
COVID-19 Vaccine Acceptance among Vulnerable Groups: Syrian Refugees in Jordan

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Instrument
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
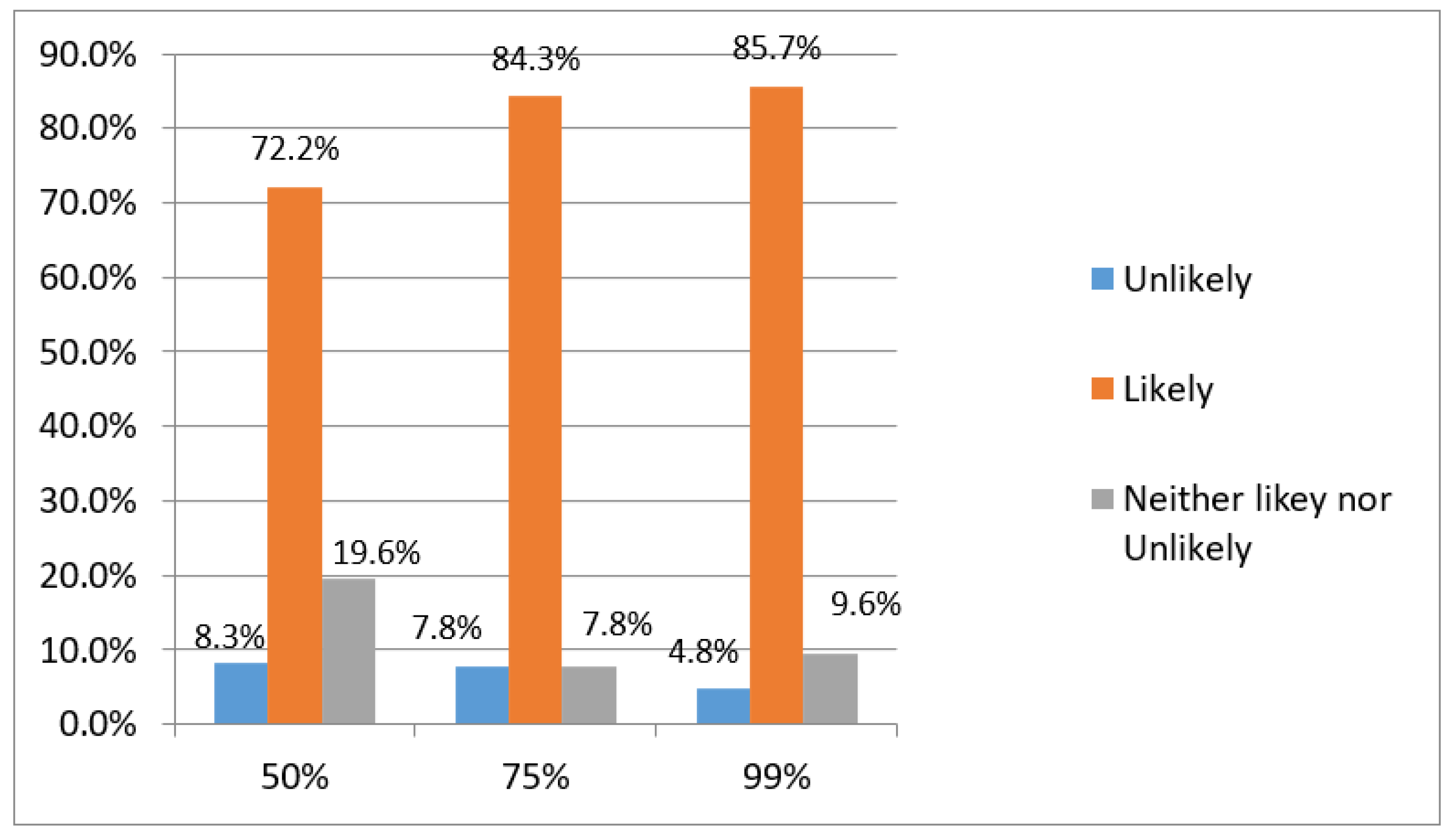
3.2. Vaccine Acceptance
3.3. Level of Knowledge
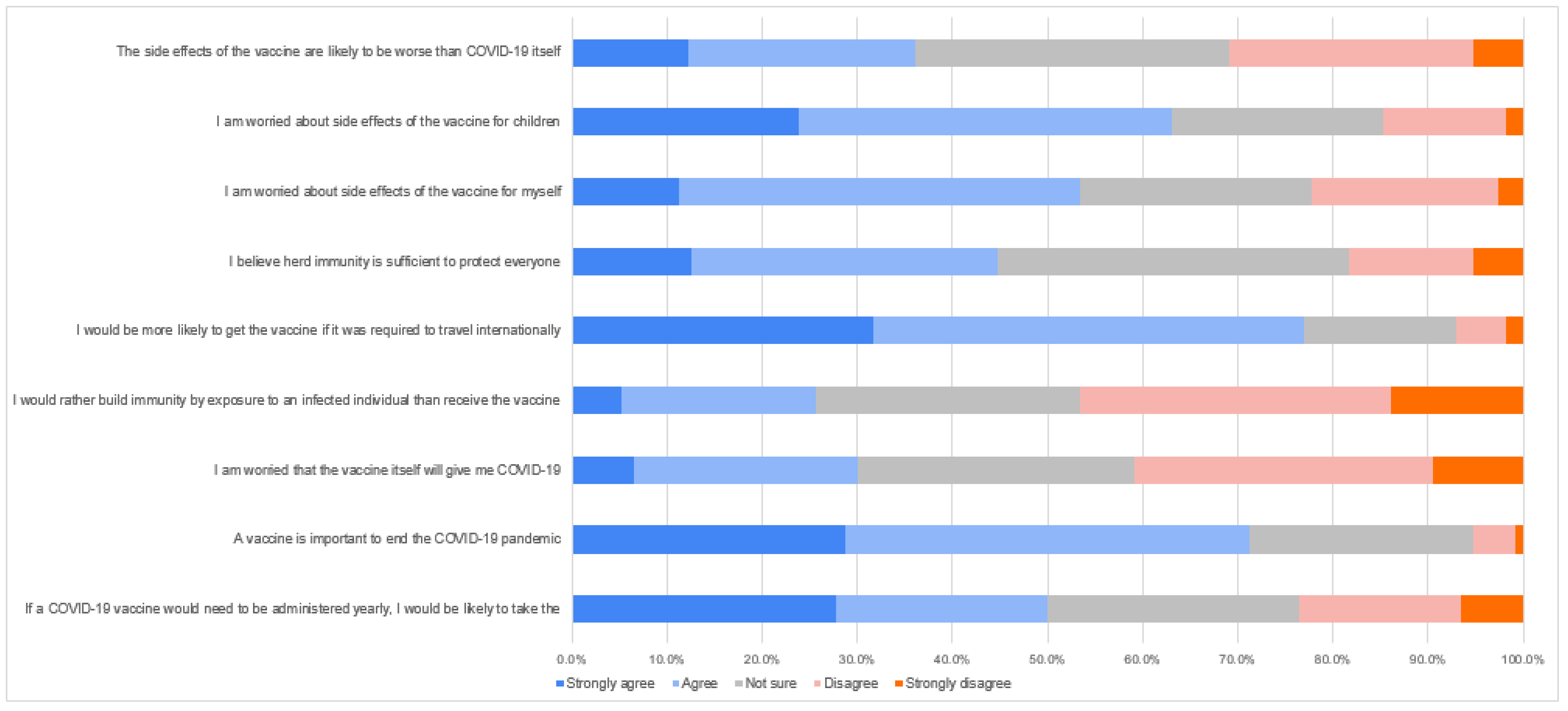
3.4. Attitudes and Beliefs toward COVID-19 Disease and Vaccine
3.5. Determinants Influencing COVID-19 Vaccine Acceptance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. Effect of COVID-19 Vaccination on Transmission of Alpha and Delta Variants. N. Engl. J. Med. 2022, 386, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Yamey, G.; Schäferhoff, M.; Hatchett, R.; Pate, M.; Zhao, F.; McDade, K.K. Ensuring Global Access to COVID-19 Vaccines. Lancet 2020, 395, 1405–1406. [Google Scholar] [CrossRef]
- Shafqat, A.; Arabi, T.Z.; Sabbah, B.N.; Abdulkader, H.S.; Shafqat, S.; Razak, A.; Kashir, J.; Alkattan, K.; Yaqinuddin, A. Understanding COVID-19 Vaccines Today: Are T-Cells Key Players? Vaccines 2022, 10, 904. [Google Scholar] [CrossRef] [PubMed]
- McAdams, D.; McDade, K.K.; Ogbuoji, O.; Johnson, M.; Dixit, S.; Yamey, G. Incentivising Wealthy Nations to Participate in the COVID-19 Vaccine Global Access Facility (COVAX): A Game Theory Perspective. BMJ Glob. Health 2020, 5, e003627. [Google Scholar] [CrossRef] [PubMed]
- Usher, A.D. Vaccine Shortages Prompt Changes to COVAX Strategy. Lancet 2021, 398, 1474. [Google Scholar] [CrossRef]
- Usher, A.D. A Beautiful Idea: How COVAX Has Fallen Short. Lancet 2021, 397, 2322–2325. [Google Scholar] [CrossRef]
- Mills, A. Health Care Systems in Low- and Middle-Income Countries. N. Engl. J. Med. 2014, 370, 552–557. [Google Scholar] [CrossRef]
- Refugees, U.N.H.C.R. for UNHCR—Refugee Statistics. Available online: https://www.unhcr.org/refugee-statistics/ (accessed on 17 June 2022).
- Hejaz, H.A. Palestinian Strategies, Guidelines, and Challenges in the Treatment and Management of Coronavirus Disease-2019 (COVID-19). Avicenna J. Med. 2020, 10, 135–162. [Google Scholar] [CrossRef]
- Malchrzak, W.; Babicki, M.; Pokorna-Kałwak, D.; Doniec, Z.; Mastalerz-Migas, A. COVID-19 Vaccination and Ukrainian Refugees in Poland during Russian-Ukrainian War-Narrative Review. Vaccines 2022, 10, 955. [Google Scholar] [CrossRef]
- Bellizzi, S.; Aidyralieva, C.; Alsawhala, L.; Al-Shaikh, A.; Santoro, A.; Profili, M.C. Vaccination for SARS-CoV-2 of Migrants and Refugees, Jordan. Bull. World Health Organ. 2021, 99, 611. [Google Scholar] [CrossRef]
- WHO Regional Office for the Eastern Mediterranean; Dator, W.; Abunab, H.; Dao Ayen, N. Health Challenges and Access to Health Care among Syrian Refugees in Jordan: A Review. East. Mediterr. Health J. 2018, 24, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Al Qutob, M.F. WHO and the Refugee Crisis in Jordan and Beyond. Lancet Glob. Health 2016, 4, e304. [Google Scholar] [CrossRef]
- Kohli, M.; Maschio, M.; Becker, D.; Weinstein, M.C. The Potential Public Health and Economic Value of a Hypothetical COVID-19 Vaccine in the United States: Use of Cost-Effectiveness Modeling to Inform Vaccination Prioritization. Vaccine 2021, 39, 1157–1164. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.; Baird, S.; Abu Hamad, B.; Bhutta, Z.A.; Oakley, E.; Shah, M.; Sajdi, J.; Yount, K.M. Compounding Inequalities: Adolescent Psychosocial Wellbeing and Resilience among Refugee and Host Communities in Jordan during the COVID-19 Pandemic. PLoS ONE 2022, 17, e0261773. [Google Scholar] [CrossRef]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef]
- Al-Mulla, R.; Abu-Madi, M.; Talafha, Q.M.; Tayyem, R.F.; Abdallah, A.M. COVID-19 Vaccine Hesitancy in a Representative Education Sector Population in Qatar. Vaccines 2021, 9, 665. [Google Scholar] [CrossRef]
- Jordan—Poverty Update: Main Report, Washington, D.C.: World Bank Group. Available online: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/418831468284339304/Main-report (accessed on 25 August 2022).
- Salibi, N.; Abdulrahim, S.; El Haddad, M.; Bassil, S.; El Khoury, Z.; Ghattas, H.; McCall, S.J. COVID-19 Vaccine Acceptance in Older Syrian Refugees: Preliminary Findings from an Ongoing Study. Prev. Med. Rep. 2021, 24, 101606. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Al-kafarna, M.; Matar, S.G.; Almadhoon, H.W.; Almaghary, B.K.; Zaazouee, M.S.; Elrashedy, A.A.; Wafi, D.S.; Jabari, S.D.; Salloum, O.H.; Ibrahim, E.A.; et al. Public Knowledge, Attitude, and Acceptance toward COVID-19 Vaccines in Palestine: A Cross-Sectional Study. BMC Public Health 2022, 22, 529. [Google Scholar] [CrossRef]
- Al-Qerem, W.; Al Bawab, A.Q.; Hammad, A.; Jaber, T.; Khdair, S.I.; Kalloush, H.; Ling, J.; Mosleh, R. Parents’ Attitudes, Knowledge and Practice towards Vaccinating Their Children against COVID-19: A Cross-Sectional Study. Hum. Vaccines Immunother. 2022, 18, 2044257. [Google Scholar] [CrossRef]
- Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Mohamud, R.; Fawaz, M.; Kateeb, E.T.; Alkhairy, O.K.; Tayyem, R.; Lounis, M.; Al-Raeei, M.; et al. Reported Adverse Effects and Attitudes among Arab Populations Following COVID-19 Vaccination: A Large-Scale Multinational Study Implementing Machine Learning Tools in Predicting Post-Vaccination Adverse Effects Based on Predisposing Factors. Vaccines 2022, 10, 366. [Google Scholar] [CrossRef] [PubMed]
- Abu-Rish, E.Y.; Bustanji, Y.; Abusal, K. Nationwide Routine Childhood Vaccination Coverage During the COVID-19 Pandemic in Jordan: Current Situation, Reasons, and Predictors of Vaccination. Int. J. Clin. Pract. 2022, 2022, 7918604. [Google Scholar] [CrossRef] [PubMed]
- Khatatbeh, M.; Albalas, S.; Khatatbeh, H.; Momani, W.; Melhem, O.; Al Omari, O.; Tarhini, Z.; A’aqoulah, A.; Al-Jubouri, M.; Nashwan, A.J.; et al. Children’s Rates of COVID-19 Vaccination as Reported by Parents, Vaccine Hesitancy, and Determinants of COVID-19 Vaccine Uptake among Children: A Multi-Country Study from the Eastern Mediterranean Region. BMC Public Health 2022, 22, 1375. [Google Scholar] [CrossRef] [PubMed]
- Ryalat, S.; Alduraidi, H.; Al-Ryalat, S.A.; Alzu’bi, M.; Alzyoud, M.; Odeh, N.; Alrawabdeh, J. Attitudes towards COVID-19 Booster Vaccines, Vaccine Preferences, Child Immunization, and Recent Issues in Vaccination among University Students in Jordan. Vaccines 2022, 10, 1258. [Google Scholar] [CrossRef]
- Naser, A.; Dahmash, E.; Alsairafi, Z.; Alwafi, H.; Alyami, H.; Jalal, Z.; Al Rajeh, A.; Paudyal, V.; Alhartani, Y.; Turkistani, F.; et al. Knowledge and Practices during the COVID-19 Outbreak in the Middle East: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 4699. [Google Scholar] [CrossRef]
- Abunada, T.; Abdallah, A.M.; Singh, R.; Abu-Madi, M. Development and Validation of a Clinical Practicum Assessment Tool for the NAACLS-Accredited Biomedical Science Program. Int. J. Environ. Res. Public Health 2022, 19, 6651. [Google Scholar] [CrossRef]
- Jordan: Refugee Response—Corona Update (April 2021). Available online: https://data.unhcr.org/fr/documents/details/86772 (accessed on 29 August 2022).
- COVID-19: Services, Info & Resources. Available online: https://help.unhcr.org/jordan/en/covid19-coronavirus-services/ (accessed on 29 August 2022).



{kind=link}
{kind=link}
| Demographic | Variable Category | n | % |
|---|---|---|---|
| Gender | Male | 100 | 43.5 |
| Female | 130 | 56.5 | |
| Age | 18–24 years | 109 | 47.4 |
| 25–31 years | 41 | 17.8 | |
| 32–38 years | 38 | 16.5 | |
| 39–45 years | 29 | 12.6 | |
| 46+ years | 13 | 5.7 | |
| Education level | Less than secondary school | 120 | 52.2 |
| Diploma | 35 | 15.2 | |
| Bachelor | 55 | 23.9 | |
| Master | 4 | 1.7 | |
| Doctorate | 2 | 0.9 | |
| Other | 14 | 6.1 | |
| Marital status | Single | 104 | 45.2 |
| Married | 119 | 51.7 | |
| Divorced | 1 | 0.4 | |
| widow | 6 | 2.6 | |
| Work | Yes | 72 | 31.3 |
| No | 158 | 68.7 | |
| Income | Less than 150 | 163 | 70.9 |
| 151–250 | 50 | 21.7 | |
| 251–350 | 14 | 6.1 | |
| 351–450 | 1 | 0.4 | |
| 650+ | 2 | 0.9 |
| Knowledge Score | Would Vaccinate n (%) | Would Not Vaccinate n (%) | X2 | p-Value |
|---|---|---|---|---|
| High (1–2.6) | 191 (90.9) | 19 (9.1) | 4.972 | 0.04 |
| Low (2.61–3) | 15 (75) | 5 (25) |
| Question | Answers | Would Vaccinate n (%) | Would Not Vaccinate n (%) | Multinomial Logistic Regression Analysis | ||
|---|---|---|---|---|---|---|
| Odds ratio | 95% CI | p | ||||
| What is your primary source of information regarding COVID-19? | Professional sources | 104 (93%) | 8 (7%) | 0.95 | 0.65–1.35 | 0.76 |
| Unprofessional sources | 94 (89%) | 12 (11%) | 4.29 | 0.77 | 0.09 | |
| Leaders | 8 (67%) | 4 (33%) | Reference | |||
| How important is it for you to get the flu vaccine every year? | Important | 142 (94%) | 9 (6%) | 5.94 | 1.65–21.3 | 0.006 |
| Somewhat important | 38 (88%) | 5 (12%) | 2.47 | 0.64–950 | 0.18 | |
| Not important | 26 (72%) | 10 (28%) | Reference | |||
| To what extent do you follow the news of COVID-19? | Follow | 81 (93%) | 6 (7%) | 1.38 | 0.38–5.05 | 0.61 |
| Neither follow nor do not follow | 56 (90%) | 6 (10%) | 0.94 | 0.27–3.23 | 0.92 | |
| Do not follow | 69 (85%) | 12 (15%) | Reference | |||
| I worry that the rushed pace of testing for a COVID-19 vaccine will fail to detect potential side effects. | Agree | 113 (89%) | 14 (11%) | 1.58 | 0.31–7.96 | 0.57 |
| Neither agree nor disagree | 74 (91%) | 7 (9%) | 1.73 | 0.31–9.50 | 0.52 | |
| Disagree | 19 (86%) | 3 (14%) | Reference | |||
| If COVID-19 vaccine is available and said it would protect 50% of those who take it, how likely you would take the vaccine? | Likely | 155 (93%) | 11 (7%) | 7.34 | 2.04–26.37 | 0.002 |
| Neither likely nor Unlikely | 39 (87%) | 6 (13%) | 5.22 | 1.21–22.51 | 0.027 | |
| Unlikely | 12 (63%) | 7 (37%) | Reference | |||
| The side effects of the vaccine are likely to be worse than COVID-19 itself. | Likely | 70 (84%) | 13 (16%) | 0.32 | 0.08–1.17 | 0.32 |
| Neither likely nor Unlikely | 70 (92) | 6 (8%) | 1.10 | 0.27–4.45 | 1.10 | |
| Unlikely | 66 (93) | 5 (7%) | Reference | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talafha, Q.M.; Al-Haidose, A.; AlSamman, A.Y.; Abdallah, S.A.; Istaiteyeh, R.; Ibrahim, W.N.; Hatmal, M.M.; Abdallah, A.M. COVID-19 Vaccine Acceptance among Vulnerable Groups: Syrian Refugees in Jordan. Vaccines 2022, 10, 1634. https://doi.org/10.3390/vaccines10101634
Talafha QM, Al-Haidose A, AlSamman AY, Abdallah SA, Istaiteyeh R, Ibrahim WN, Hatmal MM, Abdallah AM. COVID-19 Vaccine Acceptance among Vulnerable Groups: Syrian Refugees in Jordan. Vaccines. 2022; 10(10):1634. https://doi.org/10.3390/vaccines10101634
Chicago/Turabian StyleTalafha, Qusai M., Amal Al-Haidose, Ala Y. AlSamman, Saja A. Abdallah, Rasha Istaiteyeh, Wisam Nabeel Ibrahim, Ma’mon M. Hatmal, and Atiyeh M. Abdallah. 2022. "COVID-19 Vaccine Acceptance among Vulnerable Groups: Syrian Refugees in Jordan" Vaccines 10, no. 10: 1634. https://doi.org/10.3390/vaccines10101634