The Impact of Formulation on Lutein, Zeaxanthin, and meso-Zeaxanthin Bioavailability: A Randomised Double-Blind Placebo-Controlled Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
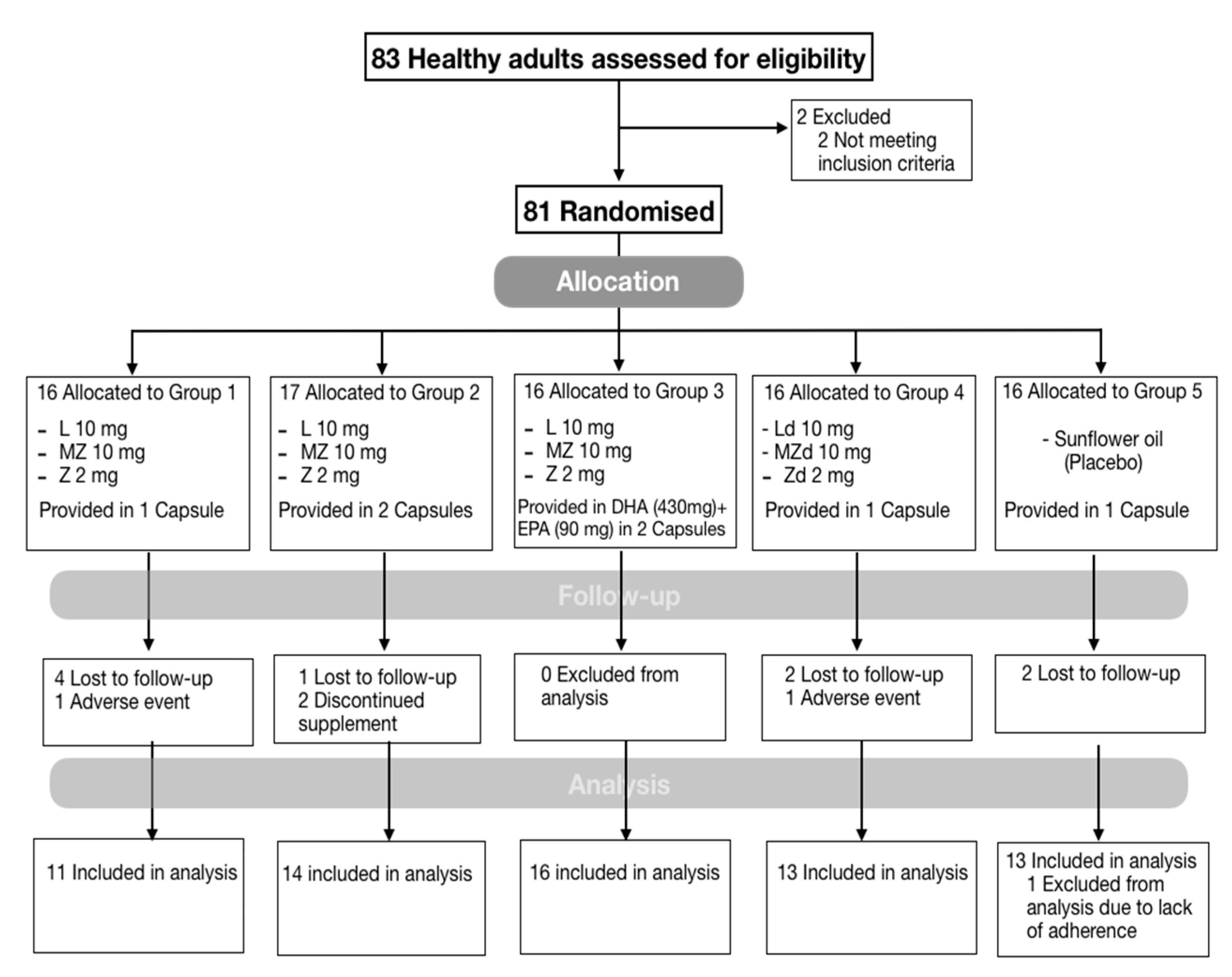
2.1. Design and Study Population
2.2. Interventions
Analysis of Supplements
2.3. Study Evaluations
2.3.1. Demographic, Lifestyle, Medical, and Dietary Assessment
2.3.2. Outcome Measures
2.3.3. Macular Pigment Measurement
2.3.4. Skin Carotenoid Concentrations
2.3.5. Carotenoid Serum Concentrations
2.4. Follow-Up and Adherence
2.5. Statistical Analysis
3. Results
3.1. Baseline Data
3.2. Analysis of Carotenoids in Supplements
3.3. L, Z, and MZ Serum Concentrations
3.4. L, Z, and MZ Tissue Concentrations
3.4.1. MP and MPOV
3.4.2. Carotenoid Skin Concentrations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Remington, L.A. Chapter 4—Retina. In Clinical Anatomy and Physiology of the Visual System, 3rd ed.; Butterworth-Heinemann: Saint Louis, MI, USA, 2012; pp. 61–92. [Google Scholar]
- Bernstein, P.S.; Li, B.; Vachali, P.P.; Gorusupudi, A.; Shyam, R.; Henriksen, B.S.; Nolan, J.M. Lutein, zeaxanthin, and meso-zeaxanthin: The basic and clinical science underlying carotenoid-based nutritional interventions against ocular disease. Prog. Retin. Eye Res. 2016, 50, 34–66. [Google Scholar] [CrossRef] [Green Version]
- Shyam, R.; Gorusupudi, A.; Nelson, K.; Horvath, M.P.; Bernstein, P.S. RPE65 has an additional function as the lutein to meso-zeaxanthin isomerase in the vertebrate eye. Proc. Natl. Acad. Sci. USA 2017, 114, 10882–10887. [Google Scholar] [CrossRef] [Green Version]
- Prado-Cabrero, A.; Beatty, S.; Stack, J.; Howard, A.; Nolan, J. Quantification of zeaxanthin stereoisomers and lutein in trout flesh using chiral high-performance liquid chromotography—Diode array detection. J. Food Compos. Anal. 2016, 50, 19–22. [Google Scholar] [CrossRef] [Green Version]
- Hobbs, R.P.; Bernstein, P.S. Nutrient supplementation for age-related macular degeneration, cataract, and dry eye. J. Ophthalmic. Vis. Res. 2014, 9, 487–493. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.M.; Dou, H.L.; Huang, F.F.; Xu, X.R.; Zou, Z.Y.; Lu, X.R.; Lin, X.M. Changes following supplementation with lutein and zeaxanthin in retinal function in eyes with early age-related macular degeneration: A randomised, double-blind, placebo-controlled trial. Br. J. Ophthalmol. 2015, 99, 371–375. [Google Scholar] [CrossRef]
- Chew, E.Y.; Clemons, T.E.; Agron, E.; Launer, L.J.; Grodstein, F.; Bernstein, P.S. Age-related eye disease study 2 research, g. effect of omega-3 fatty acids, lutein/zeaxanthin, or other nutrient supplementation on cognitive function: The AREDS2 randomized clinical trial. JAMA 2015, 314, 791–801. [Google Scholar] [CrossRef]
- Hammond, B.R.; Fletcher, L.M.; Roos, F.; Wittwer, J.; Schalch, W. A double-blind, placebo-controlled study on the effects of lutein and zeaxanthin on photostress recovery, glare disability, and chromatic contrast. Investig. Ophthalmol. Vis. Sci. 2014, 55, 8583–8589. [Google Scholar] [CrossRef] [Green Version]
- Murray, I.J.; Makridaki, M.; van der Veen, R.L.; Carden, D.; Parry, N.R.; Berendschot, T.T. Lutein supplementation over a one-year period in early AMD might have a mild beneficial effect on visual acuity: The CLEAR study. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1781–1788. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Jiang, C.; Zhang, Y.; Gong, Y.; Chen, X.; Zhang, M. Role of lutein supplementation in the management of age-related macular degeneration: Meta-analysis of randomized controlled trials. Ophthalmic. Res. 2014, 52, 198–205. [Google Scholar] [CrossRef]
- Akuffo, K.O.; Beatty, S.; Peto, T.; Stack, J.; Stringham, J.; Kelly, D.; Leung, I.; Corcoran, L.; Nolan, J.M. The Impact of supplemental antioxidants on visual function in nonadvanced age-related macular degeneration: A head-to-head randomized clinical trial. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5347–5360. [Google Scholar] [CrossRef]
- Nolan, J.M.; Power, R.; Stringham, J.; Dennison, J.; Stack, J.; Kelly, D.; Moran, R.; Akuffo, K.O.; Corcoran, L.; Beatty, S. Enrichment of macular pigment enhances contrast sensitivity in subjects free of retinal disease: Central Retinal enrichment supplementation trials—Report 1. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3429–3439. [Google Scholar] [CrossRef] [PubMed]
- Vishwanathan, R.; Iannaccone, A.; Scott, T.M.; Kritchevsky, S.B.; Jennings, B.J.; Carboni, G.; Forma, G.; Satterfield, S.; Harris, T.; Johnson, K.C. Macular pigment optical density is related to cognitive function in older people. Age Ageing 2014, 43, 271–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chew, E.Y.; Clemons, T.E.; Sangiovanni, J.P.; Danis, R.P.; Ferris, F.L., 3rd; Elman, M.J.; Antoszyk, A.N.; Ruby, A.J.; Orth, D.; Bressler, S.B.; et al. Secondary analyses of the effects of lutein/zeaxanthin on age-related macular degeneration progression: AREDS2 report No. 3. JAMA Ophthalmol. 2014, 132, 142–149. [Google Scholar] [CrossRef]
- Lin, J.H.; Lee, D.J.; Chang, J.S. Lutein production from biomass: Marigold flowers versus microalgae. Bioresour. Technol. 2015, 184, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Hauptmann, R.; Winner, B.L.; Blowers, A.; Smyser, C. Tagetes Erecta Marigolds with Altered Carotenoid Compositions and Ratios. U.S. Patent 6,784,351, 31 August 2004. [Google Scholar]
- Todd, P.H.; Locey, C.L.; Barren, J.P.; Vandenhombergh, A.P.; Berdahl, D.R.; Kanel, J.S. Capsicum Variety Exhibiting a Hyper-Accumulation of Zeaxanthin and Products Derived Therefrom. U.S. Patent 2012/0216321 A1, 23 August 2012. [Google Scholar]
- Andrewes, A.G.; Borch, G.L.; Liaaen-Jensen, S. Carotenoids of higher plants 7. * on the absolute configuration of lutein. Acta Chem. Scand. B 1974, 28, 139–140. [Google Scholar] [CrossRef] [Green Version]
- Vechpanich, J.; Shotipruk, A. Recovery of free lutein from tagetes erecta: Determination of suitable saponification and crystallization conditions. Sep. Sci. Technol. 2010, 46, 265–271. [Google Scholar] [CrossRef]
- Steiner, B.M.; McClements, D.J.; Davidov-Pardo, G. Encapsulation systems for lutein: A review. Trends Food Sci. Technol. 2018, 82, 71–81. [Google Scholar] [CrossRef]
- Li, B.; Vachali, P.P.; Shen, Z.; Gorusupudi, A.; Nelson, K.; Besch, B.M.; Bartschi, A.; Longo, S.; Mattinson, T.; Shihab, S.; et al. Retinal accumulation of zeaxanthin, lutein, and β-carotene in mice deficient in carotenoid cleavage enzymes. Exp. Eye Res. 2017, 159, 123–131. [Google Scholar] [CrossRef]
- Apanasenko, I.E.; Selyutina, O.Y.; Polyakov, N.E.; Suntsova, L.P.; Meteleva, E.S.; Dushkin, A.V.; Vachali, P.; Bernstein, P.S. Solubilization and stabilization of macular carotenoids by water soluble oligosaccharides and polysaccharides. Arch. Biochem. Biophys. 2015, 572, 58–65. [Google Scholar] [CrossRef] [Green Version]
- Olvera, R.M.; Quiroga, J.T. Absorption and Bioavailability of Carotenoids, Formulations and Applications. U.S. Patent 2008044475A1, 12 January 2008. [Google Scholar]
- Pavlović, N.; Goločorbin-Kon, S.; Ðanić, M.; Stanimirov, B.; Al-Salami, H.; Stankov, K.; Mikov, M. Bile acids and their derivatives as potential modifiers of drug release and pharmacokinetic profiles. Front. Pharm. 2018, 9, 1283. [Google Scholar] [CrossRef]
- Torres-Cardona, M.-D.; Torres-Quiroga, J.-O. Short Chain Diesters and Process for Making the Same. U.S. Patent 5959138A, 28 September 1999. [Google Scholar]
- Garavito, R.M.; Ferguson-Miller, S. Detergents as tools in membrane biochemistry. J. Biol. Chem. 2001, 276, 32403–32406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, D.; Nolan, J.M.; Howard, A.N.; Stack, J.; Akuffo, K.O.; Moran, R.; Thurnham, D.I.; Dennison, J.; Meagher, K.A.; Beatty, S. Serum and macular response to carotenoid-enriched egg supplementation in human subjects: The Egg Xanthophyll Intervention clinical Trial (EXIT). Br. J. Nutr. 2017, 117, 108–123. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T.; Mukherjee, A. Efficacy of diacetate esters of macular carotenoids: Effect of supplementation on macular pigment. J. Nutr. Metab. 2018, 2018, 4632081. [Google Scholar] [CrossRef] [Green Version]
- Landrum, J.; Bone, R.; Mendez, V.; Valenciaga, A.; Babino, D. Comparison of dietary supplementation with lutein diacetate and lutein: A pilot study of the effects on serum and macular pigment. Acta Biochim. Pol. 2012, 59, 167–169. [Google Scholar] [CrossRef] [Green Version]
- Green-Gomez, M.; Bernstein, P.S.; Curcio, C.A.; Moran, R.; Roche, W.; Nolan, J. Standardizing the assessment of macular pigment using a dual-wavelength autofluorescence technique. Transl. Vis. Sci. Technol. 2019, 8, 41. [Google Scholar] [CrossRef] [Green Version]
- Power, R.; Nolan, J.M.; Prado-Cabrero, A.; Coen, R.; Roche, W.; Power, T.; Howard, A.N.; Mulcahy, R. Targeted nutritional intervention for patients with mild cognitive impairment: The cognitive impairment study (CARES) Trial 1. J. Pers Med. 2020, 10, 43. [Google Scholar] [CrossRef]
- Chew, E.Y.; Clemons, T.E.; SanGiovanni, J.P.; Danis, R.; Ferris, F.L.; Elman, M.J.; Antoszyk, A.N.; Ruby, A.J.; O’Brien, A.; Orth, D.; et al. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: The Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013, 309, 2005–2015. [Google Scholar] [CrossRef]
- Nolan, J.M.; Meagher, K.A.; Howard, A.N.; Moran, R.; Thurnham, D.I.; Beatty, S. Lutein, zeaxanthin and meso-zeaxanthin content of eggs laid by hens supplemented with free and esterified xanthophylls. J. Nutr. Sci. 2016, 5, e1. [Google Scholar] [CrossRef] [Green Version]
- Carbonell-Capella, J.M.; Buniowska, M.; Barba, F.J.; Esteve, M.J.; Frígola, A. Analytical methods for determining bioavailability and bioaccessibility of bioactive compounds from fruits and vegetables: A review. Compr. Rev. Food Sci. Food Saf. 2014, 13, 155–171. [Google Scholar] [CrossRef]
- Sujak, A.; Gruszecki, W.I. Organization of mixed monomolecular layers formed with the xanthophyll pigments lutein or zeaxanthin and dipalmitoylphosphatidylcholine at the argon-water interface. J. Photochem. Photobiol. B 2000, 59, 42–47. [Google Scholar] [CrossRef]
- Trieschmann, M.; Beatty, S.; Nolan, J.M.; Hense, H.W.; Heimes, B.; Austermann, U.; Fobker, M.; Pauleikhoff, D. Changes in macular pigment optical density and serum concentrations of its constituent carotenoids following supplemental lutein and zeaxanthin: The LUNA study. Exp. Eye Res. 2007, 84, 718–728. [Google Scholar] [CrossRef]
- Nolan, J.; Loughman, J.; Akkali, M.C.; Stack, J.; Scanlon, G.; Davison, P.; Beatty, S. The impact of macular pigment augmentation on visual performance in normal subjects: COMPASS. Vis. Res. 2011, 51, 459–469. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; George, E.W.; Rognon, G.T.; Gorusupudi, A.; Ranganathan, A.; Chang, F.Y.; Shi, L.; Frederick, J.M.; Bernstein, P.S. Imaging lutein and zeaxanthin in the human retina with confocal resonance Raman microscopy. Proc. Natl. Acad. Sci. USA 2020. [Google Scholar] [CrossRef]
- Akuffo, K.O.; Nolan, J.M.; Howard, A.N.; Moran, R.; Stack, J.; Klein, R.; Klein, B.E.; Meuer, S.M.; Sabour-Pickett, S.; Thurnham, D.I.; et al. Sustained supplementation and monitored response with differing carotenoid formulations in early age-related macular degeneration. Eye 2015, 29, 902–912. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Subjects (n = 67) | Subjects Divided by Intervention Group | ||||
|---|---|---|---|---|---|---|
| Group 1 (n = 11) | Group 2 (n = 14) | Group 3 (n = 16) | Group 4 (n = 13) | Group 5 (n = 13) | ||
| Age (y) | 44.8 ± 10 | 46.0 ± 9.4 | 44.9 ± 8.9 | 41.6 ± 10.7 | 46.3 ± 12.2 | 46.1 ± 9.7 |
| Females, No. (%) | 32 (47.8) | 5 (45.5) | 7 (50) | 8 (50) | 5 (38.5) | 7 (53.8) |
| Smoking, No. (%) | ||||||
| Never | 32 (47.8) | 5 (45.4) | 7 (50.0) | 8 (50) | 5 (38.5) | 7 (53.8) |
| Former | 25 (37.3) | 4 (36.4) | 4 (28.6) | 6 (37.5) | 7 (53.8) | 4 (30.8) |
| Current | 10 (14.9) | 2 (18.2) | 3 (21.4) | 2 (12.5) | 1 (7.7) | 2 (15.4) |
| Education, No. (%) | ||||||
| High-school | 29 (43.3) | 2 (18.2) | 5 (35.7) | 7 (43.7) | 10 (76.9) | 5 (38.4) |
| College | 25 (37.3) | 7 (63.6) | 4 (28.6) | 6 (37.5) | 2 (15.4) | 6 (46.2) |
| Postgraduate | 13 (19.4) | 2 (18.2) | 5 (35.7) | 3 (18.8) | 1 (7.7) | 2 (15.4) |
| BMI [range] | 27.3 ± 5.6 [19–43] | 28.4 ± 6.1 [20–42] | 24.5 ± 4.5 [20–38] | 28.7 ± 6.9 [19–43] | 30.2 ± 5.3 [20–39] | 25.0 ± 3.3 [21–30] |
| Xanthophyll Carotenoid Concentrations (Serum and Tissue) | ||||||
| Serum L, μmol/L | 0.194 ± 0.096 | 0.184 ± 0.067 | 0.223 ± 0.116 | 0.188 ± 0.120 | 0.177 ± 0.108 | 0.187 ± 0.057 |
| Serum Z, μmol/L | 0.073 ± 0.029 | 0.074 ± 0.028 | 0.086 ± 0.038 | 0.071 ± 0.030 | 0.060 ± 0.022 | 0.073 ± 0.029 |
| MPOV [range] | 4553 ± 2095 [527–10,033] | 5263 ± 1789 [2243–8861] | 4793 ± 2885 [527–10,033] | 3890 ± 1925 [1327–7649] | 4277 ± 2115 [1027–8639] | 4784 ± 1446 [2632–7880] |
| Skin Carotenoid Score | 36,027 ± 12,458 | 37,970 ± 13,652 | 40,833 ± 15,063 | 34,656 ± 11,142 | 30,385 ± 12,065 | 36,538 ± 9173 |
| Carotenoid | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 |
|---|---|---|---|---|---|
| Lutein | 9.42 ± 0.11 | 5.80 ± 0.19 | 4.48 ± 0.07 | 10.24 ± 0.54 | 0 |
| Meso-zeaxanthin | 13.06 ± 0.15 | 8.12 ± 0.27 | 6.49 ± 0.12 | 10.62 ± 0.61 | 0 |
| Zeaxanthin | 2.12 ± 0.03 | 1.38 ± 0.04 | 1.75 ± 0.03 | 1.98 ± 0.11 | 0 |
| Dosage (capsule/day) | 1 | 2 | 2 | 1 | 1 |
| Total carotenoids ingested per day (mg) | 24.60 | 30.60 | 25.44 | 22.84 | 0 |
| Intervention | Outcome (μmol/L) | |||||
|---|---|---|---|---|---|---|
| L | Z | MZ | MPOV | Skin | ||
| Group 1 (n = 11) | 0 Mo | 0.18 ± 0.07 | 0.07 ± 0.03 | 0 | 5263 ± 1789 | 37,970 ± 13,652 |
| 6 Mo | 0.61 ± 0.25 | 0.09 ± 0.03 | 0.06 ± 0.03 | 5943 ± 1567 | 52,303 ± 15,253 | |
| Change | 0.43 ± 0.22 | 0.02 ± 0.02 | 0.06 ± 0.03 | 680 ± 661 | 14,333 ± 8467 | |
| p value 2 | <0.001 | 0.007 | <0.001 | 0.039 | 0.024 | |
| Group 2 (n = 14) | 0 Mo | 0.22 ± 0.12 | 0.09 ± 0.04 | 0 | 4793 ± 2885 | 40,833 ± 15,063 |
| 6 Mo | 0.56 ± 0.29 | 0.09 ± 0.02 | 0.04 ± 0.03 | 5802 ± 3254 | 48,571 ± 10,921 | |
| Change | 0.34 ± 0.29 | 0.00 ± 0.03 | 0.04 ± 0.03 | 1010 ± 914 | 7738 ± 9369 | |
| p value 2 | 0.001 | 0.366 | <0.001 | 0.006 | 0.543 | |
| Group 3 (n = 16) | 0 Mo | 0.19 ± 0.12 | 0.07 ± 0.03 | 0 | 3890 ± 1925 | 34,656 ± 11,142 |
| 6 Mo | 0.52 ± 0.29 | 0.09 ± 0.03 | 0.04 ± 0.03 | 4911 ± 1846 | 45,542 ± 10,750 | |
| Change | 0.33 ± 0.25 | 0.02 ± 0.03 | 0.04 ± 0.03 | 1021 ± 743 | 10,885 ± 7115 | |
| p value 2 | <0.001 | 0.008 | <0.001 | 0.001 | 0.087 | |
| Group 4 (n = 13) | 0 Mo | 0.18 ± 0.11 | 0.06 ± 0.02 | 0 | 4277 ± 2115 | 30,385 ± 12,065 |
| 6 Mo | 0.58 ± 0.43 | 0.11 ± 0.05 | 0.16 ± 0.15 | 5331 ± 2061 | 47,718 ± 12,718 | |
| Change | 0.40 ± 0.38 | 0.05 ± 0.04 | 0.16 ± 0.15 | 1054 ± 680 | 17,333 ± 12,664 | |
| p value 2 | 0.002 | <0.001 | 0.001 | 0.001 | 0.012 | |
| Group 5 (n = 13) | 0 Mo | 0.19 ± 0.06 | 0.07 ± 0.03 | 0 | 4784 ± 1446 | 36,538 ± 9173 |
| 6 Mo | 0.18 ± 0.06 | 0.07 ± 0.02 | 0 | 4894 ± 1581 | 42,077 ± 9557 | |
| Change | −0.01 ± 0.05 | 0.00 ± 0.01 | 0 | 110 ± 606 | 5539 ± 9125 | |
| p value 2 | - | - | - | - | - | |
| Outcome | Group 4 vs. Group 1 | Group 4 vs. Group 2 | Group 4 vs. Group 3 | |||
|---|---|---|---|---|---|---|
| Difference in Change | p-Value | Difference in Change | p-Value | Difference in Change | p-Value | |
| L | −0.027 (−0.297 to 0.244) | 0.839 | 0.056 (−0.208 to 0.320) | 0.666 | 0.070 (−0.175 to 0.315) | 0.563 |
| Z | 0.033 (0.006 to 0.059) | 0.018 | 0.045 (0.018 to 0.072) | 0.002 | 0.030 (0.005 to 0.055) | 0.019 |
| MZ | 0.109 (0.020 to 0.197) | 0.019 | 0.124 (0.036 to 0.211) | 0.009 | 0.126 (0.039 to 0.214) | 0.008 |
| MPOV | 374 (−196 to 944) | 0.187 | 45 (−598 to 687) | 0.888 | 33 (−515 to 581) | 0.903 |
| SKIN | 3000 (−6310 to 12,310) | 0.511 | 9595 (811 to 18,379) | 0.034 | 6448 (−1191 to 14,087) | 0.095 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Green-Gomez, M.; Prado-Cabrero, A.; Moran, R.; Power, T.; Gómez-Mascaraque, L.G.; Stack, J.; Nolan, J.M. The Impact of Formulation on Lutein, Zeaxanthin, and meso-Zeaxanthin Bioavailability: A Randomised Double-Blind Placebo-Controlled Study. Antioxidants 2020, 9, 767. https://doi.org/10.3390/antiox9080767
Green-Gomez M, Prado-Cabrero A, Moran R, Power T, Gómez-Mascaraque LG, Stack J, Nolan JM. The Impact of Formulation on Lutein, Zeaxanthin, and meso-Zeaxanthin Bioavailability: A Randomised Double-Blind Placebo-Controlled Study. Antioxidants. 2020; 9(8):767. https://doi.org/10.3390/antiox9080767
Chicago/Turabian StyleGreen-Gomez, Marina, Alfonso Prado-Cabrero, Rachel Moran, Tommy Power, Laura G. Gómez-Mascaraque, Jim Stack, and John M. Nolan. 2020. "The Impact of Formulation on Lutein, Zeaxanthin, and meso-Zeaxanthin Bioavailability: A Randomised Double-Blind Placebo-Controlled Study" Antioxidants 9, no. 8: 767. https://doi.org/10.3390/antiox9080767