

Reactogenicity and Humoral Immune Response after Heterologous Vaxzevria/Comirnaty Vaccination in a Group of Individuals Vaccinated in the AOU Policlinic “G. Martino” (Messina, Italy): A Retrospective Cohort Study
 , and
, and
Abstract
:1. Introduction
- (a)
- An evaluation of the reactogenicity of the heterologous COVID-19 vaccination, searching for undesirable effects reported by the vaccinated people after the administration of the first dose of the Vaxzevria vaccine and after the administration of the second dose of the Comirnaty vaccine, as well as the presence of statistically significant associations with age, sex, and comorbidities.
- (b)
- An evaluation of the antibody response after 28 days from the administration of the second dose, searching for the presence of statistically significant associations with age, sex, and comorbidities.
- (c)
- A comparison of the antibody responses after the homologous and heterologous vaccination regimens.
2. Materials and Methods
2.1. Inclusion Criteria
- –
- Age ≥ 18 years.
- –
- Administration of a dose of Vaxzevria vaccine.
- –
- Administration of a dose of Comirnaty vaccine for completing the vaccination course in the AOU Policlinic “G. Martino” (Messina, Italy).
- –
- Administration of a questionnaire before the administration of the Comirnaty vaccine and a week after the administration of the Comirnaty vaccine.
2.2. Evaluation of Reactogenicity
- (a)
- The first one regarded sociodemographic characteristics (Section 1).
- (b)
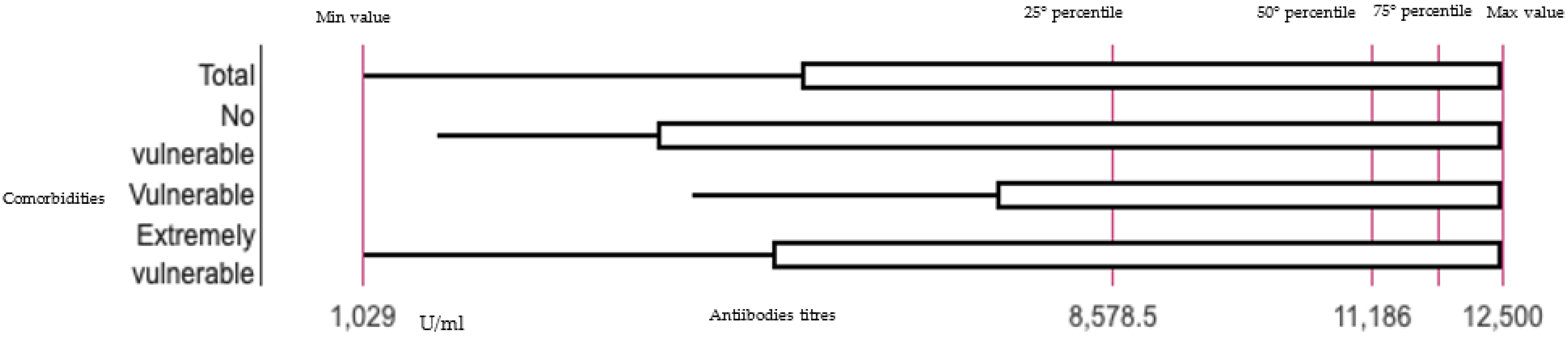
- The second one concerned the presence of comorbidities (Section 2). We divided the enrolled individuals into non-vulnerable, vulnerable, and extremely vulnerable. This classification was based on a table developed by the Sicilian region, defining as extremely vulnerable the individuals affected by some conditions characterized by pre-existing organ damage or by an immune deficiency, with a particularly elevated risk of developing severe or lethal forms of COVID-19. Vulnerable individuals were considered those with at least a chronic disease not included in the previous category. Finally, non-vulnerable individuals were those with no chronic diseases.
- (c)
- The third one concerned the presence of undesirable effects reported within 7 days of vaccine administration (Section 3).
2.3. Evaluation of Humoral Immune Response
2.4. Statistical Analysis
3. Results
Evaluation of the Humoral Immune Response
4. Discussion
4.1. Reactogenicity and Humoral Immune Response
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jameson, J.L.; Kasper, D.L.; Longo, D.L.; Fauci, A.S.; Hauser, S.L.; Loscalzo, J. Parte quinta. Harrison. Principi di medicina interna., 20th ed.; Casa Editrice Ambrosiana: Milano, Italy, 2021; Online Issue. [Google Scholar]
- WHO. COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 17 October 2022).
- Olliaro, P.; Torreele, E.; Vaillant, M. COVID-19 vaccine efficacy and effectiveness-the elephant (not) in the room. Lancet Microbe. 2021, 2, e279–e280. [Google Scholar] [CrossRef]
- AIFA. Precautionary Suspension of the AstraZeneca Vaccine. Comunicate Number 637 of 15th March 2021. Available online: https://www.aifa.gov.it/documents/20142/1289678/Comunicato_AIFA_637.pdf (accessed on 17 October 2022).
- AIFA. Communicate. Available online: https://www.aifa.gov.it/-/dopo-parere-ema-domani-riprendono-vaccinazioni-con-astrazeneca (accessed on 17 October 2022).
- Ministry of Health. Prot Number 14358 of 07/04/2021. Vaxzevria Vaccine (Formerly COVID-19 Vaccine AstraZeneca). Update Recommendations; Ministry of Health: Rome, Italy, 2021.
- Ministry of Health. Circular Note Prot Number 26246 of 11/06/2021. Vaccines Opinion Update; Ministry of Health: Rome, Italy, 2021.
- European Medicines Agency. EMA and ECDC Recommendations on Heterologous Vaccination Courses against COVID-19: ‘Mix-and-Match’ Approach Can Be Used for Both Initial Courses and Boosters. Available online: https://www.ema.europa.eu/en/news/ema-ecdc-recommendations-heterologous-vaccination-courses-against-covid-19-mix-match-approach-can-be (accessed on 2 February 2022).
- D’Amato, S.; Squeri, R.; La Fauci, V.; Pantò, G.; Esposito, E.M.; Denaro, F.; Visalli, G.; Giunta, I.; Venuto, R.; Privitera, A.; et al. COVID-19 serological evaluation in a cohort of Vaccinated and Seropositive healthcare workers. Acta Biomed. 2021, 92 (Suppl. 6), e2021415. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Shaw, R.H.; Stuart, A.S.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Safety and immunogenicity of heterologous versus homologous prime-boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): A single-blind, randomised, non-inferiority trial. Lancet 2021, 398, 856–869. [Google Scholar] [CrossRef]
- Shaw, R.H.; Stuart, A.; Greenland, M.; Liu, X.; Nguyen Van-Tam, J.S.; Snape, M.D.; Com-COV Study Group. Heterologous prime-boost COVID-19 vaccination: Initial reactogenicity data. Lancet 2021, 397, 2043–2046. [Google Scholar] [CrossRef]
- EudraVigilance. Available online: https://dap.ema.europa.eu/analytics/saw.dll?PortalPages (accessed on 23 September 2022).
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Ahmet’Yanov, M.; Reikhert, L.; Kicherova, O.; Deeva, M.; Makarova, D. Sleep Disorders in Patients After COVID-19. Zhurnal Nevrol. I Psikhiatrii Im. S.S. Korsakova 2021, 121, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Li, S.X.; Xue, P.; Zhou, J.; Tang, X. COVID-19 Vaccine Could Trigger the Relapse of Secondary Hypersomnia. Nat. Sci. Sleep 2021, 13, 2267–2271. [Google Scholar] [CrossRef] [PubMed]
- Heidari, S.; Palmer-Ross, A.; Goodman, T. A Systematic Review of the Sex and Gender Reporting in COVID-19 Clinical Trials. Vaccines 2021, 9, 1322. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.S.; Cheong, H.J. COVID-19 Vaccination for People with Comorbidities. Infect. Chemother. 2021, 53, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Stuart, A.S.; Shaw, R.H.; Liu, X.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Immunogenicity, safety, and reactogenicity of heterologous COVID-19 primary vaccination incorporating mRNA, viral-vector, and protein-adjuvant vaccines in the UK (Com-COV2): A single-blind, randomised, phase 2, non-inferiority trial. Lancet 2022, 399, 36–49. [Google Scholar] [CrossRef]
- Ganesan, S.; Al Ketbi, L.M.B.; Al Kaabi, N.; Al Mansoori, M.; Al Maskari, N.N.; Al Shamsi, M.S.; Alderei, A.S.; El Eissaee, H.N.; Al Ketbi, R.M.; Al Shamsi, N.S.; et al. Vaccine Side Effects Following COVID-19 Vaccination Among the Residents of the UAE-An Observational Study. Front. Public Health 2022, 10, 876336. [Google Scholar] [CrossRef] [PubMed]
- Firinu, D.; Perra, A.; Campagna, M.; Littera, R.; Meloni, F.; Sedda, F.; Conti, M.; Costanzo, G.; Erbi, M.; Usai, G.; et al. Evaluation of Antibody Response to Heterologous Prime–Boost Vaccination with ChAdOx1 nCoV-19 and BNT162b2: An Observational Study. Vaccines 2021, 9, 1478. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Interim Recommendations for Heterologous COVID-19 Vaccine Schedules. Interim Guidance 16 December 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Squeri, R.; La Fauci, V.; Picerno, I.A.M.; Trimarchi, G.; Cannavò, G.; Egitto, G.; Cosenza, B.; Merlina, V.; Genovese, C. Evaluation of Vaccination Coverages in the Health Care Workers of a University Hospital in Southern Italy. Ann Ig 2019, 31 (Suppl. 1), 13–24. [Google Scholar] [CrossRef] [PubMed]
- La Fauci, V.; Squeri, R.; Genovese, C.; Anzalone, C.; Fedele, F.; Squeri, A.; Alessi, V. An observational study of university students of healthcare area: Knowledge, attitudes and behaviour towards vaccinations. Clin. Ter. 2019, 170, e448–e453. [Google Scholar] [CrossRef] [PubMed]
- Genovese, C.; Costantino, C.; Odone, A.; Trimarchi, G.; La Fauci, V.; Mazzitelli, F.; D’Amato, S.; Squeri, R.; the COVID-19 Risk Perception Group. A Knowledge, Attitude, and Perception Study on Flu and COVID-19 Vaccination during the COVID-19 Pandemic: Multicentric Italian Survey Insights. Vaccines 2022, 10, 142. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Section 1. Sociodemographic Characteristics. | |||
|---|---|---|---|
| Sex | |||
| Age | |||
| Section 2. Presence of Comorbidities. | |||
| Yes | No | ||
| Extremely vulnerable: | |||
| If yes: | |||
| Respiratory diseases | |||
| Cardiocirculatory disease | |||
| Neurological diseases or disability | |||
| Diabetes/other severe endocrinopathies | |||
| Kidney diseases | |||
| Autoimmune diseases | |||
| Liver diseases | |||
| Cerebrovascular diseases | |||
| Onco-hematological diseases or haemoglobinopathies | |||
| Graft | |||
| Severe obesity (BMI > 35) | |||
| Severe underweight (BMI < 16.5) | |||
| Vulnerable: | |||
| If yes, specify what chronic disease: _______________________________________________________ | |||
| Section 3. Presence of Adverse Events. | |||
| No | |||
| Yes | Specify if a local (i.e., rash, pain, etc.) or general reaction (tiredness, headache, myalgia, arthralgia, chills, fever, etc.), its type, and duration____________________________ | ||
| N° | % | |
|---|---|---|
| Sex | ||
| Male | 48 | 27.6 |
| Female | 126 | 72.4 |
| Mean age ± SD | 51.83 ± 14.40 SD | |
| Age | ||
| 21–30 | 12 | 6.90 |
| 31–39 | 21 | 12.07 |
| 40–49 | 39 | 22.41 |
| 50–59 | 60 | 34.50 |
| 60–69 | 18 | 10.35 |
| 70–79 | 23 | 13.21 |
| >80 | 1 | 0.56 |
| Vaxzevria * | Comirnaty * | |||
|---|---|---|---|---|
| M (%) | F (%) | M (%) | F (%) | |
| Pain at injection site | 44.83% (78) | 55.17% (96) | 43.10% (75) | 56.90% (99) |
| Fatigue | 44.83% (78) | 55.17% (96) | 18.97% (33) | 81.03% (141) |
| Fever (≥38.5 °C) | 46.55% (81) | 53.45% (93) | 8.62% (15) | 91.38% (159) |
| Chills | 29.31% (51) | 70.69% (123) | 25.86% (45) | 74.14% (129) |
| Headache | 48.28% (84) | 51.72% (90) | 12.07% (21) | 87.93% (153) |
| Nausea | 20.69% (36) | 79.31% (138) | 27.59% (48) | 72.41% (126) |
| Myalgia/arthralgia | 34.48% (60) | 65.52% (114) | 3.45% (6) | 96.55% (168) |
| Vomiting | 6.90% (12) | 93.10% (162) | 3.45% (6) | 96.55% (168) |
| Swollen lymph nodes | 3.45% (6) | 96.55% (168) | 3.45% (6) | 96.55% (168) |
| Diarrhea | 3.45% (21) | 96.55% (153) | 3.45% (6) | 96.55% (168) |
| Swelling at injection site | 12.07% (18) | 87.93% (156) | 1.72% (3) | 98.28% (171) |
| Allergic reactions | 10.34% (33) | 89.66% (141) | 10.34% (18) | 89.66% (156) |
| Sleep disorders | 18.97% (12) | 81.03% (162) | 8.62% (15) | 91.38% (159) |
| Neurological disorders | 60.34% (105) | 39.66% (69) | 0.00% (0) | 0.00% (0) |
| Vaxzevria | |||
|---|---|---|---|
| Comorbidities | Non-Vulnerable | Vulnerable | Extremely Vulnerable |
| Pain at injection site | 32.76% (57) | 12.07% (21) | 17.24% (30) |
| Fatigue | 31.03% (54) | 12.07% (21) | 17.24% (30) |
| Fever (≥ 38.5 °C) | 31.03% (54) | 10.34% (18) | 17.24% (30) |
| Chills | 22.41% (39) | 8.62% (15) | 10.34% (18) |
| Headache | 31.03% (54) | 10.34% (18) | 17.24% (30) |
| Nausea | 10.34% (18) | 6.90% (12) | 8.62% (15) |
| Myalgia/arthralgia | 18.97% (33) | 10.34% (18) | 17.24% (30) |
| Vomiting | 3.45% (6) | 0.00% (0) | 5.17% (9) |
| Swollen lymph nodes | 1.72% (3) | 0.00% (0) | 1.72% (3) |
| Diarrhea | 1.72% (3) | 0.00% (0) | 1.72% (3) |
| Swelling at injection site | 3.45% (6) | 1.72% (3) | 10.34% (18) |
| Allergic reactions | 10.34% (18) | 3.45% (6) | 1.72% (3) |
| Sleep disorders | 12.07% (21) | 5.17% (9) | 10.34% (18) |
| Neurological disorders | 5.17% (9) | 5.17% (9) | 3.45% (6) |
| Comirnaty | |||
| Pain at injection site | 39.66% (69) | 20.69% (36) | 22.41% (39) |
| Fatigue | 29.31% (51) | 10.34% (18) | 12.07% (21) |
| Fever (≥ 38.5 °C) | 13.79% (24) | 3.45% (6) | 3.45% (6) |
| Chills | 3.45% (6) | 1.72% (3) | 3.45% (6) |
| Headache | 13.79% (24) | 5.17% (9) | 8.62% (15) |
| Nausea | 8.62% (15) | 0.00% (0) | 3.45% (6) |
| Myalgia/arthralgia | 15.52% (27) | 3.45% (6) | 12.07% (21) |
| Vomiting | 3.45% (6) | 0.00% (0) | 0.00% (0) |
| Swollen lymph nodes | 5.17% (9) | 0.00% (0) | 0.00% (0) |
| Diarrhea | 5.17% (9) | 1.72% (3) | 1.72% (3) |
| Swelling at injection site | 5.17% (9) | 1.72% (3) | 1.72% (3) |
| Allergic reactions | 0.00% (0) | 1.72% (3) | 3.45% |
| Sleep disorders | 0.00% (0) | 0.00% (0) | 1.72% (3) |
| Neurological disorders | 6.90% (12) | 0.00% (0) | 5.17% (9) |
| Age | <50 | 51–60 | >60 |
|---|---|---|---|
| Vaxzevria | |||
| Pain at injection site | 28% (48) | 26% (45) | 9% (15) |
| Fatigue | 29% (51) | 17% (30) | 14% (24) |
| Fever (≥38.5 °C) | 34% (60) | 16% (27) | 9% (15) |
| Chills | 22% (39) | 16% (27) | 3% (6) |
| Headache | 31% (54) | 22% (39) | 5% (9) |
| Nausea | 17% (30) | 7% (12) | 2% (3) |
| Myalgia/arthralgia | 24% (42) | 12% (21) | 10% (18) |
| Vomiting | 7% (12) | 0% (0) | 2% (3) |
| Swollen lymph nodes | 2% (3) | 2% (3) | 0% (0) |
| Diarrhea | 0% (0) | 0% (0) | 3% (6) |
| Swelling at injection site | 7% (12) | 7% (12) | 2% (3) |
| Allergic reactions | 9% (15) | 2% (3) | 5% (9) |
| Sleep disorders | 16% (27) | 7% (12) | 5% (9) |
| Neurological disorders | 3% (6) | 9% (15) | 2% (3) |
| Comirnaty | |||
| Pain at injection site | 40% (69) | 26% (45) | 17% (30) |
| Fatigue | 31% (54) | 16% (27) | 5% (9) |
| Fever (≥38.5 °C) | 14% (27) | 5% (9) | 2% (3) |
| Chills | 2% (3) | 7% (12) | 0% (0) |
| Headache | 16% (27) | 10% (18) | 2% (3) |
| Nausea | 5% (9) | 7% (12) | 0% (0) |
| Myalgia/arthralgia | 14% (24) | 12% (21) | 5% (9) |
| Vomiting | 0% (0) | 2% (3) | 2% (3) |
| Swollen lymph nodes | 2% (3) | 3% (6) | 0% (0) |
| Diarrhea | 3% (6) | 3% (6) | 2% (3) |
| Swelling at injection site | 2% (3) | 0% (0) | 3% (6) |
| Allergic reactions | 0% (0) | 0% (0) | 2% (3) |
| Sleep disorders | 9% (15) | 2% (3) | 2% (3) |
| Neurological disorders | 9% (15) | 3% (6) | 2% (3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Venuto, R.; Giunta, I.; Vaccaro, M.; La Fauci, V.; Ceccio, C.; Fedele, F.; Privitera, A.; Denaro, F.; Pantò, G.; Cortese, R.; et al. Reactogenicity and Humoral Immune Response after Heterologous Vaxzevria/Comirnaty Vaccination in a Group of Individuals Vaccinated in the AOU Policlinic “G. Martino” (Messina, Italy): A Retrospective Cohort Study. Vaccines 2022, 10, 1803. https://doi.org/10.3390/vaccines10111803
Venuto R, Giunta I, Vaccaro M, La Fauci V, Ceccio C, Fedele F, Privitera A, Denaro F, Pantò G, Cortese R, et al. Reactogenicity and Humoral Immune Response after Heterologous Vaxzevria/Comirnaty Vaccination in a Group of Individuals Vaccinated in the AOU Policlinic “G. Martino” (Messina, Italy): A Retrospective Cohort Study. Vaccines. 2022; 10(11):1803. https://doi.org/10.3390/vaccines10111803
Chicago/Turabian StyleVenuto, Roberto, Ioselita Giunta, Mario Vaccaro, Vincenza La Fauci, Concetta Ceccio, Francesco Fedele, Antonino Privitera, Federica Denaro, Giuseppe Pantò, Rosaria Cortese, and et al. 2022. "Reactogenicity and Humoral Immune Response after Heterologous Vaxzevria/Comirnaty Vaccination in a Group of Individuals Vaccinated in the AOU Policlinic “G. Martino” (Messina, Italy): A Retrospective Cohort Study" Vaccines 10, no. 11: 1803. https://doi.org/10.3390/vaccines10111803