
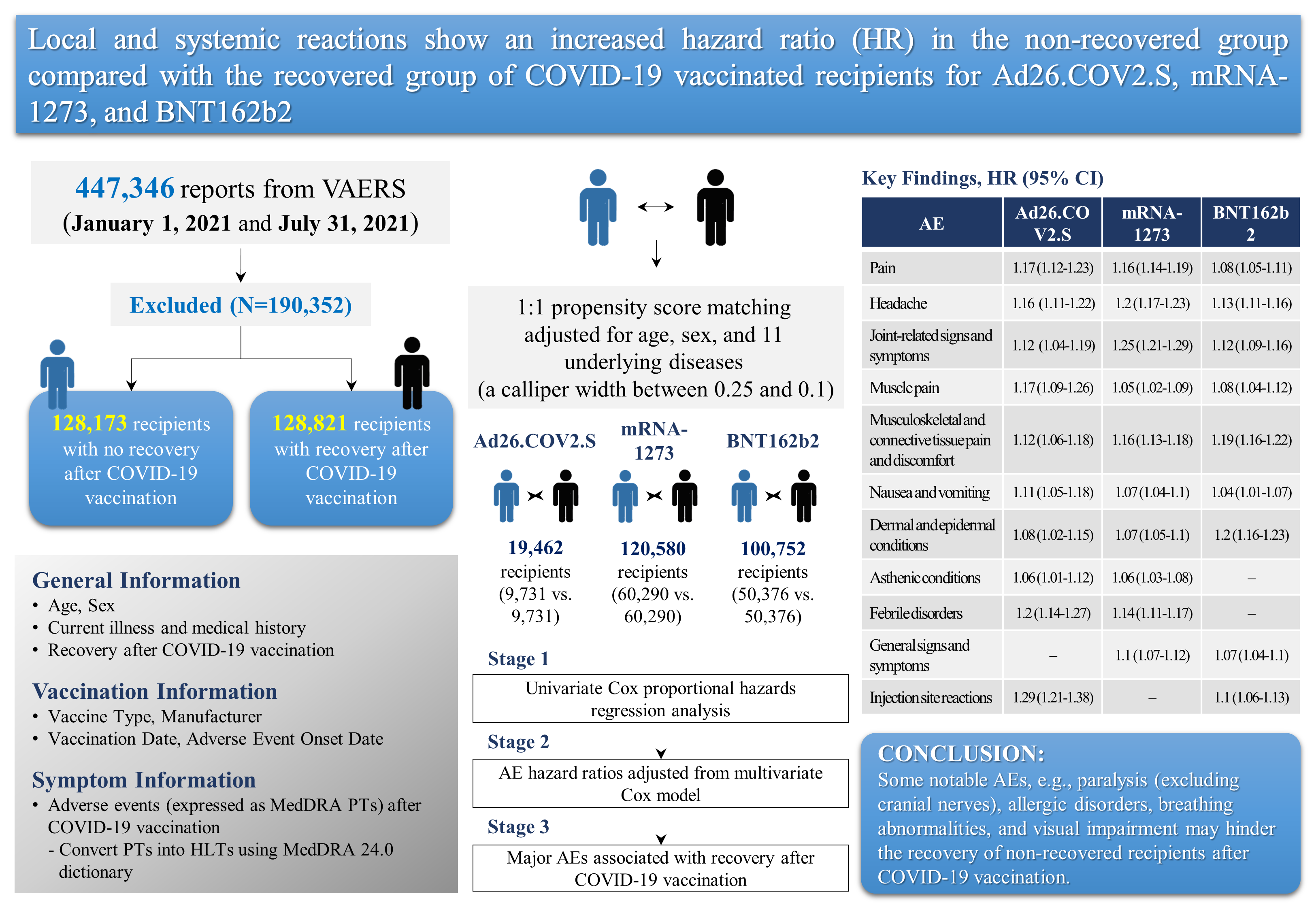
Propensity-Score-Matched Evaluation of Adverse Events Affecting Recovery after COVID-19 Vaccination: On Adenovirus and mRNA Vaccines



Abstract
:
1. Introduction
2. Materials and Methods
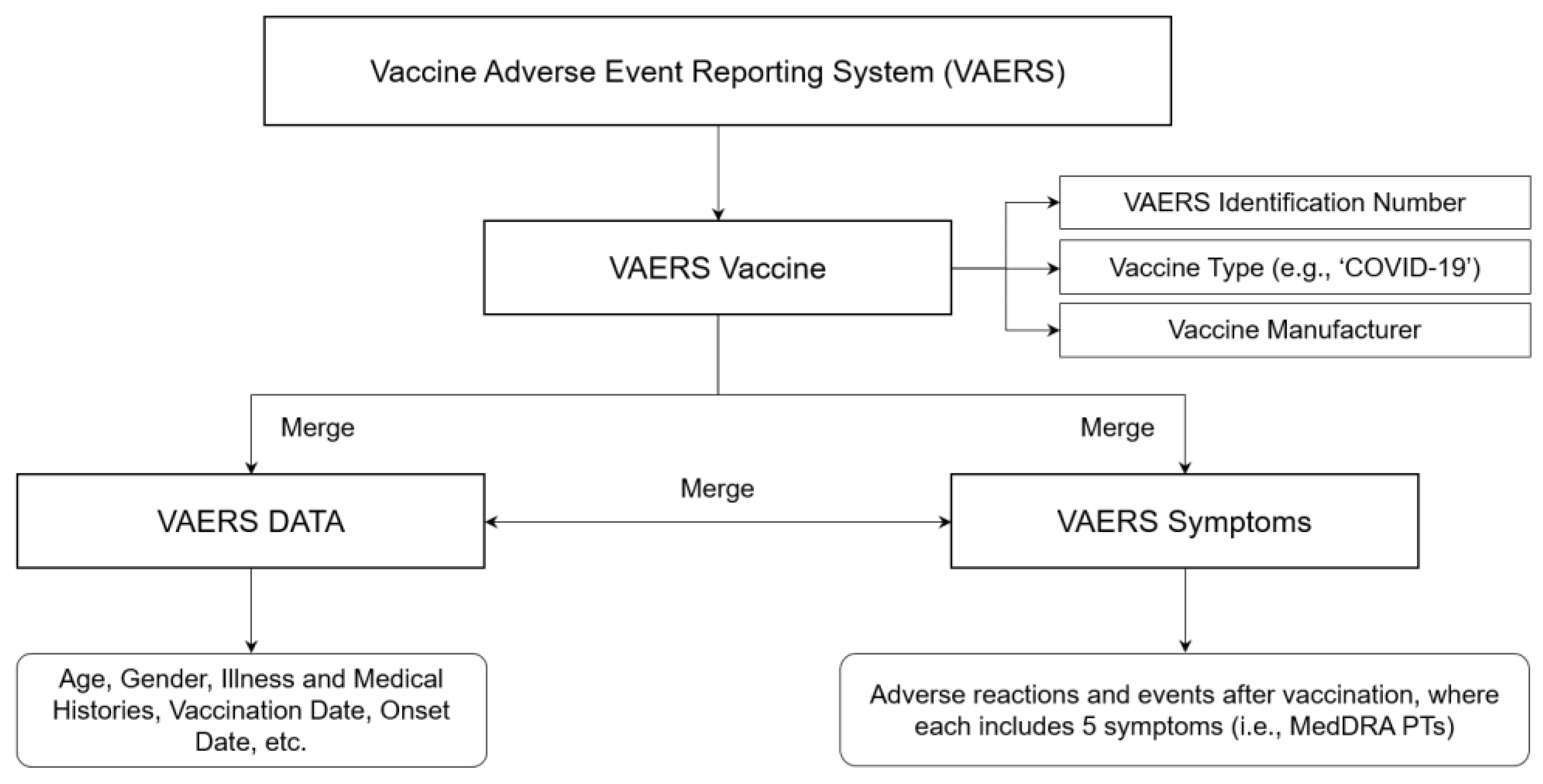
2.1. Data Source and Collection
2.2. Standard Medical Terms for Vaccine Adverse Events
2.3. Underlying Diseases
2.4. Study Design
2.5. Statistical Analysis
2.5.1. Propensity Score Matching
2.5.2. Cox Proportional Hazards Regression Analysis
2.5.3. Experimental Environment and Implementation
3. Results
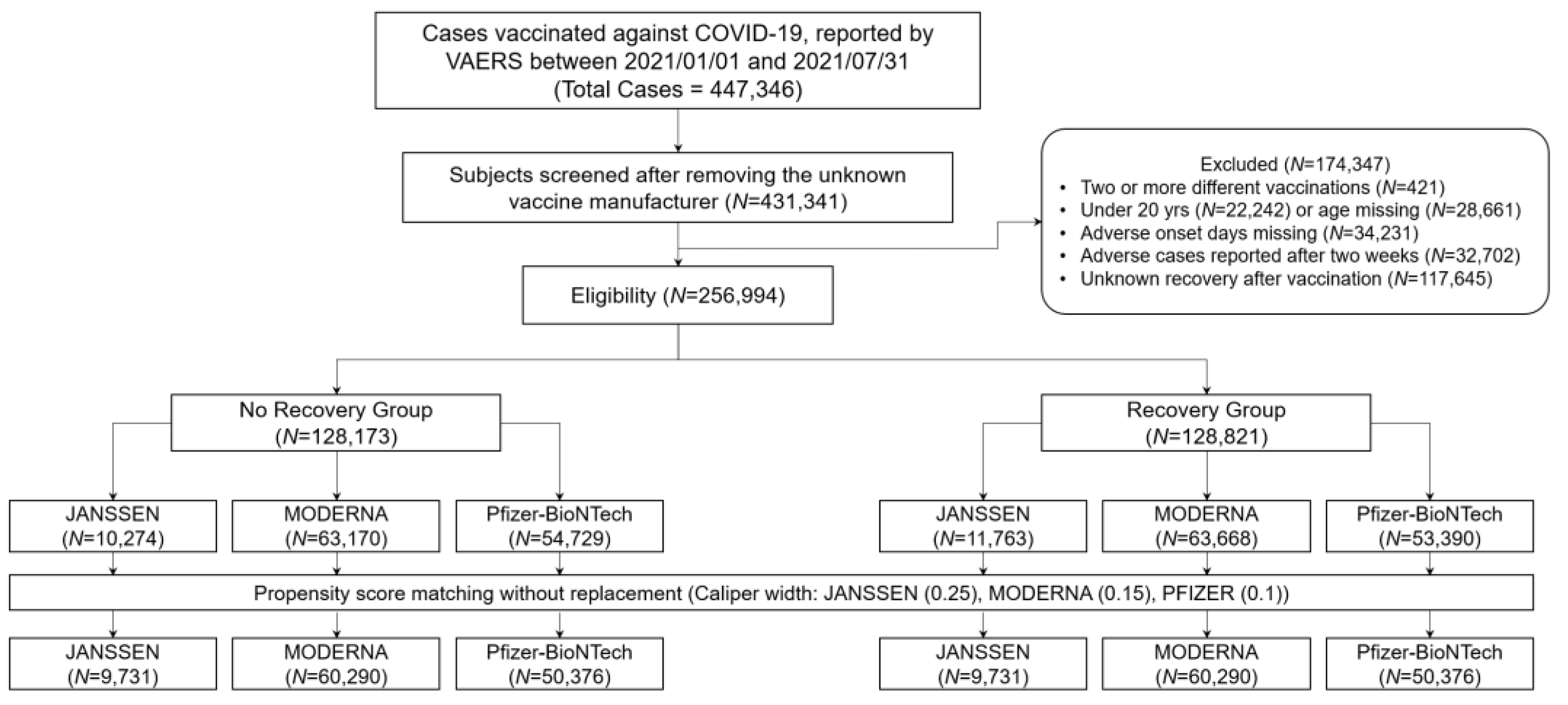
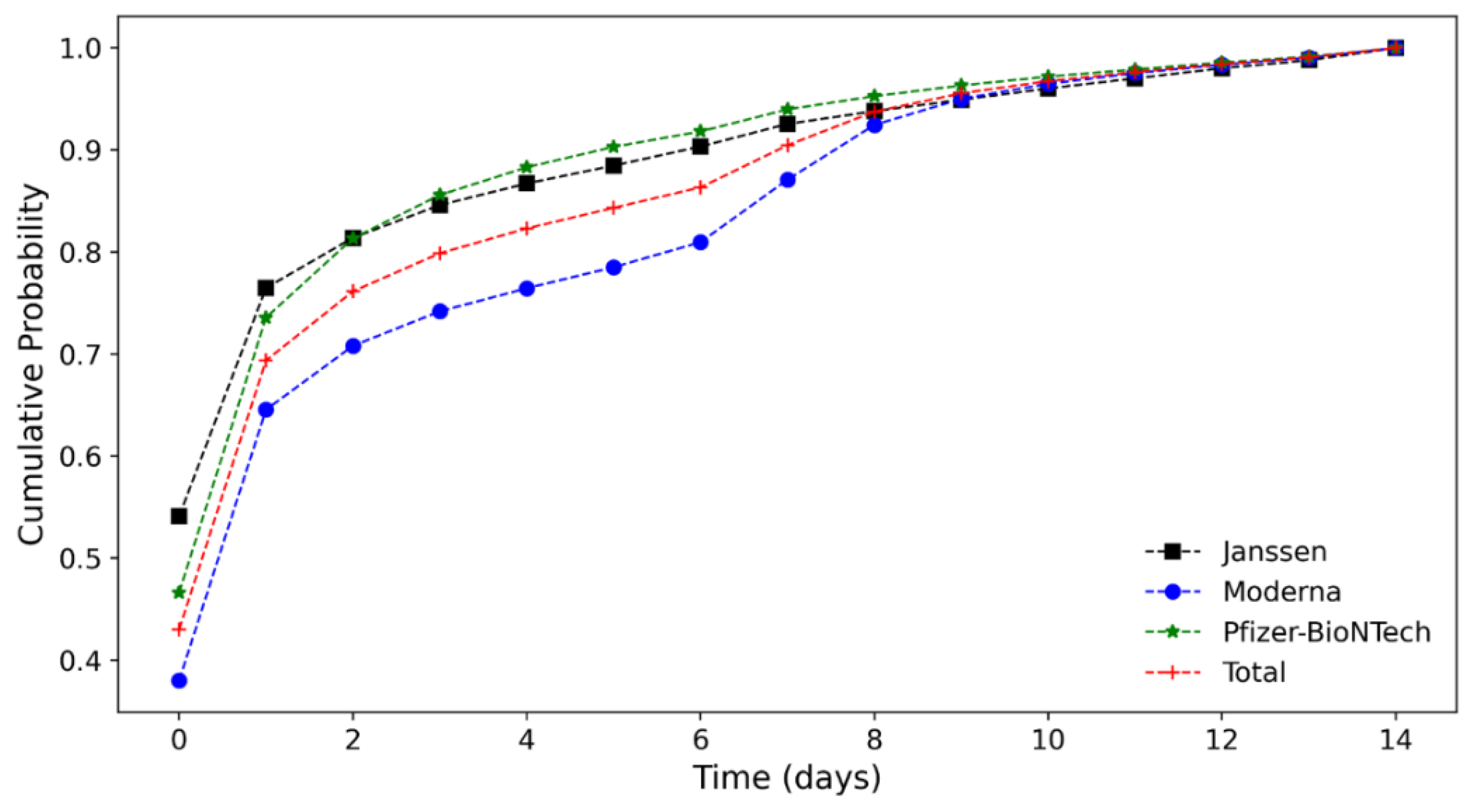
3.1. Data Characteristics
3.2. Major AEs and the Risk Levels Associated with the Three COVID-19 Vaccines
3.2.1. Janssen COVID-19 Vaccine
3.2.2. Moderna COVID-19 Vaccine
3.2.3. Pfizer-BioNTech COVID-19 Vaccine
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, W.; Pan, B.; Sakkiah, S.; Ji, Z.; Yavas, G.; Lu, Y.; Komatsu, T.E.; Lal-Nag, M.; Tong, W.; Patterson, T.A.; et al. Informing selection of drugs for COVID-19 treatment through adverse events analysis. Sci. Rep. 2021, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- FDA Emergency Use Authorization (EUA) of the Pfizer-BioNTech COVID-19 Vaccine to Prevent Coronavirus. Fact Sheet for Healthcare Providers Administering Vaccine. Available online: https://www.fda.gov/media/144413/download (accessed on 9 December 2021).
- FDA Emergency Use Authorization (EUA) of the Moderna COVID-19 Vaccine to Prevent Coronavirus Disease 2019 (COVID-19). Fact Sheet for Healthcare Providers Administering Vaccine. Available online: https://www.fda.gov/media/144637/download?utm_medium=email&utm_source=govdelivery (accessed on 26 October 2021).
- FDA Emergency Use Authorization (EUA) of the Janssen COVID-19 Vaccine to Prevent Coronavirus Disease 2019 (COVID-19). Available online: https://www.fda.gov/media/146304/download (accessed on 26 October 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- FDA Brifing Document Janssen Ad26.COV2.S Vaccine for the Prevention of COVID-19. Available online: https://www.fda.gov/media/146217/download (accessed on 26 October 2021).
- Shimabukuro, T.T.; Cole, M.; Su, J.R. Reports of anaphylaxis after receipt of mRNA COVID-19 vaccines in the US—December 14, 2020-January 18, 2021. JAMA 2021, 325, 1101–1102. [Google Scholar] [CrossRef]
- Gargano, J.W.; Wallace, M.; Hadler, S.C.; Langley, G.; Su, J.R.; Oster, M.E.; Broder, K.R.; Gee, J.; Weintraub, E.; Shimabukuro, T. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: Update from the advisory committee on immunization practices—United States, June 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 977–982. [Google Scholar] [CrossRef]
- See, I.; Su, J.R.; Lale, A.; Woo, E.J.; Guh, A.Y.; Shimabukuro, T.T.; Streiff, M.B.; Rao, A.K.; Wheeler, A.P.; Beavers, S.F. US case reports of cerebral venous sinus thrombosis with thrombocytopenia after Ad26.COV2.S vaccination, March 2 to April 21, 2021. JAMA 2021, 325, 2448–2456. [Google Scholar] [CrossRef]
- Rosenblum, H.G.; Hadler, S.C.; Moulia, D.; Shimabukuro, T.T.; Su, J.R.; Tepper, N.K.; Ess, K.C.; Woo, E.J.; Mba-Jonas, A.; Alimchandani, M. Use of COVID-19 vaccines after reports of adverse events among adult recipients of Janssen (Johnson & Johnson) and mRNA COVID-19 vaccines (Pfizer-BioNTech and Moderna): Update from the advisory committee on immunization practices—United States, July 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1094–1099. [Google Scholar] [CrossRef]
- Cirillo, N. Reported orofacial adverse effects of COVID-19 vaccines: The knowns and the unknowns. J. Oral Pathol. Med. 2021, 50, 424–427. [Google Scholar] [CrossRef]
- FDA Briefing Document Vaccines and Related Biological Products Advisory Committee Meeting. Available online: https://www.fda.gov/media/144434/download (accessed on 26 October 2021).
- Chen, G.; Li, X.; Sun, M.; Zhou, Y.; Yin, M.; Zhao, B.; Li, X. COVID-19 mRNA vaccines are generally safe in the short term: A vaccine vigilance real-world study says. Front. Immunol. 2021, 12, 1843. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Vaccine Safety Datalink. Available online: https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/vsd/index.html (accessed on 27 October 2021).
- Shimabukuro, T.T.; Nguyen, M.; Martin, D.; DeStefano, F. Safety monitoring in the vaccine adverse event reporting system (VAERS). Vaccine 2015, 33, 4398–4405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varricchio, F.; Iskander, J.; Destefano, F.; Ball, R.; Pless, R.; Braun, M.M.; Chen, R.T. Understanding vaccine safety information from the vaccine adverse event reporting system. Pediatr. Infect. Dis. J. 2004, 23, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.T.; Rastogi, S.C.; Mullen, J.R.; Hayes, S.W.; Cochi, S.L.; Donlon, J.A.; Wassilak, S.G. The vaccine adverse event reporting system (VAERS). Vaccine 1994, 12, 542–550. [Google Scholar] [CrossRef]
- Xiong, X.; Yuan, J.; Li, M.; Jiang, B.; Lu, Z.K. Age and gender disparities in adverse events following COVID-19 vaccination: Real-world evidence based on big data for risk management. Front. Med. 2021, 8, 700014. [Google Scholar] [CrossRef] [PubMed]
- Lv, G.; Yuan, J.; Xiong, X.; Li, M. Mortality rate and characteristics of deaths following COVID-19 vaccination. Front. Med. 2021, 8, 670370. [Google Scholar] [CrossRef] [PubMed]
- Kompaniyets, L.; Goodman, A.B.; Belay, B.; Freedman, D.S.; Sucosky, M.S.; Lange, S.J.; Gundlapalli, A.V.; Boehmer, T.K.; Blanck, H.M. Body mass index and risk for COVID-19–related hospitalization, intensive care unit admission, invasive mechanical ventilation, and death—united states, march–december 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 355–361. [Google Scholar] [CrossRef]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in patients younger than 60 years is a risk factor for Covid-19 hospital admission. Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [Green Version]
- Tartof, S.Y.; Qian, L.; Hong, V.; Wei, R.; Nadjafi, R.F.; Fischer, H.; Li, Z.; Shaw, S.F.; Caparosa, S.L.; Nau, C.L. Obesity and mortality among patients diagnosed with COVID-19: Results from an integrated health care organization. Ann. Intern. Med. 2020, 173, 773–781. [Google Scholar] [CrossRef]
- CDC Science Brief: Evidence Used to Update the List of Underlying Medical Conditions That Increase a Person’s Risk of Severe Illness from COVID-19. Available online: http://www.ncbi.nlm.nih.gov/pubmed/34009770 (accessed on 8 September 2021).
- Bowe, B.; Cai, M.; Xie, Y.; Gibson, A.K.; Maddukuri, G.; Al-Aly, Z. Acute kidney injury in a national cohort of hospitalized US veterans with COVID-19. Clin. J. Am. Soc. Nephrol. 2021, 16, 14–25. [Google Scholar] [CrossRef]
- Robbins-Juarez, S.Y.; Qian, L.; King, K.L.; Stevens, J.S.; Husain, S.A.; Radhakrishnan, J.; Mohan, S. Outcomes for patients with COVID-19 and acute kidney injury: A systematic review and meta-analysis. Kidney Int. Rep. 2020, 5, 1149–1160. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q. Patients with cancer appear more vulnerable to SARS-CoV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID-19 Response Team. Allergic reactions including anaphylaxis after receipt of the first dose of Pfizer-BioNTech COVID-19 vaccine—United States, December 14–23, 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team. Allergic reactions including anaphylaxis after receipt of the first dose of Moderna COVID-19 Vaccine—United States, December 21, 2020–January 10, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 125–129. [Google Scholar] [CrossRef]
- Brown, E.G.; Wood, L.; Wood, S. The medical dictionary for regulatory activities (MedDRA). Drug Saf. 1999, 20, 109–117. [Google Scholar] [CrossRef]
- MedDRA What’s New MedDRA Version 24.0. Available online: https://admin.new.meddra.org/sites/default/files/guidance/file/whatsnew_24_0_English.pdf (accessed on 2 September 2021).
- Brown, E.G. Using MedDRA. Drug Saf. 2004, 27, 591–602. [Google Scholar] [CrossRef]
- Fescharek, R.; Kübler, J.; Elsasser, U.; Frank, M.; Güthlein, P. Medical dictionary for regulatory activities (MedDRA). Int. J. Pharm. Med. 2004, 18, 259–269. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Adhikari, S.; Pulgarin, C.; Troxel, A.B.; Iturrate, E.; Johnson, S.B.; Hausvater, A.; Newman, J.D.; Berger, J.S.; Bangalore, S. Renin–angiotensin–aldosterone system inhibitors and risk of COVID-19. N. Engl. J. Med. 2020, 382, 2441–2448. [Google Scholar] [CrossRef]
- Guan, W.; Liang, W.; Zhao, Y.; Liang, H.; Chen, Z.; Li, Y.; Liu, X.; Chen, R.; Tang, C.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [Green Version]
- Baldi, E.; Sechi, G.M.; Mare, C.; Canevari, F.; Brancaglione, A.; Primi, R.; Klersy, C.; Palo, A.; Contri, E.; Ronchi, V. Out-of-hospital cardiac arrest during the Covid-19 outbreak in Italy. N. Engl. J. Med. 2020, 383, 496–498. [Google Scholar] [CrossRef]
- Alvarez-Garcia, J.; Lee, S.; Gupta, A.; Cagliostro, M.; Joshi, A.A.; Rivas-Lasarte, M.; Contreras, J.; Mitter, S.S.; LaRocca, G.; Tlachi, P. Prognostic impact of prior heart failure in patients hospitalized with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2334–2348. [Google Scholar] [CrossRef] [PubMed]
- DeFilippis, E.M.; Reza, N.; Donald, E.; Givertz, M.M.; Lindenfeld, J.; Jessup, M. Considerations for heart failure care during the COVID-19 pandemic. JACC Heart Fail. 2020, 8, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier, E.; Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S.; et al. Pulmonary embolism in patients with COVID-19. Circulation 2020, 142, 184–186. [Google Scholar] [CrossRef]
- Kremer, S.; Lersy, F.; Anheim, M.; Merdji, H.; Schenck, M.; Oesterlé, H.; Bolognini, F.; Messie, J.; Khalil, A.; Gaudemer, A. Neurologic and neuroimaging findings in patients with COVID-19: A retrospective multicenter study. Neurology 2020, 95, e1868–e1882. [Google Scholar] [CrossRef]
- Rosenthal, J.A.; Awan, S.F.; Fintzi, J.; Keswani, A.; Ein, D. Asthma is associated with increased risk of intubation but not hospitalization or death in coronavirus disease 2019. Ann. Allergy Asthma Immunol. 2021, 126, 93–95. [Google Scholar] [CrossRef]
- Yang, J.M.; Koh, H.Y.; Moon, S.Y.; Yoo, I.K.; Ha, E.K.; You, S.; Kim, S.Y.; Yon, D.K.; Lee, S.W. Allergic disorders and susceptibility to and severity of COVID-19: A nationwide cohort study. J. Allergy Clin. Immunol. 2020, 146, 790–798. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Heinze, G.; Schemper, M. A solution to the problem of monotone likelihood in Cox regression. Biometrics 2001, 57, 114–119. [Google Scholar] [CrossRef]
- Chapin-Bardales, J.; Gee, J.; Myers, T. Reactogenicity following receipt of mRNA-based COVID-19 vaccines. JAMA 2021, 325, 2201–2202. [Google Scholar] [CrossRef]
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clark, T.; Markowitz, L. First month of COVID-19 vaccine safety monitoring—United States, December 14, 2020–January 13, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef]
- Sampson, H.A.; Muñoz-Furlong, A.; Campbell, R.L.; Adkinson , N.F., Jr.; Bock, S.A.; Branum, A.; Brown, S.G.A.; Camargo, C.A., Jr.; Cydulka, R.; Galli, S.J. Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J. Allergy Clin. Immunol. 2006, 117, 391–397. [Google Scholar] [CrossRef]
- Muir, K.-L.; Kallam, A.; Koepsell, S.A.; Gundabolu, K. Thrombotic thrombocytopenia after Ad26.COV2.S vaccination. N. Engl. J. Med. 2021, 384, 1964–1965. [Google Scholar] [CrossRef]
- Gessler, F.; Schmitz, A.K.; Dubinski, D.; Bernstock, J.D.; Lehmann, F.; Won, S.-Y.; Wittstock, M.; Güresir, E.; Hadjiathanasiou, A.; Zimmermann, J. Neurosurgical considerations regarding decompressive craniectomy for intracerebral hemorrhage after SARS-CoV-2-vaccination in vaccine induced thrombotic thrombocytopenia—VITT. J. Clin. Med. 2021, 10, 2777. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef]
- European Medicines Agency AstraZeneca’s COVID-19 Vaccine: EMA Finds Possible Link to Very Rare Cases of Unusual Blood Clots with Low Blood Platelets. Available online: https://www.ema.europa.eu/en/news/astrazenecas-covid-19-vaccine-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 18 October 2021).
- Thompson, M.G.; Stenehjem, E.; Grannis, S.; Ball, S.W.; Naleway, A.L.; Ong, T.C.; DeSilva, M.B.; Natarajan, K.; Bozio, C.H.; Lewis, N.; et al. Effectiveness of COVID-19 vaccines in ambulatory and inpatient care settings. N. Engl. J. Med. 2021, 385, 1355–1371. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Ad26.COV2.S | mRNA-1273 | BNT162b2 | Total |
|---|---|---|---|---|
| Total, N (%) | 22,037 (8.57) | 126,838 (49.35) | 108,119 (42.07) | 256,994 |
| Age, mean (SD) | 44.69 ± 15.1 | 51.45 ± 16.76 | 49.4 ± 16.43 | 50.01 ± 16.59 |
| Gender | ||||
| Unknown, N (%) | 34 (0.15) | 225 (0.18) | 459 (0.42) | 718 (0.28) |
| Male, N (%) | 7438 (33.75) | 30,161 (23.78) | 28,681 (26.53) | 66,280 (25.79) |
| Female, N (%) | 14,565 (66.09) | 96,452 (76.04) | 78,979 (73.05) | 189,996 (73.93) |
| Underlying disability | ||||
| Obesity, N (%) | 280 (1.27) | 2027 (1.6) | 1378 (1.27) | 3685 (1.43) |
| Hypertension, N (%) | 1437 (6.52) | 12,148 (9.58) | 7760 (7.18) | 21,345 (8.31) |
| Diabetes, N (%) | 792 (3.59) | 6899 (5.44) | 4288 (3.97) | 11,979 (4.66) |
| Atrial fibrillation, N (%) | 34 (0.15) | 364 (0.29) | 287 (0.27) | 685 (0.27) |
| Heart failure, N (%) | 126 (0.57) | 1073 (0.85) | 676 (0.63) | 1875 (0.73) |
| Kidney disease, N (%) | 78 (0.35) | 782 (0.62) | 524 (0.48) | 1384 (0.54) |
| Pulmonary disease, N (%) | 187 (0.85) | 1396 (1.1) | 798 (0.74) | 2381 (0.93) |
| Asthma, N (%) | 1061 (4.81) | 6580 (5.19) | 4880 (4.51) | 12,521 (4.87) |
| Stroke, N (%) | 36 (0.16) | 285 (0.22) | 234 (0.22) | 555 (0.22) |
| Cancers, N (%) | 200 (0.91) | 1768 (1.39) | 1221 (1.13) | 3189 (1.24) |
| Allergies, N (%) | 559 (2.54) | 3256 (2.57) | 2557 (2.36) | 6372 (2.48) |
| Recovery | ||||
| Yes, N (%) | 11,763 (53.38) | 63,668 (50.2) | 53,390 (49.38) | 128,821 (50.13) |
| No, N (%) | 10,274 (46.62) | 63,170 (49.8) | 54,729 (50.62) | 128,173 (49.87) |
| AE onset interval (days), mean (SD *) | 1.67 ± 3.1 | 2.51 ± 3.43 | 1.64 ± 2.8 | 2.07 ± 3.18 |
| SOC | HLT | Non-Recovered Group | HR (95% CI) | |
|---|---|---|---|---|
| Total (%) | N (%) | |||
| Cardiac disorders | Ischaemic coronary artery disorders | 654 (6.72) | 654 (6.72) | 1.18 (1.09–1.29) |
| Eye disorders | Ocular disorders NEC | 193 (1.98) | 193 (1.98) | 1.16 (1.01–1.35) |
| Gastrointestinal disorders | Gastrointestinal and abdominal pains (except oral and throat) | 1964 (20.18) | 512 (5.26) | 1.11 (1.02–1.22) |
| Nausea and vomiting symptoms | 1858 (19.09) | 1.11 (1.05–1.18) | ||
| General disorders and administration site conditions | Asthenic conditions | 2827 (29.05) | 2881 (29.61) | 1.06 (1.01–1.12) |
| Febrile disorders | 2524 (25.94) | 1.2 (1.14–1.27) | ||
| Injection site reactions | 1090 (11.2) | 1.29 (1.21–1.38) | ||
| Pain and discomfort NEC | 2540 (26.1) | 1.17 (1.12–1.23) | ||
| Hepatobiliary disorders | Cholecystitis and cholelithiasis | 7 (0.07) | 7 (0.07) | 2.6 (1.21–5.63) |
| Immune system disorders | Allergic conditions NEC | 207 (2.13) | 207 (2.13) | 1.27 (1.1–1.46) |
| Musculoskeletal and connective tissue disorders | Joint-related signs and symptoms | 2307 (23.71) | 1022 (10.5) | 1.12 (1.04–1.19) |
| Muscle pains | 1006 (10.34) | 1.17 (1.09–1.26) | ||
| Musculoskeletal and connective tissue pain and discomfort | 1934 (19.87) | 1.12 (1.06–1.18) | ||
| Nervous system disorders | Auditory nerve disorders | 3769 (38.73) | 393 (4.04) | 1.41 (1.27–1.57) |
| Headaches NEC | 3526 (36.23) | 1.16 (1.11–1.22) | ||
| Sensory abnormalities NEC | 335 (3.44) | 1.22 (1.09–1.36) | ||
| Psychiatric disorders | Cognitive and attention disorders and disturbances NEC | 314 (3.23) | 117 (1.2) | 1.21 (1.01–1.46) |
| Disturbances in initiating and maintaining sleep | 207 (2.13) | 1.19 (1.03–1.37) | ||
| Respiratory, thoracic, and mediastinal disorders | Coughing and associated symptoms | 367 (3.77) | 314 (3.23) | 1.17 (1.03–1.32) |
| Pharyngeal disorders (except infections and neoplasms) | 67 (0.69) | 1.34 (1.05–1.72) | ||
| Skin and subcutaneous tissue disorders | Dermal and epidermal conditions NEC | 1485 (15.26) | 1264 (12.99) | 1.08 (1.02–1.15) |
| Erythemas | 417 (4.29) | 1.12 (1.01–1.24) | ||
| SOC | HLT | Non-Recovered Group | HR (95% CI) | |
|---|---|---|---|---|
| Total (%) | N (%) | |||
| Blood and lymphatic system disorders | Lymphatic system disorders NEC | 2943 (4.88) | 2943 (4.88) | 1.15 (1.11–1.2) |
| Cardiac disorders | Cardiac signs and symptoms NEC | 6622 (10.98) | 5455 (9.05) | 1.07 (1.04–1.1) |
| Ischaemic coronary artery disorders | 2016 (3.34) | 1.06 (1.01–1.11) | ||
| Left ventricular failures | 84 (0.14) | 1.39 (1.11–1.73) | ||
| Ventricular arrhythmias and cardiac arrest | 252 (0.42) | 1.15 (1–1.31) | ||
| Ear and labyrinth disorders | Ear disorders NEC | 743 (1.23) | 743 (1.23) | 1.1 (1.02–1.19) |
| Endocrine disorders | Hypoglycaemic conditions NEC | 12 (0.02) | 12 (0.02) | 2.13 (1.21–3.73) |
| Eye disorders | Conjunctival infections, irritations, and inflammations | 1093 (1.81) | 30 (0.05) | 1.46 (1.02–2.1) |
| Lacrimation disorders | 170 (0.28) | 1.22 (1.04–1.42) | ||
| Ocular disorders NEC | 654 (1.08) | 1.14 (1.05–1.24) | ||
| Ocular infections, inflammations, and associated manifestations | 347 (0.58) | 1.16 (1.04–1.29) | ||
| Visual impairment and blindness (except colour blindness) | 285 (0.47) | 1.13 (1–1.27) | ||
| Gastrointestinal disorders | Diarrhoea (except infective) | 8291 (13.75) | 2049 (3.4) | 1.05 (1–1.1) |
| Gastrointestinal and abdominal pains (except oral and throat) | 1127 (1.87) | 1.07 (1–1.14) | ||
| Gastrointestinal disorders NEC | 66 (0.11) | 1.29 (1.01–1.65) | ||
| Nausea and vomiting symptoms | 7059 (11.71) | 1.07 (1.04–1.1) | ||
| Oral soft tissue disorders NEC | 76 (0.13) | 1.3 (1.03–1.63) | ||
| Oral soft tissue signs and symptoms | 2022 (3.35) | 1.15 (1.09–1.2) | ||
| Oral soft tissue swelling and oedema | 10 (0.02) | 2.28 (1.23–4.23) | ||
| Stomatitis and ulceration | 183 (0.3) | 1.24 (1.06–1.44) | ||
| Tongue signs and symptoms | 203 (0.34) | 1.21 (1.05–1.39) | ||
| General disorders and administration site conditions | Asthenic conditions | 16,454 (27.29) | 12,452 (20.65) | 1.06 (1.03–1.08) |
| Death and sudden death | 1179 (1.96) | 1.57 (1.47–1.67) | ||
| Febrile disorders | 9564 (15.86) | 1.14 (1.11–1.17) | ||
| General signs and symptoms NEC | 9468 (15.7) | 1.1 (1.07–1.12) | ||
| Pain and discomfort NEC | 11,624 (19.28) | 1.16 (1.14–1.19) | ||
| Hepatobiliary disorders | Hepatobiliary signs and symptoms | 15 (0.02) | 15 (0.02) | 1.86 (1.11–3.11) |
| Immune system disorders | Allergic conditions NEC | 2035 (3.38) | 751 (1.25) | 1.25 (1.16–1.34) |
| Angio-oedemas | 1364 (2.26) | 1.1 (1.04–1.16) | ||
| Infections and infestations | Clostridia infections | 13 (0.02) | 13 (0.02) | 3.47 (2.02–5.94) |
| Injury, poisoning and procedural complications | Chest and respiratory tract injuries NEC | 96 (0.16) | 8 (0.01) | 2.42 (1.21–4.85) |
| Muscle, tendon, and ligament injuries | 88 (0.15) | 1.32 (1.07–1.63) | ||
| Investigations | Gastrointestinal histopathology procedures | 264 (0.44) | 9 (0.01) | 1.98 (1.04–3.79) |
| Musculoskeletal and soft tissue imaging procedures | 255 (0.42) | 1.23 (1.08–1.4) | ||
| Metabolism and nutrition disorders | Fluid intake decreased | 18 (0.03) | 18 (0.03) | 1.83 (1.14–2.94) |
| Musculoskeletal and connective tissue disorders | Bursal disorders | 11,522 (19.11) | 49 (0.08) | 1.65 (1.25–2.2) |
| Joint-related disorders NEC | 121 (0.2) | 1.56 (1.31–1.87) | ||
| Joint-related signs and symptoms | 5216 (8.65) | 1.25 (1.21–1.29) | ||
| Muscle pains | 3721 (6.17) | 1.05 (1.02–1.09) | ||
| Musculoskeletal and connective tissue conditions NEC | 844 (1.40) | 1.08 (1.01–1.16) | ||
| Musculoskeletal and connective tissue pain and discomfort | 9701 (16.09) | 1.16 (1.13–1.18) | ||
| Skull and face fractures | 7 (0.01) | 2.45 (1.14–5.28) | ||
| Soft tissue disorders NEC | 171 (0.28) | 1.24 (1.07–1.44) | ||
| Nervous system disorders | Auditory nerve disorders | 14,617 (24.24) | 2110 (3.5) | 1.49 (1.42–1.56) |
| Dementia (except Alzheimer’s type) | 23 (0.04) | 1.86 (1.22–2.83) | ||
| Headaches NEC | 11,704 (19.41) | 1.2 (1.17–1.23) | ||
| Neurologic visual problems NEC | 722 (1.2) | 1.15 (1.06–1.24) | ||
| Neuromuscular disorders NEC | 695 (1.15) | 1.17 (1.08–1.26) | ||
| Paraesthesia and dysesthesias | 908 (1.51) | 1.22 (1.15–1.31) | ||
| Paralysis and paresis (except cranial nerve) | 200 (0.33) | 1.17 (1.02–1.35) | ||
| Sensory abnormalities NEC | 1277 (2.12) | 1.2 (1.13–1.27) | ||
| Psychiatric disorders | Cognitive and attention disorders and disturbances NEC | 2483 (4.12) | 418 (0.69) | 1.29 (1.16–1.42) |
| Confusion and disorientation | 579 (0.96) | 1.15 (1.06–1.25) | ||
| Disturbances in initiating and maintaining sleep | 632 (1.05) | 1.24 (1.14–1.34) | ||
| Sleep disorders NEC | 1168 (1.94) | 1.19 (1.12–1.26) | ||
| Reproductive system and breast disorders | Erection and ejaculation conditions and disorders | 15 (0.02) | 15 (0.02) | 2.2 (1.32–3.67) |
| Respiratory, thoracic, and mediastinal disorders | Breathing abnormalities | 3293 (5.46) | 2595 (4.3) | 1.1 (1.06–1.15) |
| Coughing and associated symptoms | 1344 (2.23) | 1.22 (1.15–1.29) | ||
| Skin and subcutaneous tissue disorders | Dermal and epidermal conditions NEC | 7289 (12.09) | 7289 (12.09) | 1.07 (1.05–1.1) |
| Social circumstances | Disability issues | 1335 (2.21) | 1335 (2.21) | 1.08 (1.02–1.14) |
| Vascular disorders | Bruising, ecchymosis, and purpura | 1724 (2.86) | 934 (1.55) | 1.17 (1.1–1.25) |
| Cerebrovascular and spinal vascular disorders NEC | 810 (1.34) | 1.14 (1.06–1.23) | ||
| SOC | HLT | Non-Recovered Group | HR (95% CI) | |
|---|---|---|---|---|
| Total (%) | N (%) | |||
| Blood and lymphatic system disorders | Lymphatic system disorders NEC | 3735 (7.41) | 3735 (7.41) | 1.25 (1.21–1.29) |
| Cardiac disorders | Heart failure signs and symptoms | 3108 (6.17) | 204 (0.4) | 1.2 (1.04–1.38) |
| Ischaemic coronary artery disorders | 2745 (5.45) | 1.05 (1.01–1.1) | ||
| Ventricular arrhythmias and cardiac arrest | 287 (0.57) | 1.34 (1.18–1.52) | ||
| Endocrine disorders | Diabetic complications neurological | 14 (0.03) | 14 (0.03) | 1.73 (1.02–2.92) |
| Eye disorders | Choroid and vitreous haemorrhages and vascular disorders | 897 (1.78) | 6 (0.01) | 3.37 (1.48–7.7) |
| Ocular disorders NEC | 891 (1.77) | 1.13 (1.05–1.21) | ||
| Gastrointestinal disorders | Flatulence, bloating, and distension | 9051 (17.97) | 269 (0.53) | 1.13 (1–1.28) |
| Gastrointestinal and abdominal pains (except oral and throat) | 1505 (2.99) | 1.11 (1.05–1.17) | ||
| Gastrointestinal disorders NEC | 99 (0.2) | 1.3 (1.07–1.59) | ||
| Gastrointestinal dyskinetic disorders | 35 (0.07) | 1.54 (1.1–2.15) | ||
| Nausea and vomiting symptoms | 6933 (13.76) | 1.04 (1.01–1.07) | ||
| Oral soft tissue signs and symptoms | 2635 (5.23) | 1.1 (1.06–1.15) | ||
| Tongue signs and symptoms | 251 (0.5) | 1.14 (1–1.29) | ||
| General disorders and administration site conditions | Death and sudden death | 16,022 (31.8) | 848 (1.68) | 1.39 (1.3–1.5) |
| Feelings and sensations NEC | 3245 (6.44) | 1.08 (1.04–1.12) | ||
| Gait disturbances | 930 (1.85) | 1.07 (1–1.15) | ||
| General signs and symptoms NEC | 6709 (13.32) | 1.07 (1.04–1.1) | ||
| Injection site reactions | 4516 (8.96) | 1.1 (1.06–1.13) | ||
| Pain and discomfort NEC | 9810 (19.47) | 1.08 (1.05–1.11) | ||
| Vaccination site reactions | 1628 (3.23) | 1.88 (1.79–1.98) | ||
| Immune system disorders | Allergic conditions NEC | 716 (1.42) | 716 (1.42) | 1.3 (1.21–1.4) |
| Infections and infestations | Cardiac infections | 6 (0.01) | 6 (0.01) | 2.72 (1.2–6.14) |
| Injury, poisoning and procedural complications | Medication errors, product use errors and issues NEC | 491 (0.97) | 110 (0.22) | 1.51 (1.17–1.95) |
| Off label uses | 134 (0.27) | 2.16 (1.71–2.74) | ||
| Overdoses NEC | 14 (0.03) | 1.84 (1.08–3.11) | ||
| Product administration errors and issues | 507 (1.01) | 1.26 (1.15–1.38) | ||
| Radiation injuries | 15 (0.03) | 1.67 (1–2.76) | ||
| Investigations | Heart rate and pulse investigations | 3858 (7.66) | 1458 (2.89) | 1.1 (1.04–1.17) |
| Physical examination procedures and organ system status | 2411 (4.79) | 1.13 (1.09–1.18) | ||
| Vascular tests NEC (include blood pressure) | 850 (1.69) | 1.1 (1.02–1.18) | ||
| Musculoskeletal and connective tissue disorders | Joint-related disorders NEC | 9847 (19.55) | 102 (0.2) | 1.26 (1.03–1.53) |
| Joint-related signs and symptoms | 5150 (10.22) | 1.12 (1.09–1.16) | ||
| Muscle pains | 3822 (7.59) | 1.08 (1.04–1.12) | ||
| Musculoskeletal and connective tissue conditions NEC | 842 (1.67) | 1.09 (1.02–1.17) | ||
| Musculoskeletal and connective tissue pain and discomfort | 8048 (15.98) | 1.19 (1.16–1.22) | ||
| Nervous system disorders | Auditory nerve disorders | 15,176 (30.13) | 2701 (5.36) | 1.34 (1.29–1.4) |
| Dementia (except Alzheimer’s type) | 13 (0.03) | 2.13 (1.23–3.67) | ||
| Headaches NEC | 11,537 (22.9) | 1.13 (1.11–1.16) | ||
| Neurologic visual problems NEC | 917 (1.82) | 1.08 (1.01–1.15) | ||
| Neuromuscular disorders NEC | 806 (1.6) | 1.08 (1–1.16) | ||
| Paraesthesia and dysesthesias | 981 (1.95) | 1.1 (1.03–1.17) | ||
| Peripheral neuropathies NEC | 205 (0.41) | 1.21 (1.05–1.39) | ||
| Sensory abnormalities NEC | 1671 (3.32) | 1.18 (1.12–1.24) | ||
| Psychiatric disorders | Cognitive and attention disorders and disturbances NEC | 1490 (2.96) | 478 (0.95) | 1.16 (1.05–1.27) |
| Communications disorders | 79 (0.16) | 1.27 (1.01–1.58) | ||
| Disturbances in initiating and maintaining sleep | 792 (1.57) | 1.17 (1.08–1.25) | ||
| Emotional and mood disturbances NEC | 283 (0.56) | 1.13 (1–1.28) | ||
| Parasomnias | 53 (0.11) | 1.34 (1.02–1.76) | ||
| Respiratory, thoracic, and mediastinal disorders | Breathing abnormalities | 3346 (6.64) | 3097 (6.15) | 1.12 (1.08–1.17) |
| Pharyngeal disorders (except infections and neoplasms) | 419 (0.83) | 1.22 (1.1–1.34) | ||
| Skin and subcutaneous tissue disorders | Dermal and epidermal conditions NEC | 7584 (15.05) | 5694 (11.3) | 1.2 (1.16–1.23) |
| Pruritus NEC | 2898 (5.75) | 1.07 (1.03–1.12) | ||
| Vascular disorders | Cerebrovascular and spinal vascular disorders NEC | 917 (1.82) | 917 (1.82) | 1.1 (1.03–1.17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, C.-S.; Jin, S.-H.; Kang, W.-S. Propensity-Score-Matched Evaluation of Adverse Events Affecting Recovery after COVID-19 Vaccination: On Adenovirus and mRNA Vaccines. Vaccines 2022, 10, 284. https://doi.org/10.3390/vaccines10020284
Son C-S, Jin S-H, Kang W-S. Propensity-Score-Matched Evaluation of Adverse Events Affecting Recovery after COVID-19 Vaccination: On Adenovirus and mRNA Vaccines. Vaccines. 2022; 10(2):284. https://doi.org/10.3390/vaccines10020284
Chicago/Turabian StyleSon, Chang-Sik, Sang-Hyeon Jin, and Won-Seok Kang. 2022. "Propensity-Score-Matched Evaluation of Adverse Events Affecting Recovery after COVID-19 Vaccination: On Adenovirus and mRNA Vaccines" Vaccines 10, no. 2: 284. https://doi.org/10.3390/vaccines10020284