

Low Uptake of the Second Dose of Human Papillomavirus Vaccine in Dar es Salaam, Tanzania



Abstract
:1. Introduction
2. Methods
2.1. Study Area and Design
Sampling and Sample Size
2.2. Study Population
2.3. Measurements
2.4. Data Management and Analysis
2.5. Ethical Consideration
3. Results
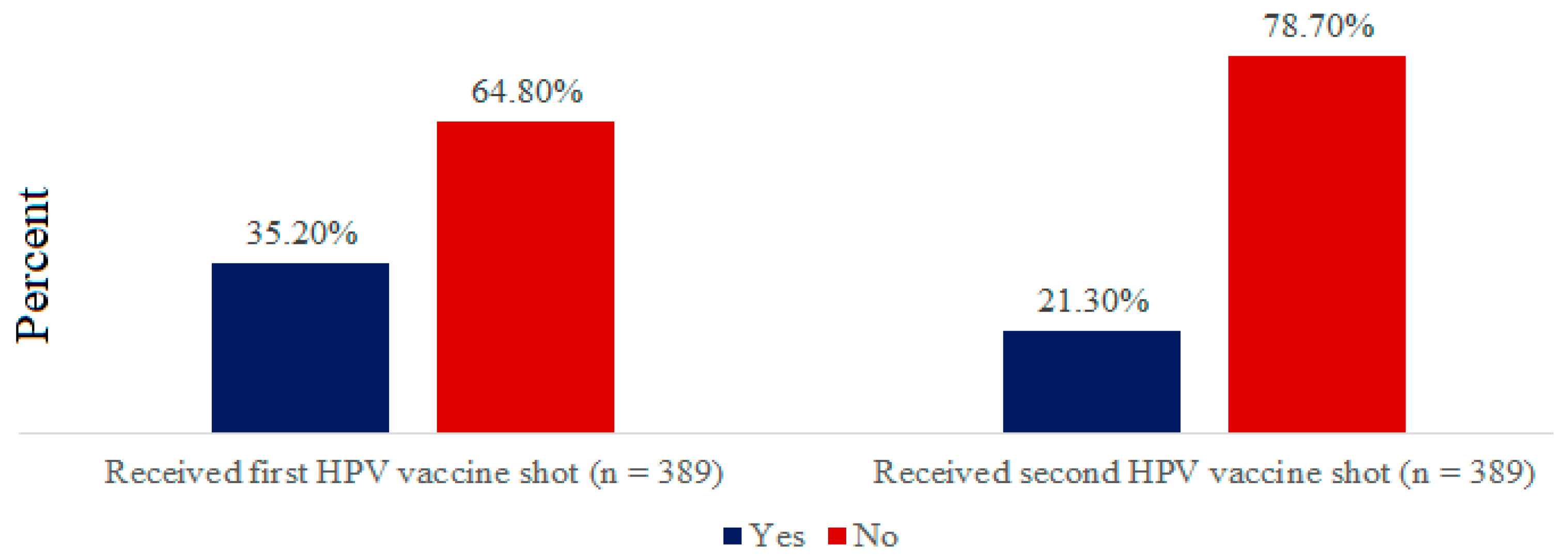
3.1. HPV Vaccine Uptake
3.2. Socio-Demographic Characteristics of HPV-2 Vaccine Uptake
3.3. Factors Associated with Uptake of the Second Dose of HPV Vaccine
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Questionnaire for School Children
| Demographic characteristics of a participant | |||
| |||
| |||
| |||
| |||
| Household wealth index | Yes | No | |
| |||
| (a) A watch? | |||
| (b) A mobile phone? | |||
| (c) A bicycle? | |||
| (d) A car or a truck? | |||
| (e) A boat with a motor? | |||
| Yes | No | |
| (a) Electricity that is connected? | |||
| (b) A radio in working condition? | |||
| (c) A television in working condition? | |||
| (d) A computer in working condition? | |||
| (e) A refrigerator in working condition? | |||
| (f) Battery or generator for power? | |||
| (g) An iron (charcoal or electricity)? | |||
| |||
| |||
| |||
| Awareness and knowledge about HPV vaccine and cervical cancer. | |||
| Variable | Response | ||
| Yes | No | ||
| |||
| |||
| If yes, | |||
| |||
| Yes | No | |
| If yes, | |||
| |||
|
(a) Television (b) Radio (c) The internet (d) Magazine/newspapers (e) Doctor or nurse (f) Teachers (g) Friends/peers (h) Parents (i) Relatives other than parents (j) Church/synagogue/mosque | |||
| Yes | No | |
| (a) Anal warts | |||
| (b) Oral cancer | |||
| (c) Genital warts | |||
| (d) Cervical cancer | |||
| Yes | No | |
| (a) Anal cancer | |||
| (b) Oral cancer | |||
| (c) Cervical cancer | |||
| (d) Genital warts | |||
| Yes | No | |
| (a) Air droplets? | |||
| (b) Contact with body fluids? | |||
| (c) Sexual intercourse? | |||
| 18. HPV infection can be prevented with: | Yes | No | |
| (a) Vaccine | |||
| (b) Use of condom | |||
| (c) Antibiotics | |||
| (d) Sexual abstinence | |||
| Perception about HPV vaccine and cervical cancer | |||
| Perception | Yes | No | Don’t know |
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| Attitude about HPV vaccine completion | |||
| |||
|
1. Strongly disagree 2. Disagree 3. Undecided 4. Agree 5. Strongly agree | |||
| |||
|
1. Strongly disagree 2. Disagree 3. Undecided 4. Agree 5. Strongly agree | |||
| |||
|
1. Strongly disagree 2. Disagree 3. Undecided 4. Agree 5. Strongly agree | |||
| |||
|
1. Strongly disagree 2. Disagree 3. Undecided 4. Agree 5. Strongly agree | |||
| |||
| |||
| |||
| |||
| |||
| |||
| HPV vaccine coverage | Yes | No | |
| |||
| |||
References
- Small, W., Jr.; Bacon, M.A.; Bajaj, A.; Chuang, L.T.; Fisher, B.J.; Harkenrider, M.M.; Jhingran, A.; Kitchener, H.C.; Mileshkin, L.R.; Viswanathan, A.N.; et al. Cervical cancer: A global health crisis. Cancer 2017, 123, 2404–2412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gultekin, M.; Ramirez, P.T.; Broutet, N.; Hutubessy, R. World Health Organization call for action to eliminate cervical cancer globally. Int. J. Gynecol. Cancer 2020, 30, 426–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatumo, M.; Gacheri, S.; Sayed, A.R.; Scheibe, A. Women’s knowledge and attitudes related to cervical cancer and cervical cancer screening in Isiolo and Tharaka Nithi counties, Kenya: A cross-sectional study. BMC Cancer 2018, 18, 745. [Google Scholar] [CrossRef] [PubMed]
- Alsbeih, G. Exploring the causes of the low incidence of cervical cancer in western Asia. Asian Pac. J. Cancer Prev. 2018, 19, 1425–1429. [Google Scholar]
- Mukama, T.; Ndejjo, R.; Musabyimana, A.; Halage, A.A.; Musoke, D. Women’s knowledge and attitudes towards cervical cancer prevention: A cross sectional study in Eastern Uganda. BMC Women’s Health 2017, 17, 9. [Google Scholar] [CrossRef] [Green Version]
- Runge, A.S.; Bernstein, M.E.; Lucas, A.N.; Tewari, K.S. Cervical cancer in Tanzania: A systematic review of current challenges in six domains. Gynecol. Oncol. Rep. 2019, 29, 40–47. [Google Scholar] [CrossRef]
- Cunningham, M.S.; Skrastins, E.; Fitzpatrick, R.; Jindal, P.; Oneko, O.; Yeates, K.; Booth, C.M.; Carpenter, J.; Aronson, K.J. Cervical cancer screening and HPV vaccine acceptability among rural and urban women in Kilimanjaro Region, Tanzania. BMJ Open 2015, 5, e005828. [Google Scholar] [CrossRef] [Green Version]
- Mwaka, A.D.; Orach, C.G.; Were, E.M.; Lyratzopoulos, G.; Wabinga, H.; Roland, M. Awareness of cervical cancer risk factors and symptoms: Cross-sectional community survey in post-conflict northern Uganda. Health Expect. 2016, 19, 854–867. [Google Scholar] [CrossRef] [Green Version]
- Sankaranarayanan, R.; Joshi, S.; Muwonge, R.; Esmy, P.O.; Basu, P.; Prabhu, P.; Bhatla, N.; Nene, B.M.; Shaw, J.; Poli, U.R.R.; et al. Can a single dose of human papillomavirus (HPV) vaccine prevent cervical cancer? Early findings from an Indian study. Vaccine 2018, 36, 4783–4791. [Google Scholar] [CrossRef]
- Orenstein, W.A.; Gellin, B.G.; Beigi, R.H.; Despres, S.; Lynfield, R.; Maldonado, Y.; Mouton, C.; Rawlins, W.; Rothholz, M.C.; National Vaccine Advisory Committee; et al. Overcoming barriers to low hpv vaccine uptake in the United States: Recommendations from the national vaccine advisory committee. Public Health Rep. 2016, 131, 17–25. [Google Scholar]
- Cartmell, K.B.; Young-Pierce, J.; McGue, S.; Alberg, A.J.; Luque, J.S.; Zubizarreta, M.; Brandt, H.M. Barriers, facilitators, and potential strategies for increasing HPV vaccination: A statewide assessment to inform action. Papillomavirus Res. 2018, 5, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.L.; Shew, M.L.; Zimet, G.D.; Ding, L.; Mullins, T.L.K.; Kahn, J.A. Human Papillomavirus Vaccine Sources of Information and Adolescents’ Knowledge and Perceptions. Glob. Pediatr. Health 2017, 4, 2333794X17743405. [Google Scholar] [CrossRef] [PubMed]
- Ndikom, C.M.; Oboh, P.I. Perception, Acceptance and Uptake of Human Papillomavirus Vaccine among Female Adolescents in Selected Secondary Schools in Ibadan. Nigeria 2017, 20, 237–244. [Google Scholar]
- Suryadevara, M.; Bonville, J.R.; Kline, R.M.; Magowan, C.; Domachowske, E.; Cibula, D.A.; Domachowske, J. Student HPV vaccine attitudes and vaccine completion by education level. Hum. Vaccines Immunother. 2016, 12, 1491–1497. [Google Scholar] [CrossRef] [PubMed]
- Kisaakye, E.; Namakula, J.; Kihembo, C.; Kisakye, A.; Nsubuga, P.; Babirye, J.N. Level and factors associated with uptake of human papillomavirus infection vaccine among female adolescents in Lira District, Uganda. Pan. Afr. Med. J. 2018, 31, 184. [Google Scholar] [CrossRef]
- Wilson, A.R.; Hashibe, M.; Bodson, J.; Gren, L.H.; Taylor, B.A.; Greenwood, J.; Jackson, B.R.; She, R.; Egger, M.J.; Kepka, D. Factors related to HPV vaccine uptake and 3-dose completion among women in a low vaccination region of the USA: An observational study. BMC Women’s Health 2016, 16, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, K.E.; LaMontagne, D.S.; Watson-Jones, D. Status of HPV vaccine introduction and barriers to country uptake. Vaccine 2018, 36, 4761–4767. [Google Scholar] [CrossRef]
- You, D.; Han, L.; Li, L.; Hu, J.; Zimet, G.D.; Alias, H.; Danaee, M.; Cai, L.; Zeng, F.; Wong, L.P. Human papillomavirus (HPV) vaccine uptake and the willingness to receive the HPV vaccination among female college students in China: A multicenter study. Vaccines 2020, 8, 31. [Google Scholar] [CrossRef] [Green Version]
- Leung, J.T.C.; Law, C.-K. Revisiting knowledge, attitudes and practice (KAP) on human papillomavirus (HPV) vaccination among female university students in Hong Kong. Hum. Vaccines Immunother. 2018, 14, 924–930. [Google Scholar] [CrossRef]
- Sisson, H.; Child, R.N.; Wilkinson, Y.; Rgn, H. An Integrative Review of the Influences on Decision-Making of Young People about Human Papillomavirus Vaccine. J. Sch. Nurs. 2019, 35, 39–50. [Google Scholar] [CrossRef]
- Ganczak, M.; Owsianka, B.; Korzeń, M. Factors that predict parentalwillingness to have their children vaccinated against HPV in a country with low HPV vaccination coverage. Int. J. Environ. Res. Public Health 2018, 15, 645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oluwole, E.O.; Idowu, O.M.; Adejimi, A.A.; Balogun, M.R.; Osanyin, G.E. Knowledge, attitude and uptake of human papillomavirus vaccination among female undergraduates in Lagos State, Nigeria. J. Fam. Med. Prim. Care. 2019, 8, 3627–3633. [Google Scholar] [CrossRef] [PubMed]
- Tung, I.L.Y.; Machalek, D.A.; Garland, S.M. Attitudes, knowledge and factors associated with Human Papillomavirus (HPV) vaccine uptake in adolescent girls and young women in Victoria, Australia. PLoS ONE 2016, 11, e0161846. [Google Scholar] [CrossRef] [PubMed]
- Cocchio, S.; Bertoncello, C.; Baldovin, T.; Fonzo, M.; Bennici, S.E.; Buja, A.; Majori, S.; Baldo, V. Awareness of HPV and drivers of HPV vaccine uptake among university students: A quantitative, cross-sectional study. Health Soc. Care Community 2020, 28, 1514–1524. [Google Scholar] [CrossRef] [PubMed]
- Bennett, A.T.; Patel, D.A.; Carlos, R.C.; Zochowski, M.K.; Pennewell, S.M.; Chi, A.M.; Dalton, V.K. Human Papillomavirus Vaccine Uptake after a Tailored, Online Educational Intervention for Female University Students: A Randomized Controlled Trial. J. Women’s Health 2015, 24, 950–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahijani, A.Y.; King, A.R.; Gullatte, M.M.; Hennink, M.; Bednarczyk, R.A. HPV Vaccine Promotion: The church as an agent of change. Soc. Sci. Med. 2021, 268, 113375. [Google Scholar] [CrossRef] [PubMed]
- Ko, L.K.; Taylor, V.M.; Mohamed, F.B.; Do, H.H.; Gebeyaw, F.A.; Ibrahim, A.; Ali, A.A.; Winer, R.L. “We brought our culture here with us”: A qualitative study of perceptions of HPV vaccine and vaccine uptake among East African immigrant mothers. Papillomavirus Res. 2019, 7, 21–25. [Google Scholar] [CrossRef]
- Yesaya, D. Knowledge, Attitude, and Practice towards Human Papilloma Virus (HPV) and Its Vaccination among Students at the University of Eastern Finland. Master’s Thesis, Itä-Suomen yliopisto, Kuopio, Finland, November 2020. [Google Scholar]
- Mendes Lobão, W.; Duarte, F.G.; Burns, J.D.; de Souza Teles Santos, C.A.; Chagas de Almeida, M.C.; Reingold, A.; Duarte Moreira, E. Low coverage of HPV vaccination in the national immunization programme in Brazil: Parental vaccine refusal or barriers in health-service based vaccine delivery? PLoS ONE 2018, 13, e0206726. [Google Scholar] [CrossRef] [Green Version]
- Netfa, F.; Tashani, M.; Booy, R.; King, C.; Rashid, H.; Skinner, S.R. Knowledge, Attitudes and Perceptions of Immigrant Parents towards Human Papillomavirus (HPV) Vaccination: A Systematic Review in Australia. Trop. Med. Infect. 2020, 5, 58. [Google Scholar] [CrossRef] [Green Version]
- Vickers, M.; Green, C.L.; Lee, H.Y.; Pierce, J.Y.; Daniel, C.L. Factors Associated with HPV Vaccination Uptake and HPV-Associated Cancers: A County-Level Analysis in the State of Alabama. J. Community Health 2019, 44, 1214–1223. [Google Scholar] [CrossRef]
- Isabirye, A.; Mbonye, M.; Asiimwe, J.B.; Kwagala, B. Factors associated with HPV vaccination uptake in Uganda: A multi-level analysis. BMC Women’s Health 2020, 20, 145. [Google Scholar] [CrossRef] [PubMed]
- Mphuru, A.; Li, A.J.; Kyesi, F.; Mwengee, W.; Mazige, F.; Nshunju, R.; Shayo, B.; Giattas, M.R.; Loharikar, A.; Lyimo, D. National introduction of human papillomavirus (HPV) vaccine in Tanzania: Programmatic decision-making and implementation. Vaccine 2022, 40, A2–A9. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Nygård, M.; Hansen, B.T. Sociodemographic correlates of human papillomavirus vaccine uptake: Opportunistic and catch-up vaccination in Norway. Cancers 2021, 13, 3483. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Received Second Dose of HPV Vaccine | ||||
|---|---|---|---|---|---|
| Yes | No | p-Value (χ2) | |||
| N | (%) | N | (%) | ||
| Age (years) | |||||
| 12–13 | 2 | (3.5) | 55 | (96.5) | <0.001 |
| 14+ | 81 | (24.4) | 251 | (75.6) | |
| Parental status | |||||
| One parent or orphan | 14 | (20.9) | 53 | (79.1) | 0.923 |
| Two parents | 69 | (21.4) | 253 | (78.6) | |
| Parental educational level | |||||
| No formal or primary education | 15 | (19.0) | 64 | (81.0) | <0.001 |
| secondary or above | 68 | (21.9) | 242 | (78.1) | |
| Parents’ occupation status | |||||
| Employed | 20 | (14.3) | 120 | (85.7) | 0.032 |
| Self employed | 53 | (24.7) | 162 | (75.3) | |
| Unemployed | 10 | (29.4) | 24 | (70.6) | |
| Household Wealth Index | |||||
| Lowest | 19 | (24.4) | 59 | (75.6) | 0.122 |
| Second | 21 | (27.3) | 56 | (72.7) | |
| Middle | 20 | (25.6) | 58 | (74.4) | |
| Fourth | 10 | (12.8) | 68 | (87.2) | |
| Highest | 13 | (16.7) | 65 | (83.3) | |
| Total | 83 | (21.3) | 306 | (78.7) | |
| Variables | N (%) | Un Adjusted OR (95%CI) | p Value | Adjusted OR (95%CI) | p Value |
|---|---|---|---|---|---|
| Age (years) | |||||
| 12–13 | 147 (37.8) | 8.87 (2.12 37.19) | 0.003 | 0.14 (0.03 0.59) | 0.008 |
| 14+ | 332 (85.3) | 1 | 1 | ||
| Parental educational status | |||||
| No formal or primary education | 79 (20.3) | 1.09 (0.59 2.00) | 0.79 | 0.61 (0.30 1.22) | 0.159 |
| Secondary or above | 310 (79.7) | 1 | 1 | ||
| Parental occupational status | |||||
| Employed | 140 (36.0) | 2.50 (1.04 6.01) | 0.04 | 0.39 (0.14 1.05) | 0.063 |
| Self employed | 215 (55.7) | 1.27 (0.57 2.84) | 0.55 | 0.70 (0.28 1.73) | 0.444 |
| Unemployed | 34 (8.7) | 1 | 1 | ||
| Household wealth index | |||||
| Lowest | 78 (20.1) | 1.61 (0.73 3.54) | 0.132 | 1.39 (0.57 3.38) | 0.468 |
| Second | 77 (19.8) | 1.87 (0.86 4.08) | 0.236 | 2.07 (0.87 4.88) | 0.098 |
| Middle | 78 (20.1) | 1.72 (0.79 3.77) | 0.114 | 1.52 (0.65 3.53) | 0.330 |
| Fourth | 78 (20.1) | 0.73 (0.30 1.79) | 0.173 | 0.57 (0.22 1.48) | 0.251 |
| Highest | 78 (20.1) | 1 | 1 | ||
| Perception of HPV-2 vaccine | |||||
| Good perception | 147 (37.8) | 1.84 (1.13–3.01) | 0.015 | 1.58 (0.88–2.84) | 0.124 |
| Poor perception | 242 (62.2) | 1 | 1 | ||
| Attitude towards HPV-2 vaccine | |||||
| Positive attitude | 219 (56.3) | 2.24 (1.33–3.79) | 0.003 | 2.04 (1.10–3.76) | 0.023 |
| Negative attitude | 170 (43.7) | 1 | 1 | ||
| Awareness of HPV-2 vaccine | |||||
| Heard about HPV vaccine | 322 (82.8) | 10.92 (2.62–45.62) | 0.001 | 9.16 (2.11–39.85) | 0.003 |
| Not heard about HPV vaccine | 67 (17.2) | 1 | 1 | ||
| Knowledge of HPV-2 vaccine | |||||
| Good knowledge | 186 (48.2) | 1.67 (1.02–2.73) | 0.041 | 1.05 (0.56–1.95) | 0.878 |
| Poor knowledge | 203 (52.2) | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nhumba, N.; Sunguya, B. Low Uptake of the Second Dose of Human Papillomavirus Vaccine in Dar es Salaam, Tanzania. Vaccines 2022, 10, 1919. https://doi.org/10.3390/vaccines10111919
Nhumba N, Sunguya B. Low Uptake of the Second Dose of Human Papillomavirus Vaccine in Dar es Salaam, Tanzania. Vaccines. 2022; 10(11):1919. https://doi.org/10.3390/vaccines10111919
Chicago/Turabian StyleNhumba, Nchang’wa, and Bruno Sunguya. 2022. "Low Uptake of the Second Dose of Human Papillomavirus Vaccine in Dar es Salaam, Tanzania" Vaccines 10, no. 11: 1919. https://doi.org/10.3390/vaccines10111919