
A Questionnaire-Based Cross-Sectional Survey of Knowledge, Attitudes, and Practices toward COVID-19 among Students and Staff in Asir, Saudi Arabia during the Second Wave of the Pandemic
 , , , and
, , , and
Abstract
:1. Introduction
2. Methodology
2.1. Study Design, Setting, and Population
2.2. Study Population and Sample Size
2.3. Survey Design and Pilot Study
2.4. Data Collection
2.5. Statistical Analysis
2.6. Ethical Approval
3. Results
3.1. Demography of Target Population
3.2. Knowledge of the Target Population towards COVID-19
3.3. Attitudes of the Target Population towards COVID-19
3.4. Practices of the Target Population towards COVID-19
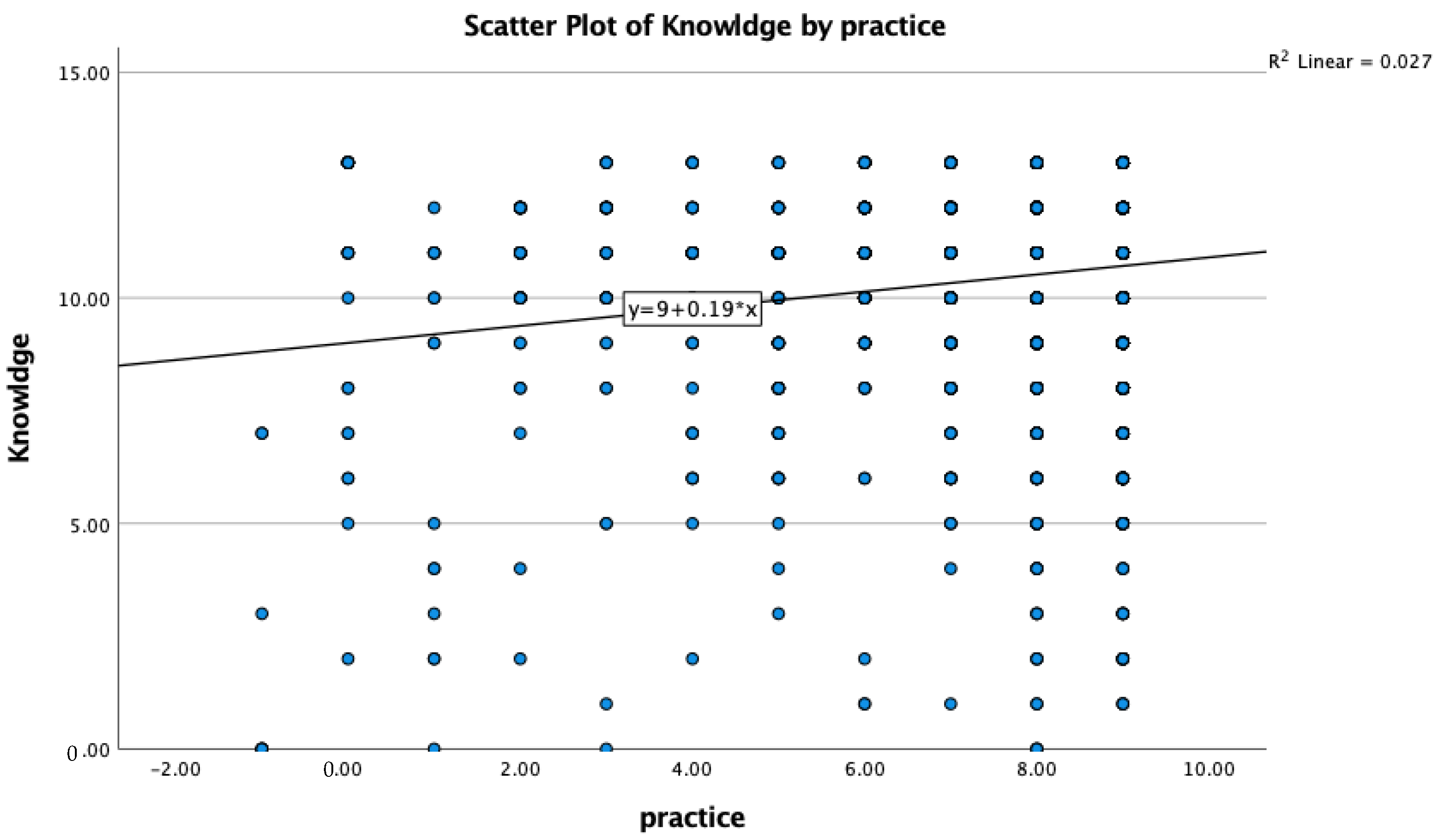
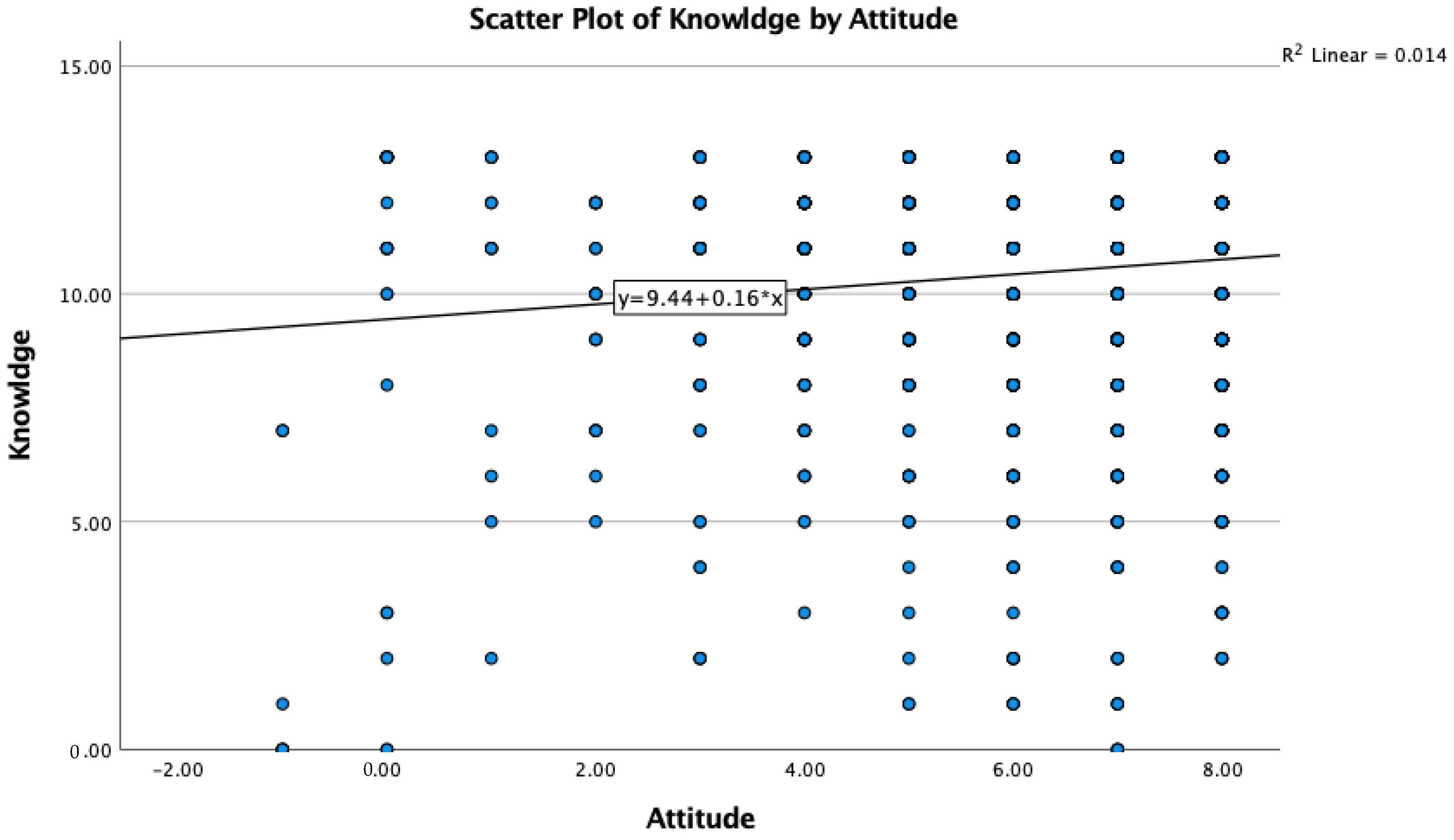
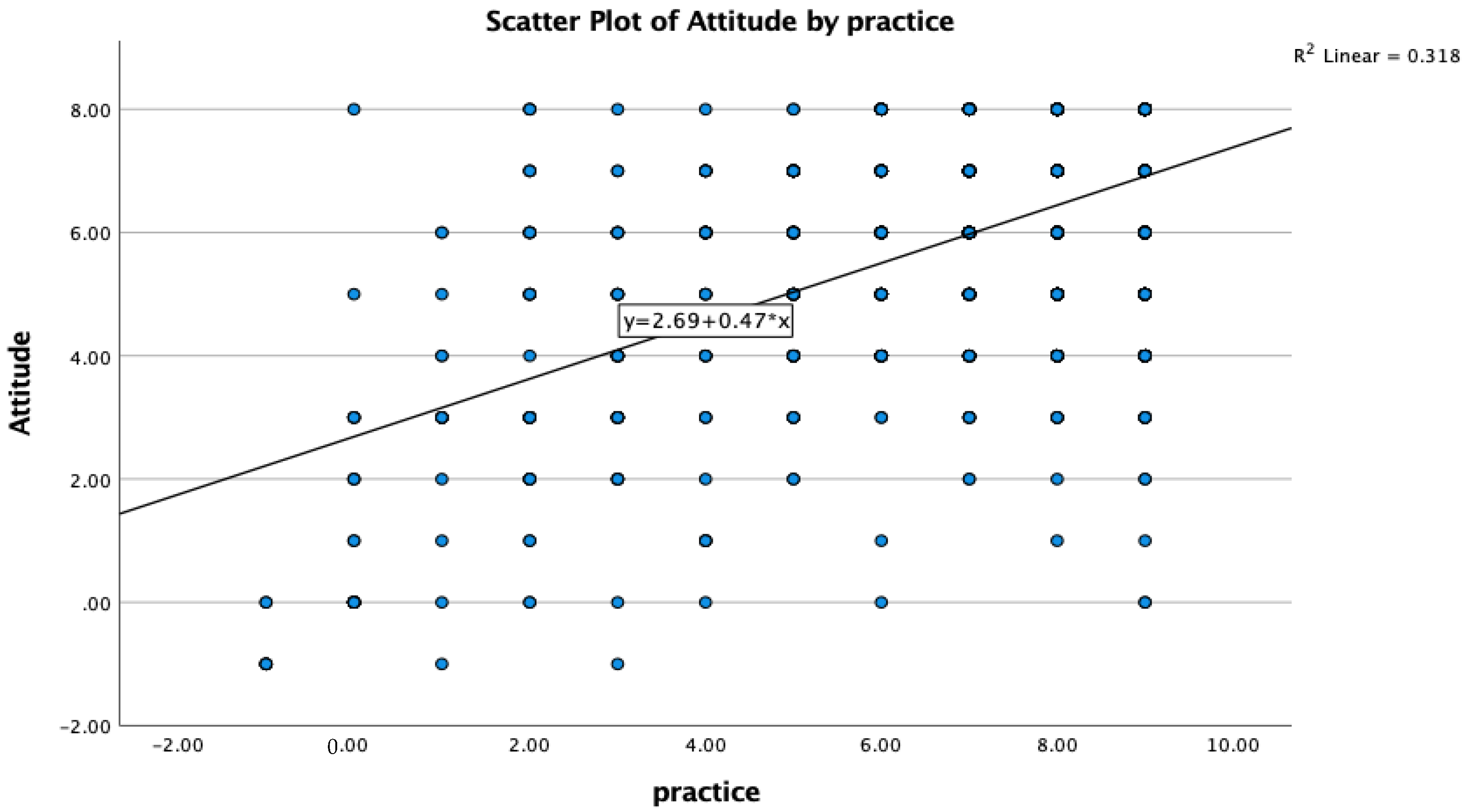
3.5. Association Analysis of the Target Population towards COVID-19
4. Discussion
5. Conclusions
6. Limitations of the Study
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Chin. J. Epidemiol. 2020, 41, 145–151. [Google Scholar]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report, 51. 2020. Available online: https://apps.who.int/iris/handle/10665/331475 (accessed on 20 March 2022).
- Centre for Disease Control (CDC). Selected Adverse Events Reported after COVID-19 Vaccination. Available online: www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html (accessed on 20 March 2021).
- Centre for Disease Control (CDC). Vaccine Breakthrough Infections. Available online: www.cdc.gov/coronavirus/2019-ncov/vaccines/effectiveness/why-measure-effectiveness/breakthrough-cases.html (accessed on 20 March 2021).
- Khan, A.; Alsofayan, Y.; Alahmari, A.; Alowais, J.; Algwizani, A.; Alserehi, H.; Assiri, A.; Jokhdar, H. COVID-19 in Saudi Arabia: The National Health Response. East. Mediterr. Health J. 2021, 27, 1114–1124. Available online: http://www.emro.who.int/in-press/reviews/covid-19-in-saudi-arabia-the-national-health-response.html (accessed on 20 November 2021). [CrossRef] [PubMed]
- Ebrahim, S.H.; Memish, Z.A. Saudi Arabia’s drastic measures to curb the COVID-19 outbreak: Temporary suspension of the Umrah pilgrimage. J. Travel Med. 2020, 27, taaa029. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Education. Moe.gov.sa. Available online: https://www.moe.gov.sa/ar/Pages/default.aspx (accessed on 22 August 2020).
- The Official Saudi Press Agency. Spa.gov.sa. Available online: https://www.spa.gov.sa/?lang=en (accessed on 22 August 2020).
- Al-Hanawi, M.K.; Angawi, K.; Alshareef, N.; Qattan, A.M.N.; Helmy, H.Z.; Abudawood, Y.; Alqurashi, M.; Kattan, W.M.; Kadasah, N.A.; Chirwa, G.C. Knowledge, Attitude and Practice Toward COVID-19 Among the Public in the Kingdom of Saudi Arabia: A Cross-Sectional Study. Front. Public Health 2022, 8, 217. [Google Scholar] [CrossRef] [PubMed]
- Alnasser, A.H.A.; Al-Tawfiq, J.A.; Al-Kalif, M.S.H.; Shahadah, R.F.B.; Almuqati, K.S.A.; Al-Sulaiman, B.S.A.; Alharbi, K.K.S.; Alabbad, F.Y.M.; Alabbad, J.Y.M.; Alquwaiz, I.A.I. Public Knowledge, Attitudes, and Practice towards COVID-19 Pandemic in Saudi Arabia: A Web-Based Cross-Sectional Survey. Med. Sci. 2021, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Alshareef, N.; Yunusa, I.; Al-Hanawi, M.K. The Influence of COVID-19 Information Sources on the Attitudes and Practices Toward COVID-19 among the General Public of Saudi Arabia: Cross-sectional Online Survey Study. JMIR Public Health Surveill. 2021, 7, e28888. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, M.O.; El-Gendy, A.O.; Abdelrahim, M.E.A. Public awareness in Egypt about COVID-19 spread in the early phase of the pandemic. Patient Educ. Couns. 2020, 103, 2598–2601. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K.; Alshareef, N.; El-Sokkary, R.H. Willingness to Receive COVID-19 Vaccination among Older Adults in Saudi Arabia: A Community-Based Survey. Vaccines 2021, 11, 1257. [Google Scholar] [CrossRef]
- El-Sokkary, R.H.; El Seifi, O.S.; Hassan, H.M.; Mortada, E.M.; Hashem, M.K.; Gadelrab, M.R.M.A.; Tash, R.M.E. Predictors of COVID-19 vaccine hesitancy among Egyptian healthcare workers: A cross-sectional study. BMC Infect. Dis. 2021, 21, 762. [Google Scholar] [CrossRef]
- General Authority for Statistics. Available online: www.stats.gov.sa/sites/default/files/aseer_region_ar.pdf (accessed on 10 March 2021).
- Ministry of Health. Statistical Yearbook 1439H. Kingdom of Saudi Arabia. 2018. Available online: www.moh.gov.sa/en/Ministry/Statistics/book/Documents/StatisticalBook-1439.pdf (accessed on 13 August 2020).
- Wee, E.G.; Giri, M.S.; Sundram, T.K.; Venudran, C.V. COVID-19: Knowledge, Attitude and Preventive Behaviours of Medical and Dental Students. Int. J. Biomed. Clin. Sci. 2020, 5, 236–256. [Google Scholar]
- Khan, M.U.; Shah, S.; Ahmad, A.; Fatokun, O. Knowledge and attitude of healthcare workers about middle east respiratory syndrome in multispecialty hospitals of Qassim, Saudi Arabia. BMC Public Health 2014, 14, 1281. [Google Scholar] [CrossRef] [Green Version]
- Nour, M.; Babilghith, A.; Natto, H.; Elamin, F.; Alawneh, S. Knowledge, attitude and practices of healthcare providers towards MERS-CoV infection at Makkah hospitals, KSA. Int. Res. J. Med. Med. Sci. 2015, 3, 103. [Google Scholar]
- Asaad, A.; El-Sokkary, R.; Alzamanan, M.; El-Shafei, M. Knowledge and attitudes towards Middle East respiratory syndrome-coronavirus (MERS-CoV) among health care workers in south-western Saudi Arabia. East. Mediterr. Health J. 2020, 26, 435–442. [Google Scholar] [CrossRef]
- Khaled, A.; Siddique, A.; Makki, S. The Knowledge and Attitude of the Community from the Aseer Region, Saudi Arabia, Toward COVID-19 and Their Precautionary Measures against the Disease. Risk Manag. Healthc. Policy 2020, 13, 1825–1834. [Google Scholar] [CrossRef]
- Akalu, Y.; Ayelign, B.; Molla, M.D. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect. Drug Resist. 2020, 13, 1949–1960. [Google Scholar] [CrossRef]
- Update on COVID-19: Omicron Wave Threatening to Overcome Health Workforce. Available online: https://www.euro.who.int/en/media-centre/sections/statements/2022/statement-update-on-covid-19-omicron-wave-threatening-to-overcome-health-workforce (accessed on 11 January 2022).
- Adam, M.; Gameraddin, M.; Alelyani, M.; Zaman, G.S.; Musa, A.; Ahmad, I.; Alshahrani, M.Y.; Alsultan, K.; Gareeballah, A. Assessment of Knowledge, Attitude, and Practice Concerning COVID-19 Among Undergraduate Students of Faculty of Applied Medical Sciences at King Khalid University, Abha, Kingdom of Saudi Arabia: A Cross-Sectional Surveyed Study. Adv. Med. Educ. Pract. 2021, 12, 789–797. [Google Scholar] [CrossRef]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.B.; Miema, J.M.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of vaccination against COVID-19 among healthcare workers in the Democratic Republic of the Congo. Pragmat. Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High rates of COVID-19 vaccine hesitancy and its association with conspiracy beliefs: A study in Jordan and Kuwait among other Arab countries. Vaccines. 2021, 9, 42. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 60. [Google Scholar] [CrossRef] [PubMed]
- Almalki, M.J. Knowledge, Attitudes, and Practices toward COVID-19 Among the General Public in the Border Region of Jazan, Saudi Arabia: A Cross-Sectional Study. Front. Public Health 2021, 8, 733125. [Google Scholar] [CrossRef] [PubMed]
- Saquib, S.A.; Al-Harthi, H.M.; Khoshhal, A.A.; Shaher, A.A.; Al-Shammari, A.B.; Khan, A. Knowledge and attitude about basic life support and emergency medical services amongst healthcare interns in University Hospitals: A Cross-Sectional Study. Emerg. Med. Int. 2019, 2019, 9342892. [Google Scholar] [CrossRef]
- Hamza, M.S.; Badary, O.A.; Elmazar, M.M. Cross-sectional study on awareness and knowledge of COVID-19 among senior pharmacy students. J. Community Health 2020, 46, 139–146. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic | n (%) N = 2191 |
|---|---|
| Age group | |
| Under 18 years old | 233 (10.6) |
| 20–<30 years old | 845 (38.6) |
| 30–<40 years old | 436 (19.9) |
| 40–<50 years old | 513 (23.4) |
| 50–60 years old | 143 (6.5) |
| >60 years | 21 (1) |
| Gender (female) | 1544 (70.5) |
| Status | |
| Administrative Staff | 364 (16.6) |
| Student | 1127 (51.4) |
| Teaching Staff | 700 (31.9) |
| Place of residence | |
| Rural | 509 (23.2) |
| Urban | 1682 (76.8) |
| Level of education | |
| Bachelor | 1508 (68.8) |
| Master | 85 (3.9) |
| Others | 544 (24.8) |
| PhD | 54 (2.5) |
| Have you ever attended COVID-19 infection training or orientation session? (yes) | 1594 (72.8) |
| Have you been infected with COVID-19? (yes) | 351 (16) |
| Has any of your colleagues been infected with COVID-19? (yes) | 1562 (71.3) |
| Would you like to take COVID-19 vaccine? (yes) | 1226 (56) |
| Knowledge about COVID-19 | Yes * n (%) | No n (%) | I Don’t Know n (%) |
|---|---|---|---|
| 1. The major clinical signs of COVID-19 are fever, fatigue, dry cough, and muscle aches. | 1859 (84.8) | 67 (3.1) | 265 (12.1) |
| 2. Stuffy nose, runny nose, and sneezing are less common in COVID-19 than in common cold. | 1292 (59) | 293 (13.4) | 606 (27.7) |
| 3. Alarming signs for COVID-19 that necessitate immediate medical care include difficulty of breathing, persistent pain or pressure in the chest. | 1944 (88.7) | 32 (1.5) | 215 (9.8) |
| 4. COVID-19 symptoms may appear 2–14 days after exposure to a source of SARS-CoV-2 virus. | 1738 (79.3) | 115 (5.2) | 338 (15.4) |
| 5. Not all persons with COVID-19 will progress from mild case to severe one. | 865 (39.5) | 698 (31.9) | 628 (28.7) |
| 6. COVID-19 may be transmitted to others even if the infected person is asymptomatic (Show no symptoms) | 1846 (84.3) | 97 (4.4) | 248 (11.3) |
| 7. The COVID-19 is transmitted through respiratory droplets of infected individuals. | 1935 (88.3) | 74 (3.4) | 182 (8.3) |
| 8. There is currently no specific treatment for COVID-19. | 1355 (61.8) | 387 (17.7) | 449 (20.5) |
| 9. Early detection and supportive treatment are corner stone in COVID-19 management. | 1816 (82.9) | 90 (4.1) | 285 (13) |
| 10. Persons who wear protective masks help control the spread of COVID-19. | 2001 (91.3) | 111 (5.1) | 79 (3.6) |
| 11. For not to get infected by the COVID-19 virus, people should avoid visiting crowded places. | 2124 (96.9) | 16 (0.7) | 51 (2.3) |
| 12. Physical distancing and treatment of COVID-19 cases are effective ways to minimize the spread of the virus. | 2124 (96.9) | 67 (3.1) | 0 (0) |
| 13. People who have connected with infected COVID-19 individuals should immediately follow the self-quarantine procedures for 14 days. | 2086 (95.2) | 49 (2.2) | 56 (2.6) |
| Attitude towards COVID-19 | Agree * n (%) | Disagree n (%) | Neutral n (%) |
|---|---|---|---|
| 1. I am always ready to protect myself from getting infected by the SARS-CoV-2 virus. | 1901 (86.8) | 182 (8.3) | 108 (4.9) |
| 2. I think it is necessary to store enough amount of food, and medicines to avoid going out of the house during the quarantine period | 1454 (66.4) | 443 (20.2) | 294 (13.4) |
| 3. I am worried to get infected by SARS-CoV-2 virus. | 1195 (54.5) | 687 (31.4) | 309 (14.1) |
| 4. It is necessary to take actions to prevent the possible transfer of COVID-19 to my family members. | 2076 (94.8) | 66 (3) | 49 (2.2) |
| 5. I feel anxious, when hearing news about increasing number of patients infected with COVID-19. | 1717 (78.4) | 300 (13.7) | 174 (7.9) |
| 6. I believe that COVID-19 will be successfully controlled soon. | 1685 (76.9) | 274 (12.5) | 232 (10.6) |
| 7. I support the government-compulsory obligatory home quarantine for up to 2 weeks for people who have been close with someone who has been examined positive for COVID19. | 1952 (89.1) | 123 (5.6) | 116 (5.3) |
| 8. I support postponing or cancelling mass gatherings such as festivals, or sporting events. | 2044 (93.3) | 79 (3.6) | 68 (3.1) |
| Questions about Practices to Control COVID-19 | Agree * n (%) | Disagree n (%) | Neutral n (%) |
|---|---|---|---|
| 1. Essential proper hygiene begins with washing hands using soap for 20 s. | 1989 (90.8) | 125 (5.7) | 77 (3.5) |
| 2. I wash my hands after touching personal items of someone who has cough and/or cold | 2052 (93.7) | 77 (3.5) | 62 (2.8) |
| 3. I wash my hands after touching any plastic or paper from sources such as groceries. | 1956 (89.3) | 131 (6) | 104 (4.7) |
| 4. I wash my hands after touching doorknobs. | 1891 (86.3) | 158 (7.2) | 142 (6.5) |
| 5. I eat nutritious foods such as vegetables and fruits to keep healthy. | 1936 (88.4) | 103 (4.7) | 152 (6.9) |
| 6. I use hand gel to sanitize my hands. | 2013 (91.9) | 98 (4.5) | 80 (3.7) |
| 7. I disinfect cell phones, headsets, laptops, and all other gadgets that are frequently used. | 1595 (72.8) | 365 (16.7) | 231 (10.5) |
| 8. I avoid touching the face, eyes, nose and mouth. | 1886 (86.1) | 167 (7.6) | 138 (6.3) |
| 9. I wear a facemask when leaving home. | 1935 (88.3) | 142 (6.5) | 114 (5.2) |
| Correlations | ||||
|---|---|---|---|---|
| Practice | Knowledge | |||
| Spearman’s rho | Practice | Correlation Coefficient | 1 | 0.070 ** |
| Sig. (2-tailed) | . | 0.001 | ||
| N | 2124 | 2124 | ||
| Knowledge | Correlation Coefficient | 0.070 ** | 1 | |
| Sig. (2-tailed) | 0.001 | . | ||
| N | 2124 | 2191 |
| Correlations | ||||
|---|---|---|---|---|
| knowledge | attitude | |||
| Spearman’s rho | Knowledge | Correlation Coefficient | 1 | 0.050 * |
| Sig. (2-tailed) | . | 0.018 | ||
| N | 2191 | 2191 | ||
| Attitude | Correlation Coefficient | 0.050 * | 1 | |
| Sig. (2-tailed) | 0.018 | . | ||
| N | 2191 | 2191 |
| Correlations | ||||
|---|---|---|---|---|
| Attitude | Practice | |||
| Spearman’s rho | Attitude | Correlation Coefficient | 1 | 0.367 ** |
| Sig. (2-tailed) | . | 0 | ||
| N | 2191 | 2124 | ||
| Practice | Correlation Coefficient | 0.367 ** | 1 | |
| Sig. (2-tailed) | 0 | . | ||
| N | 2124 | 2124 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheraba, N.S.; Orayj, K.; Alqahtani, A.; El-sokkary, R.H.; Khalid, M. A Questionnaire-Based Cross-Sectional Survey of Knowledge, Attitudes, and Practices toward COVID-19 among Students and Staff in Asir, Saudi Arabia during the Second Wave of the Pandemic. Vaccines 2022, 10, 2014. https://doi.org/10.3390/vaccines10122014
Sheraba NS, Orayj K, Alqahtani A, El-sokkary RH, Khalid M. A Questionnaire-Based Cross-Sectional Survey of Knowledge, Attitudes, and Practices toward COVID-19 among Students and Staff in Asir, Saudi Arabia during the Second Wave of the Pandemic. Vaccines. 2022; 10(12):2014. https://doi.org/10.3390/vaccines10122014
Chicago/Turabian StyleSheraba, Norhan Saif, Khalid Orayj, Ali Alqahtani, Rehab H. El-sokkary, and Mohammad Khalid. 2022. "A Questionnaire-Based Cross-Sectional Survey of Knowledge, Attitudes, and Practices toward COVID-19 among Students and Staff in Asir, Saudi Arabia during the Second Wave of the Pandemic" Vaccines 10, no. 12: 2014. https://doi.org/10.3390/vaccines10122014