulation in myalgic encephalomyelitis/chronic fatigue syndrome: A systematic review and meta-analysis. Medicine 2019, 98, e17600. [Google Scholar] [CrossRef]
- Papadopoulos, A.S.; Cleare, A.J. Hypothalamic-pituitary-adrenal axis dysfunction in chronic fatigue syndrome. Nat. Rev. Endocrinol. 2011, 8, 22–32. [Google Scholar] [CrossRef]
- Afari, N.; Buchwald, D. Chronic fatigue syndrome: A review. Am. J. Psychiatry 2003, 160, 221–236. [Google Scholar] [CrossRef]
- Huntley, C.C.; Patel, K.; Mobeen, F.; Armitage, M.N.; Pye, A.; Knight, C.B.; Mostafa, A.; Kershaw, M.; Mughal, A.Z.; McKemey, E.; et al. Pulmonary function test and computed tomography features during follow-up after SARS, MERS and COVID-19: A systematic review and meta-analysis. ERJ Open Res. 2022, 8, 00056–2022. [Google Scholar] [CrossRef]
- McElvaney, O.J.; McEvoy, N.L.; McElvaney, O.F.; Carroll, T.P.; Murphy, M.P.; Dunlea, D.M.; Ní Choileáin, O.; Clarke, J.; O’Connor, E.; Hogan, G.; et al. Characterization of the inflammatory response to severe COVID-19 illness. Am. J. Respir. Crit. Care Med. 2020, 202, 812–821. [Google Scholar] [CrossRef]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-month follow-up chest CT findings after severe covid-19 pneumonia. Radiology 2021, 299, E177–E186. [Google Scholar] [CrossRef] [PubMed]
- Bennett, B.K.; Goldstein, D.; Chen, M.; Davenport, T.A.; Vollmer-Conna, U.; Scott, E.M.; Hickie, I.B.; Lloyd, A.R. Characterization of fatigue states in medicine and psychiatry by structured interview. Psychosom. Med. 2014, 76, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. eClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Cegolon, L.; Pol, R.; Simonetti, O.; Larese Filon, F.; Luzzati, R. Molnupiravir, Nirmatrelvir/Ritonavir, or Sotrovimab for High-Risk C OVID-19 Patients Infected by the Omicron Variant: Hospitalization, Mortality, and Time until Negative Swab Test in Real Life. Pharmaceuticals 2023, 16, 721. [Google Scholar] [CrossRef] [PubMed]
- UK Government. NERVTAG: Update Note on B.1.1.7 Severity, 11 February 2021. Available online: https://www.gov.uk/government/publications/nervtag-update-note-on-b117-severity-11-february-2021 (accessed on 23 October 2023).
- Relan, P.; Motaze, N.V.; Kothari, K.; Askie, L.; Le Polain, O.; Van Kerkhove, M.D.; Diaz, J.; Tirupakuzhi Vijayaraghavan, B.K. Severity and Outcomes of Omicron Variant of SARS-CoV-2 Compared to Delta Variant and Severity of Omicron Sublineages: A Systematic Review and Metanalysis. BMJ Glob. Health 2023, 8, e012328. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuan, D.; Chen, R.H.; Ng, D.G.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895.e20. [Google Scholar] [CrossRef]
- Cegolon, L.; Mastrangelo, G.; Emanuelli, E.; Camerotto, R.; Spinato, G.; Frezza, D. Early Negativization of SARS-CoV-2 Infection by Nasal Spray of Seawater plus Additives: The RENAISSANCE Open-Label Controlled Clinical Trial. Pharmaceutics 2022, 14, 2502. [Google Scholar] [CrossRef]
- Basso, P.; Negro, C.; Cegolon, L.; Larese Filon, F. Risk of Vaccine Breakthrough SARS-CoV-2 Infection and Associated Factors in Healthcare Workers of Trieste Teaching Hospitals (North-Eastern Italy). Viruses 2022, 14, 336. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef]
- Hyassat, D.; El-Khateebn, M.; Dahbour, A.; Shunnaq, S.; Naji, D.; Bani Ata, E.; Abujbara, M.; Khawaja, N.; Batieha, A.; Ajlouni, K. Post-COVID-19 syndrome among healthcare workers in Jordan. EMHJ 2023, 29, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Twitchell, D.K.; Christensen, M.B.; Hackett, G.; Morgentaler, A.; Saad, F.; Pastuszak, A.W. Examining Male Predominance of Severe COVID-19 Outcomes: A Systematic Review. Androg. Clin. Res. Ther. 2022, 3, 41–53. [Google Scholar] [CrossRef] [PubMed]


 = Asthenia;
= Asthenia;  = Myalgia;
= Myalgia;  = Dyspnoea;
= Dyspnoea;  = Cough;
= Cough;  = Insomnia;
= Insomnia;  = Headache;
= Headache;  = Concentration deficit;
= Concentration deficit;  = Anosmia;
= Anosmia;  = Dysgeusia;
= Dysgeusia;  = Anxiety.
= Asthenia; = Myalgia; = Dyspnoea; = Cough; = Insomnia; = Headache; = Concentration deficit; = Anosmia; = Dysgeusia; = Anxiety.
= Anxiety.
= Asthenia; = Myalgia; = Dyspnoea; = Cough; = Insomnia; = Headache; = Concentration deficit; = Anosmia; = Dysgeusia; = Anxiety.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Terms | Strata | Total (Tot = 5432) N (%) | Males (Tot = 1310) N (%) | Females (Tot = 4122) N (%) | p-Value | |
|---|---|---|---|---|---|---|
| Sex | Males | 1310 (24.1) | ||||
| Females | 4122 (75.9) | |||||
| Health center | Verona | 2996 (55.1) | 716 (54.7) | 2280 (55.3) | <0.001 | |
| Padua | 1206 (22.2) | 227 (17.3) | 979 (23.7) | |||
| Trieste | 983 (18.1) | 271 (20.7) | 712 (17.3) | |||
| Modena-Reggio Emilia | 247 (4.6) | 96 (7.3) | 151 (3.7) | |||
| Age (years) (M: 830) | Mean ± SD | 44.6 ± 12.0 | 43.2 ± 12.8 | 45.1 ± 11.7 | ||
| Median (IQR) | 47 (33; 55) | 42 (31; 55) | 48 (34; 55) | <0.001 | ||
| <40 | 1716 (37.3) | 511 (46.6) | 1205 (34.4) | <0.001 | ||
| 40–54 | 1655 (36.0) | 305 (27.8) | 1350 (38.5) | |||
| 55+ | 1231 (26.7) | 281 (25.6) | 950 (27.1) | |||
| Doses of COVID-19 vaccine (number) | 0 | 1020 (18.8) | 313 (23.9) | 707 (17.2) | <0.001 | |
| 1 | 208 (3.8) | 56 (4.3) | 152 (3.1) | |||
| 2 | 352 (6.5) | 65 (5.0) | 287 (7.0) | |||
| 3 | 3839 (70.7) | 872 (66.2) | 2967 (72.0) | |||
| 4 | 13 (0.2) | 4 (0.3) | 9 (0.2) | |||
| COVID-19 Infections (number) | 0 | 3.058 (56.3) | 783 (59.8) | 2275 (55.2) | 0.027 | |
| 1 | 2163 (39.8) | 479 (36.6) | 1657 (40.2) | |||
| 2 | 230 (4.2) | 46 (3.5) | 184 (4.5) | |||
| 3 | 8 (0.2) | 2 (0.1) | 6 (0.1) | |||
| Time between COVID-19 infections (days) | 1st–2nd (missing: 33) | M ± SD | 387.7 ± 225.4 | 442.4 ± 248.8 | 373.0 ± 217.1 | |
| M (IQR) | 411 (176; 540) | 462 (216; 665) | 400 (25; 75) | 0.042 | ||
| 2nd–3rd (missing: 3) | M ± SD | 312 ± 183.5 | 366 ± 251.7 | 276.3 ± 175.6 | ||
| M (IQR) | 284 (142.5; 496) | 366 | 284 | 0.563 | ||
| Marital status (M: 37) | Single | 1636 (31.0) | 473 (37.2) | 1163 (29.9) | <0.001 | |
| Married | 2466 (46.7) | 545 (42.9) | 1921 (47.9) | |||
| Cohabitant | 711 (13.5) | 197 (15.5) | 514 (12.8) | |||
| Divorced/separated/widow | 469 (8.8) | 57 (4.4) | 412 (10.4) | |||
| Country of birth (M: 26) | Italy | 5185 (96.0) | 1257 (96.7) | 3928 (95.8) | 0.361 | |
| Other EU country | 106 (2.0) | 21 (1.6) | 85 (2.1) | |||
| Extra-EU country | 109 (2.0) | 22 (1.7) | 87 (2.1) | |||
| Education (M: 153) | Junior secondary | 326 (6.2) | 37 (2.9) | 289 (7.2) | <0.001 | |
| Secondary | 1512 (28.6) | 273 (21.4) | 1239 (31.0) | |||
| University | 2242 (42.5) | 577 (45.2) | 1665 (41.6) | |||
| Postgraduate | 1199 (22.7) | 390 (30.5) | 809 (20.2) | |||
| Ethnicity (M: 603) | Caucasian | 4295 (88.9) | 1103 (91.9) | 3192 (88.0) | <0.001 | |
| African | 13 (0.3) | 4 (0.3) | 9 (0.3) | |||
| Asian | 9 (0.2) | 2 (0.2) | 7 (0.2) | |||
| Arab | 7 (0.1) | 4 (0.3) | 3 (0.1) | |||
| Latino | 414 (8.6) | 75 (6.3) | 339 (9.2) | |||
| Other | 91 (1.9) | 12 (1.0) | 79 (2.2) | |||
| BMI (M: 231) | <18 | 136 (2.6) | 6 (0.5) | 130 (3.3) | <0.001 | |
| 18–25 | 3391 (65.2) | 721 (56.9) | 2670 (67.9) | |||
| 26–30 | 1177 (22.6) | 419 (33.1) | 758 (19.3) | |||
| 31+ | 497 (9.6) | 121 (9.4) | 376 (9.5) | |||
| Smoking (M: 39) | Never smoker | 3404 (63.1) | 765 (58.9) | 2639 (64.5) | 0.001 | |
| Smoker | 975 (18.1) | 273 (21.0) | 702 (17.2) | |||
| Ex-smoker | 1014 (18.8) | 261 (20.1) | 753 (18.4) | |||
| Years of smoking (number) (M: 37) (restricted to current smokers) | Mean ± SD | 19.0 ± 11.6 | 17.3 ± 11.4 | 19.8 ± 11.6 | ||
| Median (IQR) | 20 (10; 30) | 15 (10; 25) | 20 (10; 30) | 0.002 | ||
| <6 | 135 (14.3) | 43 (16.0) | 92 (13.7) | 0.001 | ||
| 6–10 | 194 (20.7) | 60 (22.3) | 134 (19.9) | |||
| 11–20 | 267 (28.3) | 93 (34.6) | 174 (25.8) | |||
| 21+ | 346 (36.7) | 73 (27.1) | 273 (40.6) | |||
| Cigarettes smoked (daily number) (M: 235) (restricted to current smokers) | Mean ± SD | 8.1 ± 5.9 | 8.9 ± 7.8 | 7.8 ± 5.0 | ||
| Median (IQR) | 7 (4; 10) | 8.5 (4; 12) | 7 (4; 10) | 0.135 | ||
| <5 | 196 (26.4) | 54 (26.7) | 142 (26.3) | 0.022 | ||
| 5–10 | 405 (54.5) | 97 (48.0) | 308 (56.9) | |||
| 11+ | 142 (19.1) | 51 (15.3) | 91 (16.8) | |||
| Years since smoking cessation (number) (M: 72) (restricted to ex-smokers) | Mean ± SD | 12.7 ± 10.3 | 11.9 ± 10.7 | 13.0 ± 10.1 | ||
| Median (IQR) | 10 (4; 21) | 8 (3; 17) | 11 (4; 21) | 0.062 | ||
| <5 | 273 (28.3) | 76 (30.8) | 197 (27.5) | 0.010 | ||
| 5–10 | 211 (21.9) | 68 (27.5) | 143 (19.8) | |||
| 11–20 | 237 (24.6) | 45 (18.2) | 192 (26.9) | |||
| 21+ | 243 (25.2) | 58 (23.5) | 185 (25.8) | |||
| Any pre-existing comorbidities | No | 3922 (74.2) | 982 (76.5) | 2940 (73.4) | 0.030 | |
| Yes | 1366 (25.8) | 302 (23.5) | 1064 (26.6) | |||
| Immune-depression | No | 5309 (97.7) | 1282 (97.1) | 4027 (97.7) | 0.723 | |
| Yes | 123 (2.3) | 28 (2.9) | 95 (2.3) | |||
| Job task (M:25) | Medical consultant | 681 (12.6) | 302 (23.4) | 279 (7.0) | <0.001 | |
| Medical trainee | 536 (9.9) | 194 (15.1) | 342 (8.6) | |||
| Nurse | 1889 (35.1) | 261 (20.3) | 1628 (40.8) | |||
| Laboratorist | 158 (2.9) | 20 (1.6) | 138 (3.4) | |||
| Nurse aid | 527 (9.8) | 74 (5.7) | 453 (11.3) | |||
| Administrative clerk | 519 (9.8) | 127 (9.9) | 392 (9.8) | |||
| Health technician | 263 (4.9) | 73 (5.7) | 190 (4.8) | |||
| Midwife | 44 (0.8) | 0 | 44 (1.1) | |||
| Pharmacist | 34 (0.6) | 11 (0.9) | 23 (0.6) | |||
| Psychologist | 53 (0.9) | 5 (0.4) | 48 (1.2) | |||
| Physio-therapist | 104 (1.9) | 24 (1.9) | 80 (2.0) | |||
| Undergraduate student | 228 (4.2) | 78 (6.1) | 150 (3.7) | |||
| Other | 343 (6.4) | 120 (9.3) | 223 (5.6) | |||
| Job seniority (years) (M: 613) | <6 | 1525 (28.1) | 487 (42.6) | 1038 (28.2) | <0.001 | |
| 7–17 | 1648 (30.4) | 265 (23.2) | 783 (21.3) | |||
| 18–29 | 1169 (21.6) | 224 (19.6) | 945 (25.7) | |||
| 30+ | 1077 (19.9) | 167 (14.6) | 910 (24.8) | |||
| Employed in COVID-19 unit now | No | 4774 (90.3) | 1150 (90.8) | 3624 (90.2) | 0.564 | |
| Yes | 510 (9.7) | 117 (9.2) | 393 (9.8) | |||
| Actual workplace (M: 182) | Infectious diseases | 79 (1.5) | 16 (1.3) | 63 (1.6) | 0.008 | |
| Pneumology | 63 (1.2) | 22 (1.7) | 41 (1.0) | |||
| ICU | 383 (7.3) | 87 (6.9) | 296 (7.4) | |||
| Internal medicine | 384 (7.2) | 76 (6.1) | 308 (7.7) | |||
| Surgical ward | 592 (11.3) | 135 (10.8) | 457 (11.4) | |||
| Radiology | 147 (2.8) | 48 (3.8) | 99 (2.5) | |||
| Administrative services | 338 (6.4) | 96 (7.7) | 242 (6.1) | |||
| Other | 3264 (62.3) | 775 (61.7) | 2489 (62.3) | |||
| Workplace during 2020–2022 (M: 160) | Administrative | 679 (12.9) | 190 (15.2) | 489 (12.2) | <0.001 | |
| Outpatient | 519 (9.8) | 90 (7.2) | 429 (10.7) | |||
| COVID-19 unit | 46 (0.9) | 10 (0.8) | 36 (0.9) | |||
| Non-COVID-19 unit | 918 (17.4) | 168 (13.4) | 750 (18.7) | |||
| COVID-19 unit (low risk) | 432 (8.2) | 87 (6.9) | 345 (8.0) | |||
| COVID-19 unit (high risk) | 425 (8.1) | 97 (7.7) | 328 (8.2) | |||
| Operating theatre | 474 (9.0) | 185 (14.8) | 289 (7.2) | |||
| Other | 1779 (33.8) | 426 (34.0) | 1353 (33.7) | |||
| Terms | Strata | COVID-19 Infections | |||
|---|---|---|---|---|---|
| Only One (N = 2163) | Only Two (N = 230) | Three (N = 8) | |||
| Center | Verona | 1063 (49.1) | 122 (53.0) | 3 (37.5) | |
| Padua | 594 (27.5) | 45 (19.6) | 2 (25.0) | ||
| Trieste | 381 (17.6) | 50 (21.7) | 1 (12.5) | ||
| Modena-Reggio Emilia | 125 (5.8) | 13 (5.7) | 2 (25.0) | ||
| Doses of COVID-19 vaccine before infection | 0 | 246 (11.4) | 52 (22.6) | 1 (12.5) | |
| 1 | 88 (4.1) | 17 (7.4) | 0 | ||
| 2 | 205 (9.5) | 43 (18.7) | 4 (50.0) | ||
| 3 | 1623 (75.0) | 118 (51.3) | 3 (37.5) | ||
| 4 | 1 (0.1) | 0 | 0 | ||
| COVID-19 wave | 1 March 2020–31 October 2020 | 153 (7.2) | 0 | 0 | |
| 1 November 2020–31 May 2021 | 291 (13.6) | 14 (6.0) | 0 | ||
| 1 June 2021–30 November 2021 | 69 (3.1) | 6 (2.6) | 0 | ||
| 1 December 2021–25 August 2022 | 1622 (76.0) | 215 (91.9) | 8 (14.3) | ||
| Time between last dose of COVID-19 vaccine and SARS-CoV-2 infection (days) | Any dose | M ± SD | 136.3 ± 85.6 | 152.6 ± 111.6 | 143.86 ± 87.0 |
| M (IQR) | 122 (74; 178) | 127 (75; 205) | 121 (65; 227) | ||
| 1st dose | M ± SD | 344.2 ± 130.3 | 351.9 ± 125.1 | NA | |
| M (IQR) | 381 (245; 451) | 366 (276; 451) | NA | ||
| 2nd dose | M ± SD | 244.5 ± 119.9 | 167 ± 122.9 | 172 ± 71.7 | |
| M (IQR) | 254 (150; 344) | 139.5 (62.5; 244.5) | 170.5 (106; 239.5) | ||
| 3rd dose | M ± SD | 121.1 ± 61.3 | 117.7 ± 60.5 | 106.3 ± 106.2 | |
| M (IQR) | 118 (70; 167) | 106 (73; 153) | 65 (27; 227) | ||
| 4th dose | M ± SD | NA | NA | NA | |
| M (IQR) | NA | NA | NA | ||
| Viral shedding time (days) | Mean ± SD | 13.5 ± 8.0 | 10.0 ± 4.5 | 9.3 ± 5.7 | |
| Median (IQR) | 11 (9; 15) | 8.5 (7; 12) | 7 (7; 10.5) | ||
| 0–7 | 431 (21.2) | 91 (42.05) | 5 (83.3) | ||
| 8–10 | 560 (27.5) | 64 (29.9) | 0 | ||
| 11–14 | 402 (19.8) | 23 (10.8) | 0 | ||
| 15+ | 642 (31.6) | 36 (16.8) | 1 (16.7) | ||
| Hospitalization | No | 2146 (99.2) | 229 (99.6) | 8 (100) | |
| Yes | 17 (0.8) | 1 (0.4) | 0 | ||
| Length of stay (days) | Mean ± SD | 6.9 ± 5.1 | 1 | NA | |
| Median (IQR) | 6.5 (2; 10) | 1 | NA | ||
| <6 | 7 (43.8) | 1 | NA | ||
| 6–10 | 6 (37.5) | 0 | NA | ||
| 11–15 | 3 (18.8) | 0 | NA | ||
| 16+ | 0 | 0 | NA | ||
| Term | Strata | Wuhan | Alpha | Delta | Omicron |
|---|---|---|---|---|---|
| Admission after 1st COVID-19 infection | No | 207 (95.4) | 387 (99.5) | 79 (98.5) | 1638 (99.6) |
| Yes | 10 (4.6) | 2 (0.5) | 2 (2.5) | 6 (0.4) |
| Post-COVID-19 Symptoms | Number | (%) | |
|---|---|---|---|
| Single symptoms | Asthenia | 126 | 14.2 |
| Cough | 79 | 8.9 | |
| Myalgia | 27 | 3.0 | |
| Dyspnea | 18 | 2.0 | |
| Anosmia | 16 | 1.8 | |
| Concentration deficit | 13 | 1.5 | |
| Headache | 12 | 1.4 | |
| Dysgeusia | 9 | 1.0 | |
| 2 symptoms combined | Asthenia, myalgia | 53 | 6.0 |
| Asthenia, cough | 42 | 4.7 | |
| Asthenia, dyspnea | 34 | 3.8 | |
| Anosmia, ageusia | 26 | 2.9 | |
| Asthenia, headache | 23 | 2.6 | |
| Asthenia, concentration deficit | 21 | 2.4 | |
| 3 symptoms combined | Asthenia, myalgia, dyspnea | 14 | 1.6 |
| Asthenia, myalgia, cough | 11 | 1.2 | |
| Asthenia, anosmia, dysgeusia | 10 | 1.1 | |
| Asthenia, myalgia, concentration deficit | 10 | 1.1 | |
| Asthenia, myalgia, headache | 10 | 1.1 | |
| Total symptom count | Asthenia | 596 | 30.3 |
| Myalgia | 270 | 13.7 | |
| Cough | 244 | 12.4 | |
| Dyspnea | 200 | 10.2 | |
| Concentration deficit | 160 | 8.1 | |
| Headache | 143 | 7.3 | |
| Anosmia | 128 | 6.5 | |
| Dysgeusia | 113 | 5.7 | |
| Insomnia | 102 | 5.2 | |
| Anxiety | 84 | 4.3 | |
| Symptoms | Asthenia | Myalgia | Cough | Dyspnea | Concentration Deficit | Headache | Anosmia | Dysgeusia | Insomnia | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1st COVID-19 infection | Asthenia | 1 | 0.412 ** | 0.182 ** | 0.328 ** | 0.321 ** | 0.238 ** | 0.098 ** | 0.121 ** | 0.241 ** |
| Myalgia | 1 | 0.073 ** | 0.247 ** | 0.215 ** | 0.225 ** | 0.060 * | 0.091 ** | 0.190 ** | ||
| Cough | 1 | 0.123 ** | 0.060 * | 0.093 ** | 0.069 * | 0.022 | 0.059 * | |||
| Dyspnea | 1 | 0.162 ** | 0.165 ** | 0.065 * | 0.149 ** | 0.147 ** | ||||
| Concentration deficit | 1 | 0.185 ** | 0.060 * | 0.035 | 0.276 ** | |||||
| Headache | 1 | 0.058 * | 0.084 ** | 0.225 ** | ||||||
| Anosmia | 1 | 0.045 * | ||||||||
| Dysgeusia | 1 | 0.072 ** | ||||||||
| Insomnia | 1 | |||||||||
| 2nd COVID-19 infection | Asthenia | 1 | - | 0.247 ** | 0.034 | 0.107 | 0.187 * | 0.003 | 0.268 ** | 0.125 |
| Myalgia | 1 | - | - | - | - | - | - | - | ||
| Cough | 1 | −0.027 | −0.008 | −0.015 | −0.017 | −0.015 | −0.013 | |||
| Dyspnea | 1 | 0.143 | 0.151 | 0.204 * | −0.047 | −0.043 | ||||
| Concentration deficit | 1 | −0.015 | 0.238 ** | −0.015 | −0.013 | |||||
| Headache | 1 | 0.119 | −0.026 | 0.164 * | ||||||
| Anosmia | 1 | −0.030 | 0.164 * | |||||||
| Dysgeusia | 1 | 0.027 | ||||||||
| Insomnia | 1 | |||||||||
| Strata | Symptoms during Acute COVID-19 | Overall Post-COVID-19 Symptoms | Persisting Symptoms * | Novel Symptoms ** | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | At 30–60 days | At 61+ days | ||||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| General | 1526/1969 | 77.5 | 692/1969 | 35.1 | 344/692 | 49.7 | 226/691 | 32.7 | 639/1526 | 41.9 | 79/443 | 17.8 |
| ENT | 1393/1969 | 70.8 | 319/1969 | 16.2 | 148/319 | 46.4 | 98/317 | 30.9 | 282/1393 | 20.2 | 51/576 | 8.9 |
| Pulmonary | 1067/1969 | 54.2 | 413/1969 | 21.0 | 187/413 | 45.3 | 109/413 | 26.4 | 377/1067 | 35.3 | 44/902 | 4.9 |
| Gastro-enteric | 486/1969 | 24.7 | 58/1969 | 2.4 | 28/58 | 48.3 | 17/58 | 29.3 | 51/486 | 10.5 | 12/1483 | 0.8 |
| Psychological | 325/1969 | 16.5 | 167/1969 | 8.4 | 115/167 | 68.9 | 76/167 | 45.5 | 127/325 | 39.1 | 47/1644 | 2.9 |
| Neurological | 326/1969 | 16.6 | 210/1969 | 10.7 | 142/210 | 67.6 | 99/209 | 47.4 | 150/326 | 46.0 | 80/1643 | 4.9 |
| Term | Strata | 1st COVID-19 Infection (N = 2401) N (%) | Long COVID-19 after Primary Infection | |||||
|---|---|---|---|---|---|---|---|---|
| 30–60 Days Since First Negative Swab | 61+ Days Since First Negative Swab | |||||||
| No (N = 1825) N (%) | Yes (N = 576) N (%) | OR (95%CI) | No (N = 2005) N (%) | Yes (N = 389) N (%) | OR (95%CI) | |||
| Center | Verona | 1188 (49.5) | 904 (76.1) | 284 (23.9) | reference | 993 (83.8) | 192 (16.2) | reference |
| Padua | 641 (26.7) | 483 (75.4) | 158 (24.6) | 1.04 (0.83; 1.30) | 542 (84.6) | 99 (15.4) | 0.94 (0.73; 1.23) | |
| Trieste | 431 (18.0) | 311 (72.0) | 121 (28.0) | 1.24 (0.97; 1.59) | 337 (78.7) | 91 (21.3) | 1.39 (1.06; 1.84) | |
| Modena-Reggio Emilia | 140 (5.8) | 127 (90.7) | 13 (9.3) | 0.33 (0.18: 0.59) | 133 (95.0) | 7 (5.0) | 0.27 (0.13; 0.59) | |
| COVID-19 wave | 1 March 2020–31 October 2020 | 291 (9.3) | 115 (52.5) | 104 (47.5) | 4.77 (3.00; 7.71) | 94 (63.1) | 55 (36.9) | 6.31 (4.09; 9.75) |
| 1 November 2020–31 May 2021 | 393 (16.7) | 229 (58.3) | 164 (41.7) | 3.78 (2.88; 5.00) | 266 (64.9) | 144 (35.1) | 4.43 (3.30; 5.94) | |
| 1 June 2021–30 November 2021 | 82 (3.5) | 59 (72.0) | 23 (15.9) | 2.06 (1.05; 4.04) | 110 (81.6) | 25 (18.5) | 2.60 (1.17; 5.80) | |
| 1 December 2021–25 August 2022 | 1665 (70.6) | 1400 (84.1) | 265 (16.0) | reference | 1513 (90.9) | 152 (9.2) | reference | |
| SARS-CoV-2 p4ositivity (days) | 0–7 | 444 (19.6) | 397 (89.4) | 47 (10.6) | reference | 419 (94.4) | 25 (5.6) | reference |
| 8–10 | 604 (26.7) | 502 (83.1) | 102 (16.9) | 1.72 (1.17; 2.52) | 543 (90.4) | 58 (9.7) | 1.79 (0.91; 3.54) | |
| 11–14 | 431 (19.1) | 343 (79.6) | 88 (20.4) | 2.17 (1.49; 3.16) | 381 (88.6) | 49 (11.4) | 2.16 (0.99; 4.68) | |
| 15+ | 783 (35.6) | 469 (59.9) | 314 (40.1) | 5.66 (5.21; 6.14) | 542 (69.5) | 238 (30.5) | 7.36 (5.36; 10.12) | |
| Hospitalization | No | 2380 (99.1) | 1816 (76.3) | 564 (23.7) | reference | 1995 (84.0) | 379 (16.1) | reference |
| Yes | 21 (0.9) | 9 (42.9) | 12 (57.1) | 4.28 (1.48; 12.39) | 10 (50.0) | 10 (50.0) | 5.25 (2.50; 11.00) | |
| Vaccination status (number of doses before 1st infection) | 0 | 827 (34.7) | 504 (60.9) | 323 (39.1) | reference | 583 (70.5) | 244 (29.5) | reference |
| 1 | 90 (3.8) | 76 (84.4) | 14 (15.6) | 0.29 (0.17; 0.50) | 81 (90.0) | 9 (10.0) | 0.27 (0.15; 0.48) | |
| 2 | 206 (8.6) | 166 (80.6) | 40 (19.4) | 0.38 (0.29; 0.49) | 179 (86.9) | 27 (13.1) | 0.36 (0.25; 0.53) | |
| 3 | 1263 (52.9) | 1069 (84.6) | 194 (15.4) | 0.28 (0.20; 0.40) | 1156 (91.5) | 107 (8.5) | 0.22 (0.15; 0.33) | |
| 4 | 0 | NA | NA | NA | 0 | 1 | NA | |
| Sex | Male | 535 (22.1) | 453 (84.7) | 82 (15.3) | reference | 488 (91.2) | 47 (8.8) | reference |
| Female | 1866 (77.7) | 1372 (73.5) | 484 (26.5) | 1.99 (1.67; 2.36) | 1517 (81.6) | 342 (18.4) | 2.34 (1.75; 3.14) | |
| Age (years) | Mean ± SD | 44.7 ± 12.0 | 42.6 ± 11.7 | 46.7 ± 10.4 | NA | 42.6 ± 11.7 | 46.7 ± 10.4 | NA |
| Median (IQR) | 47 (33; 55) | 43 (31; 53) | 49 (39; 55) | p < 0.001 | 43 (31; 53) | 49 (39; 55) | p < 0.001 | |
| <40 | 860 (41.0) | 728 (84.7) | 132 (15.4) | reference | 771 (89.8) | 88 (10.2) | reference | |
| 40–54 | 798 (38.0) | 562 (70.4) | 236 (29.6) | 2.32 (1.72; 3.12) | 634 (79.5) | 164 (20.6) | 2.27 (1.74; 2.96) | |
| 55+ | 441 (21.0) | 311 (70.5) | 130 (29.5) | 2.30 (1.95; 2.73) | 352 (80.2) | 87 (19.8) | 2.17 (1.74; 2.69) | |
| Country of birth | Italy | 2300 (96.2) | 1756 (76.4) | 544 (23.7) | reference | 1926 (84.0) | 367 (16.0) | reference |
| EU | 45 (1.9) | 34 (75.6) | 11 (24.4) | 1.04 (0.31; 3.47) | 35 (77.8) | 10 (22.2) | 1.50 (0.49; 4.57) | |
| Extra-EU | 46 (1.9) | 28 (60.9) | 18 (39.1) | 2.08 (1.13; 3.81) | 36 (78.3) | 10 (21.7) | 1.46 (1.16; 1.84) | |
| Ethnicity | Caucasian | 1912 (89.1) | 1492 (78.0) | 420 (22.0) | reference | 1631 (85.3) | 276 (14.5) | reference |
| Other | 235 (11.0) | 166 (70.6) | 69 (29.4) | 1.43 (1.24; 1.65) | 179 (76.5) | 55 (23.5) | 1.82 (1.60; 2.06) | |
| Educational level | Junior secondary | 143 (6.1) | 88 (61.5) | 55 (38.5) | reference | 105 (73.9) | 37 (25.5) | reference |
| Secondary | 612 (26.1) | 441 (72.1) | 171 (27.9) | 0.63 (0.46; 0.87) | 485 (79.5) | 125 (20.5) | 0.73 (0.66; 0.81) | |
| University | 1083 (46.2) | 860 (79.4) | 223 (20.6) | 0.41 (0.32 0.59) | 935 (86.6) | 145 (13.7) | 0.44 (0.33; 0.59) | |
| Postgraduate | 505 (21.6) | 397 (78.6) | 108 (21.4) | 0.48 (0.42; 0.52) | 438 (86.9) | 66 (13.4) | 0.43 (0.40; 0.46) | |
| Marital Status | Single | 689 (29.1) | 557 (80.8) | 132 (19.2) | reference | 605 (87.7) | 86 (12.1) | reference |
| Married | 1096 (46.2) | 805 (73.5) | 291 26.6) | 1.54 (1.12; 2.12) | 898 (81.6) | 202 (18.4) | 1.60 (0.91; 2.80) | |
| Cohabitant | 363 (15.3) | 299 (82.4) | 64 (17.6) | 0.89 (0.69; 1.13) | 318 (87.6) | 45 (12.4) | 1.01 (0.77; 1.32) | |
| Divorced/separated/widow | 191 (8.1) | 120 (62.8) | 71 (37.2) | 2.49 (2.09; 2.97) | 147 (76.2) | 46 (23.8) | 2.23 (1.74; 2.85) | |
| BMI (kg/m2) | <18 | 53 (2.3) | 38 (67.9) | 18 (32.1) | 1.72 (0.80; 3.67) | 47 (83.9) | 9 (17.0) | 1.18 (0.45; 3.12) |
| 18–25 | 1523 (65.8) | 1251 (78.4) | 345 (21.6) | reference | 1370 (86.1) | 222 (13.9) | reference | |
| 26–30 | 521 (22.5) | 393 (71.7) | 155 (28.3) | 1.43 (1.10; 1.90) | 435 (79.7) | 111 (20.3) | 1.57 (1.27; 1.96) | |
| 31+ | 218 (9.4) | 142 (63.4) | 82 (36.6) | 2.09 (1.24; 3.52) | 167 (74.6) | 57 (25.5) | 2.11 (1.22; 3.64) | |
| Any pre-existing conditions | No | 2034 (38.4) | 767 (73.5) | 276 (26.5) | reference | 857 (82.5) | 182 817.5) | reference |
| Yes | 3263 (61.6) | 1075 (76.3) | 334 (23.7) | 0.86 (0.65; 1.15) | 1182 (84.1) | 224 (15.9) | 0.89 (0.64; 1.25) | |
| Under psychological therapy | No | 2313 (97.8) | 1761 (76.1) | 552 (23.9) | reference | 1934 (83.9) | 372 (16.1) | reference |
| Yes | 51 (2.2) | 35 (68.6) | 16 (31.4) | 1.46 (0.94; 2.27) | 38 (74.5) | 13 (25.5) | 1.78 (0.89; 3.57) | |
| Smoking status | Never smoked | 1509 (63.3) | 1170 (77.5) | 339 (22.5) | reference | 1278 (84.9) | 227 (15.1) | reference |
| Smoker | 402 (16.9) | 301 (74.9) | 101 (25.1) | 1.16 (0.85; 1.58) | 337 (84.0) | 64 (16.0) | 1.07 (0.81; 1.41) | |
| Ex- smoker | 473 (19.8) | 342 (72.3) | 131 (27.7) | 1.32 (1.16; 1.50) | 378 (80.2) | 93 (19.8) | 1.39 (1.17; 1.64) | |
| Years of smoking (Number) | Mean ± SD | 17.1 ± 11.0 | 16.2 ± 11.2 | 19.3 ± 10.3 | NA | 16.5 ± 11.0 | 20.0 ± 10.5 | NA |
| Median (IQR) | 15 (8; 25) | 15 (8; 25) | 20 (10; 28) | 0.008 | 15 (8; 25) | 20 (10; 30) | 0.016 | |
| <6 | 70 (18.0) | 60 (85.7) | 10 (14.3) | reference | 64 (92.8) | 5 (7.2) | reference | |
| 6–10 | 88 (22.7) | 69 (78.4) | 19 (21.6) | 1.65 (1.10; 2.48) | 75 (85.2) | 13 (14.8) | 2.22 (1.08; 4.54) | |
| 11–20 | 114 (29.4) | 83 (72.8) | 31 (27.2) | 2.24 (1.51; 3.34) | 93 (81.6) | 21 (18.4) | 2.89 (1.55; 5.40) | |
| 21+ | 116 (29.9) | 81 (69.8) | 35 (30.2) | 2.59 (1.94; 3.46) | 94 (81.0) | 22 (19.0) | 3.00 (1.46; 6.14) | |
| Cigarettes smoked (daily number) | Mean ± SD | 7.2 ± 4.8 | 7.1 ± 4.9 | 7.4 ± 4.6 | NA | 7.2 ± 4.8 | 7.2 ± 4.6 | NA |
| Median (IQR) | 6 (3; 10) | 6 (3; 10) | 6 (3; 10) | 0.914 | 6 (3; 10) | 6 (3; 10) | 0.480 | |
| <5 | 97 (32.1) | 79 (81.4) | 18 (18.6) | reference | 85 (87.6) | 12 (12.5) | reference | |
| 5–10 | 161 (53.3) | 121 (75.2) | 40 (24.8) | 1.45 (1.02; 2.06) | 137 (85.1) | 24 (15.0) | 1.24 (0.81; 1.91) | |
| 11+ | 44 (14.6) | 35 (79.6) | 9 (20.5) | 1.13 (0.54; 2.36) | 39 (88.6) | 5 (11.6) | 0.91 (0.19; 4.41) | |
| Years since smoking cessation (Number) | Mean ± SD | 11.5 ± 9.4 | 11.3 ± 9.3 | 13.3 ± 9.6 | NA | 11.0 ± 9.4 | 13.3 ± 9.4 | NA |
| Median (IQR) | 9.5 (3; 19) | 9 (3; 18) | 12 (4.5; 22) | 0.031 | 8 (3; 18) | 11.5 (5.5; 21.5) | 0.026 | |
| <5 | 145 (31.5) | 112 (77.2) | 33 (22.8) | reference | 125 (86.2) | 20 (13.8) | reference | |
| 5–10 | 103 (22.4) | 80 (77.7) | 23 (22.3) | 0.98 (0.54; 1.75) | 86 (84.3) | 16 (15.7) | 1.16 (0.49; 2.77) | |
| 11–20 | 120 (26.1) | 85 (70.8) | 35 (29.2) | 1.40 (1.04;1.87) | 94 (78.3) | 26 (21.7) | 1.73 (0.90; 3.31) | |
| 21+ | 92 (20.0) | 60 (65.2) | 32 (34.8) | 1.81 (1.27; 2.58) | 69 (75.8) | 22 (24.2) | 1.99 (0.84; 4.73) | |
| Current workplace | Infectious diseases | 45 (1.9) | 35 (77.8) | 10 (22.2) | 0.55 (0.40; 0.75) | 37 (84.1) | 7 /15.9) | 0.66 (0.51; 0.86) |
| Pneumology | 36 (1.5) | 32 (88.9) | 4 (11.1) | 0.24 (0.06; 0.95) | 32 (91.4) | 3 (8.6) | 0.33 (0.06; 1.70) | |
| ICU | 183 (7.8) | 139 (76.0) | 44 (24.0) | 0.61 (0.41; 0.91) | 147 (80.3) | 36 (19.7) | 0.86 (0.48; 1.52) | |
| Internal medicine | 199 (8.5) | 153 (76.9) | 46 (23.1) | 0.58 (0.33; 1.03) | 167 (83.9) | 32 (16.1) | 0.67 (0.48; 0.93) | |
| Surgical ward | 293 (12.5) | 218 (74.4) | 75 (25.6) | 0.66 (0.49; 0.89) | 250 (85.3) | 43 (14.7) | 0.60 (0.37; 0.97) | |
| Radiology | 54 (2.3) | 40 (74.1) | 14 (25.9) | 0.67 (0.36; 1.27) | 44 (81.5) | 10 (18.5) | 0.80 (0.47; 1.33) | |
| Administrative services | 117 (5.0) | 77 (65.8) | 40 (34.2) | Reference | 91 (77.8) | 26 (22.2) | reference | |
| Other | 1415 (60.4) | 1080 (76.3) | 335 (23.7) | 0.60 (0.49; 0.72) | 1185 (84.0) | 225 (16.0) | 0.66 (0.50; 0.88) | |
| Employed in COVID-19 unit now | No | 2056 (88.4) | 1575 (76.6) | 481 (23.4) | reference | 1731 (84.2) | 325 (15.8) | reference |
| Yes | 269 (11.6) | 191 (71.0) | 78 (29.0) | 1.34 (1.00; 1.79) | 216 (80.3) | 53 (19.7) | 1.31 (1.17; 1.46) | |
| Job task | Medical consultant | 282 (11.8) | 224 (79.4) | 58 (20.6) | 0.57 (0.30; 1.08) | 249 (88.3) | 33 (11.7) | 0.44 (0.31; 0.61) |
| Medical trainee | 276 (11.6) | 253 (91.7) | 23 (8.3) | 0.20 (0.15; 0.26) | 261 (94.9) | 14 (5.1) | 0.18 (0.13; 0.24) | |
| Nurse | 923 (38.8) | 655 (71.0) | 268 (29.0) | 0.90 (0.67; 1.21) | 735 (79.8) | 186 (20.2) | 0.83 (0.63; 1.10) | |
| Laboratorist | 71 (3.0) | 60 (84.5) | 11 (15.5) | 0.40 (0.19; 0.87) | 65 (91.6) | 6 (8.5) | 0.30 (0.12; 0.80) | |
| Nurse aid | 245 (10.3) | 160 (65.3) | 85 (34.7) | 1.17 (0.73; 1.86) | 187 (76.3) | 58 (23.7) | 1.02 (0.56; 1.87) | |
| Administrative clerk | 182 (7.6) | 125 (68.7) | 57 (31.3) | reference | 138 (76.7) | 42 (23.3) | reference | |
| Health technician | 107 (4.5) | 88 (82.2) | 19 (17.8) | 0.47 (0.32; 0.69) | 94 (87.9) | 13 (12.2) | 0.45 (0.23; 0.88) | |
| Midwife | 24 (1.0) | 20 (83.3) | 4 (16.7) | 0.44 (0.18; 1.06) | 21 (87.5) | 3 (12.5) | 0.47 (0.21; 1.05) | |
| Pharmacist | 15 (0.6) | 13 (86.7) | 2 (13.3) | 0.34 (0.07; 1.73) | 14 (93.3) | 1 (6.7) | 0.23 (0.05; 1.19) | |
| Psychologist | 28 (1.2) | 23 (82.1) | 5 (17.9) | 0.48 (0.33; 0.69) | 24 (85.7) | 4 (14.3) | 0.55 (0.20; 1.47) | |
| Physio-therapist | 47 (2.0) | 39 (83.0) | 8 (17.0) | 0.45 (0.24; 0.85) | 41 (91.1) | 4 (8.9) | 0.32 (0.13; 0.79) | |
| Undergraduate student | 62 (2.6) | 58 (93.6) | 4 (6.5) | 0.15 (0.12; 0.18) | 58 (93.6) | 4 (6.5) | 0.23 (0.19; 0.26) | |
| Other | 120 (5.0) | 94 (78.3) | 25 (21.7) | 0.61 (0.44; 0.83) | 100 (83.3) | 20 (16.5) | 0.66 (0.42; 1.02) | |
| Job seniority (years) | <6 | 749 (34.6) | 631 (84.3) | 118 (15.8) | reference | 674 (90.1) | 74 (9.9) | reference |
| 7–17 | 484 (22.4) | 354 (73.1) | 130 (26.9) | 1.96 (1.48; 2.61) | 399 (82.4) | 85 (17.6) | 1.94 (1.41; 2.68) | |
| 18–29 | 530 (24.5) | 365 (68.9) | 165 (31.1) | 2.42 (1.95; 2.99) | 415 (78.6) | 113 (21.4) | 2.48 (1.68; 3.67) | |
| 30+ | 401 (18.5) | 287 (71.6) | 114 (28.4) | 2.12 (1.66; 2.72) | 313 (78.8) | 84 (21.2) | 2.44 (1.59; 3.76) | |
| Workplace during 2020–2022 | Administrative | 236 (10.1) | 168 (71.2) | 68 (28.8) | reference | 193 (81.8) | 43 (18.2) | reference |
| Outpatient | 226 (9.6) | 173 (76.6) | 53 (23.5) | 0.76 (0.52; 1.10) | 187 (83.5) | 37 (16.5) | 0.89 (0.62; 1.26) | |
| COVID-19 unit | 19 (0.8) | 13 (68.4) | 6 (31.6) | 1.14 (0.48; 2.73) | 14 (73.7) | 5 (26.3) | 1.60 (0.54; 4.76) | |
| Non-COVID-19 unit | 462 (19.7) | 354 (76.6) | 108 (23.4) | 0.75 (0.51; 1.12) | 391 (84.6) | 71 (15.4) | 0.82 (0.55; 1.20) | |
| COVID-19 unit (low risk) | 231 (9.8) | 168 (72.7) | 63 (27.3) | 0.93 (0.58; 1.48) | 192 (83.5) | 38 (16.5) | 0.89 (0.72; 1.09) | |
| COVID-19 unit (high risk) | 206 (8.8) | 160 (77.7) | 46 (22.3) | 0.71 (0.36; 1.41) | 166 (80.6) | 40 (19.4) | 1.08 (0.59; 1.97) | |
| Operating theatre | 209 (8.9) | 173 (82.8) | 36 (17.2) | 0.51 (0.35; 0.76) | 191 (91.8) | 17 (8.2) | 0.40 (0.24; 0.65) | |
| Other | 758 (32.3) | 572 (75.5) | 183 (24.5) | 0.80 (0.59; 1.09) | 625 (82.8) | 130 (17.0) | 0.93 (0.68; 1.27) | |
| Term | Strata | Long COVID-19 after Primary Infecion (aOR; 95%CI) | |
|---|---|---|---|
| 30–60 Days Since 1st Negative Swab (1602 Obs.) | 61+ Days Since 1st Negative Swab (1611 Obs.) | ||
| Sex | Male | reference | reference |
| Female | 1.91 (1.30; 2.80) | 2.14 (1.69; 2.71) | |
| Age (years) | <40 | reference | Reference |
| 40–54 | 1.73 (1.25; 2.39) | 1.69 (1.47; 1.93) | |
| 55+ | 1.60 (1.45; 1.76) | 1.60 (1.24; 2.06) | |
| COVID-19 wave | 1 March 2020–31 October 2020 | 2.16 (1.14; 4.09) | 2.25 (1.00; 5.09) |
| 1 November 2020–31 May 2021 | 2.05 (1.25; 3.38) | 1.91 (0.86; 4.21) | |
| 1 June 2021–30 November 2021 | 1.68 (0.72; 3.93) | 2.18 (0.71; 6.68) | |
| 1 December 2021–25 August 2022 | reference | reference | |
| Viral shedding time (days) | 0–7 | reference | reference |
| 8–10 | 1.68 (1.11; 2.53) | 2.03 (1.02; 4.04) | |
| 11–14 | 1.92 (1.49; 2.48) | 1.97 (1.46; 2.67) | |
| 15+ | 3.20 (2.07; 4.94) | 5.00 (2.84; 8.81) | |
| COVID-19 hospitalization | No | reference | reference |
| Yes | 3.34 (1.62; 6.89) | 4.09 (2.25; 7.44) | |
| COVID-19 vaccination status before infection (number of doses) | 0 | reference | reference |
| 1 | 0.83 (0.54; 1.27) | 0.60 (0.36; 1.36) | |
| 2 | 0.57 (0.34; 0.94) | 0.60 (0.36; 0.99) | |
| 3 | 0.77 (0.51; 1.17) | 0.71 (0.44; 1.14) | |
| Ethnicity | Caucasian | reference | reference |
| Other | 1.21 (0.97; 1.51) | 1.83 (1.41; 2.36) | |
| Educational level | Junior secondary | reference | |
| Secondary | 0.73 (0.23; 2.24) | ||
| University | 0.67 (0.24; 1.89) | ||
| Postgraduate | 0.56 (0.19; 1.71) | ||
| Marital status | Single | reference | |
| Married | 0.91 (0.67; 1.22) | ||
| Cohabitant | 0.70 (0.47; 1.05) | ||
| Divorced/separated/widow | 1.22 (1.15; 1.30) | ||
| BMI (Kg/m2) | <18 | 2.52 (1.29; 4.92) | 1.40 (0.33; 5.93) |
| 18–25 | reference | reference | |
| 26–30 | 1.43 (1.18; 1.73) | 1.72 (1.29; 2.29) | |
| 31+ | 1.68 (1.48; 1.91) | 1.56 (1.26; 1.92) | |
| Job task (M: 41) | Medical consultant | 1.23 (0.76; 2.01) | 0.81 (0.55; 1.19) |
| Medical trainee | 0.74 (0.59; 0.93) | 0.47 (0.29; 0.77) | |
| Nurse | 1.31 (0.95; 1.79) | 0.86 (0.48; 1.55) | |
| Laboratorist | 0.67 (0.32; 1.43) | 0.37 (0.21; 0.67) | |
| Nurse aid | 1.10 (0.79; 1.54) | 0.53 (0.38; 0.72) | |
| Administrative clerk | reference | reference | |
| Health technician | 0.86 (0.68; 1.09) | 0.73 (0.59; 0.91) | |
| Midwife | 0.62 (0.18; 2.05) | 0.37 (0.21; 0.64) | |
| Pharmacist | 1.07 (0.14; 8.24) | 0.71 (0.17; 2.93) | |
| Psychologist | 1.09 (0.93; 1.27) | 1.40 (0.78; 2.51) | |
| Physio-therapist | 1.25 (0.81; 1.93) | 0.40 (0.13; 1.26) | |
| Undergraduate student | 0.27 (0.19; 0.40) | 0.72 (0.41; 1.25) | |
| Other | 1.15 (0.84; 1.57) | 1.31 (0.58; 2.95) | |
| Current workplace (M: 59) | Infectious diseases | 0.46 (0.12; 1.76) | 1.74 (0.21; 14.54) |
| Pneumology | 0.38 (0.08; 1.87) | 0.90 (0.10; 8.31) | |
| ICU | 0.71 (0.39; 1.31) | 1.75 (0.51; 6.01) | |
| Internal medicine | 0.39 (0.24; 0.62) | 0.78 (0.44; 1.39) | |
| Surgical ward | 0.52 (0.36; 0.77) | 0.69 (0.15; 3.30) | |
| Radiology | 1.05 (0.51; 2.19) | 2.25 (0.75; 6.78) | |
| Administrative services | reference | reference | |
| Other | 0.64 (0.52; 0.78) | 1.20 (0.47; 3.06) | |
| Term | Strata | 2nd COVID-19 Infection (N = 238) N (%) | Long COVID-19 at 30–60 Days Since 1st Negative Swab | Long COVID-19 at 61+ Days Since 1st Negative Swab | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No (N = 213) N (%) | Yes (N = 25) N (%) | Logistic regression | No (N = 225) N (%) | Yes (N = 13) N (%) | Logistic regression | |||||
| Univariable (OR; 95%CI) | Multivariable (aOR; 95%CI) (214 obs.) | Univariable (OR; 95%CI) | Multivariable (aOR; 95%CI) (141 obs.) | |||||||
| COVID-19 vaccination status before infection | 0 | 44 (18.7) | 36 (81.8) | 8 (17.4) | reference | reference | 38 (86.4) | 6 (13.0) | reference | reference |
| 1 | 25 (10.6) | 23 (92.0) | 2 (8.0) | 0.39 (0.10; 1.47) | 0.71 (0.16; 3.12) | 24 (96.0) | 1 (4.0) | 0.26 (0.05; 1.49) | 0.44 (0.17; 1.11) | |
| 2 | 56 (23.8) | 53 (94.6) | 3 (5.5) | 0.25 (0.06; 1.02) | 0.47 (0.08; 2.76) | 56 (100) | 0 | omitted | omitted | |
| 3 | 110 (46.8) | 99 (90.0) | 11 (10.0) | 0.50 (0.17; 1.50) | 0.93 (0.18; 4.90) | 105 (95.5) | 5 (4.8) | 0.30 (0.07; 1.23) | 0.40 (0.10; 1.67) | |
| 4 | 0 | NA | NA | NA | NA | NA | NA | NA | NA | |
| Sex | Male | 48 (20.2) | 42 (87.5) | 6 (12.5) | reference | reference | 45 (93.8) | 3 (6.3) | reference | reference |
| Female | 190 (79.8) | 171 (90.0) | 19 (10.0) | 0.78 (0.49; 1.24) | 0.77 (0.40; 1.46) | 180 (94.7) | 10 (5.3) | 0.83 (0.44; 1.58) | 0.74 (0.31; 1.76) | |
| Age (years) | <40 | 88 (43.1) | 83 (94.3) | 5 (5.7) | reference | 86 (97.7) | 2 (2.3) | reference | ||
| 40–54 | 83 (40.7) | 73 (88.0) | 10 (12.1) | 2.27 (0.80; 6.50) | 79 (95.2) | 4 (4.8) | 2.18 (0.31; 15.16) | |||
| 55+ | 33 (16.2) | 29 (87.9) | 4 (12.1) | 2.29 (0.63; 6.27) | 30 (90.9) | 3 (9.1) | 4.30 (0.66; 27.92) | |||
| COVID-19 wave | 1 March 2020–31 Oct 2020 | 0 | 0 | 0 | omitted | omitted | 0 | 0 | Omitted | Omitted |
| 1 Nov 2020–31 May 2021 | 14 (6.0) | 11 (78.6) | 3 (21.4) | 2.52 (1.64; 3.86) | 1.03 (0.30; 3.57) | 12 (85.7) | 2 (14.3) | 3.42 (0.67; 17.36) | 0.54 (0.03; 9.87) | |
| 1 June 2021–30 Nov 2021 | 6 (2.6) | 6 (100) | 0 | 1 | Omitted | 6 (100) | 0 | Omitted | Omitted | |
| 1 Dec 2021–25 Aug 2022 | 215 (91.5) | 194 (90.2) | 21 (9.8) | reference | reference | 205 (95.4) | 10 (4.7) | reference | reference | |
| Viral shedding time (days) | 0–7 | 95 (43.0) | 90 (94.7) | 5 (5.3) | reference | reference | 92 (96.8) | 3 (3.2) | reference | reference |
| 8–10 | 65 (29.4) | 59 (90.8) | 6 (9.2) | 1.83 (1.25; 2.69) | 1.71 (1.51; 1.95) | 62 (95.4) | 3 (4.6) | 1.48 (0.44; 4.97) | 1.13 (0.38; 3.30) | |
| 11–14 | 23 (10.4) | 22 (95.7) | 1 (4.4) | 0.82 (0.10; 6.70) | 0.78 (0.08; 7.42) | 23 (100) | 0 | omitted | omitted | |
| 15+ | 38 (17.2) | 30 (79.0) | 8 (21.1) | 4.80 (2.87; 8.02) | 4.76 (2.81; 8.07) | 35 (92.1) | 3 (7.9) | 2.63 (1.49; 4.63) | 2.30 (0.98; 5.41) | |
| BMI (Kg/m2) | <18 | 2 (0.9) | 2 (100) | 0 | Omitted | 2 (100) | 0 | Omitted | Omitted | |
| 18–25 | 157 (68.6) | 140 (82.1) | 12 (7.9) | reference | 152 (96.8) | 5 (3.2) | reference | reference | ||
| 26–30 | 46 (20.1) | 37 (80.4) | 9 (19.6) | 2.94 (0.82; 10.59) | 41 (89.1) | 5 (10.9) | 3.71 (2.81; 4.90) | 4.66 (3.54; 6.14) | ||
| 31+ | 24 (10.5) | 20 (83.3) | 4 (16.7) | 2.42 (0.28; 21.43) | 21 (87.5) | 3 (12.5) | 4.34 (0.57; 33.01) | 1.73 (0.33; 8.97) | ||
| Ethnicity | Caucasian | 182 (87.5) | 162 (89.0) | 20 (11.0) | reference | reference | 45 (93.8) | 3 (6.3) | reference | reference |
| Other | 26 (12.5) | 22 (84.6) | 4 (15.5) | 1.47 (0.73; 2.96) | 2.44 (0.53; 11.28) | 180 (94.7) | 10 (5.3) | 2.51 (1.43; 4.40) | 5.70 (0.23; 140.57) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cegolon, L.; Mauro, M.; Sansone, D.; Tassinari, A.; Gobba, F.M.; Modenese, A.; Casolari, L.; Liviero, F.; Pavanello, S.; Scapellato, M.L.; et al. A Multi-Center Study Investigating Long COVID-19 in Healthcare Workers from North-Eastern Italy: Prevalence, Risk Factors and the Impact of Pre-Existing Humoral Immunity—ORCHESTRA Project. Vaccines 2023, 11, 1769. https://doi.org/10.3390/vaccines11121769
Cegolon L, Mauro M, Sansone D, Tassinari A, Gobba FM, Modenese A, Casolari L, Liviero F, Pavanello S, Scapellato ML, et al. A Multi-Center Study Investigating Long COVID-19 in Healthcare Workers from North-Eastern Italy: Prevalence, Risk Factors and the Impact of Pre-Existing Humoral Immunity—ORCHESTRA Project. Vaccines. 2023; 11(12):1769. https://doi.org/10.3390/vaccines11121769
Chicago/Turabian StyleCegolon, Luca, Marcella Mauro, Donatella Sansone, Alice Tassinari, Fabrizio Maria Gobba, Alberto Modenese, Loretta Casolari, Filippo Liviero, Sofia Pavanello, Maria Luisa Scapellato, and et al. 2023. "A Multi-Center Study Investigating Long COVID-19 in Healthcare Workers from North-Eastern Italy: Prevalence, Risk Factors and the Impact of Pre-Existing Humoral Immunity—ORCHESTRA Project" Vaccines 11, no. 12: 1769. https://doi.org/10.3390/vaccines11121769