
Antibody Response of Combination of BNT162b2 and CoronaVac Platforms of COVID-19 Vaccines against Omicron Variant

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
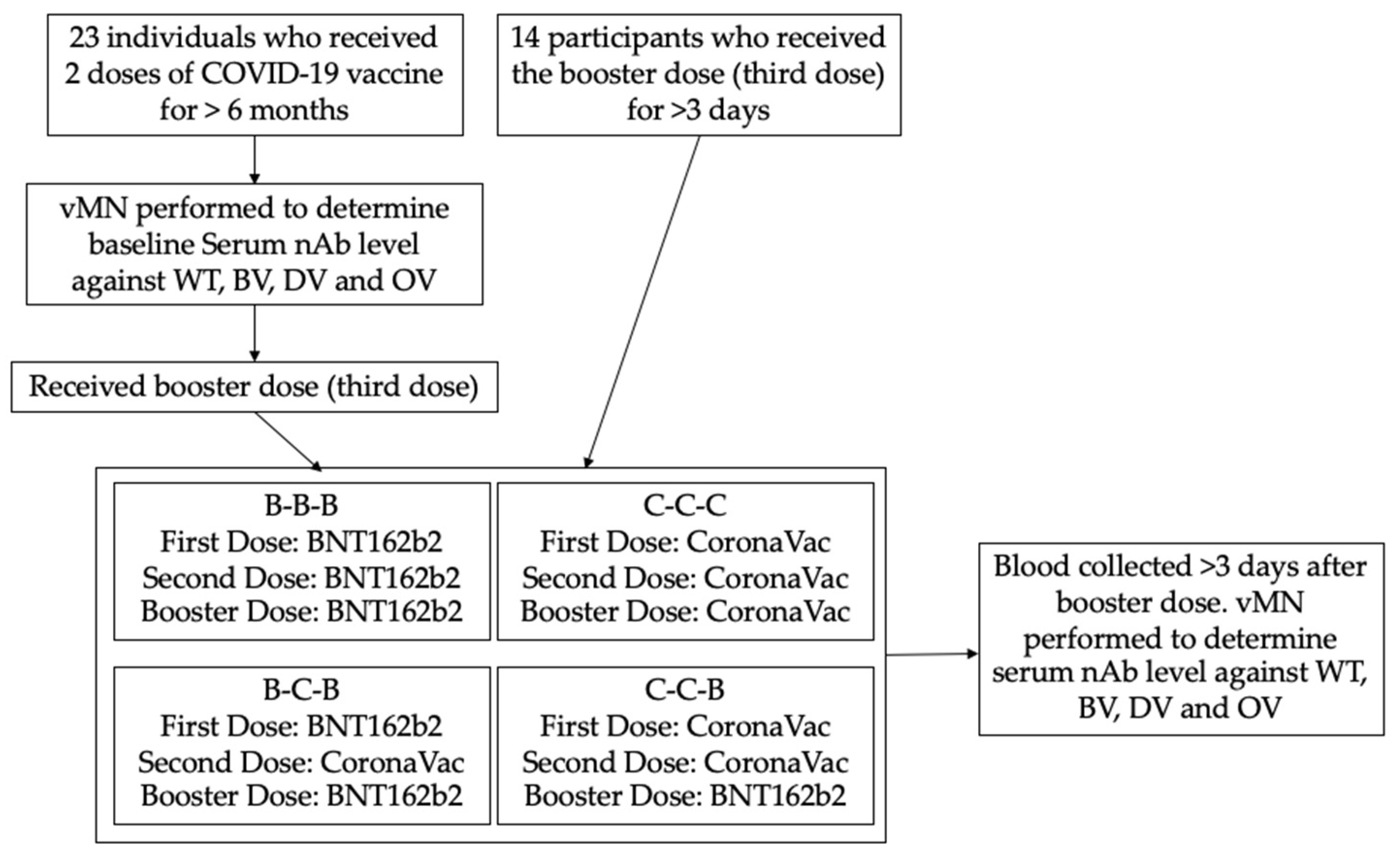
2.1. Study Design and Participants
2.2. Procedure
2.3. Outcome
2.4. Statistical Analysis
3. Results
3.1. Subjects
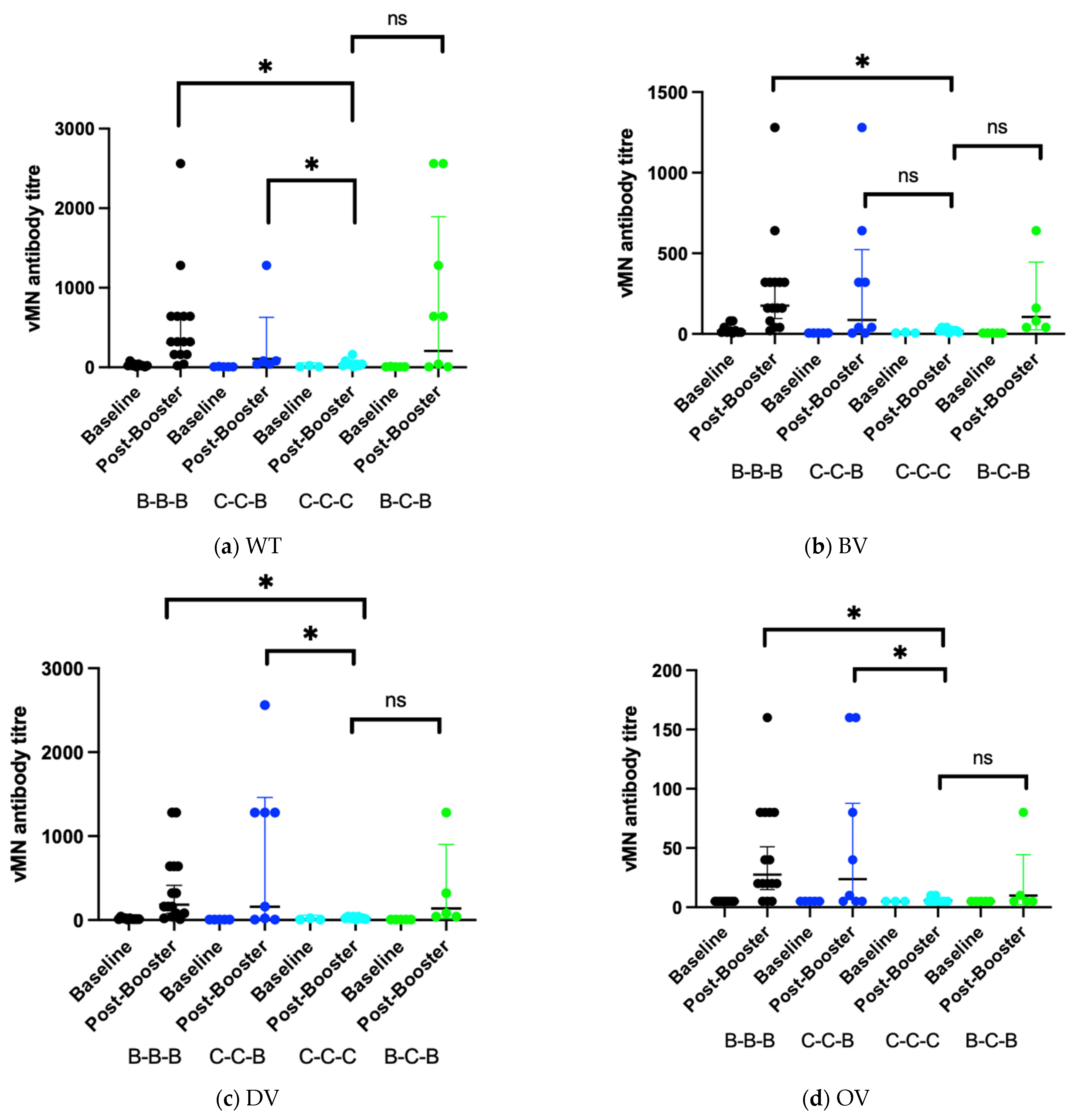
3.2. Immunogenicity of Different Vaccine Combinations
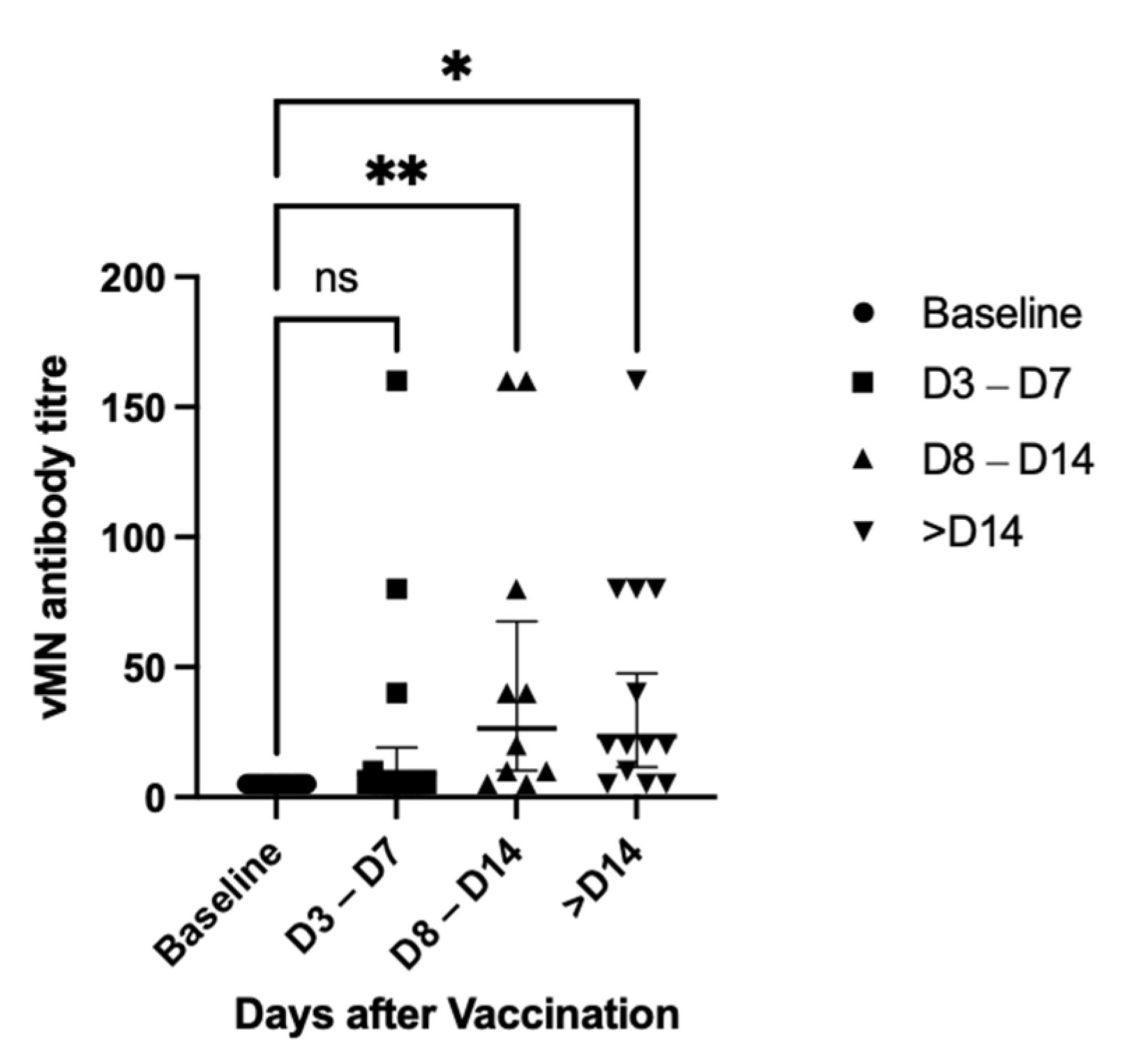
3.3. Changes in GMT against OV Level after Booster Dose
3.4. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Baseline (n = 23) | Day 3–Day 7 (N = 14) | Day 8–Day 14 (n = 10) | Day 14 or After (n = 13) | p-Value | |
|---|---|---|---|---|---|
| Age (Years) | 53 (22–70) | 49.5 (22–64) | 57.5 (24–70) | 64 (31–76) | 0.045 |
| Sex | 0.513 | ||||
| Male | 9 (39.1%) | 5 (35.7%) | 4 (40%) | 8 (61.5%) | |
| Female | 14 (60.9%) | 9 (64.3%) | 6 (60%) | 5 (38.5%) | |
| Comorbidities | 5 (21.7%) | 4 (28.6%) | 3 (30%) | 6 (46.2%) | 0.498 |
References
- Walsh, E.E.; Frenck, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Richmond, P.; Hatchuel, L.; Dong, M.; Ma, B.; Hu, B.; Smolenov, I.; Li, P.; Liang, P.; Han, H.H.; Liang, J.; et al. Safety and immunogenicity of S-Trimer (SCB-2019), a protein subunit vaccine candidate for COVID-19 in healthy adults: A phase 1, randomised, double-blind, placebo-controlled trial. Lancet 2021, 397, 682–694. [Google Scholar] [CrossRef]
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.W. Omicron (B.1.1.529): Infectivity, vaccine breakthrough, and antibody resistance. arXiv 2021, arXiv:2112.01318v1. [Google Scholar] [CrossRef]
- Lu, L.; Mok, B.W.; Chen, L.L.; Chan, J.M.; Tsang, O.T.; Lam, B.H.; Chuang, V.W.; Chu, A.W.; Chan, W.M.; Ip, J.D.; et al. Neutralization of SARS-CoV-2 Omicron variant by sera from BNT162b2 or Coronavac vaccine recipients. Clin. Infect. Dis. 2021, ciab1041. [Google Scholar] [CrossRef]
- He, Q.; Mao, Q.; An, C.; Zhang, J.; Gao, F.; Bian, L.; Li, C.; Liang, Z.; Xu, M.; Wang, J. Heterologous prime-boost: Breaking the protective immune response bottleneck of COVID-19 vaccine candidates. Emerg. Microbes Infect. 2021, 10, 629–637. [Google Scholar] [CrossRef]
- Li, Y.; Bi, Y.; Xiao, H.; Yao, Y.; Liu, X.; Hu, Z.; Duan, J.; Yang, Y.; Li, Z.; Li, Y.; et al. A novel DNA and protein combination COVID-19 vaccine formulation provides full protection against SARS-CoV-2 in rhesus macaques. Emerg. Microbes Infect. 2021, 10, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Gao, Q.; Bao, L.; Mao, H.; Wang, L.; Xu, K.; Yang, M.; Li, Y.; Zhu, L.; Wang, N.; Lv, Z.; et al. Development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020, 369, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Leung, K.Y.; Zhang, R.R.; Liu, D.; Fan, Y.; Chen, H.; Yuen, K.Y.; Hung, I.F. Performance of a Surrogate SARS-CoV-2-Neutralizing Antibody Assay in Natural Infection and Vaccination Samples. Diagnostics 2021, 11, 1757. [Google Scholar] [CrossRef]
- Chu, H.; Chan, J.F.; Yuen, T.T.; Shuai, H.; Yuan, S.; Wang, Y.; Hu, B.; Yip, C.C.; Tsang, J.O.; Huang, X.; et al. Comparative tropism, replication kinetics, and cell damage profiling of SARS-CoV-2 and SARS-CoV with implications for clinical manifestations, transmissibility, and laboratory studies of COVID-19: An observational study. Lancet Microbe 2020, 1, e14–e23. [Google Scholar] [CrossRef]
- Chen, L.L.; Lu, L.; Choi, C.Y.; Cai, J.P.; Tsoi, H.W.; Chu, A.W.; Ip, J.D.; Chan, W.M.; Zhang, R.R.; Zhang, X.; et al. Impact of SARS-CoV-2 variant-associated RBD mutations on the susceptibility to serum antibodies elicited by COVID-19 infection or vaccination. Clin. Infect. Dis. 2021, ciab656. [Google Scholar] [CrossRef]
- Li, X. Omicron: Call for updated vaccines. J. Med. Virol. 2021. [Google Scholar] [CrossRef]
- Khan, N.A.; Al-Thani, H.; El-Menyar, A. The emergence of new SARS-CoV-2 variant (Omicron) and increasing calls for COVID-19 vaccine boosters-The debate continues. Travel Med. Infect. Dis. 2021, 45, 102246. [Google Scholar] [CrossRef]
- Lu, S. Heterologous prime-boost vaccination. Curr. Opin. Immunol. 2009, 21, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Sapkota, B.; Saud, B.; Shrestha, R.; Al-Fahad, D.; Sah, R.; Shrestha, S.; Rodriguez-Morales, A.J. Heterologous prime-boost strategies for COVID-19 vaccines. J. Travel Med. 2021, taab191. [Google Scholar] [CrossRef] [PubMed]
- Ai, J.; Zhang, H.; Zhang, Y.; Lin, K.; Zhang, Y.; Wu, J.; Wan, Y.; Huang, Y.; Song, J.; Fu, Z.; et al. Omicron variant showed lower neutralizing sensitivity than other SARS-CoV-2 variants to immune sera elicited by vaccines after boost. Emerg. Microbes Infect. 2021, 1–24. [Google Scholar] [CrossRef]
- Zhang, R.; Khong, K.-W.; Leung, K.-Y.; Liu, D.; Fan, Y.; Lu, L.; Chan, P.-C.; Chen, L.; To, K.K.-W.; Chen, H.; et al. Antibody Response of BNT162b2 and CoronaVac Platforms in Recovered Individuals Previously Infected by COVID-19 against SARS-CoV-2 Wild Type and Delta Variant. Vaccines 2021, 9, 1442. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Muik, A.; Vogler, I.; Derhovanessian, E.; Kranz, L.M.; Vormehr, M.; Quandt, J.; Bidmon, N.; Ulges, A.; Baum, A.; et al. BNT162b2 induces SARS-CoV-2-neutralising antibodies and T cells in humans. Nature 2021, 595, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.W.; Mak, L.; Leung, G.M.; Cowling, B.J.; Peiris, M. Comparative immunogenicity of mRNA and inactivated vaccines against COVID-19. Lancet Microbe 2021, 2, e423. [Google Scholar] [CrossRef]
- Chang, X.; Augusto, G.S.; Liu, X.; Kündig, T.M.; Vogel, M.; Mohsen, M.O.; Bachmann, M.F. BNT162b2 mRNA COVID-19 vaccine induces antibodies of broader cross-reactivity than natural infection, but recognition of mutant viruses is up to 10-fold reduced. Allergy 2021, 76, 2895–2998. [Google Scholar] [CrossRef] [PubMed]



| B-B-B (n = 15) | B-C-B (n = 5) | C-C-C (n = 9) | C-C-B (n = 8) | p-Value | |
|---|---|---|---|---|---|
| Age (Years) | 53 (26–76) | 47 (22–58) | 58 (31–64) | 58.5 (27–70) | 0.54 |
| Sex | 0.888 | ||||
| Male | 7 (46.7%) | 2 (40%) | 5 (55.6%) | 3 (37.5%) | |
| Female | 8 (53.3%) | 3 (60%) | 4 (44.4%) | 5 (62.5%) | |
| Comorbidities | 4 (26.7%) | 1 (20%) | 5 (55.6%) | 2 (25%) | 0.395 |
| Date Post-3rd Dose (Days) | 14 (3–39) | 5 (5–7) | 14 (5–32) | 8 (4–29) | 0.2443 |
| B-B-B (n = 15) | B-C-B (n = 5) | C-C-C (n = 9) | C-C-B (n = 8) | p-Value | |
|---|---|---|---|---|---|
| WT | |||||
| Baseline GMT 1 | 20 (10.8–37.1) 2 | 5.74 (3.91–8.44) | 7.94 (1.09–58) 3 | 5.74 (3.91–8.44) 4 | 0.046 |
| Post-Booster GMT | 306 (154–608) | 106 (17.7–629) | 34.3 (16.3–72.1) | 207 (22.7–1893) | 0.058 |
| GMT fold increase | 15.3 (7.14–32.7) 5 | 18.4 (2.84–119) | 4.32 (1.99–9.37) 5 | 36.1 (4.21–310) 5 | 0.012 |
| BV | |||||
| Baseline GMT | 18.7 (9.46–36.8) 2 | 5 (5–5) | 6.3 (2.33–17) 3 | 5 (5–5) 4 | 0.086 |
| Post-Booster GMT | 175 (95–324) | 106 (25–446) | 18.5 (11.3–30.4) | 87.2 (14.5–523) | 0.148 |
| GMT fold increase | 9.4 (5.77–15.3) 5 | 21.1 (5–89.1) | 2.94 (1.84–4.7) 5 | 17.4 (2.91–105) 5 | 0.026 |
| DV | |||||
| Baseline GMT | 13.2 (8.69–20) 2 | 5 (5–5) | 7.94 (1.09–58) 3 | 5 (5–5) 4 | 0.044 |
| Post-Booster GMT | 184 (81.7–413) | 139 (21.9–900) | 20 (11.7–34.1) | 160 (17.5–1461) | 0.041 |
| GMT fold increase | 13.9 (5.75–33.7) 5 | 27.9 (4.31–180) | 2.52 (1.36–4.66) 5 | 32 (3.5–292) 5 | 0.011 |
| OV | |||||
| Baseline GMT | 5 (5–5) 2 | 5 (5–5) | 5 (5–5) 3 | 5 (5–5) 4 | - |
| Post-Booster GMT | 27.6 (15–51) | 10 (2.25–44.4) | 5.83 (4.61–7.38) | 23.8 (6.45–87.7) | 0.077 |
| GMT fold increase | 5.53 (2.99–10.2) 5 | 2 (0.45–8.88) | 1.17 (0.992–1.42) 5 | 4.76 (1.29–17.5) 5 | 0.077 |
| B-B-B (n = 15) | C-C-B (n = 6) | C-C-C (n = 9) | B-C-B (n = 5) | p-Value | |
|---|---|---|---|---|---|
| Fever | 0 (0%) | 1 (16.7%) | 0 (0%) | 0 (0%) | 0.174 |
| Chills | 0 (0%) | 1 (16.7%) | 0 (0%) | 1 (20%) | 0.196 |
| Headache | 2 (13.3%) | 3 (50%) | 0 (0%) | 2 (40%) | 0.063 |
| Tiredness | 6 (40%) | 3 (50%) | 4 (44.4%) | 1 (20%) | 0.763 |
| Nausea | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Vomiting | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Diarrhea | 0 (0%) | 0 (0%) | 0 (0%) | 1 (20%) | 0.103 |
| Muscle Pain | 4 (26.7%) | 2 (33.3%) | 2 (22.2%) | 2 (40%) | 0.899 |
| Joint Pain | 2 (13.3%) | 2 (33.3%) | 2 (22.2%) | 0 (0%) | 0.483 |
| Facial Dropping | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Skin Rash | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| SAE 1 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Injection Site Reaction | |||||
| Pain | 12 (80%) | 5 (83.3%) | 7 (77.8%) | 5 (100%) | 0.733 |
| Redness | 1 (6.67%) | 1 (16.7%) | 0 (0%) | 1 (20%) | 0.523 |
| Swelling | 3 (20%) | 1 (16.7%) | 0 (0%) | 1 (20%) | 0.560 |
| Ecchymoses | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Itching | 2 (13.3%) | 1 (16.7%) | 0 (0%) | 3 (60%) | 0.037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khong, K.-W.; Liu, D.; Leung, K.-Y.; Lu, L.; Lam, H.-Y.; Chen, L.; Chan, P.-C.; Lam, H.-M.; Xie, X.; Zhang, R.; et al. Antibody Response of Combination of BNT162b2 and CoronaVac Platforms of COVID-19 Vaccines against Omicron Variant. Vaccines 2022, 10, 160. https://doi.org/10.3390/vaccines10020160
Khong K-W, Liu D, Leung K-Y, Lu L, Lam H-Y, Chen L, Chan P-C, Lam H-M, Xie X, Zhang R, et al. Antibody Response of Combination of BNT162b2 and CoronaVac Platforms of COVID-19 Vaccines against Omicron Variant. Vaccines. 2022; 10(2):160. https://doi.org/10.3390/vaccines10020160
Chicago/Turabian StyleKhong, Ka-Wa, Danlei Liu, Ka-Yi Leung, Lu Lu, Hoi-Yan Lam, Linlei Chen, Pui-Chun Chan, Ho-Ming Lam, Xiaochun Xie, Ruiqi Zhang, and et al. 2022. "Antibody Response of Combination of BNT162b2 and CoronaVac Platforms of COVID-19 Vaccines against Omicron Variant" Vaccines 10, no. 2: 160. https://doi.org/10.3390/vaccines10020160