
Organisational and Structural Drivers of Childhood Immunisation in the European Region: A Systematic Review
 , , , ,
, , , ,
Abstract
:1. Introduction
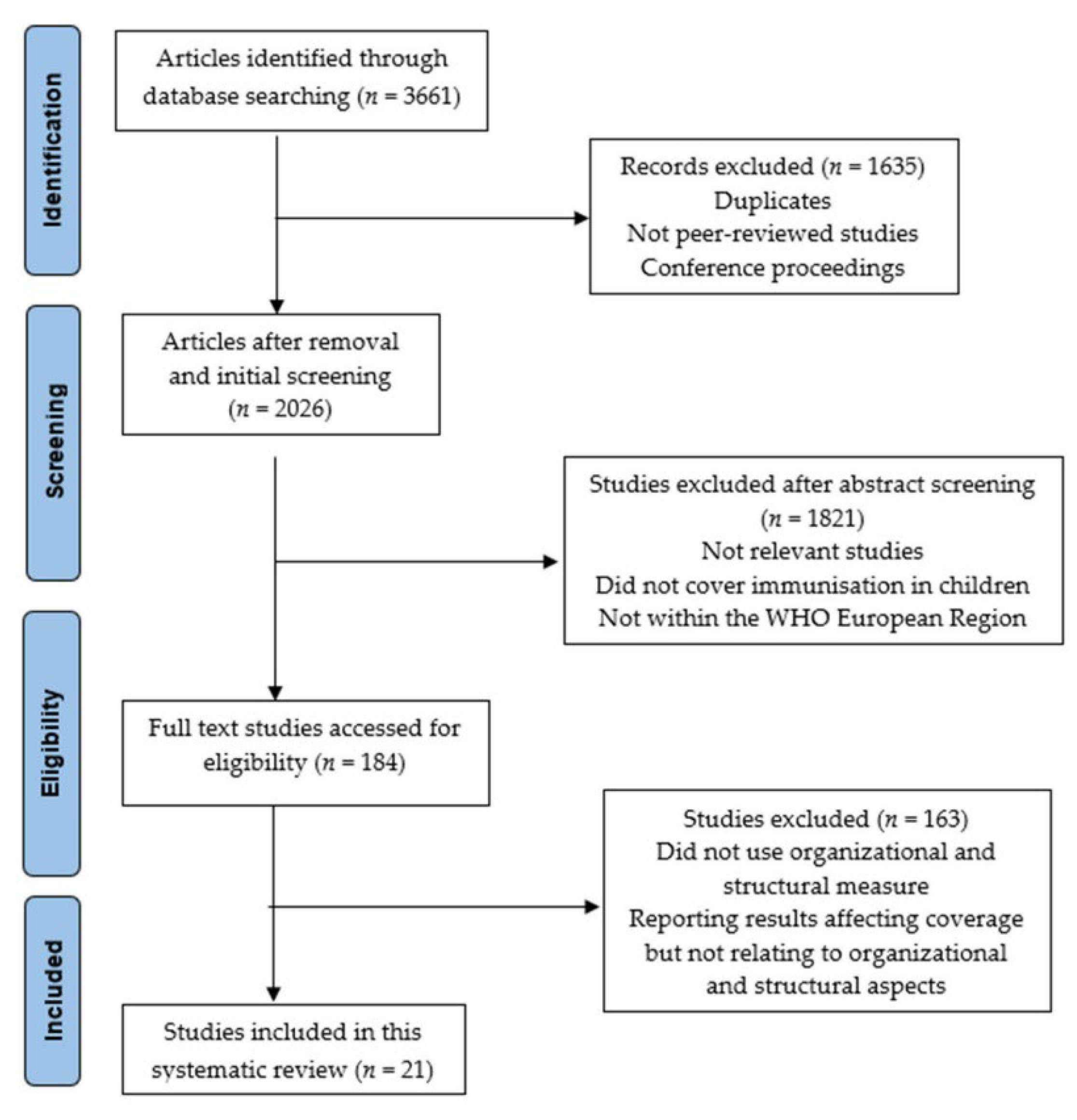
2. Methodology
2.1. Criteria for Inclusion and Exclusion
2.2. Search Strategy
2.3. Data Extraction and Quality Assessment
3. Results
3.1. Characteristics of Included Articles
3.2. Parents’ Engagement and Personalisation Intervention
3.3. Mandatory Immunisation Policy
3.4. Vaccination Program Remodeling
3.5. Vaccination Procurement and Distribution
3.6. Combination/Multiple Vaccine Administration
3.7. Improved Immunisation Timing and Intervals
3.8. Parental Education and Reminder
3.9. Surveillance Tools and Supplementary Immunisation Activity (SIA)
3.10. Information Technology
4. Discussion and Implications
5. Strengths and Limitations
6. Policy Implications and Future Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, X.; Mukandavire, C.; Cucunubá, Z.M.; Echeverria Londono, S.; Abbas, K.; Clapham, H.E.; Jit, M.; Johnson, H.L.; Papadopoulos, T.; Vynnycky, E.; et al. Estimating the health impact of vaccination against ten pathogens in 98 low-income and middle-income countries from 2000 to 2030: A modelling study. Lancet 2021, 397, 398–408. [Google Scholar] [CrossRef]
- Galles, N.C.; Liu, P.Y.; Updike, R.L.; Fullman, N.; Nguyen, J.; Rolfe, S.; Sbarra, A.N.; Schipp, M.F.; Marks, A.; Abady, G.G.; et al. Measuring routine childhood vaccination coverage in 204 countries and territories, 1980–2019: A systematic analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021, 398, 503–521. [Google Scholar] [CrossRef]
- World Health Organization. The Global Vaccine Action Plan 2011–2020: Review and Lessons Learned: Strategic Advisory Group of Experts on Immunization; WHO: Geneva, Switzerland, 2019; p. 77. [Google Scholar]
- Muhoza, P.; Danovaro-Holliday, M.C.; Diallo, M.S.; Murphy, P.; Sodha, S.V.; Requejo, J.H.; Wallace, A.S. Routine Vaccination Coverage—Worldwide, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1495–1500. [Google Scholar] [CrossRef]
- World Health Organization. Immunization, Vaccines and Biologicals. Available online: https://apps.who.int/immunization_monitoring/globalsummary/timeseries/tscoveragemcv2.html (accessed on 10 June 2021).
- Vecchio, A.L.; Cambriglia, M.D.; Fedele, M.C.; Basile, F.W.; Chiatto, F.; del Giudice, M.M.; Guarino, A. Determinants of low measles vaccination coverage in children living in an endemic area. Eur. J. Pediatr. 2018, 178, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Chiappini, E.; Parigi, S.; Galli, L.; Licari, A.; Brambilla, I.; Tosca, M.A.; Ciprandi, G.; Marseglia, G. Impact that the COVID-19 pandemic on routine childhood vaccinations and challenges ahead: A narrative review. Acta Paediatr. 2021, 110, 2529–2535. [Google Scholar] [CrossRef]
- DeSilva, M.B.; Haapala, J.; Vazquez-Benitez, G.; Daley, M.F.; Nordin, J.D.; Klein, N.P.; Henninger, M.L.; Williams, J.T.B.; Hambidge, S.J.; Jackson, M.L.; et al. Association of the COVID-19 Pandemic with Routine Childhood Vaccination Rates and Proportion Up to Date with Vaccinations Across 8 US Health Systems in the Vaccine Safety Datalink. JAMA Pediatr. 2022, 176, 68. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N. Differences in vaccinations in European Union. Hum. Vaccines 2008, 4, 313–315. [Google Scholar] [CrossRef]
- Pelullo, C.P.; Marino, S.; Abuadili, A.J.V.; Signoriello, G.; Attena, F. Is it reasonable to abandon obligatory vaccinations in Italy? A 2013 survey. Eurosurveillance 2014, 19, 20889. [Google Scholar] [CrossRef]
- Loer, K. Approaches and Instruments in Health Promotion and the Prevention of Diseases. In Behavioural Policies for Health Promotion and Disease Prevention; Springer International Publishing: Berlin, Germany, 2019; pp. 29–52. [Google Scholar]
- Rigby, M.J.; Chronaki, C.E.; Deshpande, S.S.; Altorjai, P.; Brenner, M.; Blair, M.E. European Union Initiatives in Child Immunization - The Need for Child Centricity, e-Health and Holistic Delivery. Eur J. Public Health 2020, 30, 449–455. [Google Scholar] [CrossRef]
- Wiese-Posselt, M.; Reiter, S.; Gilsdorf, A.; Krause, G. Notwendigkeiten Und Hürden Einheitlicher Impfempfehlungen in Der Europäischen Union. Bundesgesundheitsblatt Gesundh. Gesundh. 2009, 52, 1099–1104. [Google Scholar] [CrossRef] [Green Version]
- Blume, S. Anti-Vaccination Movements and Their Interpretations. Soc. Sci. Med. 2006, 62, 628–642. [Google Scholar] [CrossRef] [PubMed]
- Three Shots at Prevention: The HPV Vaccine and the Politics of Medicine’s. Available online: https://books.google.it/books?hl=en&lr=&id=_fBcYB4g5DkC&oi=fnd&pg=PA270&dq=L%C3%B6wy+I.+HPV+vaccination+in+context:+a+view+from+France.+In:+Wailoo+K,+Livingston+J,+Epstein+S,+Aronowitz+R,+editors.+The+HPV+vaccine+controversies.+New+Brunswick:+Rutgers+University+Press%3B+2010.+p.+270%E2%80%93&ots=ByWo6qLolE&sig=FUu153ZFxljqcYzyBREy_2C-gig&redir_esc=y#v=onepage&q&f=false (accessed on 11 June 2021).
- Bram, J.T.; Warwick-Clark, B.; Obeysekare, E.; Mehta, K. Utilization and Monetization of Healthcare Data in Developing Countries. Big Data 2015, 3, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.F.; Kroll, J.S.; Hudson, M.J.; Ramsay, M.; Green, J.; Long, S.J.; Vincent, C.A.; Fraser, G.; Sevdalis, N. Factors Underlying Parental Decisions about Combination Childhood Vaccinations Including MMR: A Systematic Review. Vaccine 2010, 28, 4235–4248. [Google Scholar] [CrossRef] [PubMed]
- Williams, N.; Woodward, H.; Majeed, A.; Saxena, S. Primary care strategies to improve childhood immunisation uptake in developed countries: Systematic review. JRSM Short Rep. 2011, 2, 1–21. [Google Scholar] [CrossRef]
- Henrikson, N.B.; Opel, D.J.; Grothaus, L.; Nelson, J.; Scrol, A.; Dunn, J.; Faubion, T.; Roberts, M.; Marcuse, E.K.; Grossman, D.C. Physician Communication Training and Parental Vaccine Hesitancy: A Randomized Trial. Pediatrics 2015, 136, 70–79. [Google Scholar] [CrossRef]
- Turner, N.M.; Charania, N.A.; Chong, A.; Stewart, J.; Taylor, L. The challenges and opportunities of translating best practice immunisation strategies among low performing general practices to reduce equity gaps in childhood immunisation coverage in New Zealand. BMC Nurs. 2017, 16, 31. [Google Scholar] [CrossRef]
- Sadaf, A.; Richards, J.L.; Glanz, J.; Salmon, D.A.; Omer, S.B. A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine 2013, 31, 4293–4304. [Google Scholar] [CrossRef]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- Nowak, G.J.; Gellin, B.G.; MacDonald, N.E.; Butler, R. Addressing vaccine hesitancy: The potential value of commercial and social marketing principles and practices. Vaccine 2015, 33, 4204–4211. [Google Scholar] [CrossRef]
- Olson, O.; Berry, C.; Kumar, N. Addressing Parental Vaccine Hesitancy towards Childhood Vaccines in the United States: A Systematic Literature Review of Communication Interventions and Strategies. Vaccines 2020, 8, 590. [Google Scholar] [CrossRef]
- Kumar, D.; Chandra, R.; Mathur, M.; Samdariya, S.; Kapoor, N. Vaccine hesitancy: Understanding better to address better. Isr. J. Health Policy Res. 2016, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Koshy, E.; Murray, J.; Bottle, A.; Sharland, M.; Saxena, S. Impact of the seven-valent pneumococcal conjugate vaccination (PCV7) programme on childhood hospital admissions for bacterial pneumonia and empyema in England: National time-trends study, 1997–2008. Thorax 2010, 65, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Derrough, T.; Olsson, K.; Gianfredi, V.; Simondon, F.; Heijbel, H.; Danielsson, N.; Kramarz, P.; Pastore-Celentano, L. Immunisation Information Systems—Useful Tools for Monitoring Vaccination Programmes in EU/EEA Countries, 2016. Eurosurveillance 2017, 22, 30519. [Google Scholar] [CrossRef] [PubMed]
- Fadda, M.; Depping, M.K.; Schulz, P.J. Addressing Issues of Vaccination Literacy and Psychological Empowerment in the Measles-Mumps-Rubella (MMR) Vaccination Decision-Making: A Qualitative Study Infectious Disease Epidemiology. BMC Public Health 2015, 15, 836. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Rayyan. Intelligent Systematic Review. Available online: https://www.rayyan.ai/ (accessed on 1 March 2022).
- Wells, G.; Shea, B.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Ott. Ott. Hosp. Res. Inst. 2011, 2, 1–12. [Google Scholar]
- Joanna Briggs Institute. Checklist for Systematic Reviews and Research Syntheses Critical Appraisal Checklist for Systematic Reviews and Research Syntheses 2; Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- AMSTAR—Assessing the Methodological Quality of Systematic Reviews. Available online: https://amstar.ca/Amstar_Checklist.php (accessed on 15 February 2022).
- Gofen, A.; Blomqvist, P.; Needham, C.E.; Warren, K.; Winblad, U. Negotiated compliance at the street level: Personalizing immunization in England, Israel and Sweden. Public Adm. 2017, 97, 195–209. [Google Scholar] [CrossRef]
- Lwembe, S.; Green, S.A.; Tanna, N.; Connor, J.; Valler, C.; Barnes, R. A Qualitative Evaluation to Explore the Suitability, Fea-sibility and Acceptability of Using a “celebration Card” Intervention in Primary Care to Improve the Uptake of Childhood Vaccinations. BMC Fam. Pract. 2016, 17, 1–11. [Google Scholar] [CrossRef]
- Gamlund, E.; Müller, K.E.; Paquet, K.K.; Solberg, C.T. Mandatory childhood vaccination: Should Norway follow? Etikk i Praksis Nord. J. Appl. Ethics 2020, 14, 7–27. [Google Scholar] [CrossRef]
- Bozzola, E.; Spina, G.; Russo, R.; Bozzola, M.; Corsello, G.; Villani, A. Mandatory vaccinations in European countries, undocumented information, false news and the impact on vaccination uptake: The position of the Italian pediatric society. Ital. J. Pediatr. 2018, 44, 1–4. [Google Scholar] [CrossRef]
- Lévy-Bruhl, D.; Desenclos, J.C.; Quelet, S.; Bourdillon, F. Extension of French Vaccination Mandates: From the Recommendation of the Steering Committee of the Citizen Consultation on Vaccination to the Law. Eurosurveillance 2018, 23, 18-00048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianfredi, V.; D’Ancona, F.; Maraglino, F.; Cenci, C.; Iannazzo, S. Polio and measles: Reasons of missed vaccination in Italy, 2015–2017. Ann. Ig. Med. Prev. Comunita 2019, 31, 191–201. [Google Scholar] [CrossRef]
- Martinot, A.; Leboucher, B.; Cohen, R.; Stahl, J.-P.; Subtil, D.; Pujol, P.; Lepetit, H.; Longfier, L.; Gaudelus, J. Evolution between 2008 and 2018 of mothers’ perception regarding vaccination and infant vaccine coverage in France. Infect. Dis. Now 2021, 51, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Panovska-Griffiths, J.; Crowe, S.; Pagel, C.; Shiri, T.; Grove, P.; Utley, M. A method for evaluating and comparing immunisation schedules that cover multiple diseases: Illustrative application to the UK routine childhood vaccine schedule. Vaccine 2018, 36, 5340–5347. [Google Scholar] [CrossRef]
- Hardelid, P.; Rait, G.; Gilbert, R.; Petersen, I. Factors associated with influenza vaccine uptake during a universal vaccination programme of preschool children in England and Wales: A cohort study. J. Epidemiol. Community Health 2016, 70, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Petráš, M.; Adámková, V. Epidemiology of Invasive Pneumococcal Disease in Czech Children under 5 Years of Age after Routine Immunisation. Cent. Eur. J. Public Health 2016, 24, 133–136. [Google Scholar] [CrossRef]
- Grieco, L.; Panovska-Griffiths, J.; van Leeuwen, E.; Grove, P.; Utley, M. Exploring the role of mass immunisation in influenza pandemic preparedness: A modelling study for the UK context. Vaccine 2020, 38, 5163–5170. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K.B.; Holck, M.E.; Jensen, A.K.; Suppli, C.H.; Benn, C.S.; Krause, T.G.; Sørup, S. How are children who are delayed in the Childhood Vaccination Programme vaccinated: A nationwide register-based cohort study of Danish children aged 15–24 months and semi-structured interviews with vaccination providers. Scand. J. Public Health 2018, 48, 96–105. [Google Scholar] [CrossRef]
- Bielicki, J.A.; Achermann, R.; Berger, C. Timing of Measles Immunization and Effective Population Vaccine Coverage. Pediatrics 2012, 130, e600–e606. [Google Scholar] [CrossRef]
- Schweitzer, A.; Krause, G.; Pessler, F.; Akmatov, M.K. Improved coverage and timing of childhood vaccinations in two post-Soviet countries, Armenia and Kyrgyzstan. BMC Public Health 2015, 15, 798. [Google Scholar] [CrossRef]
- Napolitano, F.; D’Alessandro, A.; Angelillo, I.F. Investigating Italian parents’ vaccine hesitancy: A cross-sectional survey. Hum. Vaccines Immunother. 2018, 14, 1558–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlopoulou, I.D.; Michail, K.A.; Samoli, E.; Tsiftis, G.; Tsoumakas, K. Immunization coverage and predictive factors for complete and age-appropriate vaccination among preschoolers in Athens, Greece: A cross-sectional study. BMC Public Health 2013, 13, 908. [Google Scholar] [CrossRef] [PubMed]
- Stoeckel, F.; Carter, C.; Lyons, B.A.; Reifler, J. Association of vaccine hesitancy and immunization coverage rates in the European Union. Vaccine 2021, 39, 3935–3939. [Google Scholar] [CrossRef]
- Edelstein, M.; White, J.; Bukasa, A.; Saliba, V.; Ramsay, M.E. Triangulation of measles vaccination data in the United Kingdom of Great Britain and Northern Ireland. Bull. World Health Organ. 2019, 97, 754–763. [Google Scholar] [CrossRef]
- Alfonsi, V.; D’Ancona, F.; Rota, M.C.; Giambi, C.; Ranghiasci, A.; Iannazzo, S. Regional Coordinators for Infectious Diseases and Collective Regional coordinators for infectious diseases and vaccinations Immunisation registers in Italy: A patchwork of computerisation. Eurosurveillance 2012, 17, 20156. [Google Scholar] [CrossRef]
- Crowe, S.; Utley, M.; Walker, G.; Panovska-Griffiths, J.; Grove, P.; Pagel, C. A novel approach to evaluating the UK childhood immunisation schedule: Estimating the effective coverage vector across the entire vaccine programme. BMC Infect. Dis. 2015, 15, 585. [Google Scholar] [CrossRef]
- Trillium II. Available online: https://trillium2.eu/ (accessed on 17 August 2022).
- Glanz, J.M.; Kraus, C.R.; Daley, M.F. Addressing Parental Vaccine Concerns: Engagement, Balance, and Timing. PLoS Biol. 2015, 13, e1002227. [Google Scholar] [CrossRef]
- Trentini, F.; Poletti, P.; Melegaro, A.; Merler, S. The introduction of ‘No jab, No school’ policy and the refinement of measles immunisation strategies in high-income countries. BMC Med. 2019, 17, 86. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Harmon, S.; Dube, E.; Steenbeek, A.; Crowcroft, N.; Opel, D.J.; Faour, D.; Leask, J.; Butler, R. Mandatory infant & childhood immunization: Rationales, issues and knowledge gaps. Vaccine 2018, 36, 5811–5818. [Google Scholar] [CrossRef]
- Charting Mandatory Childhood Vaccination Policies Worldwide|Elsevier Enhanced Reader. Available online: https://reader.elsevier.com/reader/sd/pii/S0264410X21005478?token=0FB3D24C6C236210BCD2D8FEFA34AD340958D56343033E3FECB1AA06EA91056F374A722CE116A4F97484704307341EA7&originRegion=eu-west-1&originCreation=20220110091743 (accessed on 10 January 2022).
- Waight, P.A.; Andrews, N.J.; Ladhani, S.N.; Sheppard, C.L.; Slack, M.P.E.; Miller, E. Effect of the 13-valent pneumococcal conjugate vaccine on invasive pneumococcal disease in England and Wales 4 years after its introduction: An observational cohort study. Lancet Infect. Dis. 2015, 15, 535–543. [Google Scholar] [CrossRef]
- Saeterdal, I.; Lewin, S.; Austvoll-Dahlgren, A.; Glenton, C.; Munabi-Babigumira, S. Interventions aimed at communities to inform and/or educate about early childhood vaccination. Cochrane Database Syst. Rev. 2014, 11, CD010232. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, M.S.; Fiks, A.G. Utilizing health information technology to improve vaccine communication and coverage. Hum. Vaccines Immunother. 2013, 9, 1802–1811. [Google Scholar] [CrossRef] [PubMed]
- Chantler, T.; Karafillakis, E.; Wodajo, S.; Demissie, S.D.; Sile, B.; Mohammed, S.; Olorunsaiye, C.; Landegger, J.; Larson, H.J. ‘We All Work Together to Vaccinate the Child’: A Formative Evaluation of a Community-Engagement Strategy Aimed at Closing the Immunization Gap in North-West Ethiopia. Int. J. Environ. Res. Public Health 2018, 15, 667. [Google Scholar] [CrossRef] [PubMed]
- Vaz, O.M.; Ellingson, M.K.; Weiss, P.; Jenness, S.M.; Bardají, A.; Bednarczyk, R.A.; Omer, S.B. Mandatory Vaccination in Europe. Pediatrics 2020, 145. [Google Scholar] [CrossRef]
- Miron, V.D.; Toma, A.R.; Filimon, C.; Bar, G.; Craiu, M. Optional Vaccines in Children—Knowledge, Attitudes, and Practices in Romanian Parents. Vaccines 2022, 10, 404. [Google Scholar] [CrossRef]
- O’Doherty, K.C.; Crann, S.; Bucci, L.M.; Burgess, M.M.; Chauhan, A.; Goldenberg, M.J.; McMurtry, C.M.; White, J.; Willison, D.J. Deliberation on Childhood Vaccination in Canada: Public Input on Ethical Trade-Offs in Vaccination Policy. AJOB Empir. Bioeth. 2021, 12, 253–265. [Google Scholar] [CrossRef]
- Webster, P.C. Go local, European review of electronic health records advises. Can. Med Assoc. J. 2011, 183, E535–E536. [Google Scholar] [CrossRef]
- Global Diffusion of EHealth: Making Universal Health Coverage Achievable—World Health Organization. Available online: https://books.google.it/books?hl=en&lr=&id=MnOyDwAAQBAJ&oi=fnd&pg=PP4&dq=The+ability+of+various+systems+to+manage+vaccination+coverage+data+at+the+regional+level+varies+greatly%3B+only+six+of+the+15+completely+computerized+regions+can+calculate+vaccine+coverage+automatically&ots=agT3EWjDvj&sig=QBaIRxv6xeDwwIzLNZTPPqdgyGQ&redir_esc=y#v=onepage&q&f=false (accessed on 17 February 2022).
- Marshall, S.; Sahm, L.J.; Moore, A.C. Microneedle technology for immunisation: Perception, acceptability and suitability for paediatric use. Vaccine 2016, 34, 723–734. [Google Scholar] [CrossRef]
- Harvey, H.; Reissland, N.; Mason, J. Parental reminder, recall and educational interventions to improve early childhood immunisation uptake: A systematic review and meta-analysis. Vaccine 2015, 33, 2862–2880. [Google Scholar] [CrossRef]
- Lombardi, N.; Crescioli, G.; Bettiol, A.; Tuccori, M.; Rossi, M.; Bonaiuti, R.; Ravaldi, C.; Levi, M.; Mugelli, A.; Ricci, S.; et al. Vaccines Safety in Children and in General Population: A Pharmacovigilance Study on Adverse Events Following Anti-Infective Vaccination in Italy. Front. Pharmacol. 2019, 10, 948. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, Y.; Wang, Y.; Liang, H. Evaluation of potentially achievable vaccination coverage of the second dose of measles containing vaccine with simultaneous administration and risk factors for missed opportunities among children in Zhejiang province, east China. Hum. Vaccines Immunother. 2017, 14, 875–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syiroj, A.T.R.; Pardosi, J.F.; Heywood, A.E. Exploring parents’ reasons for incomplete childhood immunisation in Indonesia. Vaccine 2019, 37, 6486–6493. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. DTaP5-HB-IPV-Hib Vaccine (Vaxelis®): A Review of its Use in Primary and Booster Vaccination. Pediatr. Drugs 2016, 19, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Bulula, N.; Mwiru, D.P.; Swalehe, O.; Mori, A.T. Vaccine storage and distribution between expanded program on immunization and medical store department in Tanzania: A cost-minimization analysis. Vaccine 2020, 38, 8130–8135. [Google Scholar] [CrossRef]
- Wang, W.; Wang, Y.; Wang, Y.; Yan, F.; Wang, N.; Fu, C. Vaccine bidding, procurement and distribution management practices in mainland China: A nationwide study. Vaccine 2021, 39, 7584–7589. [Google Scholar] [CrossRef]
- Decouttere, C.; Vandaele, N.; De Boeck, K.; Banzimana, S. A Systems-Based Framework for Immunisation System Design: Six Loops, Three Flows, Two Paradigms. Health Syst. 2021, 1–16. [Google Scholar] [CrossRef]
- Danovaro-Holliday, M.C.; Dansereau, E.; Rhoda, D.A.; Brown, D.W.; Cutts, F.T.; Gacic-Dobo, M. Collecting and Using Reliable Vaccination Coverage Survey Estimates: Summary and Recommendations from the “Meeting to Share Lessons Learnt from the Roll-out of the Updated WHO Vaccination Coverage Cluster Survey Reference Manual and to Set an Operational Research Agenda around Vaccination Coverage Surveys” Geneva, 18–21 April 2017. Vaccine 2018, 36, 5150–5159. [Google Scholar] [CrossRef]
- World Health Organization. 2019 Intervention Guidebook Intervention Guidebook for Implementing and Monitoring Activities to Reduce Missed Opportunities for Vaccination; World Health Organization: Geneva, Switzerland, 2019; pp. 1–42. [Google Scholar]
- Cutts, F.T.; Claquin, P.; Danovaro-Holliday, M.C.; Rhoda, D.A. Monitoring vaccination coverage: Defining the role of surveys. Vaccine 2016, 34, 4103–4109. [Google Scholar] [CrossRef]
- Opel, D.J.; Marcuse, E.K. Rethinking vaccine policy making in an era of vaccine hesitancy: Time to rebuild, not remodel? Hum. Vaccines Immunother. 2013, 9, 2672–2673. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Search | Search Terms |
|---|---|
| 1 | “vaccine hesitancy” AND (“European Union” or EU or Europe) AND (child or pediatric or paediatric or kids) |
| 2 | (“primary care” or “primary health care” or “primary healthcare”) AND (“childhood immunization” or vaccine) AND (“developed countries” and “developing countries”) |
| 3 | (“vaccine hesitancy” or “vaccine refusal”) AND (“European Union” or EU or Europe) OR organizational structure in healthcare AND (child or kids or pediatric) |
| 4 | “vaccination coverage” AND (“European Union” or EU or Europe) AND (child or pediatric or paediatric) AND (immune and vaccine) |
| No. of Papers | n = 6 | n = 3 | n = 3 | n = 1 | n = 1 | n = 1 | n = 2 | n = 1 | n = 1 | n = 1 | n = 1 | n = 21 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | UK | EU | Italy | England, Israel, Sweden | Armenia and Kyrgyzstan | Denmark | France | Greece | Norway | Switzerland | Czech Republic | Total |
| Publication year | ||||||||||||
| 2012–2014 | 1 | 1 | 1 | 3 | ||||||||
| 2015–2018 | 3 | 1 | 2 | 1 | 1 | 1 | 9 | |||||
| 2019–2021 | 3 | 2 | 1 | 1 | 1 | 1 | 9 | |||||
| Study Design | ||||||||||||
| Cohort | 4 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | ||||
| Cross-sectional | 1 | 1 | 2 | 1 | 1 | 6 | ||||||
| Qualitative | 1 | 1 | 2 | |||||||||
| Narrative | 1 | 1 | ||||||||||
| Ecological | 1 | 1 | ||||||||||
| Systematic and Meta-analysis | 1 | 1 | ||||||||||
| Quality Assessment | ||||||||||||
| High | 5 | 2 | 3 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 18 | |
| Intermediate | 1 | 1 | 2 | |||||||||
| Satisfactory | 1 | 1 |
| Study Characteristics of Parents’ Engagement and Personalisation Intervention | ||||||
|---|---|---|---|---|---|---|
| Study | Quality | Type of Study | Setting/(Country) | Population/ (Subject) | Intervention/Method | Result/Outcomes |
| Gofen, 2019 | 10/10 | Qualitative Study | Backwords mapping Approach/England Israel and Sweden | Personalizing Immunisation | Two questions guided this study:
| In all three countries, street-level negotiation emerged as a similar three-phase process:
|
| Lwembe, 2021 | 9/10 | Qualitative Study | Celebrate and Protect program/UK | Children under 5 years old | Engaging with parents and carers of children in order to improve the relationships between service users and providers thru data collection from conducting semi-structured telephone interviews or focused group. | Responses from the focus groups (and some providers) indicated that the participants’ perceptions of the celebration cards were more of a reminder than a ‘call to action’. |
| Study Characteristics of Mandatory Immunisation Policy | ||||||
| Study | Quality | Type of Study | Setting /(Country) | Population/ (Subject) | Intervention/Method | Result/Outcomes |
| Gamlund, 2020 | Low quality | Narrative Literature Review | Norway | Arguments against introducing a mandatory childhood vaccination programme | Potential arguments that justify the benefits of mandatory immunization:
| Three arguments justified the potential benefits of mandatory immunisation that outweigh the disadvantages:
|
| Bozzola, 2018 | 7/10 | Cross-sectional study | EU | Mandatory vaccination policies in European Union | Policies of mandatory or recommended vaccinations of the European Countries gathered by ECDC compared to Italian guidelines. |
|
| Levy-Bruhl, 2019 | 8/10 | Cohort study | National Social Security Reimbursement Data/France | Children under 2 years | Assessing the potential consequences of changes on mandated vaccination coverage extension of recommended vaccines thru data collection:
|
|
| Gianfredi, 2019 | 8/10 | Cohort Study | Regional data/Italy | Children 24 months old and younger | Electronically developing data in Microsoft Excel® for VC collection that contains a specific section named “Reasons for no or incomplete vaccination against polio and measles” that includes a list of pre-defined reasons, updated in 2014, which consists of:
|
|
| Martinot, 2021 | 9/10 | Cross-sectional | Implementation of vaccine policy and its effectiveness/ France | 0 to 35 months old | Internet-standardised questionnaire; mothers answered based on opinion on vaccination and vaccinations recorded in their child’s health record. |
|
| Study Characteristics of Vaccination Program Remodeling | ||||||
| Study | Quality | Type of Study | Setting /(Country) | Population/(Subject) | Intervention/Method | Result/Outcomes |
| Crowe, 2015 | 8/10 | Cohort study | A Novel Framework/UK | 2 to 60 months old aged children/developing a modelling framework and estimate the effective coverage against all Vaccination Preventable Diseases within an Immunisation schedule | Estimating the effective coverage against all diseases within a schedule through Modelling Approach. |
|
| Panovska-Griffiths, 2018 | 8/10 | Cohort Study | UK | Transmission Modelling (for four diseases) and historic data synthesis (against the associated disease)/associating vaccination schedule to vaccine preventable disease. |
|
|
| Study Characteristics of Vaccination Procurement and Distribution | ||||||
| Study | Quality | Type of Study | Setting /(Country) | Population/(Subject) | Intervention/Method | Result/Outcomes |
| Hardelid, 2016 | 8/10 | Cohort study | The Health Improvement Network (THIN)/England and Wales | Preschool children aged 2- 4 years old | Encoding and analysing data that contains patients’ information entered into patient electronic records during patient consultation. |
|
| Petras, 2016 | 8/10 | Cohort study | National Surveillance Programme/ Czech Republic | Children under 5 years old/analysis of immunisation coverage and IPD occurrence | Assessing the situation before and after routine immunisation over a two-year period, i.e., 2007–2008 (pre-immunisation period) and 2012– 2013 (post-immunisation period), respectively. |
|
| Grieco, 2020 | 8/10 | Cross-sectional study | Modelling Framework/UK | Epidemiological Model of Influenza to estimate the beneficial mass immunisation |
|
|
| Study Characteristics of Combination/Multiple Vaccine Administration | ||||||
| Study | Quality | Type of Study | Setting/(Country) | Population/ (Subject) | Intervention/Method | Result/Outcomes |
| Pedersen, 2020 | 8/10 | Cohort study | Nationwide register-based study/Denmark | Children 15- missed MMR-1 and DTaP- IPV-Hib-3 doses | Assessing the compliance of the immunisation guidelines and the reasons for non-compliance with a focus on vaccination providers thru semi-structured telephone interviews with vaccination providers. |
|
| Study Characteristics of Improved Immunisation Timing and Intervals | ||||||
| Study | Quality | Type of Study | Setting/(Country) | Population/(Subject) | Intervention/Method | Result/Outcomes |
| Bielicki, 2012 | 8/10 | Cohort study | Switzerland | Timing and timeliness of measles immunisations influence effective population vaccine coverage 0–3 years old |
|
|
| Schweitzer, 2015 | 9/10 | Cohort Study | Demographic and Health Surveys/Armenia and Kyrgyzstan | Children between 12 and 59 months of age for DTP vaccines and between 18 and 59 months assessing the up-to-date vaccination coverage |
|
|
| Study Characteristics of Parental Education and Reminder | ||||||
| Study | Quality | Type of Study | Setting /(Country) | Population/ (Subject) | Intervention/Method | Result/Outcomes |
| Napolitano, 2018 | 9/10 | Cross-sectional study | Italy | Children aged 2 to 6 years | Questionnaires and Parent Attitudes about Childhood Vaccines Survey (PACV) |
|
| Pavlopoulou, 2013 | 8/10 | Cross-sectional study | Greece | 10–65 months old |
|
|
| Study Characteristics of Surveillance Tool and Supplementary Immunisation Activity | ||||||
| Study | Quality | Type of Study | Setting /(Country) | Population/ (Subject) | Intervention/Method | Result/Outcomes |
| Stoeckel, 2021 | 10/16 | Ecological study | European Union | Relationship between vaccine hesitancy scores and uptake rates of DTP3, MCV1, and MCV2. |
|
|
| Edelstein, 2019 | 8/10 | Cohort Study | United Kingdom of Great Britain and Northern Ireland | Children 24 months old and younger | Calculating the proportion of English population susceptible to measles using data from Primary Care and child health records. |
|
| Study Characteristics of Information Technology | ||||||
| Study | Quality | Type of Study | Setting /(Country) | Population/ (Subject) | Intervention/Method | Result/Outcomes |
| Alfonsi, 2012 | 8/10 | Cross- sectional study | Level of computerization of immunization registers /Italy | Incorporating technology in childhood immunization program |
|
|
| Rigby, 2020 | High | Systematic Review and Meta- analyses | European Union | Electronic Health Record |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdecantos, R.L.; Palladino, R.; Lo Vecchio, A.; Montella, E.; Triassi, M.; Nardone, A. Organisational and Structural Drivers of Childhood Immunisation in the European Region: A Systematic Review. Vaccines 2022, 10, 1390. https://doi.org/10.3390/vaccines10091390
Valdecantos RL, Palladino R, Lo Vecchio A, Montella E, Triassi M, Nardone A. Organisational and Structural Drivers of Childhood Immunisation in the European Region: A Systematic Review. Vaccines. 2022; 10(9):1390. https://doi.org/10.3390/vaccines10091390
Chicago/Turabian StyleValdecantos, Ronan Lemwel, Raffaele Palladino, Andrea Lo Vecchio, Emma Montella, Maria Triassi, and Antonio Nardone. 2022. "Organisational and Structural Drivers of Childhood Immunisation in the European Region: A Systematic Review" Vaccines 10, no. 9: 1390. https://doi.org/10.3390/vaccines10091390