
Prophylactic Human Papillomavirus Vaccination: From the Origin to the Current State
 , and
, and 
Abstract
:1. Introduction
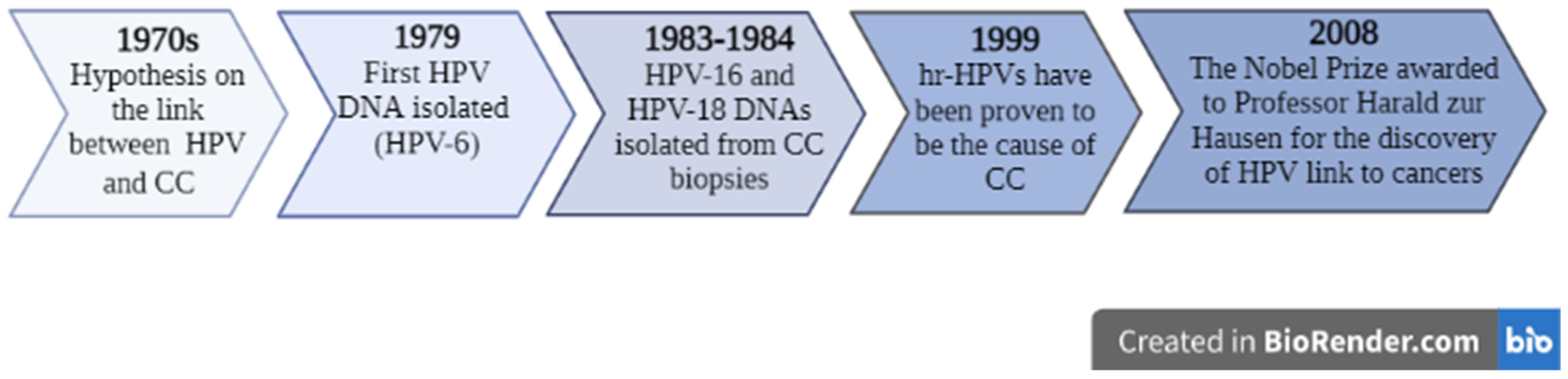
2. Harald zur Hausen’s Investigations on HPV
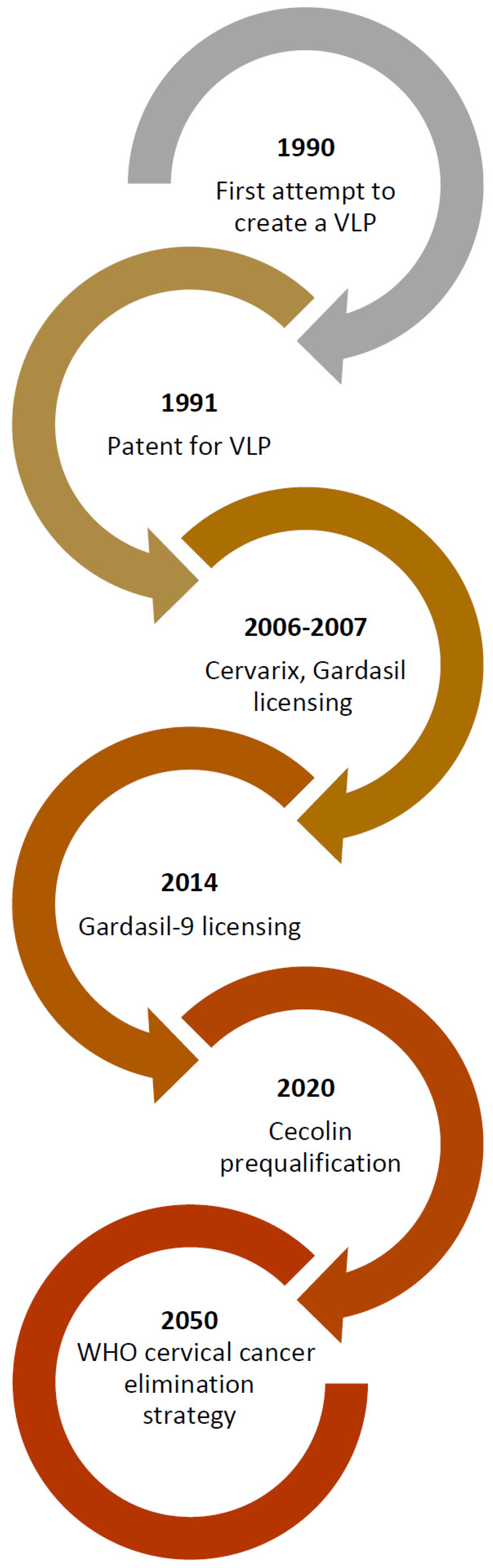
3. Prophylactic HPV Vaccine Development
4. Prophylactic HPV Vaccines’ Mechanism of Action
5. Prophylactic HPV Vaccines: Types, Safety, and Immunogenicity
5.1. Types
5.1.1. Bivalent Prophylactic HPV Vaccines: Cervarix and Cecolin
Cervarix
Cecolin
5.1.2. Quadrivalent Prophylactic HPV Vaccine: Gardasil
5.1.3. Nonavalent Prophylactic HPV Vaccine: Gardasil-9
5.2. Safety
5.3. Immunogenicity
6. Vaccine Dosing Regimens
6.1. Three-Dose Schedule
6.2. Two-Dose Schedule
6.3. Single-Dose Schedule
7. Implementation of Prophylactic HPV Vaccination
8. Myths about HPV Vaccination
9. Challenges and Further Steps in Increasing Preventative HPV Vaccination Coverage
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nicol, A.F.; Andrade, C.V.; Russomano, F.B.; Rodrigues, L.L.; Oliveira, N.S.; Provance, D.W., Jr. HPV vaccines: A controversial issue? Braz. J. Med. Biol. Res. 2016, 49, e5060. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, C.-L.; Lin, Z.-J.; Bi, Z.-F.; Qiu, L.-X.; Hu, F.-F.; Liu, X.-H.; Lin, B.-Z.; Su, Y.-Y.; Pan, H.-R.; Zhang, T.-Y.; et al. Inflammation-related adverse reactions following vaccination potentially indicate a stronger immune response. Emerg. Microbes Infect. 2021, 10, 365–375. [Google Scholar] [CrossRef]
- World Health Organization. Vaccines and Immunization. 2022. Available online: https://www.who.int/health-topics/vaccines-and-immunization#tab=tab_1 (accessed on 6 February 2021).
- Zur Hausen, H. Papillomaviruses and cancer: From basic studies to clinical application. Nat. Rev. Cancer 2002, 2, 342–350. [Google Scholar] [CrossRef]
- Zur Hausen, H. Papillomaviruses in the causation of human cancers—A Brief historical account. Virology 2009, 384, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Frazer, I.H. Cervical cancer vaccine development. Sex. Health 2010, 7, 230–234. [Google Scholar] [CrossRef]
- Harper, D.M.; DeMars, L.R. HPV Vaccines—A review of the first decade. Gynecol. Oncol. 2017, 146, 196–204. [Google Scholar] [CrossRef] [Green Version]
- Aimagambetova, G.; Babi, A.; Issa, T.; Issanov, A. What Factors Are Associated with Attitudes towards HPV Vaccination among Kazakhstani Women? Exploratory Analysis of Cross-Sectional Survey Data. Vaccines 2022, 10, 824. [Google Scholar] [CrossRef]
- Issa, T.; Babi, A.; Issanov, A.; Akilzhanova, A.; Nurgaliyeva, K.; Abugalieva, Z.; Azizan, A.; Khan, S.A.; Chan, C.K.; Alibekova, R.; et al. Knowledge and awareness of human papillomavirus infection and human papillomavirus vaccine among Kazakhstani women attending gynecological clinics. PLoS ONE 2021, 16, e0261203. [Google Scholar] [CrossRef]
- De Oliveira, C.M.; Fregnani, J.H.T.; Villa, L.L. HPV Vaccine: Updates and Highlights. Acta Cytol. 2019, 63, 159–168. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. HPV-Associated Cancer Statistics. Available online: https://www.cdc.gov/cancer/hpv/statistics/index.htm (accessed on 14 September 2022).
- Spayne, J.; Hesketh, T. Estimate of global human papillomavirus vaccination coverage: Analysis of country-level indicators. BMJ Open 2021, 11, e052016. [Google Scholar] [CrossRef]
- Hancock, G.; Hellner, K.; Dorrell, L. Therapeutic HPV vaccines. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 59–72. [Google Scholar] [CrossRef]
- Akhatova, A.; Chan, C.K.; Azizan, A.; Aimagambetova, G. The Efficacy of Therapeutic DNA Vaccines Expressing the Human Papillomavirus E6 and E7 Oncoproteins for Treatment of Cervical Cancer: Systematic Review. Vaccines 2021, 10, 53. [Google Scholar] [CrossRef]
- Wang, R.; Pan, W.; Jin, L.; Huang, W.; Li, Y.; Wu, D.; Gao, C.; Ma, D.; Liao, S. Human papillomavirus vaccine against cervical cancer: Opportunity and challenge. Cancer Lett. 2020, 471, 88–102. [Google Scholar] [CrossRef]
- Bruni, L.; Diaz, M.; Barrionuevo-Rosas, L.; Herrero, R.; Bray, F.; Bosch, F.X.; de Sanjosé, S.; Castellsagué, X. Global estimates of human papillomavirus vaccination coverage by region and income level: A pooled analysis. Lancet Glob. Health 2016, 4, e453–e463, Erratum in: Lancet Glob. Health 2017, 5, e662. [Google Scholar] [CrossRef] [Green Version]
- Bruni, L.; Saura-Lázaro, A.; Montoliu, A.; Brotons, M.; Alemany, L.; Diallo, M.S.; Afsar, O.Z.; LaMontagne, D.S.; Mosina, L.; Contreras, M.; et al. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Prev. Med. 2021, 144, 106399. [Google Scholar] [CrossRef]
- Scotto, J.; Bailar, I.J.C. Rigoni-Stern and Medical Statistics. A Nineteenth-Century Approach to Cancer Research. J. Hist. Med. Allied Sci. 1969, 24, 65–75. [Google Scholar] [CrossRef]
- Frazer, I.H. The HPV Vaccine Story. ACS Pharmacol. Transl. Sci. 2019, 2, 210–212. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, E.L.; Schiller, J.T. Human Papillomavirus Vaccines. J. Infect. Dis. 2021, 224 (Suppl. 2), S367–S378. [Google Scholar] [CrossRef]
- Hausen, H.Z. Papillomaviruses—To vaccination and beyond. Biochemistry 2008, 73, 498–503. [Google Scholar] [CrossRef]
- Hausen, H.Z. Papillomaviruses in Human Cancers. Proc. Assoc. Am. Physicians 1999, 111, 581–587. [Google Scholar] [CrossRef]
- Gissmann, L.; Boshart, M.; Durst, M.; Ikenberg, H.; Wagner, D.; Hausen, H.Z. Presence of Human Papillomavirus in Genital Tumors. J. Investig. Dermatol. 1984, 83 (Suppl. 1), 26s–28s. [Google Scholar] [CrossRef]
- Hausen, H.Z.; Meinhof, W.; Scheiber, W.; Bornkamm, G.W. Attempts to detect virus-specific DNA in human tumors. I. Nucleic acid hybridizations with complementary RNA of human wart virus. Int. J. Cancer 1974, 13, 650–656. [Google Scholar] [CrossRef]
- Hausen, H.Z.; Schulte-Holthausen, H.; Wolf, H.; Dörries, K.; Egger, H. Attempts to detect virus-specific DNA in human tumors. II. Nucleic acid hybridizations with complementary RNA of human herpes group viruses. Int. J. Cancer 1974, 13, 657–664. [Google Scholar] [CrossRef] [Green Version]
- The Nobel Prize. The Nobel Prize in Physiology or Medicine 2008. Available online: https://www.nobelprize.org/prizes/medicine/2008/summary/ (accessed on 21 September 2022).
- The Nobel Prize. Harald zur Hausen. Available online: https://www.nobelprize.org/prizes/medicine/2008/hausen/biographical/ (accessed on 21 September 2022).
- Hausen, H.Z.; de Villiers, E.-M.; Gissmann, L. Papillomavirus infections and human genital cancer. Gynecol. Oncol. 1981, 12 Pt 2, S124–S128. [Google Scholar] [CrossRef]
- De Villiers, E.M.; Gissmann, L.; Hausen, H.Z. Molecular cloning of viral DNA from human genital warts. J. Virol. 1981, 40, 932–935. [Google Scholar] [CrossRef] [Green Version]
- Gissmann, L.; Wolnik, L.; Ikenberg, H.; Koldovsky, U.; Schnürch, H.G.; Hausen, H.Z. Human papillomavirus types 6 and 11 DNA sequences in genital and laryngeal papillomas and in some cervical cancers. Proc. Natl. Acad. Sci. USA 1983, 80, 560–563. [Google Scholar] [CrossRef] [Green Version]
- Dürst, M.; Gissmann, L.; Ikenberg, H.; Zur Hausen, H.Z. A papillomavirus DNA from a cervical carcinoma and its prevalence in cancer biopsy samples from different geographic regions. Proc. Natl. Acad. Sci. USA 1983, 80, 3812–3815. [Google Scholar] [CrossRef] [Green Version]
- Grace, K. Harald zur Hausen’s Experiments on Human Papillomavirus Causing Cervical Cancer (1976–1987). Embryo Proj. Encycl. 2017. Available online: http://embryo.asu.edu/handle/10776/11444 (accessed on 22 September 2022).
- Inglis, S.; Shaw, A.; Koenig, S. Chapter 11: HPV vaccines: Commercial Research & Development. Vaccine 2006, 24 (Suppl. 3), S99–S105. [Google Scholar] [CrossRef]
- Frazer, I.; Crapper, R.; Medley, G.; Brown, T.; Mackay, I. Association between Anorectal Dysplasia, Human Papillomavirus, and Human Immunodeficiency Virus Infection in Homosexual Men. Lancet 1986, 2, 657–660. [Google Scholar] [CrossRef]
- Tindle, R.W.; Frazer, I.H. Immunology of Anogenital Human Papillomavirus (HPV) Infection. Aust. N. Z. J. Obstet. Gynaecol. 1990, 30, 370–375. [Google Scholar] [CrossRef]
- Park, D.S.; Selvey, L.A.; Kelsall, S.R.; Frazer, I.H. Human papillomavirus type 16 E6, E7 and L1 and type 18 E7 proteins produced by recombinant baculoviruses. J. Virol. Methods 1993, 45, 303–318. [Google Scholar] [CrossRef]
- Tindle, R.W.; Zhou, W.D.; Saul, A.; Frazer, I. The molecular specificity of linear B-epitopes in the E7 open reading frame protein of human papillomavirus 16 defined by monoclonal antibodies. Pept. Res. 1990, 3, 162–166. [Google Scholar]
- Zhou, J.; Sun, X.Y.; Stenzel, D.J.; Frazer, I. Expression of vaccinia recombinant HPV 16 L1 and L2 ORF proteins in epithelial cells is sufficient for assembly of HPV virion-like particles. Virology 1991, 185, 251–257. [Google Scholar] [CrossRef]
- Zhou, J.; Sun, X.Y.; Louis, K.; Frazer, I.H. Interaction of human papillomavirus (HPV) type 16 capsid proteins with HPV DNA requires an intact L2 N-terminal sequence. J. Virol. 1994, 68, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Doorbar, J.; Sun, X.Y.; Crawford, L.V.; McLean, C.S.; Frazer, I.H. Identification of the nuclear localization signal of human papillomavirus type 16 L1 protein. Virology 1991, 185, 625–632. [Google Scholar] [CrossRef]
- Zhao, K.-N.; Zhang, L.; Qu, J. Dr. Jian Zhou: The great inventor of cervical cancer vaccine. Protein Cell 2017, 8, 79–82. [Google Scholar] [CrossRef] [Green Version]
- Koutsky, L.A.; Ault, K.A.; Wheeler, C.M.; Brown, D.R.; Barr, E.; Alvarez, F.B.; Chiacchierini, L.M.; Jansen, K.U. A Controlled Trial of a Human Papillomavirus Type 16 Vaccine. N. Engl. J. Med. 2002, 347, 1645–1651. [Google Scholar] [CrossRef]
- European Patent Office. Ian Frazer (Australia), Jian Zhou (China)† Winners of the European Inventor Award 2015. Available online: https://www.epo.org/news-events/events/european-inventor/finalists/2015/frazer.html (accessed on 28 September 2022).
- Markowitz, E.L.; Naleway, A.L.; Klein, N.P.; Lewis, R.M.; Crane, B.; Querec, T.D.; Hsiao, A.; Aukes, L.; Timbol, J.; Weinmann, S.; et al. Human Papillomavirus Vaccine Effectiveness Against HPV Infection: Evaluation of One, Two, and Three Doses. J. Infect. Dis. 2020, 221, 910–918. [Google Scholar] [CrossRef]
- Emberger, J. The HPV Vaccine: Overcoming Barriers to Acceptance of a Medical Triumph. AMA J. Ethics 2015, 17, 854–857. [Google Scholar] [CrossRef] [Green Version]
- Dilley, S.; Miller, K.M.; Huh, W.K. Human papillomavirus vaccination: Ongoing challenges and future directions. Gynecol. Oncol. 2020, 156, 498–502. [Google Scholar] [CrossRef]
- Spinner, C.; Ding, L.; Bernstein, D.I.; Brown, D.R.; Franco, E.L.; Covert, C.; Kahn, J.A. Human Papillomavirus Vaccine Effectiveness and Herd Protection in Young Women. Pediatrics 2019, 143, e20181902. [Google Scholar] [CrossRef]
- Araldi, R.P.; Sant’Ana, T.A.; Módolo, D.G.; de Melo, T.C.; Spadacci-Morena, D.D.; de Cassia Stocco, R.; Cerutti, J.M.; de Souza, E.B. The human papillomavirus (HPV)-related cancer biology: An overview. Biomed. Pharmacother. 2018, 106, 1537–1556. [Google Scholar] [CrossRef] [Green Version]
- Stanley, M. Pathology and epidemiology of HPV infection in females. Gynecol. Oncol. 2010, 117 (Suppl. 2), S5–S10. [Google Scholar] [CrossRef]
- Wang, C.J.; Palefsky, J.M. HPV-Associated Anal Cancer in the HIV/AIDS Patient. Cancer Treat. Res. 2019, 177, 183–209. [Google Scholar] [CrossRef]
- Chan, C.K.; Aimagambetova, G.; Ukybassova, T.; Kongrtay, K.; Azizan, A. Human Papillomavirus Infection and Cervical Cancer: Epidemiology, Screening, and Vaccination—Review of Current Perspectives. J. Oncol. 2019, 2019, 3257939. [Google Scholar] [CrossRef]
- Gravitt, P.E.; Winer, R.L. Natural History of HPV Infection across the Lifespan: Role of Viral Latency. Viruses 2017, 9, 267. [Google Scholar] [CrossRef]
- Narisawa-Saito, M.; Kiyono, T. Basic mechanisms of high-risk human papillomavirus-induced carcinogenesis: Roles of E6 and E7 proteins. Cancer Sci. 2007, 98, 1505–1511. [Google Scholar] [CrossRef]
- Huber, B.; Wang, J.; Roden, R.; Kirnbauer, R. RG1-VLP and Other L2-Based, Broad-Spectrum HPV Vaccine Candidates. J. Clin. Med. 2021, 10, 1044. [Google Scholar] [CrossRef]
- Logel, M.; Laurie, C.; El-Zein, M.; Guichon, J.; Franco, E.L. A Review of Ethical and Legal Aspects of Gender-Neutral Human Papillomavirus Vaccination. Cancer Epidemiol. Biomark. Prev. 2022, 31, 919–931. [Google Scholar] [CrossRef]
- Kamolratanakul, S.; Pitisuttithum, P. Human Papillomavirus Vaccine Efficacy and Effectiveness against Cancer. Vaccines 2021, 9, 1413. [Google Scholar] [CrossRef]
- Llave, C.L.; Uy, M.E.V.; Lam, H.Y.; Aldaba, J.G.; Yacapin, C.C.; Miranda, M.B.; Valverde, H.A.; Silva, W.T.; Nawaz, S.; Slavkovsky, R.C.; et al. The cost-effectiveness of human papillomavirus vaccination in the Philippines. Vaccine 2022, 40, 3802–3811. [Google Scholar] [CrossRef]
- Cecolin Wantai BioPharm Official Web. Available online: http://www.ystwt.cn/cecolin/ (accessed on 8 September 2022).
- PATH. New HPV Vaccine from Innovax Receives WHO Prequalification. 19 October 2021. Available online: https://www.path.org/media-center/new-hpv-vaccine-innovax-receives-who-prequalification/ (accessed on 14 September 2022).
- Food and Drug Administration. Gardasil-9 Package Insert. Available online: https://www.fda.gov/media/90064/download (accessed on 6 September 2022).
- Barzon, L.; Squarzon, L.; Masiero, S.; Pacenti, M.; Marcati, G.; Mantelli, B.; Gabrielli, L.; Pascucci, M.G.; Lazzarotto, T.; Caputo, A.; et al. Neutralizing and cross-neutralizing antibody titres induced by bivalent and quadrivalent human papillomavirus vaccines in the target population of organized vaccination programmes. Vaccine 2014, 32, 5357–5362. [Google Scholar] [CrossRef]
- Food and Drug Administration. Cervarix Package Insert. Available online: https://www.fda.gov/vaccines-blood-biologics/vaccines/cervarix (accessed on 14 September 2022).
- Arbyn, M.; Xu, L.; Simoens, C.; Martin-Hirsch, P.P. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. Cochrane Database Syst. Rev. 2018, 5, CD009069. [Google Scholar] [CrossRef]
- Schauner, S.; Lyon, C. Bivalent HPV Recombinant Vaccine (Cervarix) for the Prevention of Cervical Cancer. Am. Fam. Physician 2010, 82, 1541–1542. [Google Scholar]
- Szarewski, A. HPV Vaccine: Cervarix. Expert Opin. Biol. Ther. 2010, 10, 477–487. [Google Scholar] [CrossRef]
- Isidean, S.D.; Tota, E.J.; Gagnon, A.J.; Franco, E.L. Human papillomavirus vaccines: Key factors in planning cost-effective vaccination programs. Expert Rev. Vaccines 2014, 14, 119–133. [Google Scholar] [CrossRef]
- David, M.-P.; Van Herck, K.; Hardt, K.; Tibaldi, F.; Dubin, G.; Descamps, D.; Van Damme, P. Long-term persistence of anti-HPV-16 and -18 antibodies induced by vaccination with the AS04-adjuvanted cervical cancer vaccine: Modeling of sustained antibody responses. Gynecol. Oncol. 2009, 115 (Suppl. 3), S1–S6. [Google Scholar] [CrossRef]
- Fraser, C.; Tomassini, J.E.; Xi, L.; Golm, G.; Watson, M.; Giuliano, A.R.; Barr, E.; Ault, K.A. Modeling the long-term antibody response of a human papillomavirus (HPV) virus-like particle (VLP) type 16 prophylactic vaccine. Vaccine 2007, 25, 4324–4333. [Google Scholar] [CrossRef]
- WHO—Prequalification of Medical Products (IVDs, Medicines, Vaccines and Immunization Devices, Vector Control). Available online: https://extranet.who.int/pqweb/content/cecolin%C2%AE (accessed on 8 September 2022).
- Zou, Z.; Fairley, C.K.; Ong, J.J.; Hocking, J.; Canfell, K.; Ma, X.; Chow, E.P.F.; Xu, X.; Zhang, L.; Zhuang, G. Domestic HPV vaccine price and economic returns for cervical cancer prevention in China: A cost-effectiveness analysis. Lancet Glob. Health 2020, 8, e1335–e1344. [Google Scholar] [CrossRef]
- Garland, S.M.; Kjaer, S.K.; Muñoz, N.; Block, S.L.; Brown, D.R.; DiNubile, M.J.; Lindsay, B.R.; Kuter, B.J.; Perez, G.; Dominiak-Felden, G.; et al. Impact and Effectiveness of the Quadrivalent Human Papillomavirus Vaccine: A Systematic Review of 10 Years of Real-world Experience. Clin. Infect. Dis. 2016, 63, 519–527. [Google Scholar] [CrossRef]
- Castle, P.E.; Maza, M. Prophylactic HPV Vaccination: Past, present, and future. Epidemiol. Infect. 2016, 144, 449–468, Erratum in: Epidemiol. Infect. 2016, 144, 2472. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administartion. Gardasil Package Insert. Available online: https://www.fda.gov/files/vaccines,%20blood%20&%20biologics/published/Package-Insert---Gardasil.pdf. (accessed on 14 September 2022).
- McCormack, P.L. Quadrivalent Human Papillomavirus (Types 6, 11, 16, 18) Recombinant Vaccine (Gardasil®): A Review of Its Use in the Prevention of Premalignant Anogenital Lesions, Cervical and Anal Cancers, and Genital Warts. Drugs 2014, 74, 1253–1283. [Google Scholar] [CrossRef]
- Dobson, S.R.; McNeil, S.; Dionne, M.; Dawar, M.; Ogilvie, G.; Krajden, M.; Sauvageau, C.; Scheifele, D.W.; Kollman, T.R.; Halperin, S.A.; et al. Immunogenicity of 2 doses of HPV vaccine in younger adolescents vs 3 doses in young women: A randomized clinical trial. JAMA 2013, 309, 1793–1802. [Google Scholar]
- Petrosky, E.; Bocchini, J.A., Jr.; Hariri, S.; Chesson, H.; Curtis, C.R.; Saraiya, M.; Unger, E.R.; Markowitz, L.E.; Centers for Disease Control and Prevention (CDC). Use of 9-Valent Human Papillomavirus (HPV) Vaccine: Updated HPV Vaccination Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 300–304. [Google Scholar]
- Du, J.; Ährlund-Richter, A.; Näsman, A.; Dalianis, T. Human papilloma virus (HPV) prevalence upon HPV vaccination in Swedish youth: A review based on our findings 2008–2018, and perspectives on cancer prevention. Arch. Gynecol. Obstet. 2021, 303, 329–335. [Google Scholar] [CrossRef]
- Dadar, M.; Chakraborty, S.; Dhama, K.; Prasad, M.; Khandia, R.; Hassan, S.; Munjal, A.; Tiwari, R.; Karthik, K.; Kumar, D.; et al. Advances in Designing and Developing Vaccines, Drugs and Therapeutic Approaches to Counter Human Papilloma Virus. Front. Immunol. 2018, 9, 2478. [Google Scholar] [CrossRef]
- Arbyn, M.; Xu, L. Efficacy and safety of prophylactic HPV vaccines. A Cochrane review of randomized trials. Expert Rev. Vaccines 2018, 17, 1085–1091. [Google Scholar] [CrossRef]
- World Health Organization. Human Papillomavirus Vaccines Safety. Available online: https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/human-papillomavirus-vaccines/safety (accessed on 7 September 2022).
- Villa, A.; Patton, L.L.; Giuliano, A.R.; Estrich, C.G.; Pahlke, S.C.; O’Brien, K.K.; Lipman, R.D.; Araujo, M.W. Summary of the evidence on the safety, efficacy, and effectiveness of human papillomavirus vaccines: Umbrella review of systematic reviews. J. Am. Dent. Assoc. 2020, 151, 245–254. [Google Scholar] [CrossRef]
- Quattrone, F.; Canale, A.; Filippetti, E.; Tulipani, A.; Porretta, A.; Lopalco, P.L. Safety of HPV Vaccines in the Age of Nonavalent Vaccination. Minerva Pediatr. 2018, 70, 59–66. [Google Scholar] [CrossRef]
- Gonçalves, A.K.; Cobucci, R.N.; Rodrigues, H.M.; de Melo, A.G.; Giraldo, P.C. Safety, tolerability and side effects of human papillomavirus vaccines: A systematic quantitative review. Braz. J. Infect. Dis. 2014, 18, 651–659. [Google Scholar] [CrossRef] [Green Version]
- Einstein, M.H.; Baron, M.; Levin, M.J.; Chatterjee, A.; Fox, B.; Scholar, S.; Rosen, J.; Chakhtoura, N.; Meric, D.; Dessy, F.J.; et al. Comparative immunogenicity and safety of human papillomavirus (HPV)-16/18 vaccine and HPV-6/11/16/18 vaccine. Hum. Vaccines 2011, 7, 1343–1358. [Google Scholar] [CrossRef] [Green Version]
- Palmieri, B.; Poddighe, D.; Vadalà, M.; Laurino, C.; Carnovale, C.; Clementi, E. Severe somatoform and dysautonomic syndromes after HPV vaccination: Case series and review of literature. Immunol. Res. 2017, 65, 106–116. [Google Scholar] [CrossRef] [Green Version]
- Poddighe, D.; Castelli, L.; Marseglia, G.L.; Bruni, P. A sudden onset of a pseudo-neurological syndrome after HPV-16/18 AS04-adjuvated vaccine: Might it be an autoimmune/inflammatory syndrome induced by adjuvants (ASIA) presenting as a somatoform disorder? Immunol. Res. 2014, 60, 236–246. [Google Scholar] [CrossRef]
- Turner, T.B.; Huh, W.K. HPV vaccines: Translating immunogenicity into efficacy. Hum. Vaccines Immunother. 2016, 12, 1403–1405. [Google Scholar] [CrossRef]
- Schwarz, T.F.; Huang, L.-M.; Valencia, A.; Panzer, F.; Chiu, C.-H.; Decreux, A.; Poncelet, S.; Karkada, N.; Folschweiller, N.; Lin, L.; et al. A ten-year study of immunogenicity and safety of the AS04-HPV-16/18 vaccine in adolescent girls aged 10-14 years. Hum. Vaccines Immunother. 2019, 15, 1970–1979. [Google Scholar] [CrossRef] [Green Version]
- Tota, E.J.; Struyf, F.; Hildesheim, A.; Gonzalez, P.; Ryser, M.; Herrero, R.; Schussler, J.; Karkada, N.; Rodriguez, A.C.; Folschweiller, N.; et al. Efficacy of AS04-Adjuvanted Vaccine Against Human Papillomavirus (HPV) Types 16 and 18 in Clearing Incident HPV Infections: Pooled Analysis of Data from the Costa Rica Vaccine Trial and the PATRICIA Study. J. Infect. Dis. 2021, 223, 1576–1581. [Google Scholar] [CrossRef]
- Porras, C.; Sampson, J.N.; Herrero, R.; Gail, M.H.; Cortés, B.; Hildesheim, A.; Cyr, J.; Romero, B.; Schiller, J.T.; Montero, C.; et al. Rationale and design of a double-blind randomized non-inferiority clinical trial to evaluate one or two doses of vaccine against human papillomavirus including an epidemiologic survey to estimate vaccine efficacy: The Costa Rica ESCUDDO trial. Vaccine 2022, 40, 76–88. [Google Scholar] [CrossRef]
- Stanley, M.A.; Sudenga, S.; Giuliano, A.R. Alternative dosage schedules with HPV virus-like particle vaccines. Expert Rev. Vaccines 2014, 13, 1027–1038. [Google Scholar] [CrossRef]
- Einstein, M.H.; Takacs, P.; Chatterjee, A.; Sperling, R.S.; Chakhtoura, N.; Blatter, M.M.; Lalezari, J.; David, M.-P.; Lin, L.; Struyf, F.; et al. Comparison of long-term immunogenicity and safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine and HPV-6/11/16/18 vaccine in healthy women aged 18-45 years: End-of-study analysis of a Phase III randomized trial. Hum. Vaccines Immunother. 2014, 10, 3435–3445. [Google Scholar] [CrossRef] [Green Version]
- Bergman, H.; Buckley, B.S.; Villanueva, G.; Petkovic, J.; Garritty, C.; Lutje, V.; Riveros-Balta, A.X.; Low, N.; Henschke, N. Comparison of different human papillomavirus (HPV) vaccine types and dose schedules for prevention of HPV-related disease in females and males. Cochrane Database Syst. Rev. 2019, 11, CD013479. [Google Scholar] [CrossRef]
- Hu, Y.-M.; Guo, M.; Li, C.-G.; Chu, K.; He, W.-G.; Zhang, J.; Gu, J.-X.; Li, J.; Zhao, H.; Wu, X.-H.; et al. Immunogenicity noninferiority study of 2 doses and 3 doses of an Escherichia coli-produced HPV bivalent vaccine in girls vs. 3 doses in young women. Sci. China Life Sci. 2019, 63, 582–591. [Google Scholar] [CrossRef]
- Schiller, J.; Lowy, D. Explanations for the high potency of HPV prophylactic vaccines. Vaccine 2018, 36 Pt A, 4768–4773. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Rodriguez, A.C.; Hildesheim, A.; Herrero, R.; Porras, C.; Schiffman, M.; Solomon, D.; Jimenez, S.; Schiller, J.T.; Lowy, D.R.; et al. Proof-of-principle evaluation of the efficacy of fewer than three doses of a bivalent HPV16/18 vaccine. J. Natl. Cancer Inst. 2011, 103, 1444–1451. [Google Scholar]
- Hildesheim, A.; Wacholder, S.; Catteau, G.; Struyf, F.; Dubin, G.; Herrero, R.; CVT Group. Efficacy of the HPV-16/18 vaccine: Final according to protocol results from the blinded phase of the randomized Costa Rica HPV-16/18 vaccine trial. Vaccine 2014, 32, 5087–5097. [Google Scholar] [CrossRef] [Green Version]
- Sankaranarayanan, R.; Prabhu, P.R.; Pawlita, M.; Gheit, T.; Bhatla, N.; Muwonge, R.; Nene, B.M.; Esmy, P.O.; Joshi, S.; Poli, U.R.R.; et al. Immunogenicity and HPV infection after one, two, and three doses of quadrivalent HPV vaccine in girls in India: A multicentre prospective cohort study. Lancet Oncol. 2015, 17, 67–77. [Google Scholar] [CrossRef]
- Porras, C.; Tsang, S.H.; Herrero, R.; Guillén, D.; Darragh, T.M.; Stoler, M.H.; Hildesheim, A.; Wagner, S.; Boland, J.; Lowy, D.R.; et al. Efficacy of the bivalent HPV vaccine against HPV 16/18-associated precancer: Long-term follow-up results from the Costa Rica Vaccine Trial. Lancet Oncol. 2020, 21, 1643–1652. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Herrero, R.; Sampson, J.N.; Porras, C.; Lowy, D.R.; Schiller, J.T.; Schiffman, M.; Rodriguez, A.C.; Chanock, S.; Jimenez, S.; et al. Evidence for single-dose protection by the bivalent HPV vaccine—Review of the Costa Rica HPV vaccine trial and future research studies. Vaccine 2018, 36 Pt A, 4774–4782. [Google Scholar] [CrossRef]
- Herweijer, E.; Sundström, K.; Ploner, A.; Uhnoo, I.; Sparén, P.; Arnheim-Dahlström, L. Quadrivalent HPV vaccine effectiveness against high-grade cervical lesions by age at vaccination: A population-based study. Int. J. Cancer 2016, 138, 2867–2874. [Google Scholar] [CrossRef] [Green Version]
- Walling, E.B.; Dodd, S.; Bobenhouse, N.; Reis, E.C.; Sterkel, R.; Garbutt, J. Implementation of Strategies to Improve Human Papillomavirus Vaccine Coverage: A Provider Survey. Am. J. Prev. Med. 2019, 56, 74–83. [Google Scholar] [CrossRef]
- Iversen, O.-E.; Miranda, M.J.; Ulied, A.; Soerdal, T.; Lazarus, E.; Chokephaibulkit, K.; Block, S.L.; Skrivanek, A.; Azurah, A.G.N.; Fong, S.M.; et al. Immunogenicity of the 9-Valent HPV Vaccine Using 2-Dose Regimens in Girls and Boys vs. a 3-Dose Regimen in Women. JAMA 2016, 316, 2411–2421. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Sampson, J.N.; Porras, C.; Schiller, J.T.; Kemp, T.; Herrero, R.; Wagner, S.; Boland, J.; Schussler, J.; Lowy, D.R.; et al. Evaluation of Durability of a Single Dose of the Bivalent HPV Vaccine: The CVT Trial. J. Natl. Cancer Inst. 2020, 112, 1038–1046. [Google Scholar] [CrossRef] [Green Version]
- PAHO/WHO—Human Papillomavirus (HPV) Vaccine. One-Dose Human Papillomavirus (HPV) Vaccine Offers Solid Protection against Cervical Cancer. Available online: https://www.paho.org/en/news/11-4-2022-one-dose-human-papillomavirus-hpv-vaccine-offers-solid-protection-against-cervical (accessed on 12 October 2022).
- Bosch, F.X.; Robles, C.; Díaz, M.; Arbyn, M.; Baussano, I.; Clavel, C.; Ronco, G.; Dillner, J.; Lehtinen, M.; Petry, K.-U.; et al. HPV-FASTER: Broadening the scope for prevention of HPV-related cancer. Nat. Rev. Clin. Oncol. 2016, 13, 119–132. [Google Scholar] [CrossRef]
- Bosch, F.X.; Robles, C. HPV-FASTER: Combined strategies of HPV vaccination and HPV screening towards a one visit for cervical cancer preventive campaigns. Salud Publica Mex. 2018, 60, 612–616. [Google Scholar] [CrossRef] [Green Version]
- León-Maldonado, L.; Cabral, A.; Brown, B.; Ryan, G.W.; Maldonado, A.; Salmerón, J.; Allen-Leigh, B.; Lazcano-Ponce, E. Feasibility of a combined strategy of HPV vaccination and screening in Mexico: The FASTER-Tlalpan study experience. Hum. Vaccines Immunother. 2019, 15, 1986–1994. [Google Scholar] [CrossRef]
- Brotherton, J.M. Impact of HPV vaccination: Achievements and future challenges. Papillomavirus Res. 2019, 7, 138–140. [Google Scholar] [CrossRef]
- Patel, C.; Brotherton, J.M.; Pillsbury, A.; Jayasinghe, S.; Donovan, B.; Macartney, K.; Marshall, H. The impact of 10 years of human papillomavirus (HPV) vaccination in Australia: What additional disease burden will a nonavalent vaccine prevent? Eurosurveillance 2018, 23, 1700737. [Google Scholar] [CrossRef] [Green Version]
- Drolet, M.; Laprise, J.-F.; Brotherton, J.M.L.; Donovan, B.; Fairley, C.K.; Ali, H.; Bénard, É.; Martin, D.; Brisson, M. The Impact of Human Papillomavirus Catch-Up Vaccination in Australia: Implications for Introduction of Multiple Age Cohort Vaccination and Postvaccination Data Interpretation. J. Infect. Dis. 2017, 216, 1205–1209. [Google Scholar] [CrossRef] [Green Version]
- Drolet, M.; Bénard, É.; Boily, M.-C.; Ali, H.; Baandrup, L.; Bauer, H.; Beddows, S.; Brisson, J.; Brotherton, J.M.L.; Cummings, T.; et al. Population-level impact and herd effects following human papillomavirus vaccination programmes: A systematic review and meta-analysis. Lancet Infect. Dis. 2015, 15, 565–580. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, J.C.; Roteli-Martins, C.M. HPV Vaccines: Separating Myths from Reality. Rev. Bras. Ginecol. Obstet. 2019, 41, 417–418. [Google Scholar] [CrossRef] [Green Version]
- Patel, H.; Wilson, E.; Vizzotti, C.; Parston, G.; Prestt, J.; Darzi, A. Argentina’s Successful Implementation of a National Human Papillomavirus Vaccination Program. Health Aff. 2016, 35, 301–308. [Google Scholar] [CrossRef]
- Ortu, G.; Barret, A.-S.; Danis, K.; Duchesne, L.; Levy-Bruhl, D.; Velter, A. Low vaccination coverage for human papillomavirus disease among young men who have sex with men, France, 2019. Eurosurveillance 2021, 26, 2001965. [Google Scholar] [CrossRef]
- Escriva-Boulley, G.; Mandrik, O.; Préau, M.; Herrero, R.; Villain, P. Cognitions and behaviours of general practitioners in France regarding HPV vaccination: A theory-based systematic review. Prev. Med. 2021, 143, 106323. [Google Scholar] [CrossRef]
- Haut Conseil de la Santé Publique (HCSP). Recommandations Vaccinales contre les Infections à Papillomavirus Humains chez les Hommes; [Vaccination Recommendations against Human Papillomavirus Infections in Men]; HCSP: Paris, France, 2016; Available online: https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=553 (accessed on 20 September 2022).
- Karafillakis, E.; Peretti-Watel, P.; Verger, P.; Chantler, T.; Larson, H. “We don’t have the same bodies; we don’t react the same way”: Mothers and Adolescent Girls’ Perceptions of the Risks and Benefits of HPV Vaccination in France. Hum. Vaccines Immunother. 2022, 18, 2036555. [Google Scholar] [CrossRef]
- Grigore, M.; Teleman, S.I.; Pristavu, A.; Matei, M. Awareness and Knowledge About HPV and HPV Vaccine Among Romanian Women. J. Cancer Educ. 2018, 33, 154–159. [Google Scholar] [CrossRef]
- Diaconescu, L.V.; Gheorghe, I.R.; Cheşcheş, T.; Popa-Velea, O. Psychological Variables Associated with HPV Vaccination Intent in Romanian Academic Settings. Int. J. Environ. Res. Public Health 2021, 18, 8938. [Google Scholar] [CrossRef]
- Dorleans, F.; Giambi, C.; Dematte, L.; Cotter, S.; Stefanoff, P.; Mereckiene, J.; O’Flanagan, D.; Lopalco, P.L.; D’Ancona, F.; Lévy-Bruhl, D. The current state of introduction of human papillomavirus vaccination into national immunisation schedules in Europe: First results of the VENICE2 2010 survey. Eurosurveillance 2010, 15, 19730. [Google Scholar]
- Hanley, S.J.B.; Yoshioka, E.; Ito, Y.; Kishi, R. HPV vaccination crisis in Japan. Lancet 2015, 385, 2571. [Google Scholar] [CrossRef] [Green Version]
- Penţa, M.A.; Băban, A. Mass media coverage of HPV vaccination in Romania: A content analysis. Health Educ. Res. 2014, 29, 977–992. [Google Scholar] [CrossRef] [Green Version]
- Bednarczyk, R.A. Addressing HPV vaccine myths: Practical information for healthcare providers. Hum. Vaccines Immunother. 2019, 15, 1628–1638. [Google Scholar] [CrossRef]
- Katz, A. CE: Human Papillomavirus-Related Oral Cancers: The Nurse’s Role in Mitigating Stigma and Dispelling Myths. Am. J. Nurs. 2017, 117, 34–39. [Google Scholar] [CrossRef]
- Taumberger, N.; Joura, A.E.; Arbyn, M.; Kyrgiou, M.; Sehouli, J.; Gultekin, M. Myths and fake messages about human Papillomavirus (HPV) vaccination: Answers from the ESGO Prevention Committee. Int. J. Gynecol. Cancer 2022, 32, 1316–1320. [Google Scholar] [CrossRef]
- World Health Organization. Cervical Cancer. Available online: https://www.who.int/health-topics/cervical-cancer#tab=tab_1 (accessed on 12 October 2022).
- Brisson, M.; Kim, J.J.; Canfell, K.; Drolet, M.; Gingras, G.; Burger, A.E.; Martin, D.; Simms, K.T.; Bénard, É.; Boily, M.-C.; et al. Impact of HPV vaccination and cervical screening on cervical cancer elimination: A comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet 2020, 395, 575–590. [Google Scholar] [CrossRef] [Green Version]
- Yadav, R.; Zhai, L.; Tumban, E. Virus-like Particle-Based L2 Vaccines against HPVs: Where Are We Today? Viruses 2019, 12, 18. [Google Scholar] [CrossRef] [Green Version]
- Yadav, R.; Zhai, L.; Kunda, N.; Muttil, P.; Tumban, E. Mixed Bacteriophage MS2-L2 VLPs Elicit Long-Lasting Protective Antibodies against HPV Pseudovirus 51. Viruses 2021, 13, 1113. [Google Scholar] [CrossRef]
- Rossi, I.; Spagnoli, G.; Buttini, F.; Sonvico, F.; Stellari, F.; Cavazzini, D.; Chen, Q.; Müller, M.; Bolchi, A.; Ottonello, S.; et al. A respirable HPV-L2 dry-powder vaccine with GLA as amphiphilic lubricant and immune-adjuvant. J. Control. Release 2021, 340, 209–220. [Google Scholar] [CrossRef]
- Vujadinovic, M.; Khan, S.; Oosterhuis, K.; Uil, T.G.; Wunderlich, K.; Damman, S.; Boedhoe, S.; Verwilligen, A.; Knibbe, J.; Serroyen, J.; et al. Adenovirus based HPV L2 vaccine induces broad cross-reactive humoral immune responses. Vaccine 2018, 36, 4462–4470. [Google Scholar] [CrossRef]
- Newman, A.P.; Logie, C.H.; Doukas, N.; Asakura, K. HPV vaccine acceptability among men: A systematic review and meta-analysis. Sex. Transm. Infect. 2013, 89, 568–574. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Vaccine Type | HPV Types/L1 Included | Brand Name | Producer | Eligible Group | Indications | Ref |
|---|---|---|---|---|---|---|
| Bivalent | HPV-16; HPV-18 | Cervarix | GSK, Rixensart, Belgium | Girls and women 9–25 years | Prevention of cervical cancer, CIN grade I-III and AIS, caused by HPV types 16 and 18. | [62] |
| Cecolin | Xiamen Innovax Biotech Co., Ltd., Xiamen, China | Girls and women 9–45 years | Prevention of cervical cancer, CIN grade I-III and AIS, caused by HPV types 16 and 18. | [69] | ||
| Quadrivalent | HPV-6; HPV-11; HPV-16; HPV-18 | Gardasil | Merck Co. Inc., Rahway, NJ, USA | Girls and women 9–26 years | Prevention of: 1. Vulvar and vaginal cancer; 2. Cervical cancer; 3. Genital warts; 4. CIN grade I-III; 5. Cervical AIS; 6. VIN grade II-III; 7. VaIN grade II-III; 8. AIN grades I-III. | [73] |
| Boys and men 9–26 years | Prevention of: 1. Genital warts caused by HPV types 6 and 11; 2. Anal cancer and associated precancerous lesions linked to HPV types 6, 11, 16, and 18. | [73] | ||||
| Nonavalent | HPV-6; HPV-11; HPV-16; HPV-18; HPV-31; HPV-33; HPV-45; HPV-52; HPV-58 | Gardasil-9 | Merck Sharp & Dohme Corp., Whitehouse Station, NJ, USA | Girls and women 9–45 years | Prevention of: 1.Cervical, vulvar, vaginal, anal, oropharyngeal, and other head and neck cancers, which are caused by HPV types 16, 18, 31, 33, 45, 52, and 58; 2.Genital warts caused by HPV types 6 and 11; 3.CIN grade I-III; 4.Cervical AIS; 5.VIN grade II-III; 6.VaIN grade II-III; 7.AIN grades I-III. | [60] |
| Boys and men 9–45 years | Prevention of: 1. Anal, oropharyngeal, and other head and neck cancers caused by HPV types 16, 18, 31, 33, 45, 52, and 58; 2. Genital warts caused by HPV types 6 and 11; 3. AIN grades I-III. | [60] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akhatova, A.; Azizan, A.; Atageldiyeva, K.; Ashimkhanova, A.; Marat, A.; Iztleuov, Y.; Suleimenova, A.; Shamkeeva, S.; Aimagambetova, G. Prophylactic Human Papillomavirus Vaccination: From the Origin to the Current State. Vaccines 2022, 10, 1912. https://doi.org/10.3390/vaccines10111912
Akhatova A, Azizan A, Atageldiyeva K, Ashimkhanova A, Marat A, Iztleuov Y, Suleimenova A, Shamkeeva S, Aimagambetova G. Prophylactic Human Papillomavirus Vaccination: From the Origin to the Current State. Vaccines. 2022; 10(11):1912. https://doi.org/10.3390/vaccines10111912
Chicago/Turabian StyleAkhatova, Ayazhan, Azliyati Azizan, Kuralay Atageldiyeva, Aiymkul Ashimkhanova, Aizada Marat, Yerbolat Iztleuov, Assem Suleimenova, Saikal Shamkeeva, and Gulzhanat Aimagambetova. 2022. "Prophylactic Human Papillomavirus Vaccination: From the Origin to the Current State" Vaccines 10, no. 11: 1912. https://doi.org/10.3390/vaccines10111912