
Epidemiological Characteristics of Varicella under Different Immunisation Strategies in Suzhou Prefecture, Jiangsu Province
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Data Resources and Target Population
2.3. Estimation of Varicella Vaccination Coverage
2.4. Descriptive Statistical Analysis
3. Results
3.1. Demographic Characteristics and Age Distribution
3.2. Geographic Distribution
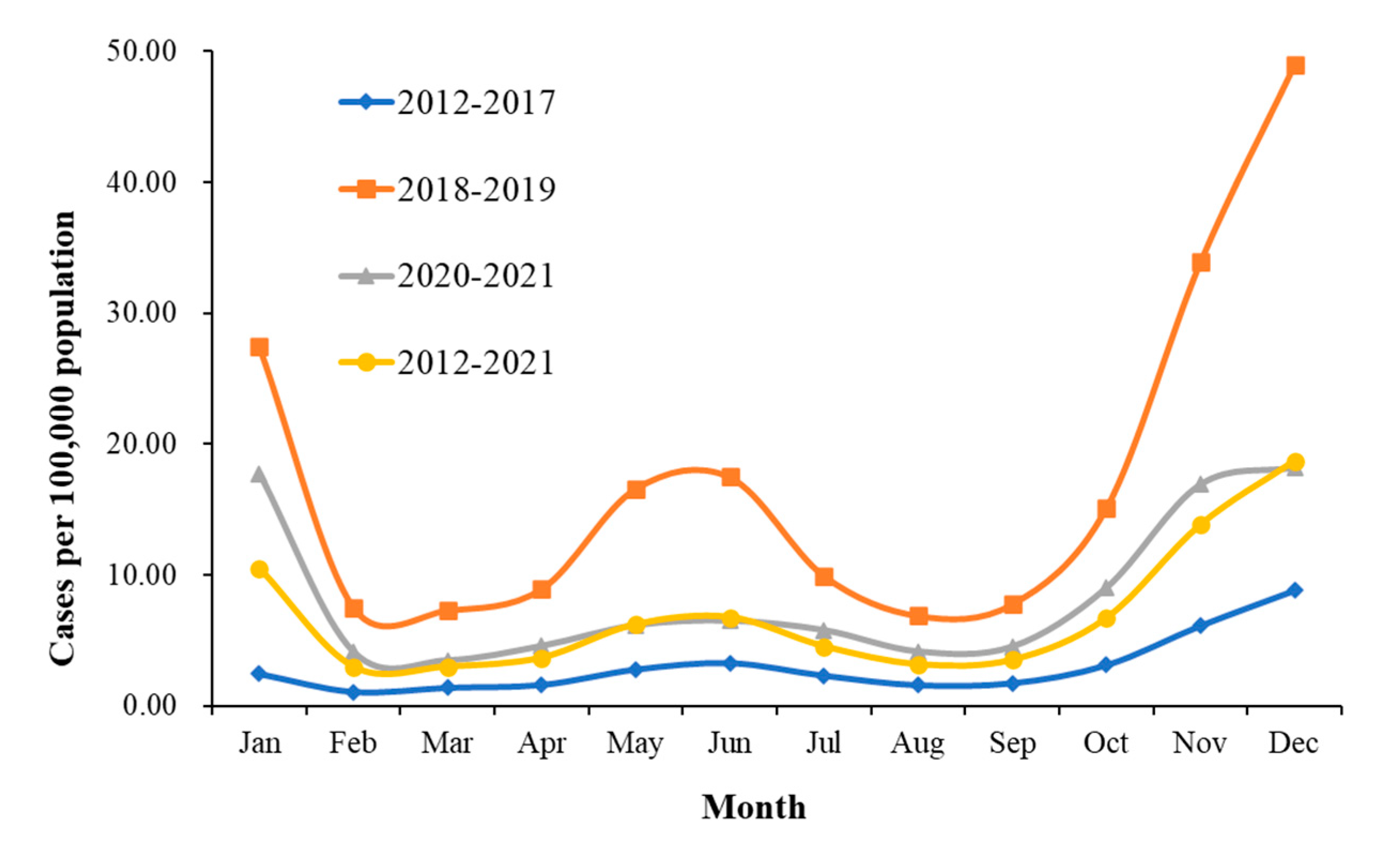
3.3. Seasonal Distribution
3.4. Estimation of Varicella Vaccination Coverage
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ulrich, H.; Jane, F. Seward Varicella. Lancet 2006, 368, 1365–1376. [Google Scholar]
- Anne, A.G.; Judith, B.; Jeffrey, I.C.; Randall, J.C.; Michael, D.G.; Don, G.; Charles, G.; Sophie, H.; Peter, G.E.K.; Michael, N.O.; et al. Varicella Zoster Virus Infection. Nat. Rev. Dis. Primers 2015, 1, 15016. [Google Scholar]
- Zhu, Y.; Zhu, J.W.; Cao, Y.L.; Lu, F.L. Meta-analysis of the protective effect of live attenuated varicella vaccine in Chinese children. Chin. Prev. Med. 2017, 18, 587–592. [Google Scholar]
- Arvin, A.M. Varicella-Zoster Virus. Clin. Microbiol Rev. 1996, 9, 361–381. [Google Scholar] [CrossRef]
- Hu, P.; Yang, F.; Li, X.F.; Wang, Y.; Xiao, T.T.; Li, H.; Wang, W.C.; Guan, J.; Li, S.P. Effectiveness of One-Dose versus Two-Dose Varicella Vaccine in Children in Qingdao, China: A Matched Case-Control Study. Hum. Vaccin Immunother. 2021, 17, 5311–5315. [Google Scholar] [CrossRef]
- Xu, Y.Y.; Liu, Y.; Zhang, X.P.; Zhang, X.C.; Du, J.; Cai, Y.X.; Wang, J.; Che, X.R.; Gu, W.W.; Jiang, W.; et al. Epidemiology of Varicella and Effectiveness of Varicella Vaccine in Hangzhou, China, 2019. Hum. Vaccin Immunother. 2021, 17, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Dong, P.M.; Wang, M.; Liu, Y.M. Epidemiological characteristics of varicella in China form 2016–2019. Chin. J. Vaccines Immun. 2020, 26, 403–406. [Google Scholar]
- Sui, H.T.; Li, J.C.; Wang, M.M.; Liu, Y.M.; Yin, D.P. Epidemiological characteristics of varicella in China from 2005–2015. Chin. J. Vaccines Immun. 2019, 25, 155–159. [Google Scholar]
- Choo, P.W.; Donahue, J.G.; Manson, J.E.; Platt, R. The Epidemiology of Varicella and Its Complications. J. Infect. Dis. 1995, 172, 706–712. [Google Scholar] [CrossRef]
- Fu, J.; Jiang, C.; Wang, J.; Zhao, F.; Ma, T.; Shi, R.; Zhao, Y.; Zhang, X. Epidemiology of Varicella in Haidian District, Beijing, China—2007–2015. Vaccine 2017, 35, 2365–2371. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, F.; Cao, Y.; Zhang, N. Epidemiological Characteristics of Varicella before and after the Implementation of Two-Dose Vaccination Schedule in Chaoyang District, Beijing, 2007–2019. J. Infect. 2021, 83, 607–635. [Google Scholar] [CrossRef]
- Miller, E.; Vurdien, J.; Farrington, P. Shift in Age in Chickenpox. Lancet 1993, 341, 308–309. [Google Scholar] [CrossRef]
- Lenis-Ballesteros, V.; Ochoa, J.; Hincapié-Palacio, D.; León-Álvarez, A.; Vargas-Restrepo, F.; Ospina, M.C.; Buitrago-Giraldo, S.; Díaz, F.J.; Gonzalez-Ortíz, D. Seroprevalence of Varicella in Pregnant Women and Newborns in a Region of Colombia. Vaccines 2021, 10, 52. [Google Scholar] [CrossRef]
- Parente, S.; Moriello, N.S.; Maraolo, A.E.; Tosone, G. Management of Chickenpox in Pregnant Women: An Italian Perspective. Eur. J. Clin. Microbiol Infect. Dis. 2018, 37, 1603–1609. [Google Scholar] [CrossRef]
- Leineweber, B.; Grote, V.; Schaad, B.; Heininger, U. Transplacentally Acquired Immunoglobulin G Antibodies against Measles, Mumps, Rubella and Varicella-Zoster Virus in Preterm and Full Term Newborns. Pediatric. Infect. Dis. J. 2004, 23, 361–363. [Google Scholar] [CrossRef]
- Varicella and Herpes Zoster Vaccines: WHO Position Paper, June 2014–Recommendations. Vaccine 2016, 34, 198–199. [CrossRef]
- Edmunds, W.J.; Brisson, M. The Effect of Vaccination on the Epidemiology of Varicella Zoster Virus. J. Infect. 2002, 44, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Maria, L.Á.A.; Sandra, B.; José, B.D.C.; María, E.C.D.; Luis, E.C.; Carmen, D.; Roberto, D.; Carlos, E.; Luiza, H.F.A.; Antonio, J.G.M.; et al. Varicella Epidemiology in Latin America and the Caribbean. Expert Rev. Vaccines 2018, 17, 175–183. [Google Scholar]
- Zhang, Z.J.Z.; Suo, L.D.; Pan, J.B.; Zhao, D.; Lu, L. Two-Dose Varicella Vaccine Effectiveness in China: A Meta-Analysis and Evidence Quality Assessment. BMC Infect. Dis. 2021, 21, 543. [Google Scholar] [CrossRef] [PubMed]
- Siedler, A.; Rieck, T.; Tolksdorf, K. Strong Additional Effect of a Second Varicella Vaccine Dose in Children in Germany, 2009–2014. J. Pediatrics 2016, 173, 202–206.e2. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, L.; Wang, Y.; Zhang, W.; Jia, N.; Xie, Z.; Huang, L.; You, W.; Lu, W.; Li, E.; et al. Immunogenicity and Safety of a Booster Dose of Live Attenuated Varicella Vaccine, and Immune Persistence of a Primary Dose for Children Aged 2 to 6 Years. Vaccines 2022, 10, 660. [Google Scholar] [CrossRef] [PubMed]
- Immunization procedures and instructions for children with national immunization program vaccines (2021 version). Chin. J. Viral. Dis. 2021, 11, 241–245.
- Rice, P.S. Ultra-Violet Radiation Is Responsible for the Differences in Global Epidemiology of Chickenpox and the Evolution of Varicella-Zoster Virus as Man Migrated out of Africa. Virol. J. 2011, 8, 189. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Zhang, Z.; He, Q.; Ma, X.; Yang, Z. Association between Climatic Factors and Varicella Incidence in Guangzhou, Southern China, 2006–2018. Sci. Total Environ. 2020, 728, 138777. [Google Scholar] [CrossRef] [PubMed]
- Cersosimo, A.; Riccardi, M.; Amore, L.; Cimino, G.; Arabia, G.; Metra, M.; Vizzardi, E. Varicella Zoster Virus and Cardiovascular Diseases. Monaldi Arch. Chest Dis 2022. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.F.; Chen, Y.; Wu, W.L.; Guo, L.; Xu, W.W.; Chen, J.; Sun, S.H.; Li, J.J.; Chen, Z.W.; Gu, L.Y.; et al. Varicella Zoster Virus Infections Increase the Risk of Disease Flares in Patients with SLE: A Matched Cohort Study. Lupus Sci Med. 2019, 6, e000339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Hou, Y.; Li, J.; Wang, J. The Role of Astaxanthin on Chronic Diseases. Crystals 2021, 11, 505. [Google Scholar] [CrossRef]
- Sun, X.; Xue, Z.; Yasin, A.; He, Y.; Chai, Y.; Li, J.; Zhang, K. Colorectal Cancer and Adjacent Normal Mucosa Differ in Apoptotic and Inflammatory Protein Expression. Eng. Regen. 2021, 2, 279–287. [Google Scholar] [CrossRef]
- Kitano, T. The Estimated Burden of 15 Vaccine-Preventable Diseases from 2008 to 2020 in Japan: A Transition by the COVID-19 Pandemic. J. Infect. Chemother. 2021, 27, 1482–1488. [Google Scholar] [CrossRef]
- Bhatt, P.; Strachan, J.; Easton, M.; Franklin, L.; Drewett, G. Effect of COVID-19 Restrictions and Border Closures on Vaccine Preventable Diseases in Victoria, Australia, 2020–2021. Commun. Dis. Intell. 2022, 46. [Google Scholar] [CrossRef]
- Dong, S.B.; Wang, X.L.; Huo, D.; Li, R.Q.; Yang, Y.; Liang, Z.C.; Wang, Q.Y.; Jia, L. Epidemiological characteristics of hand, foot and mouth disease among people aged 6 and over in Beijing, 2011–2020. Zhonghua Liu Xing Bing Xue Za Zhi 2022, 43, 207–212. [Google Scholar] [PubMed]
- Wang, J.; Xu, Z.; Gao, Q. Varicella Outbreaks in Schools and Kindergartens in Shanghai, China from 2011 to 2020. PLoS ONE 2022, 17, e0270630. [Google Scholar] [CrossRef] [PubMed]
- Hao, B.; Chen, Z.; Zeng, G.; Huang, L.; Luan, C.; Xie, Z.; Chen, J.; Bao, M.; Tian, X.; Xu, B.; et al. Efficacy, Safety and Immunogenicity of Live Attenuated Varicella Vaccine in Healthy Children in China: Double-Blind, Randomized, Placebo-Controlled Clinical Trial. Clin. Microbiol. Infect. 2019, 25, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, Q.; Du, X.; Zhao, X.; Yin, Z. Vaccine Coverage and Effectiveness in a School-Based Varicella Outbreak in Jinan Prefecture, Shandong Province. Vaccines 2022, 10, 1225. [Google Scholar] [CrossRef] [PubMed]
- Barbara, K.; Holly, M.; Henry, S.; Steve, B.; Penelope, D.; Barbara, W.; Keith, R.; Lee, L.K.; Lisa, L.; Jonathan, H.; et al. Ten Year Follow-up of Healthy Children Who Received One or Two Injections of Varicella Vaccine. Pediatr Infect. Dis. J. 2004, 23, 132–137. [Google Scholar]
- Eugene, D.S.; Marietta, V.; Daina, E.; Nancy, H.; Sharon, P.S.; James, D.; Philip, S.L.; Anne, A.G. Effectiveness of 2 Doses of Varicella Vaccine in Children. J. Infect. Dis 2011, 203, 312–315. [Google Scholar]
- Ma, C.; Li, J.; Wang, N.; Wang, Y.; Song, Y.; Zeng, X.; Zheng, C.; An, Z.; Rodewald, L.; Yin, Z. Prioritization of Vaccines for Inclusion into China’s Expanded Program on Immunization: Evidence from Experts’ Knowledge and Opinions. Vaccines 2022, 10, 1010. [Google Scholar] [CrossRef]
- Giglio, N.; Lasalvia, P.; Pawaskar, M.; Parellada, C.I.; Rojas, Y.G.; Micone, P.; Babic, V.V.; Neyro, S.E. Trends in Varicella Burden of Disease Following Introduction of Routine Childhood Varicella Vaccination in Argentina: A 12-Year Time Series Analysis. Vaccines 2022, 10, 1151. [Google Scholar] [CrossRef]
- Sharomi, O.; Xausa, I.; Nachbar, R.; Pillsbury, M.; Matthews, I.; Petigara, T.; Elbasha, E.; Pawaskar, M. Modeling the Impact of Exogenous Boosting and Universal Varicella Vaccination on the Clinical and Economic Burden of Varicella and Herpes Zoster in a Dynamic Population for England and Wales. Vaccines 2022, 10, 1416. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Period | Average Incidence (per 100,000) | χ2 | p-Value | Vaccination Schedule |
|---|---|---|---|---|
| 2012–2017 | 49.17 | 98.077 | 0.00 | before the government implemented free varicella vaccination |
| 2018–2019 | 207.98 | 36.83 | 0.00 | 1-dose varicella vaccine included in local EPI |
| 2020–2021 | 101.26 | 2-dose varicella vaccine included in local EPI |
| District | Average Incidence (per 100,000) | P1 | P2 | |||||
|---|---|---|---|---|---|---|---|---|
| 2012–2021 | 2012–2017 | 2018–2019 | 2020–2021 | |||||
| Gusu | 80.51 | 22.05 | 145.83 | 81.86 | 91.265 | 0.00 | 17.973 | 0.00 |
| Xiangcheng | 74.36 | 30.30 | 76.67 | 54.49 | 20.101 | 0.00 | 3.7508 | 0.05278 |
| Zhangjiagang | 45.67 | 25.96 | 257.02 | 36.90 | 188.67 | 0.00 | 164.85 | 0.00 |
| Kunshan | 44.41 | 56.57 | 201.83 | 30.98 | 127.47 | 0.00 | 164.85 | 0.00 |
| Taicang | 74.51 | 21.46 | 249.96 | 58.19 | 192.37 | 0.00 | 119.34 | 0.00 |
| SNP | 117.01 | 77.07 | 316.98 | 43.21 | 146.06 | 0.00 | 208.08 | 0.00 |
| Wujiang | 58.77 | 10.37 | 141.01 | 56.25 | 112.74 | 0.00 | 36.42 | 0.00 |
| Wuzhong | 80.00 | 89.17 | 280.90 | 36.64 | 99.334 | 0.00 | 187.89 | 0.00 |
| SIP | 118.28 | 35.60 | 360.95 | 98.67 | 266.93 | 0.00 | 149.67 | 0.00 |
| Changshu | 113.29 | 44.81 | 211.47 | 54.12 | 108.37 | 0.00 | 93.233 | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Liu, N.; Zhang, J.; Xu, J.; Wang, W.; Xiao, J.; Wang, T.; Luan, L.; Zhang, Y. Epidemiological Characteristics of Varicella under Different Immunisation Strategies in Suzhou Prefecture, Jiangsu Province. Vaccines 2022, 10, 1745. https://doi.org/10.3390/vaccines10101745
Zhang Z, Liu N, Zhang J, Xu J, Wang W, Xiao J, Wang T, Luan L, Zhang Y. Epidemiological Characteristics of Varicella under Different Immunisation Strategies in Suzhou Prefecture, Jiangsu Province. Vaccines. 2022; 10(10):1745. https://doi.org/10.3390/vaccines10101745
Chicago/Turabian StyleZhang, Zhuoyu, Na Liu, Jun Zhang, Juan Xu, Wenyu Wang, Jiaqi Xiao, Tianyu Wang, Lin Luan, and Yunyan Zhang. 2022. "Epidemiological Characteristics of Varicella under Different Immunisation Strategies in Suzhou Prefecture, Jiangsu Province" Vaccines 10, no. 10: 1745. https://doi.org/10.3390/vaccines10101745