
Immunotherapy for Urological Tumors on YouTubeTM: An Information-Quality Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
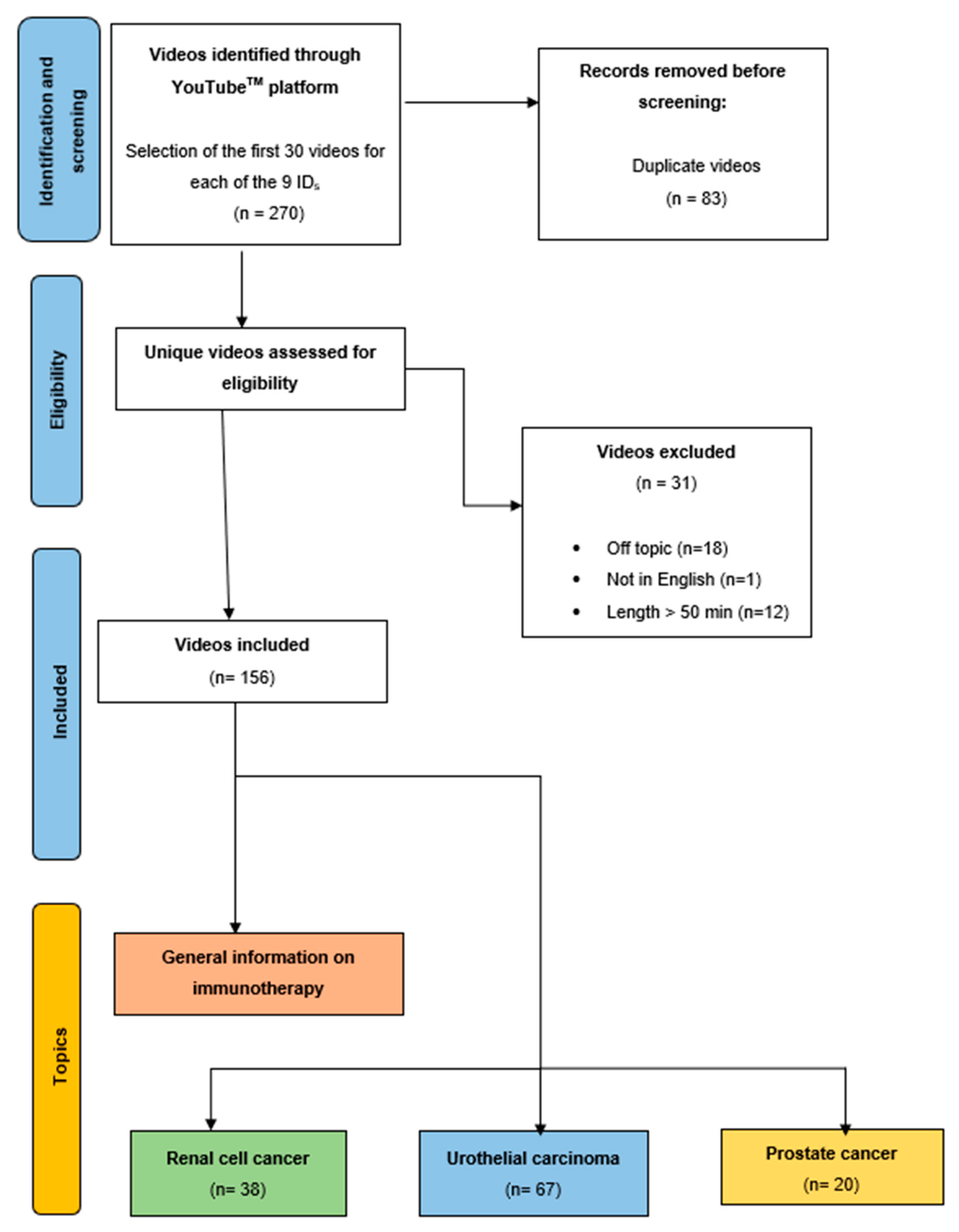
2.1. Search Strategy and Video Selection Criteria
2.2. Quality and Misinformation Assessment Tools
2.3. Statistical Analyses
3. Results
3.1. Videographic Characteristics and Video-Quality Assessment by Topic
3.1.1. Urothelial Carcinoma
3.1.2. Renal Cell Cancer
3.1.3. Prostate Cancer
3.1.4. General Information on Immunotherapy
3.2. Variable Correlations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Califano, G.; Ouzaid, I.; Laine-Caroff, P.; Peyrottes, A.; Ruvolo, C.C.; Pradère, B.; Elalouf, V.; Misrai, V.; Hermieu, J.-F.; Shariat, S.F.; et al. Current Advances in Immune Checkpoint Inhibition and Clinical Genomics in Upper Tract Urothelial Carcinoma: State of the Art. Curr. Oncol. 2022, 29, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Chang, Y.-H.; Hajek, J.; Symeonides, S.N.; Lee, J.L.; Sarwar, N.; et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N. Engl. J. Med. 2021, 385, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; de Wit, R.; Pang, L.; et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Balar, A.V.; Kamat, A.M.; Kulkarni, G.S.; Uchio, E.M.; Boormans, J.L.; Roumiguié, M.; Krieger, L.E.M.; Singer, E.; Bajorin, D.F.; Grivas, P.; et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. 2021, 22, 919–930. [Google Scholar] [CrossRef]
- Martini, A.; Fallara, G.; Pellegrino, F.; Cirulli, G.O.; Larcher, A.; Necchi, A.; Montorsi, F.; Capitanio, U. Neoadjuvant and adjuvant immunotherapy in renal cell carcinoma. World J. Urol. 2021, 39, 1369–1376. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Xu, L.; Yi, M.; Yu, S.; Wu, K.; Luo, S. Novel immune checkpoint targets: Moving beyond PD-1 and CTLA-4. Mol. Cancer 2019, 18, 155. [Google Scholar] [CrossRef] [Green Version]
- EAU Guidelines on MIBC—DISEASE MANAGEMENT—Uroweb. Uroweb—European Association of Urology. Available online: https://uroweb.org/guidelines/muscle-invasive-and-metastatic-bladder-cancer/chapter/disease-management (accessed on 15 May 2022).
- EAU Guidelines on Upper Urinary Tract Urothelial Cell Carcinoma—INTRODUCTION—Uroweb. Uroweb—European Association of Urology. Available online: https://uroweb.org/guidelines/upper-urinary-tract-urothelial-cell-carcinoma (accessed on 3 July 2022).
- EAU Guidelines on RCC—DISEASE MANAGEMENT—Uroweb. Uroweb—European Association of Urology. Available online: https://uroweb.org/guidelines/renal-cell-carcinoma/chapter/disease-management (accessed on 11 September 2022).
- Albiges, L.; Tannir, N.M.; Burotto, M.; McDermott, D.; Plimack, E.R.; Barthélémy, P.; Porta, C.; Powles, T.; Donskov, F.; George, S.; et al. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: Extended 4-year follow-up of the phase III CheckMate 214 trial. ESMO Open 2020, 5, e001079. [Google Scholar] [CrossRef]
- Weiss, S.A.; Djureinovic, D.; Jessel, S.; Krykbaeva, I.; Zhang, L.; Jilaveanu, L.; Ralabate, A.; Johnson, B.; Levit, N.S.; Anderson, G.; et al. A Phase I Study of APX005M and Cabiralizumab with or without Nivolumab in Patients with Melanoma, Kidney Cancer, or Non-Small Cell Lung Cancer Resistant to Anti-PD-1/PD-L1. Clin. Cancer Res. 2021, 27, 4757–4767. [Google Scholar] [CrossRef]
- Braun, D.A.; Bakouny, Z.; Hirsch, L.; Flippot, R.; Van Allen, E.M.; Wu, C.J.; Choueiri, T.K. Beyond conventional immune-checkpoint inhibition—Novel immunotherapies for renal cell carcinoma. Nat. Rev. Clin. Oncol. 2021, 18, 199–214. [Google Scholar] [CrossRef]
- Powles, T.; Plimack, E.R.; Soulières, D.; Waddell, T.; Stus, V.; Gafanov, R.; Nosov, D.; Pouliot, F.; Melichar, B.; Vynnychenko, I.; et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. 2020, 21, 1563–1573. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef]
- Tannir, N.M.; Frontera, O.A.; Hammers, H.J.; Carducci, M.A.; McDermott, D.F.; Salman, P.; Escudier, B.; Beuselinck, B.; Amin, A.; Porta, C.; et al. Thirty-month follow-up of the phase III CheckMate 214 trial of first-line nivolumab + ipilimumab (N+I) or sunitinib (S) in patients (pts) with advanced renal cell carcinoma (aRCC). JCO 2019, 37 (Suppl. 7), 547. [Google Scholar] [CrossRef]
- Motzer, R.; Tannir, N.; McDermott, D.; Burotto, M.; Choueiri, T.; Hammers, H.; Plimack, E.; Porta, C.; George, S.; Powles, T.; et al. 661P Conditional survival and 5-year follow-up in CheckMate 214: First-line nivolumab + ipilimumab (N+I) versus sunitinib (S) in advanced renal cell carcinoma (aRCC). Ann. Oncol. 2021, 32, S685–S687. [Google Scholar] [CrossRef]
- Motzer, R.J.; Choueiri, T.K.; Powles, T.; Burotto, M.; Bourlon, M.T.; Hsieh, J.J.; Maruzzo, M.; Shah, A.Y.; Suarez, C.; Barrios, C.H.; et al. Nivolumab + cabozantinib (NIVO+CABO) versus sunitinib (SUN) for advanced renal cell carcinoma (aRCC): Outcomes by sarcomatoid histology and updated trial results with extended follow-up of CheckMate 9ER. JCO 2021, 39 (Suppl. 6), 308. [Google Scholar] [CrossRef]
- Motzer, R.; Alekseev, B.; Rha, S.-Y.; Porta, C.; Eto, M.; Powles, T.; Grünwald, V.; Hutson, T.E.; Kopyltsov, E.; Méndez-Vidal, M.J.; et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N. Engl. J. Med. 2021, 384, 1289–1300. [Google Scholar] [CrossRef]
- Vuky, J.; Balar, A.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Bellmunt, J.; Powles, T.; Bajorin, D.; Hahn, N.M.; Savage, M.J.; et al. Long-Term Outcomes in KEYNOTE-052: Phase II Study Investigating First-Line Pembrolizumab in Cisplatin-Ineligible Patients With Locally Advanced or Metastatic Urothelial Cancer. J. Clin. Oncol. 2020, 38, 2658–2666. [Google Scholar] [CrossRef]
- Galsky, M.D.; Arija, J.Á.A.; Bamias, A.; Davis, I.D.; De Santis, M.; Kikuchi, E.; Garcia-Del-Muro, X.; De Giorgi, U.; Mencinger, M.; Izumi, K.; et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): A multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2020, 395, 1547–1557. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; van der Heijden, M.S.; Castellano, D.; Galsky, M.D.; Loriot, Y.; Petrylak, D.P.; Ogawa, O.; Park, S.H.; Lee, J.-L.; De Giorgi, U.; et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): A randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2020, 21, 1574–1588. [Google Scholar] [CrossRef]
- Powles, T.; Csőszi, T.; Özgüroğlu, M.; Matsubara, N.; Géczi, L.; Cheng, S.Y.; Fradet, Y.; Oudard, S.; Vulsteke, C.; Barrera, R.M.; et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 931–945. [Google Scholar] [CrossRef]
- Necchi, A.; Anichini, A.; Raggi, D.; Briganti, A.; Massa, S.; Lucianò, R.; Colecchia, M.; Giannatempo, P.; Mortarini, R.; Bianchi, M.; et al. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J. Clin. Oncol. 2018, 36, 3353–3360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldeek, B.; Alahmadi, J.; Al-Attas, M.; Sait, K.; Anfinan, N.; Aljahdali, E.; Ajaj, H.; Sait, H. Knowledge, perception, and attitudes about cancer and its treatment among healthy relatives of cancer patients: Single institution hospital-based study in Saudi Arabia. J. Cancer Educ. 2014, 29, 772–780. [Google Scholar] [CrossRef]
- Sait, K.H.; Anfinan, N.M.; Eldeek, B.; Al-Ahmadi, J.; Al-Attas, M.; Sait, H.K.; Basalamah, H.A.; Al-Ama, N.; El Sayed, M.E. Perception of patients with cancer towards support management services and use of complementary alternative medicine—A single institution hospital-based study in Saudi Arabia. Asian Pac. J. Cancer Prev. 2014, 15, 2547–2554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scandurra, C.; Muzii, B.; La Rocca, R.; Di Bello, F.; Bottone, M.; Califano, G.; Longo, N.; Maldonato, N.M.; Mangiapia, F. Social Support Mediates the Relationship between Body Image Distress and Depressive Symptoms in Prostate Cancer Patients. Int. J. Environ. Res. Public Health 2022, 19, 4825. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Mangiapia, F.; La Rocca, R.; Di Bello, F.; De Lucia, N.; Muzii, B.; Cantone, M.; Zampi, R.; Califano, G.; Maldonato, N.M.; et al. A cross-sectional study on demoralization in prostate cancer patients: The role of masculine self-esteem, depression, and resilience. Support. Care Cancer 2022, 30, 7021–7030. [Google Scholar] [CrossRef]
- Dinesh, A.A.; Pinto, S.H.P.S.; Brunckhorst, O.; Dasgupta, P.; Ahmed, K. Anxiety, depression and urological cancer outcomes: A systematic review. Urol. Oncol. 2021, 39, 816–828. [Google Scholar] [CrossRef]
- Pew Research Center. Social Media Fact Sheet. Available online: https://www.pewinternet.org/fact-sheet/social-media/ (accessed on 25 March 2022).
- Creta, M.; Sagnelli, C.; Celentano, G.; Napolitano, L.; La Rocca, R.; Capece, M.; Califano, G.; Calogero, A.; Sica, A.; Mangiapia, F.; et al. SARS-CoV-2 infection affects the lower urinary tract and male genital system: A systematic review. J. Med. Virol. 2021, 93, 3133–3142. [Google Scholar] [CrossRef]
- Ruvolo, C.C.; Califano, G.; Tuccillo, A.; Tolentino, S.; Cancelliere, E.; Di Bello, F.; Celentano, G.; Creta, M.; Longo, N.; Morra, S.; et al. YouTubeTM as a source of information on placenta accreta: A quality analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 272, 82–87. [Google Scholar] [CrossRef]
- Melchionna, A.; Collà Ruvolo, C.; Capece, M.; La Rocca, R.; Celentano, G.; Califano, G.; Creta, M.; Napolitano, L.; Morra, S.; Cilio, S.; et al. Testicular pain and youtubeTM: Are uploaded videos a reliable source to get information? Int. J. Impot. Res. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Turco, C.; Ruvolo, C.C.; Cilio, S.; Celentano, G.; Califano, G.; Creta, M.; Capece, M.; La Rocca, R.; Napolitano, L.; Mangiapia, F.; et al. Looking for cystoscopy on YouTube: Are videos a reliable information tool for internet users? Arch. Ital. Urol. Androl. 2022, 94, 57–61. [Google Scholar] [CrossRef]
- Di Bello, F.; Collà Ruvolo, C.; Cilio, S.; La Rocca, R.; Capece, M.; Creta, M.; Celentano, G.; Califano, G.; Morra, S.; Iacovazzo, C.; et al. Testicular cancer and YouTube: What do you expect from a social media platform? Int. J. Urol. 2022, 29, 685–691. [Google Scholar] [CrossRef]
- Morra, S.; Collà Ruvolo, C.; Napolitano, L.; La Rocca, R.; Celentano, G.; Califano, G.; Creta, M.; Capece, M.; Turco, C.; Cilio, S.; et al. YouTubeTM as a source of information on bladder pain syndrome: A contemporary analysis. Neurourol. Urodyn. 2022, 41, 237–245. [Google Scholar] [CrossRef]
- McKay, R.R. The Promise of Adjuvant Immunotherapy in Renal-Cell Carcinoma. N. Engl. J. Med. 2021, 385, 756–758. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Aren Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Mendiratta, P.; Rini, B.I.; Ornstein, M.C. Emerging immunotherapy in advanced renal cell carcinoma. Urol. Oncol. 2017, 35, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Sosman, J.A.; Atkins, M.B.; Leming, P.D.; et al. Five-Year Survival and Correlates Among Patients with Advanced Melanoma, Renal Cell Carcinoma, or Non-Small Cell Lung Cancer Treated with Nivolumab. JAMA Oncol. 2019, 5, 1411–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDermott, D.F.; Lee, J.-L.; Bjarnason, G.A.; Larkin, J.M.G.; Gafanov, R.A.; Kochenderfer, M.D.; Jensen, N.V.; Donskov, F.; Malik, J.; Poprach, A.; et al. Open-Label, Single-Arm Phase II Study of Pembrolizumab Monotherapy as First-Line Therapy in Patients With Advanced Clear Cell Renal Cell Carcinoma. J. Clin. Oncol. 2021, 39, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
- Massard, C.; Gordon, M.S.; Sharma, S.; Rafii, S.; Wainberg, Z.A.; Luke, J.; Curiel, T.J.; Colon-Otero, G.; Hamid, O.; Sanborn, R.E.; et al. Safety and Efficacy of Durvalumab (MEDI4736), an Anti-Programmed Cell Death Ligand-1 Immune Checkpoint Inhibitor, in Patients with Advanced Urothelial Bladder Cancer. J. Clin. Oncol. 2016, 34, 3119–3125. [Google Scholar] [CrossRef] [Green Version]
- Bristol-Myers Squibb. A Phase 3 Randomized, Double-Blind Study of Nivolumab Monotherapy or Nivolumab Combined With Ipilimumab vs. Placebo in Participants With Localized Renal Cell Carcinoma Who Underwent Radical or Partial Nephrectomy and Who Are at High Risk of Relapse. clinicaltrials.gov; 2022 mag. Report No.: NCT03138512. Available online: https://clinicaltrials.gov/ct2/show/NCT03138512 (accessed on 15 June 2022).
- Ruvolo, C.C.; Nocera, L.; Stolzenbach, L.F.; Wenzel, M.; Cucchiara, V.; Tian, Z.; Shariat, S.F.; Saad, F.; Longo, N.; Montorsi, F.; et al. Incidence and Survival Rates of Contemporary Patients with Invasive Upper Tract Urothelial Carcinoma. Eur. Urol. Oncol. 2021, 4, 792–801. [Google Scholar] [CrossRef]
- Approval Timelines of Active Immunotherapies. Cancer Research Institute. Available online: https://www.cancerresearch.org/en-us/scientists/immuno-oncology-landscape/fda-approval-timeline-of-active-immunotherapies (accessed on 28 September 2022).
- Capece, M.; Di Giovanni, A.; Cirigliano, L.; Napolitano, L.; La Rocca, R.; Creta, M.; Califano, G.; Crocetto, F.; Ruvolo, C.C.; Celentano, G.; et al. YouTube as a source of information on penile prosthesis. Andrologia 2021, 54, e14246. [Google Scholar] [CrossRef] [PubMed]
- Cilio, S.; Collà Ruvolo, C.; Turco, C.; Creta, M.; Capece, M.; La Rocca, R.; Celentano, G.; Califano, G.; Morra, S.; Melchionna, A.; et al. Analysis of quality information provided by «Dr. YouTubeTM» on Phimosis. Int. J. Impot. Res. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gerundo, G.; Ruvolo, C.C.; Puzone, B.; Califano, G.; La Rocca, R.; Parisi, V.; Capece, M.; Celentano, G.; Creta, M.; Rengo, G.; et al. Personal protective equipment in Covid-19: Evidence-based quality and analysis of YouTube videos after one year of pandemic. Am. J. Infect. Control 2021, 50, 300–305. [Google Scholar] [CrossRef]
- Peyrottes, A.; Ouzaid, I.; Califano, G.; Hermieu, J.-F.; Xylinas, E. Neoadjuvant Immunotherapy for Muscle-Invasive Bladder Cancer. Medicina 2021, 57, 769. [Google Scholar] [CrossRef]
- Califano, G.; Ouzaid, I.; Verze, P.; Hermieu, J.-F.; Mirone, V.; Xylinas, E. Immune checkpoint inhibition in upper tract urothelial carcinoma. World J. Urol. 2021, 39, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Califano, G.; Ouzaid, I.; Verze, P.; Stivalet, N.; Hermieu, J.-F.; Xylinas, E. New immunotherapy treatments in non-muscle invasive bladder cancer. Arch. Esp. Urol. 2020, 73, 945–953. [Google Scholar] [PubMed]
- Longo, N.; Capece, M.; Celentano, G.; La Rocca, R.; Califano, G.; Ruvolo, C.C.; Buonerba, C.; Esposito, F.; Napolitano, L.; Mangiapia, F.; et al. Clinical and Pathological Characteristics of Metastatic Renal Cell Carcinoma Patients Needing a Second-Line Therapy: A Systematic Review. Cancers 2020, 12, 3634. [Google Scholar] [CrossRef]
- Morra, S.; Napolitano, L.; Ruvolo, C.C.; Celentano, G.; La Rocca, R.; Capece, M.; Creta, M.; Passaro, F.; Di Bello, F.; Cirillo, L.; et al. Could YouTubeTM encourage men on prostate checks? A contemporary analysis. Arch. Ital. Urol. Androl. 2022, 94, 285–290. [Google Scholar] [CrossRef]
- Hyatt, A.; Morkunas, B.; Davey, D.; Thai, A.A.; Trewhella, M.; Duffy, M.; Dawson, T.; Gourlay, P.; Hutchison, J.; Milne, D. Co-design and development of online video resources about immunotherapy with patients and their family. Patient. Educ. Couns. 2021, 104, 290–297. [Google Scholar] [CrossRef]
- Califano, G.; Xylinas, E. Re: Phase II Trial of Neoadjuvant Systemic Chemotherapy Followed by Extirpative Surgery in Patients with High Grade Upper Tract Urothelial Carcinoma. Eur. Urol. 2020, 78, 113–114. [Google Scholar] [CrossRef]
- Pereira, R.C.A.; Moreira, M.L.; Costa, I.P.D.A.; Tenório, F.M.; Barud, N.A.; Fávero, L.P.; Al-Qudah, A.A.; Gomes, C.F.S.; dos Santos, M. Feasibility of a Hospital Information System for a Military Public Organization in the Light of the Multi-Criteria Analysis. Healthcare 2022, 10, 2147. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Overall N = 156 | UC N = 67 (42.9%) | RCC N = 38 (24.3%) | PCa N = 20 (12.8%) | General Information on IMT N = 31 (19.8%) | p Value | |
|---|---|---|---|---|---|---|---|
| Length (sec) | Median (IQR) | 293.5(151–971.8) | 342 (168.5–1135) | 166.5 (89–408.8) | 573.5 (294–1588.5) | 303 (210.5–912) | 0.3 |
| Number of views | Median (IQR) | 691.5 (224–8041) | 420 (118–2003.5) | 369 (174.2–896) | 1570 (213.8–4612) | 33242 (8247.5–126,449) | <0.001 |
| Persistence on YouTube™ (days) | Median (IQR) | 1365 (614.5–1795.5) | 1269 (560–1695.5) | 1608.5 (897.5–1919.5) | 1324.5 (622–1635.5) | 1359 (637–1751.5) | 0.5 |
| Thumbs up (n) | Median (IQR) | 7 (1–64.2) | 3 (1–13.5) | 2.5 (1–11) | 10.5 (0.8–51) | 261 (93–913.5) | <0.001 |
| Number of comments | Median (IQR) | 1 (0–6) | 0 (0–1) | 0 (0–1) | 0 (0–6) | 17 (5–93) | <0.001 |
| Channel subscribers (n) | Median (IQR) | 16,900 (4500–30,375) | 12,200 (4500–16,900) | 16,900 (4590–17,500) | 30,600 (17,900–140,100) | 41,700 (7300–684,000) | 0.07 |
| View ratio | Median (IQR) | 1 (0.2–6.2) | 0.4 (0.1–3.3) | 0.4 (0.1–1.1) | 1 (0.3–6.6) | 33.5 (4.8–161.5) | <0.001 |
| Videos with disabled comments n (%) | No | 135 (86.5) | 55 (82.1) | 34 (89.5) | 19 (95) | 27 (87.1) | 0.2 |
| Yes | 21 (13.5) | 12 (17.9) | 4 (10.5) | 1 (5) | 4 (12.9) | ||
| Video author n (%) | Medical Association | 85 (54.5) | 38 (56.7) | 26 (68.4) | 5 (25) | 16 (51.6) | 0.01 |
| Medical Center, Hospital, or University | 35 (22.4) | 11 (16.4) | 5 (13.2) | 9 (45) | 10 (32.3) | 0.01 | |
| Other | 36 (23.1) | 18 (26.9) | 7 (18.4) | 6 (30) | 5 (16.1) | 0.5 |
| Overall N = 156 | UC N = 67 (42.9%) | RCC N = 38 (24.3%) | PCa N = 20 (12.8%) | General Information on IMT N = 31 (19.8%) | p Value | ||
|---|---|---|---|---|---|---|---|
| PEMAT Understandability | Median (IQR) | 40 (20–61.5) | 40 (20–61.5) | 26.1 (20–44.1) | 28.2 (20–52.1) | 61.5 (50–75) | <0.001 |
| PEMAT Actionability | Median (IQR) | 0 (0–25) | 0 (0–0) | 0 (0–18.8) | 0 (0–0) | 25 (0–50) | <0.001 |
| Overall N = 156 | UC N = 67 (42.9%) | RCC N = 38 (24.3%) | PCa N = 20 (12.8%) | General information on IMT N = 31 (19.8%) | p Value | |||
|---|---|---|---|---|---|---|---|---|
| Section 1: Is the publication reliable? | SUM Section 1 (max score 40) Question 1–8 | Median (IQR) | 20 (16–24) | 20 (17–24.5) | 21 (15.2–23) | 20.5 (16–24) | 16 (14–20.5) | 0.3 |
| Section 2: How good is the quality of information on treatment choices? | SUM Section 2 (max score 35) Question 9–15 | Median (IQR) | 20 (16–24) | 20 (17–24.5) | 21 (15.2–23) | 20.5 (16–24) | 16 (14–20.5) | 0.01 |
| Section 3: Overall Quality rating | 16. Based on the answers to all the above questions, rate the overall quality of the publication as a source of information about treatment choices (max score 5) | Median (IQR) | 4 (4–4) | 4 (3–4) | 4 (4–4) | 4 (4–4) | 4 (3.5–5) | 0.5 |
| DISCERN score | Median (IQR) | 44 (39–53.2) | 45 (40–55.5) | 43.5 (41–52) | 46.5 (41–53) | 45 (36–49.5) | 0.2 | |
| Overall N = 156 | UCs N = 67 (42.9%) | RCC N = 38 (24.3%) | PCa N = 20 (12.8%) | General information on IMT N = 31 (19.8%) | p value | ||
|---|---|---|---|---|---|---|---|
| 1.“Logical sequence of information” | Median (IQR) | 4 (3–4) | 3 (3–4) | 4 (2–4) | 4 (3–4) | 4 (3–5) | 0.01 |
| 2.“Therapeutic effects” | Median (IQR) | 4 (3–4) | 3 (3–4) | 4 (2–4) | 4 (3–4) | 4 (3–5) | 0.3 |
| 3.“Treatment-emergent adverse effects” | Median (IQR) | 3 (2–4) | 4 (2–4) | 2 (2–4) | 3 (2–4) | 2 (2–4) | 0.8 |
| 4.“IMT in multimodality approach” | Median (IQR) | 2 (2–3) | 3 (2–3) | 2 (2–3.8) | 2.5 (2–3) | 2 (1–3) | 0.2 |
| 5.“Future perspective” | Median (IQR) | 2 (1.8–4) | 2 (2–3.5) | 3 (1–4) | 3 (2–4) | 2 (1–3) | 0.03 |
| Misinformation score | Median (IQR) | 2.8 (2.4–3.6) | 2.8 (2.4–3.6) | 3 (2.2–3.6) | 2.3 (2.4–4) | 2.8 (2.4–3.5) | 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Bello, F.; Di Mauro, E.; Collà Ruvolo, C.; Creta, M.; La Rocca, R.; Celentano, G.; Capece, M.; Napolitano, L.; Fraia, A.; Pezone, G.; et al. Immunotherapy for Urological Tumors on YouTubeTM: An Information-Quality Analysis. Vaccines 2023, 11, 92. https://doi.org/10.3390/vaccines11010092
Di Bello F, Di Mauro E, Collà Ruvolo C, Creta M, La Rocca R, Celentano G, Capece M, Napolitano L, Fraia A, Pezone G, et al. Immunotherapy for Urological Tumors on YouTubeTM: An Information-Quality Analysis. Vaccines. 2023; 11(1):92. https://doi.org/10.3390/vaccines11010092
Chicago/Turabian StyleDi Bello, Francesco, Ernesto Di Mauro, Claudia Collà Ruvolo, Massimiliano Creta, Roberto La Rocca, Giuseppe Celentano, Marco Capece, Luigi Napolitano, Agostino Fraia, Gabriele Pezone, and et al. 2023. "Immunotherapy for Urological Tumors on YouTubeTM: An Information-Quality Analysis" Vaccines 11, no. 1: 92. https://doi.org/10.3390/vaccines11010092