
“Maternal Vaccination Greatly Depends on Your Trust in the Healthcare System”: A Qualitative Study on the Acceptability of Maternal Vaccines among Pregnant Women and Healthcare Workers in Barcelona, Spain


 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. Participants’ Characteristics
3.2. General Perceptions of Vaccines
“I’m always afraid that there is some risk, to be honest (…) I know that during pregnancy, you can’t even take ibuprofen (…) So, it seems extreme to me that suddenly they vaccinate you, they put many more things in your body than they usually advise. (…) I said yes when they explained it to me, as I see that it is something that has been experimented with for a long time and many pregnant women do it”.105-01 (Pregnant woman)
3.3. Decision-Making Factors for Vaccination during Pregnancy
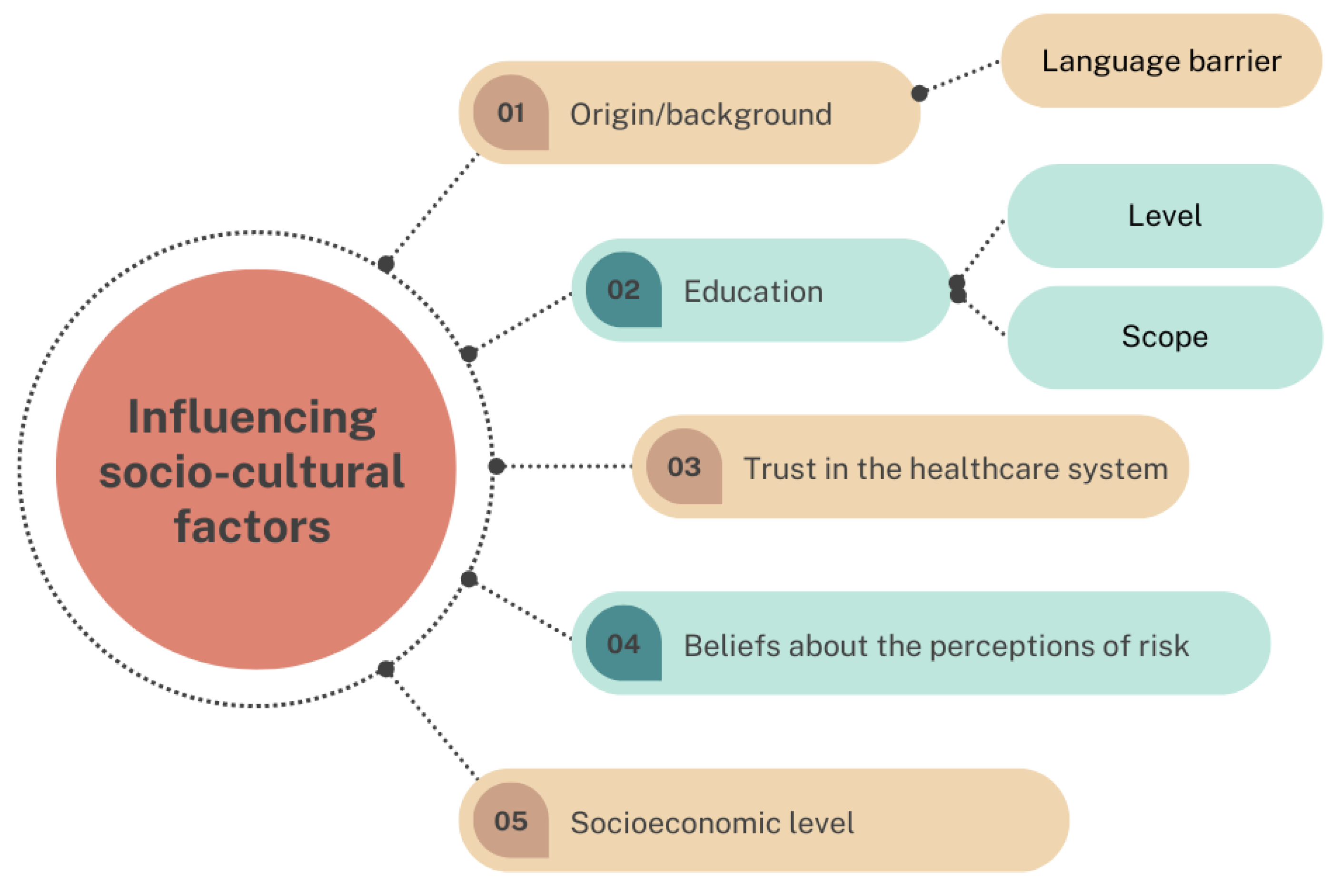
3.3.1. Factors Influencing Decision-Making Regarding Maternal Vaccinations
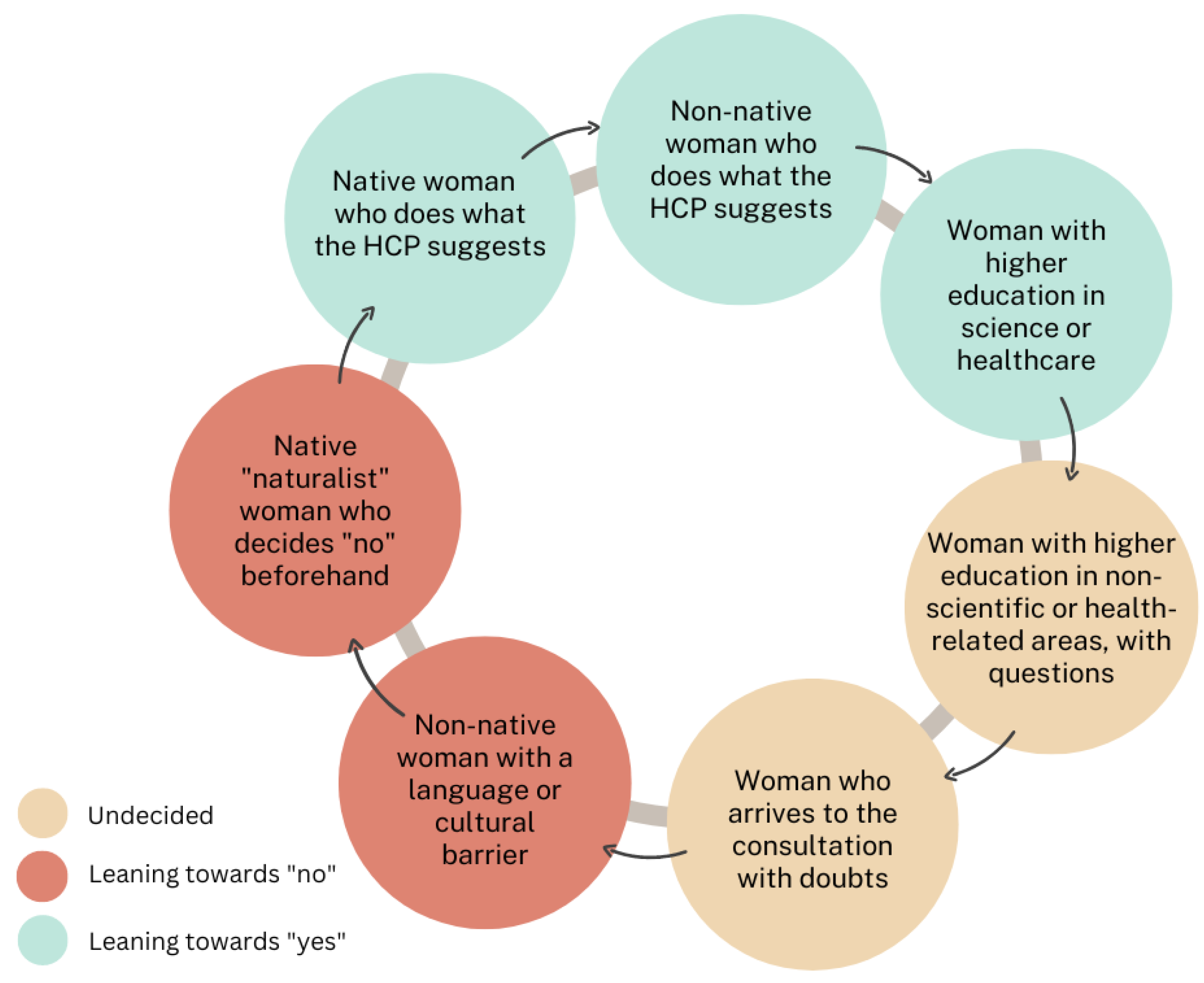
3.3.2. Healthcare Professionals’ Perceptions of Pregnant Women’s Decisions to Be Vaccinated
3.3.3. Vaccines: Opinions, Credibility and Trust
3.4. COVID-19 Vaccination in Pregnancy
3.4.1. Recommendation of the COVID-19 Vaccine
3.4.2. Perceptions of the Role of Health Authorities
3.4.3. Sources of Information and the Influence of the Media
3.5. Clinical Trials during Pregnancy and Motives to Participate or Not
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuciel, N.; Mazurek, J.; Hap, K.; Marciniak, D.; Biernat, K.; Sutkowska, E. COVID-19 Vaccine Acceptance in Pregnant and Lactating Women and Mothers of Young Children in Poland. Int. J. Womens. Health 2022, 14, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Adeyanju, G.C.; Engel, E.; Koch, L.; Ranzinger, T.; Shahid, I.B.M.; Head, M.G.; Eitze, S.; Betsch, C. Determinants of influenza vaccine hesitancy among pregnant women in Europe: A systematic review. Eur. J. Med. Res. 2021, 26, 116. [Google Scholar] [CrossRef]
- Ryan, M.; Marlow, L.A.V.; Forster, A. Countering Vaccine Hesitancy among Pregnant Women in England: The Case of Boostrix-IPV. Int. J. Environ. Res. Public Health 2020, 17, 4984. [Google Scholar] [CrossRef]
- World Health Organization. Maternal Immunization and Antenatal Care Situation Analysis (MIACSA) Project Results Dissemination Meeting; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Tailoring Immunization Programmes for Seasonal Influenza (TIP FLU)—A Guide for Increasing Pregnant Women’s Uptake of Seasonal Influenza Vaccination; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Abu Raya, B.; Edwards, K.M.; Scheifele, D.W.; Halperin, S.A. Pertussis and influenza immunisation during pregnancy: A landscape review. Lancet. Infect. Dis. 2017, 17, e209–e222. [Google Scholar] [CrossRef]
- Håberg, S.E.; Trogstad, L.; Gunnes, N.; Wilcox, A.J.; Gjessing, H.K.; Samuelsen, S.O.; Skrondal, A.; Cappelen, I.; Engeland, A.; Aavitsland, P.; et al. Risk of Fetal Death after Pandemic Influenza Virus Infection or Vaccination. N. Engl. J. Med. 2013, 368, 333–340. [Google Scholar] [CrossRef] [Green Version]
- Coberturas de Vacunación Frente a Gripe en ≥65 años, en ≥75 años, Personas de Personas de 65–74 años, Personas de Per-sonas de 60–64 Años, Embarazadas y Personal Sanitario. 2020. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/calendario-y-coberturas/coberturas/docs/Tabla13.pdf (accessed on 24 January 2022).
- Mott, K.; Huybrechts, K.F.; Glynn, R.J.; Mogun, H.; Hernández-Díaz, S. Tetanus, Diphtheria, Acellular Pertussis Vaccination During Pregnancy and Risk of Pertussis in the Newborn in Publicly and Privately Insured Mother-infant Pairs in the United States. Pediatr. Infect. Dis. J. 2021, 40, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Saso, A.; Kampmann, B. Maternal Immunization: Nature Meets Nurture. Front. Microbiol. 2020, 11, 1499. [Google Scholar] [CrossRef]
- ECDC. Pertussis Annual Epidemiological Report for 2018 Key Facts; Annual Epidemiological Report for 2018; European Centre for Disease Prevention and Control: Solna, Sweden, 2020. [Google Scholar]
- Olsen, S.J.; Azziz-Baumgartner, E.; Budd, A.P.; Brammer, L.; Sullivan, S.; Pineda, R.F.; Cohen, C.; Fry, A.M. Decreased Influenza Activity During the COVID-19 Pandemic–United States, Australia, Chile, and South Africa, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1305–1309. [Google Scholar] [CrossRef] [PubMed]
- Isabel Fernández-Cano, M.; Arreciado Marañón, A.; Reyes-Lacalle, A.; Feijoo-Cid, M.; Maria Manresa-Domínguez, J.; Montero-Pons, L.; Maria Cabedo-Ferreiro, R.; Toran-Monserrat, P.; Falguera-Puig, G.; Nord, M.; et al. Influenza and Pertussis Maternal Vaccination Coverage and Influencing Factors in Spain: A Study Based on Primary Care Records Registry. Int. J. Environ. Res. Public Heal. 2022, 19, 4391. [Google Scholar] [CrossRef]
- Arreciado Marañón, A.; Fernández-Cano, M.I.; Montero-Pons, L.; Feijoo-Cid, M.; Reyes-Lacalle, A.; Cabedo-Ferreiro, R.M.; Manresa-Domínguez, J.M.; Falguera-Puig, G. Knowledge, Perceptions, Attitudes and Practices of Midwives Regarding Maternal Influenza and Pertussis Vaccination: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 8391. [Google Scholar] [CrossRef]
- Update on WHO Interim Recommendations on COVID-19 Vaccination of Pregnant and Lactating Women. Available online: https://www.who.int/publications/m/item/update-on-who-interim-recommendations-on-covid-19-vaccination-of-pregnant-and-lactating-women (accessed on 24 January 2022).
- Ceulemans, M.; Foulon, V.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Cleary, B.; O’shaughnessy, F.; Passier, A.; Richardson, J.L.; et al. Vaccine Willingness and Impact of the COVID-19 Pandemic on Women’s Perinatal Experiences and Practices—A Multinational, Cross-Sectional Study Covering the First Wave of the Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3367. [Google Scholar] [CrossRef] [PubMed]
- Dashraath, P.; Nielsen-Saines, K.; Madhi, S.A.; Baud, D. COVID-19 vaccines and neglected pregnancy. Lancet 2020, 396, e22. [Google Scholar] [CrossRef]
- Bardají, A.; Sevene, E.; Cutland, C.; Menéndez, C.; Omer, S.B.; Aguado, T.; Muñoz, F.M. The need for a global COVID-19 maternal immunisation research plan. Lancet 2021, 397, e17–e18. [Google Scholar] [CrossRef]
- Goncu Ayhan, S.; Oluklu, D.; Atalay, A.; Menekse Beser, D.; Tanacan, A.; Moraloglu Tekin, O.; Sahin, D. COVID-19 vaccine acceptance in pregnant women. Int. J. Gynaecol. Obstet. 2021, 154, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Marbán-Castro, E.; Pons-Duran, C.; García-Otero, L.; Chen, H.; Herrera, L.B.; Del Mar Gil, M.; Goncé, A.; Ferriols-Pérez, E.; Rodríguez, M.Á.; Toro, P.; et al. Acceptability of clinical trials on COVID-19 during pregnancy among pregnant women and healthcare providers: A qualitative study. Int. J. Environ. Res. Public Health 2021, 18, 10717. [Google Scholar] [CrossRef]
- Garg, I.; Shekhar, R.; Sheikh, A.B.; Pal, S. COVID-19 Vaccine in Pregnant and Lactating Women: A Review of Existing Evidence and Practice Guidelines. Infect. Dis. Rep. 2021, 13, 685–699. [Google Scholar] [CrossRef]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Sociology Press: Mill Valley, CA, USA, 1967. [Google Scholar]
- Thyer, B. The Handbook of Social Work Research Methods; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2010. [Google Scholar]
- Bowen, G.A. Naturalistic inquiry and the saturation concept: A research note. Qual. Res. 2008, 8, 137–152. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Palma, D.; Hernández, A.; Picchio, C.A.; Jodar, G.; Galbany-Estragués, P.; Simón, P.; Guillaumes, M.; Diez, E.; Rius, C. Confidence in a Vaccine against COVID-19 among Registered Nurses in Barcelona, Spain across Two Time Periods. Vaccines 2022, 10, 873. [Google Scholar] [CrossRef]
- Ekmez, M.; Ekmez, F. Assessment of factors affecting attitudes and knowledge of pregnant women about COVID-19 vaccination. J. Obstet. Gynaecol. 2022, 42, 1984–1990. [Google Scholar] [CrossRef]
- Huang, L.; Riggan, K.A.; Ashby, G.B.; Rivera-Chiauzzi, E.Y.; Allyse, M.A. Pregnant and Postpartum Patients’ Views of COVID-19 Vaccination. J. Community Health 2022, 47, 871–878. [Google Scholar] [CrossRef]
- Kiefer, M.K.; Mehl, R.; Costantine, M.M.; Johnson, A.; Cohen, J.; Summerfield, T.L.; Landon, M.B.; Rood, K.M.; Venkatesh, K.K. Characteristics and perceptions associated with COVID-19 vaccination hesitancy among pregnant and postpartum individuals: A cross-sectional study. BJOG 2022, 129, 1342–1351. [Google Scholar] [CrossRef]
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; Le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 vaccination during pregnancy: Coverage and safety. Am. J. Obstet. Gynecol. 2022, 226, 236.e1–236.e14. [Google Scholar] [CrossRef]
- Sutanto, M.Y.; Hosek, M.G.; Stumpff, S.K.; Neuhoff, B.K.; Hernandez, B.S.; Wang, Z.; Ramsey, P.S.; Boyd, A.R. Sociodemographic predictors of COVID-19 vaccine hesitancy and leading concerns with COVID-19 vaccines among pregnant women at a South Texas clinic. J. Matern. Fetal. Neonatal Med. 2022, 4, 1–7. [Google Scholar] [CrossRef]
- Cavaliere, A.F.; Zaami, S.; Pallottini, M.; Perelli, F.; Vidiri, A.; Marinelli, E.; Straface, G.; Signore, F.; Scambia, G.; Marchi, L. Flu and Tdap Maternal Immunization Hesitancy in Times of COVID-19: An Italian Survey on Multiethnic Sample. Vaccines 2021, 9, 1107. [Google Scholar] [CrossRef]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Vergallo, G.M.; Del Rio, A.; Negro, F.; Zaami, S. COVID-19 vaccine mandates: What are the current European public perspectives? Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 643–652. [Google Scholar] [CrossRef]
- Marbán-Castro, E.; Nedic, I.; Ferrari, M.; Crespo-Mirasol, E.; Ferrer, L.; Noya, B.; Marin, A.; Fumadó, V.; López, M.; Menéndez, C.; et al. Perceptions of COVID-19 Maternal Vaccination among Pregnant Women and Healthcare Workers and Factors That Influence Vaccine Acceptance: A Cross-Sectional Study in Barcelona, Spain. Vaccines 2022, 10, 1930. [Google Scholar] [CrossRef]
- Erchick, D.J.; Agarwal, S.; Kaysin, A.; Gibson, D.G.; Labrique, A.B. Changes in prenatal care and vaccine willingness among pregnant women during the COVID-19 pandemic. BMC Pregnancy Childbirth 2022, 22, 558. [Google Scholar] [CrossRef]
- Skirrow, H.; Barnett, S.; Bell, S.; Mounier-Jack, S.; Kampmann, B.; Holder, B. Women’s views and experiences of accessing pertussis vaccination in pregnancy and infant vaccinations during the COVID-19 pandemic: A multi-methods study in the UK. Vaccine 2022, 40, 4942. [Google Scholar] [CrossRef] [PubMed]
- Zapletal, J.; Drochýtek, V.; Vařbuchtová, A.; Halaška, M.J.; Rob, L. Analysis of awareness and acceptance of SARS-CoV-2 vaccination among pregnant women. Ces. Gynekol. 2022, 87, 100–103. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pregnant Women N = 21 | Healthcare Workers N = 14 | |||
|---|---|---|---|---|
| Characteristics | n | (%) | n | (%) |
| Age (years) * | ||||
| ≤25 | 3 | (14.3) | 1 | (7.1) |
| 26–30 | 5 | (23.8) | 4 | (28.6) |
| 31–35 | 4 | (19) | 2 | (14.3) |
| 36–40 | 6 | (28.6) | 0 | (0) |
| 41–45 | 3 | (14.3) | 0 | (0) |
| ≥46 | 0 | (0) | 6 | (42.9) |
| Nationality | ||||
| Spain | 13 | (61.9) | 12 | (85.7) |
| Bolivia | 1 | (4.8) | 1 | (7.1) |
| Colombia | 2 | (9.5) | 0 | (0) |
| Honduras | 1 | (4.8) | 0 | (0) |
| Italy | 1 | (4.8) | 0 | (0) |
| Poland | 1 | (4.8) | 0 | (0) |
| The Dominican Republic | 1 | (4.8) | 0 | (0) |
| Venezuela | 1 | (4.8) | 1 | (7.1) |
| Education | ||||
| Primary | 2 | (9.5) | 0 | (0) |
| Secondary | 2 | (9.5) | 0 | (0) |
| Vocational training | 4 | (19) | 0 | (0) |
| University | 13 | (61.9) | 14 | (100) |
| Occupation | ||||
| Employed | 19 | (90.5) | 14 | (100) |
| Unemployed | 2 | (9.5) | 0 | (0) |
| Gestational age (weeks) | ||||
| <24 | 8 | (38.1) | N/A | N/A |
| 24 or more | 13 | (61.9) | N/A | N/A |
| Marital status | ||||
| Single | 2 | (9.5) | N/A | N/A |
| In a relationship | 9 | (42.9) | N/A | N/A |
| Domestic partnership | 3 | (14.3) | N/A | N/A |
| Married | 6 | (28.6) | N/A | N/A |
| Widowed | 1 | (4.8) | N/A | N/A |
| Gravidity | ||||
| Primigravidae | 6 | (28.6) | N/A | N/A |
| Multigravidae | 15 | (71.4) | N/A | N/A |
| Religion | ||||
| Christian | 7 | (33.3) | N/A | N/A |
| None | 14 | (66.7) | N/A | N/A |
| COVID-19 status | ||||
| Had COVID-19 before pregnancy | 10 | (47.6) | N/A | N/A |
| Had COVID-19 during pregnancy | 10 | (47.6) | N/A | N/A |
| Medical speciality | ||||
| Gynaecologist/ Obstetrician | N/A | N/A | 5 | (35.7) |
| Midwife | N/A | N/A | 7 | (50) |
| General practitioner | N/A | N/A | 1 | (7.1) |
| Paediatrician | N/A | N/A | 1 | (7.1) |
| Reasons for Accepting Vaccination in Pregnancy | Translated Quotes in English |
|---|---|
| Good for the baby and the mother. | “The gynaecologist told me about the vaccine. Ehh, she explained it very well. She told me what benefits it would have, what it was good for, ehh that it would help my baby, that it would generate more antibodies in my body. I mean, I didn’t have to think about it much, neither yes nor no. I mean, I really agreed with the vaccination”. 213-01 |
| Avoiding infection. | “I understand that, yes, that all of them can have a risk, but I understand that the risk is low compared to the risk that the disease itself can bring”. 204-01 |
| Good for the community. | “In the first place, the COVID-19 vaccine, because I think we are in a serious pandemic situation and that the need is imminent, right? to stop it (…) So, I think that if, for example, you can get vaccinated and avoid it, then it is important. And if you don’t prevent it with the vaccine, at least perhaps you reduce the effects of, ehh, the virus so that it’s not so severe”. 203-01 |
| Recommendation by healthcare workers. | “Oh, it’s just that no, I mean, for me, it’s not… I mean, I haven’t considered a rejection, I mean, not getting vaccinated for me, it was a matter of definitely getting vaccinated. I mean, it wasn’t… it’s not debatable. (…) if a doctor tells me that I have to get this, well, I think he is the one who knows the criteria so that, so that I take a medicine or a vaccine or whatever”. 214-01 |
| Trust in the healthcare system. | “…I think that it [maternal vaccination] greatly depends on your opinion, on your trust in the healthcare system, and the trust in vaccines, medicines, treatments, well, all these things”. 204-01 |
| Reasons for Refusing Vaccination in Pregnancy | Translated Quotes in English |
|---|---|
| Fear that it could affect foetal development. | “There are people who are very distrusting and very, very suspicious. But it is true that pregnant women are perhaps obviously afraid that vaccines can affect the development of the foetus and that they don’t see these advantages, do they? To protect themselves from all the infections that others may have that can pass to the foetus through the placenta”. 207-02 |
| Low perception of disease risk. | “Because I thought I wouldn’t… no, no… get vaccinated… I didn’t have to save myself from getting the flu. And if I got the flu, well, well, I’d be in bed for a week with a stuffy nose. But hey… nothing happens, right? (…) I did not see the need, the usefulness”. 203-01 |
| Distrust in the healthcare system. | “Their arguments are very irrational, “what if they think we are here to be guinea pigs”, “what if not… we don’t have any kind of trust”. I mean, in fact, I anything, “I knew a person who was vaccinated and look what happened to them…”. (…) They don’t listen and they’re making generalisations or having a very catastrophic outlook or considering a very suspicious view”. 207-02 |
| Not being able to counteract the side effects with medication. | “Man, I think… well, let’s see, what can affect (the decision) a little more is that if you feel sick, so to speak, or you get a fever, maybe because you can’t have as many medications or don’t have them… yes you can take paracetamol. But hey, it’s not very appropriate for you to take it either. Well, maybe going through those symptoms without anything is what can cause doubts” 205-01 |
| Political views/Moral values. | “They say that the vaccines are not safe or that it is manipulation by the pharmaceutical companies. (…) And at the end of the day, they also don’t see individual benefits, don’t they? Because if it has to be a group benefit, then they don’t see it” 205-02 |
| Not believing in vaccines or other medications. | “Generally, people who do not want to be vaccinated do not want other medications either, that is, if they have diabetes, they would not inject insulin either. In other words, it is usually people who are already reluctant to any medication for fear that…” 105-02 |
| Fear of contracting an illness through vaccination. | “[Somebody] got the flu vaccine one day and they think they developed flu, which is not true because they cannot develop it because it is an inactivated vaccine. But… but well, it’s their belief. Then these people are more reluctant to get the vaccine”. 102-02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marín-Cos, A.; Marbán-Castro, E.; Nedic, I.; Ferrari, M.; Crespo-Mirasol, E.; Ventura, L.F.; Zamora, B.N.; Fumadó, V.; Menéndez, C.; Martínez Bueno, C.; et al. “Maternal Vaccination Greatly Depends on Your Trust in the Healthcare System”: A Qualitative Study on the Acceptability of Maternal Vaccines among Pregnant Women and Healthcare Workers in Barcelona, Spain. Vaccines 2022, 10, 2015. https://doi.org/10.3390/vaccines10122015
Marín-Cos A, Marbán-Castro E, Nedic I, Ferrari M, Crespo-Mirasol E, Ventura LF, Zamora BN, Fumadó V, Menéndez C, Martínez Bueno C, et al. “Maternal Vaccination Greatly Depends on Your Trust in the Healthcare System”: A Qualitative Study on the Acceptability of Maternal Vaccines among Pregnant Women and Healthcare Workers in Barcelona, Spain. Vaccines. 2022; 10(12):2015. https://doi.org/10.3390/vaccines10122015
Chicago/Turabian StyleMarín-Cos, Anna, Elena Marbán-Castro, Ivana Nedic, Mara Ferrari, Esther Crespo-Mirasol, Laia Ferrer Ventura, Berta Noya Zamora, Victoria Fumadó, Clara Menéndez, Cristina Martínez Bueno, and et al. 2022. "“Maternal Vaccination Greatly Depends on Your Trust in the Healthcare System”: A Qualitative Study on the Acceptability of Maternal Vaccines among Pregnant Women and Healthcare Workers in Barcelona, Spain" Vaccines 10, no. 12: 2015. https://doi.org/10.3390/vaccines10122015