Antioxidants as a Potential Target against Inflammation and Oxidative Stress in Attention-Deficit/Hyperactivity Disorder

 ,
,
Abstract
:1. Introduction
1.1. Attention-Deficit/Hyperactivity Disorder
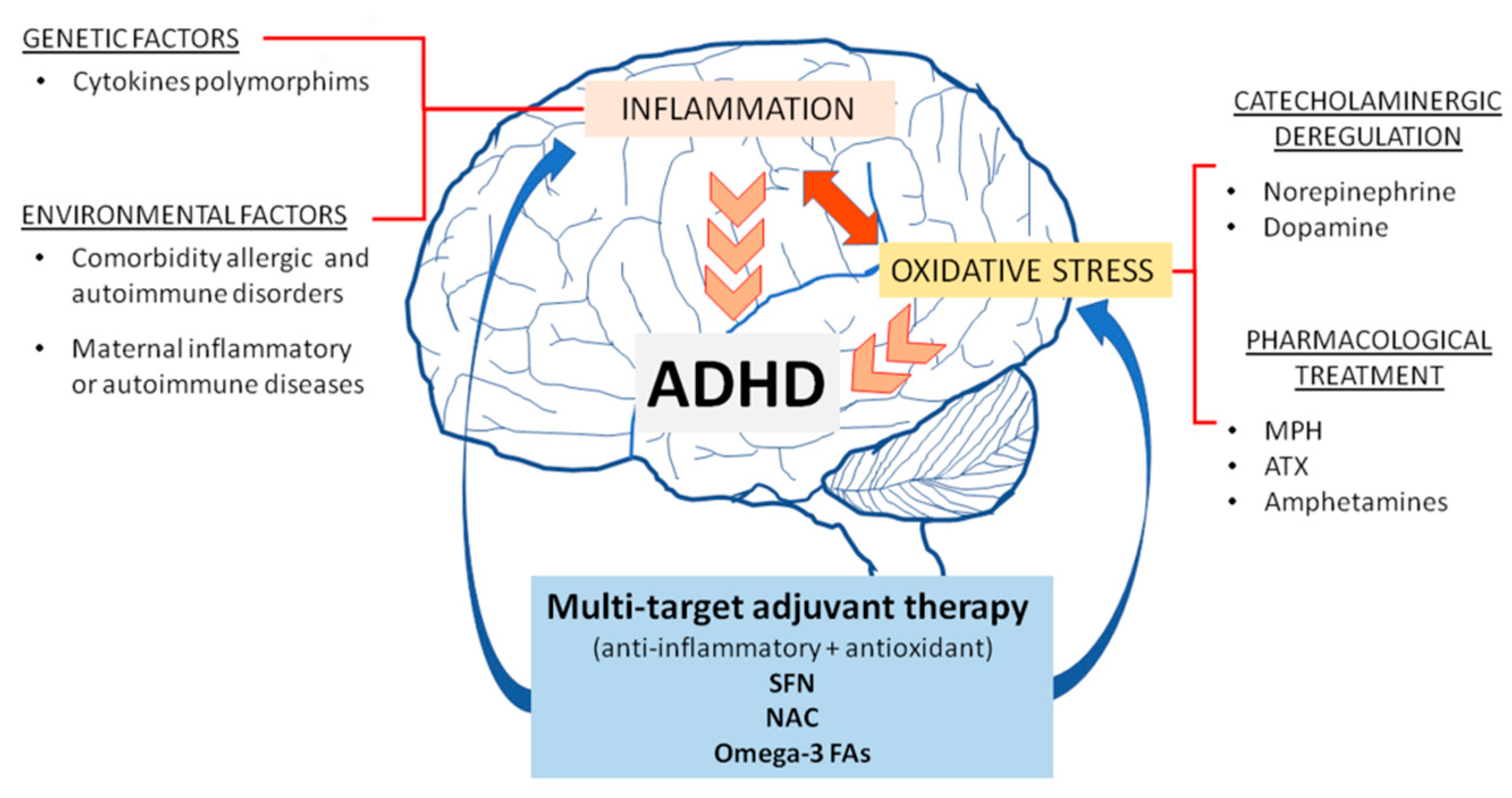
1.2. Pathophysiology
1.3. Pharmacological Treatment
2. Inflammation and the Relationship with ADHD
3. Antioxidant Treatment Against Inflammation in ADHD
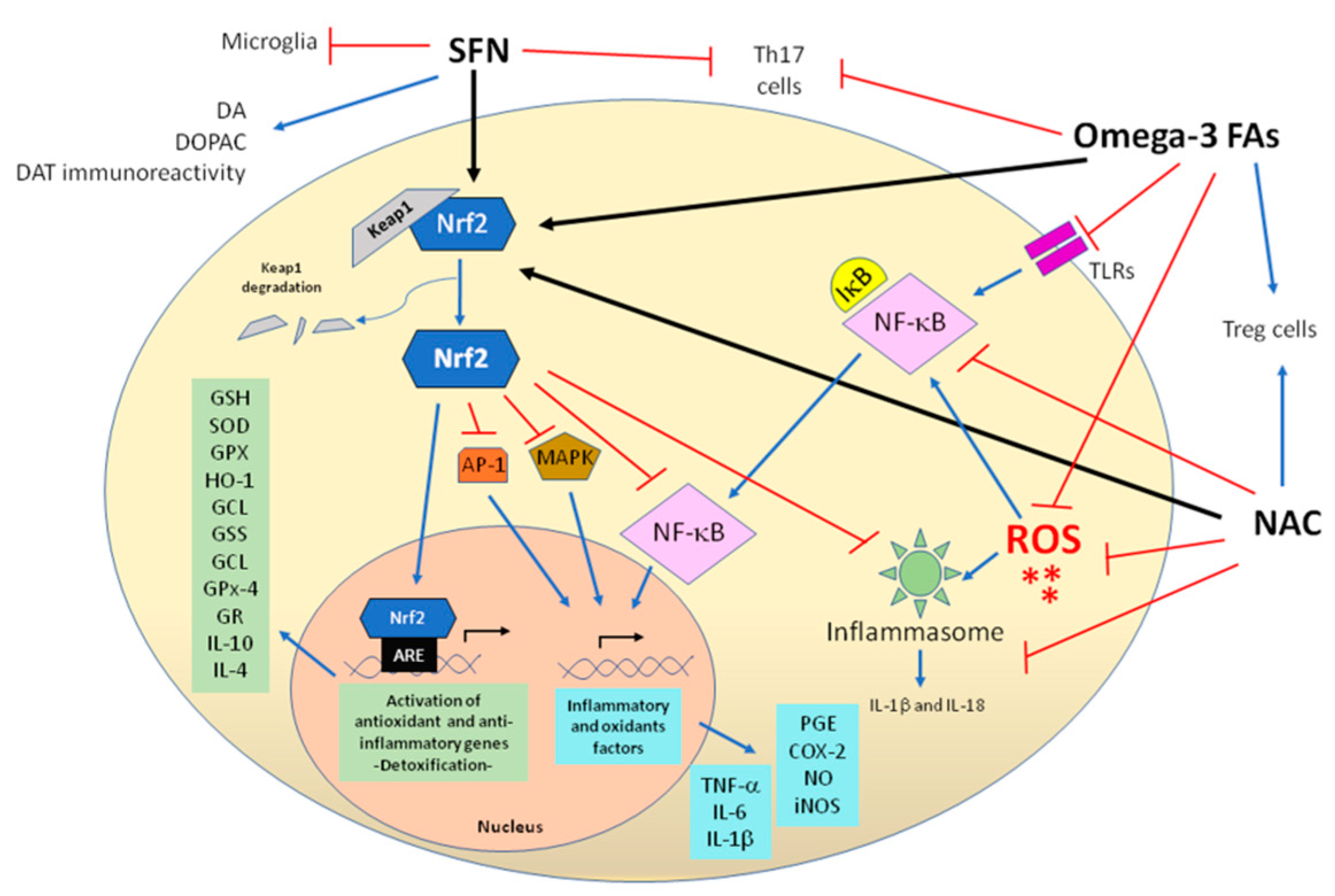
3.1. Sulforaphane Exerts Anti-Inflammatory Activity
3.2. N-Acetylcysteine Decreases Inflammatory Response
3.3. Omega-3 Fatty Acids Prevent Inflammation
4. Oxidative Stress and the Relationship with ADHD
5. Antioxidant Treatment Against Oxidative Stress in ADHD
5.1. Sulforaphane Exerts Antioxidant Activity
5.2. N-Acetylcysteine Exerts Antioxidant Activity
5.3. Omega-3 Fatty Acids Exert Antioxidant Activity
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Faraone, S.V.; Asherson, P.; Banaschewski, T.; Biederman, J.; Buitelaar, J.K.; Ramos-Quiroga, J.A.; Rohde, L.A.; Sonuga-Barke, E.J.; Tannock, R.; Franke, B. Attention-Deficit/Hyperactivity Disorder. Nat. Rev. Dis. Primers 2015, 1, 15020. [Google Scholar] [CrossRef] [PubMed]
- Corona, J.C. Natural Compounds for the Management of Parkinson’s Disease and Attention-Deficit/Hyperactivity Disorder. BioMed Res. Int. 2018, 2018, 4067597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polanczyk, G.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The Worldwide Prevalence of ADHD: A Systematic Review and Metaregression Analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Sayal, K.; Prasad, V.; Daley, D.; Ford, T.; Coghill, D. ADHD in Children and Young People: Prevalence, Care Pathways, and Service Provision. Lancet Psychiatry 2018, 5, 175–186. [Google Scholar] [CrossRef]
- Willcutt, E.G. The Prevalence of DSM-IV Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Wolraich, M.L.; Hagan, J.F.; Allan, C.; Chan, E.; Davison, D.; Earls, M.; Evans, S.W.; Flinn, S.K.; Froehlich, T.; Frost, J.; et al. Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics 2019, 144, e20192528. [Google Scholar] [CrossRef] [Green Version]
- Wilens, T.E.; Faraone, S.V.; Biederman, J. Attention-Deficit/Hyperactivity Disorder in Adults. JAMA 2004, 292, 619–623. [Google Scholar] [CrossRef]
- Jensen, P.S.; Hinshaw, S.P.; Kraemer, H.C.; Lenora, N.; Newcorn, J.H.; Abikoff, H.B.; March, J.S.; Arnold, L.E.; Cantwell, D.P.; Conners, C.K.; et al. ADHD Comorbidity Findings from the MTA Study: Comparing Comorbid Subgroups. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 147–158. [Google Scholar] [CrossRef]
- Tejeda-Romero, C.; Kobashi-Margáin, R.A.; Alvarez-Arellano, L.; Corona, J.C.; González-García, N. Differences in Substance Use, Psychiatric Disorders and Social Factors between Mexican Adolescents and Young Adults. Am. J. Addict. 2018, 27, 625–631. [Google Scholar] [CrossRef]
- Newcorn, J.H.; Halperin, J.M.; Jensen, P.S.; Abikoff, H.B.; Arnold, L.E.; Cantwell, D.P.; Conners, C.K.; Elliott, G.R.; Epstein, J.N.; Greenhill, L.L.; et al. Symptom Profiles in Children with ADHD: Effects of Comorbidity and Gender. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 137–146. [Google Scholar] [CrossRef]
- Del Campo, N.; Chamberlain, S.R.; Sahakian, B.J.; Robbins, T.W. The Roles of Dopamine and Noradrenaline in the Pathophysiology and Treatment of Attention-Deficit/Hyperactivity Disorder. Boil. Psychiatry 2011, 69, e145–e157. [Google Scholar] [CrossRef] [PubMed]
- Prince, J. Catecholamine Dysfunction in Attention-Deficit/Hyperactivity Disorder: An Update. J. Clin. Psychopharmacol. 2008, 28, S39–S45. [Google Scholar] [CrossRef] [PubMed]
- Instanes, J.T.; Halmøy, A.; Engeland, A.; Haavik, J.; Furu, K.; Klungsøyr, K. Attention-Deficit/Hyperactivity Disorder in Offspring of Mothers with Inflammatory and Immune System Diseases. Boil. Psychiatry 2017, 81, 452–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, G.A.; Nigg, J.T.; Sullivan, E.L. Neuroinflammation as a Risk Factor for Attention Deficit Hyperactivity Disorder. Pharmacol. Biochem. Behav. 2019, 182, 22–34. [Google Scholar] [CrossRef]
- Lopresti, A.L. Oxidative and Nitrosative Stress in ADHD: Possible Causes and the Potential of Antioxidant-Targeted Therapies. ADHD Atten. Deficit Hyperact. Disord. 2015, 7, 237–247. [Google Scholar] [CrossRef]
- Joseph, N.; Zhang-James, Y.; Perl, A.; Faraone, S.V. Oxidative Stress and ADHD: A Meta-Analysis. J. Atten. Disord. 2015, 19, 915–924. [Google Scholar] [CrossRef]
- Koda, K.; Ago, Y.; Cong, Y.; Kita, Y.; Takuma, K.; Matsuda, T. Effects of Acute and Chronic Administration of Atomoxetine and Methylphenidate on Extracellular Levels of Noradrenaline, Dopamine and Serotonin in the Prefrontal Cortex and Striatum of Mice. J. Neurochem. 2010, 114, 259–270. [Google Scholar] [CrossRef]
- Cinnamon Bidwell, L.; Dew, R.E.; Kollins, S.H. Alpha-2 Adrenergic Receptors and Attention-Deficit/Hyperactivity Disorder. Curr. Psychiatry Rep. 2010, 12, 366–373. [Google Scholar] [CrossRef] [Green Version]
- Bymaster, F.; Katner, J.S.; Nelson, D.L.; Hemrick-Luecke, S.K.; Threlkeld, P.G.; Heiligenstein, J.H.; Morin, S.M.; Gehlert, D.R.; Perry, K.W. Atomoxetine Increases Extracellular Levels of Norepinephrine and Dopamine in Prefrontal Cortex of Rat: A Potential Mechanism for Efficacy in Attention Deficit/Hyperactivity Disorder. Neuropsychopharmacology 2002, 27, 699–711. [Google Scholar] [CrossRef]
- Clemow, D.B. Misuse of Methylphenidate. Curr. Top Behav. Neurosci. 2017, 34, 99–124. [Google Scholar]
- Swanson, J.M.; Elliott, G.R.; Greenhill, L.L.; Wigal, T.; Arnold, L.E.; Vitiello, B.; Hechtman, L.; Epstein, J.N.; Pelham, W.E.; Abikoff, H.B.; et al. Effects of Stimulant Medication on Growth Rates Across 3 Years in the MTA Follow-up. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 1015–1027. [Google Scholar] [CrossRef] [PubMed]
- Reed, V.A.; Buitelaar, J.K.; Anand, E.; Day, K.A.; Treuer, T.; Upadhyaya, H.P.; Coghill, D.R.; Kryzhanovskaya, L.A.; Savill, N.C. The Safety of Atomoxetine for the Treatment of Children and Adolescents with Attention-Deficit/Hyperactivity Disorder: A Comprehensive Review of Over a Decade of Research. CNS Drugs 2016, 30, 603–628. [Google Scholar] [CrossRef] [PubMed]
- Taghizadeh, M.; Tamtaji, O.R.; Dadgostar, E.; Kakhaki, R.D.; Bahmani, F.; Abolhassani, J.; Aarabi, M.H.; Kouchaki, E.; Memarzadeh, M.R.; Asemi, Z. The Effects of Omega-3 Fatty Acids and Vitamin E Co-Supplementation on Clinical and Metabolic Status in Patients with Parkinson’s disease: A randomized, double-blind, placebo-controlled trial. Neurochem. Int. 2017, 108, 183–189. [Google Scholar] [CrossRef]
- Adair, J.C.; Knoefel, J.E.; Morgan, N. Controlled Trial of N-Acetylcysteine for Patients with Probable Alzheimer’s disease. Neurology 2001, 57, 1515–1517. [Google Scholar] [CrossRef]
- Puri, B.K.; Leavitt, B.R.; Hayden, M.; Ross, C.A.; Rosenblatt, A.; Greenamyre, J.T.; Hersch, S.; Vaddadi, K.S.; Sword, A.; Horrobin, D.F.; et al. Ethyl-EPA in Huntington Disease: A Double-Blind, Randomized, Placebo-Controlled Trial. Neurology. 2005, 65, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Sedlak, T.W.; Nucifora, L.G.; Koga, M.; Shaffer, L.S.; Higgs, C.; Tanaka, T.; Wang, A.M.; Coughlin, J.M.; Barker, P.B.; Fahey, J.W.; et al. Sulforaphane Augments Glutathione and Influences Brain Metabolites in Human Subjects: A Clinical Pilot Study. Mol. Neuropsychiatry 2018, 3, 214–222. [Google Scholar] [CrossRef]
- Lynch, R.; Diggins, E.L.; Connors, S.L.; Zimmerman, A.W.; Singh, K.; Liu, H.; Talalay, P.; Fahey, J.W. Sulforaphane from Broccoli Reduces Symptoms of Autism: A Follow-up Case Series from a Randomized Double-blind Study. Glob. Adv. Health Med. 2017, 6. [Google Scholar] [CrossRef]
- Ellegaard, P.K.; Licht, R.W.; Poulsen, H.E.; Nielsen, R.E.; Berk, M.; Dean, O.M.; Mohebbi, M.; Nielsen, C.T. Add-On Treatment with N-Acetylcysteine for Bipolar Depression: A 24-Week Randomized Double-Blind Parallel Group Placebo-Controlled Multicentre Trial (NACOS-Study Protocol). Int. J. Bipolar Disord. 2018, 6, 11. [Google Scholar] [CrossRef]
- Shabab, T.; Khanabdali, R.; Moghadamtousi, S.Z.; Kadir, H.A.; Mohan, G. Neuroinflammation Pathways: A General Review. Int. J. Neurosci. 2017, 127, 624–633. [Google Scholar] [CrossRef]
- Kohman, R.A.; Rhodes, J.S. Neurogenesis, Inflammation and Behavior. Brain Behav. Immun. 2013, 27, 22–32. [Google Scholar] [CrossRef]
- Oades, R.D.; Myint, A.-M.; Dauvermann, M.R.; Schimmelmann, B.G.; Schwarz, M.J. Attention-Deficit Hyperactivity Disorder (ADHD) and Glial Integrity: An Exploration of Associations of Cytokines and Kynurenine Metabolites with Symptoms and Attention. Behav. Brain Funct. 2010, 6, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darwish, A.H.; Elgohary, T.M.; Nosair, N.A. Serum Interleukin-6 Level in Children with Attention-Deficit Hyperactivity Disorder (ADHD). J. Child Neurol. 2019, 34, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Donfrancesco, R.; Nativio, P.; Di Benedetto, A.; Villa, M.P.; Andriola, E.; Melegari, M.G.; Cipriano, E.; Di Trani, M. Anti-Yo Antibodies in Children with ADHD: First Results About Serum Cytokines. J. Atten. Disord. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozłowska, A.; Wojtacha, P.; Równiak, M.; Kolenkiewicz, M.; Huang, A.C.W. ADHD Pathogenesis in the Immune, Endocrine and Nervous Systems of Juvenile and Maturating SHR and WKY Rats. Psychopharmacology 2019, 236, 2937–2958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawley, L.C.; Hueston, C.M.; O’Leary, J.D.; Kozareva, D.A.; Cryan, J.F.; O’Leary, O.F.; Nolan, Y.M. Chronic Intrahippocampal Interleukin-1β Overexpression in Adolescence Impairs Hippocampal Neurogenesis but not Neurogenesis-Associated Cognition. Brain Behav. Immun. 2020, 83, 172–179. [Google Scholar] [CrossRef]
- Augusto-Oliveira, M.; Arrifano, G.P.; Lopes-Araujo, A.; Santos-Sacramento, L.; Takeda, P.Y.; Anthony, D.C.; Malva, J.O.; Crespo-Lopez, M.E. What Do Microglia Really Do in Healthy Adult Brain? Cells 2019, 8, 1293. [Google Scholar] [CrossRef] [Green Version]
- Yirmiya, R.; Goshen, I. Immune Modulation of Learning, Memory, Neural Plasticity and Neurogenesis. Brain Behav. Immun. 2011, 25, 181–213. [Google Scholar] [CrossRef]
- Buske-Kirschbaum, A.; Schmitt, J.; Plessow, F.; Romanos, M.; Weidinger, S.; Roessner, V. Psychoendocrine and Psychoneuroimmunological Mechanisms in the Comorbidity of Atopic Eczema and Attention Deficit/Hyperactivity Disorder. Psychoneuroendocrinology 2013, 38, 12–23. [Google Scholar] [CrossRef]
- Drtilkova, I.; Sery, O.; Theiner, P.; Uhrova, A.; Zackova, M.; Balastikova, B.; Znojil, V. Clinical and Molecular-Genetic Markers of ADHD in Children. Neuroendocrinol. Lett. 2008, 29, 320–327. [Google Scholar]
- Segman, R.H.; Meltzer, A.; Gross-Tsur, V.; Kosov, A.; Frisch, A.; Inbar, E.; Darvasi, A.; Levy, S.; Goltser, T.; Weizman, A.; et al. Preferential Transmission of Interleukin-1 Receptor Antagonist Alleles in Attention Deficit Hyperactivity Disorder. Mol. Psychiatry 2002, 7, 72–74. [Google Scholar] [CrossRef]
- Misener, V.L.; Schachar, R.; Ickowicz, A.; Malone, M.; Roberts, W.; Tannock, R.; Kennedy, J.L.; Pathare, T.; Barr, C.L. Replication Test for Association of the IL-1 Receptor Antagonist Gene, IL1RN, with Attention-Deficit/Hyperactivity Disorder. Neuropsychobiology 2004, 50, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-J.; Yu, Y.-H.; Fu, M.-L.; Yeh, W.-T.; Hsu, J.-L.; Yang, Y.-H.; Chen, W.J.; Chiang, B.-L.; Pan, W.-H. Attention Deficit-Hyperactivity Disorder is Associated with Allergic Symptoms and Low Levels of Hemoglobin and Serotonin. Sci. Rep. 2018, 8, 10229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.-F.; Yang, C.-C.; Wang, I.-J. Association between Allergic Diseases, Allergic Sensitization and Attention-Deficit/Hyperactivity Disorder in Children: A Large-Scale, Population-Based Study. J. Chin. Med. Assoc. 2018, 81, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.R.; Benros, M.E.; Dalsgaard, S. Associations Between Autoimmune Diseases and Attention-Deficit/Hyperactivity Disorder: A Nationwide Study. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Sun, S.; Zhang, J.; Sharma, E.; Chang, Z.; Kuja-Halkola, R.; Almqvist, C.; Larsson, H.; Faraone, S.V. Association Between Attention Deficit Hyperactivity Disorder and Asthma: A Systematic Review and Meta-Analysis and a Swedish Population-Based Study. Lancet Psychiatry 2018, 5, 717–726. [Google Scholar] [CrossRef]
- Zhu, Z.; Zhu, X.; Liu, C.-L.; Shi, H.; Shen, S.; Yang, Y.; Hasegawa, K.; Camargo, C.A.; Liang, L. Shared Genetics of Asthma and Mental Health Disorders: A Large-Scale Genome-Wide Cross-Trait Analysis. Eur. Respir. J. 2019, 54, 1901507. [Google Scholar] [CrossRef]
- Rosenkranz, M.A.; Busse, W.W.; Johnstone, T.; Swenson, C.A.; Crisafi, G.M.; Jackson, M.M.; Bosch, J.A.; Sheridan, J.F.; Davidson, R.J. Neural Circuitry Underlying the Interaction between Emotion and Asthma Symptom Exacerbation. Proc. Natl. Acad. Sci. USA 2005, 102, 13319–13324. [Google Scholar] [CrossRef] [Green Version]
- Passarelli, F.; Donfrancesco, R.; Nativio, P.; Pascale, E.; Di Trani, M.; Patti, A.M.; Vulcano, A.; Gozzo, P.; Villa, M.P. Anti-Purkinje Cell Antibody as a Biological Marker in Attention Deficit/Hyperactivity Disorder: A Pilot Study. J. Neuroimmunol. 2013, 258, 67–70. [Google Scholar] [CrossRef]
- Giana, G.; Romano, E.; Porfirio, M.C.; D’Ambrosio, R.; Giovinazzo, S.; Troianiello, M.; Barlocci, E.; Travaglini, D.; Granstrem, O.; Pascale, E.; et al. Detection of Auto-Antibodies to DAT in the Serum: Interactions with DAT Genotype and Psycho-Stimulant Therapy for ADHD. J. Neuroimmunol. 2015, 278, 212–222. [Google Scholar] [CrossRef]
- Toto, M.; Margari, F.; Simone, M.; Craig, F.; Petruzzelli, M.G.; Tafuri, S.; Margari, L. Antibasal Ganglia Antibodies and Antistreptolysin O in Noncomorbid ADHD. J. Atten. Disord. 2015, 19, 965–970. [Google Scholar] [CrossRef]
- Rivera, H.M.; Christiansen, K.J.; Sullivan, E.L. The Role of Maternal Obesity in the Risk of Neuropsychiatric Disorders. Front. Mol. Neurosci. 2015, 9, 194. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; A Klomparens, E. The Neuroprotective Mechanisms and Effects of Sulforaphane. Brain Circ. 2019, 5, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Sova, M.; Saso, L. Design and Development of Nrf2 Modulators for Cancer Chemoprevention and Therapy: A Review. Drug Des. Dev. Ther. 2018, 12, 3181–3197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinkova-Kostova, A.T.; Abramov, A.Y. The Emerging Role of Nrf2 in Mitochondrial Function. Free Radic. Boil. Med. 2015, 88, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, R.E. The Effects of Dietary Supplements That Overactivate the Nrf2/ARE System. Curr. Med. Chem. 2019, 26, 1. [Google Scholar] [CrossRef]
- Hashimoto, K. Recent Advances in the Early Intervention in Schizophrenia: Future Direction from Preclinical Findings. Curr. Psychiatry Rep. 2019, 21, 75. [Google Scholar] [CrossRef]
- Singh, K.; Connors, S.L.; Macklin, E.A.; Smith, K.D.; Fahey, J.W.; Talalay, P.; Zimmerman, A.W. Sulforaphane Treatment of Autism Spectrum Disorder (ASD). Proc. Natl. Acad. Sci. USA 2014, 111, 15550–15555. [Google Scholar] [CrossRef] [Green Version]
- Myzak, M.C.; Dashwood, R.H. Chemoprotection by Sulforaphane: Keep One Eye beyond Keap1. Cancer Lett. 2006, 233, 208–218. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.M.U.; Luo, L.; Namani, A.; Wang, X.J.; Tang, X. Nrf2 Signaling Pathway: Pivotal Roles in Inflammation. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2017, 1863, 585–597. [Google Scholar] [CrossRef]
- Aladaileh, S.H.; Hussein, O.E.; Abukhalil, M.H.; Saghir, S.A.M.; Bin-Jumah, M.; Alfwuaires, M.A.; Germoush, M.O.; Almaiman, A.A.; Mahmoud, A.M. Formononetin Upregulates Nrf2/HO-1 Signaling and Prevents Oxidative Stress, Inflammation and Kidney Injury in Methotrexate-Induced Rats. Antioxidants 2019, 8, 430. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Peng, G.; Yang, F.; Zhang, Y.; Mu, Z.; Han, X. Sulforaphane Has a Therapeutic Effect in an Atopic Dermatitis Murine Model and Activates the Nrf2/HO-1 axis. Mol. Med. Rep. 2019, 20, 1761–1771. [Google Scholar] [CrossRef] [Green Version]
- Subedi, L.; Lee, J.H.; Yumnam, S.; Ji, E.; Kim, S.Y. Anti-Inflammatory Effect of Sulforaphane on LPS-Activated Microglia Potentially through JNK/AP-1/NF-kappaB Inhibition and Nrf2/HO-1 Activation. Cells 2019, 8, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, T.; Xu, F.; Yan, X.; Li, S.; Li, H. Sulforaphane Exerts Anti-Inflammatory Effects against Lipopolysaccharide-Induced Acute Lung Injury in Mice through the Nrf2/ARE Pathway. Int. J. Mol. Med. 2016, 37, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.-F.; Shen, X.-Y.; Lio, C.K.; Dai, Y.; Cheng, C.-S.; Liu, J.-X.; Yao, Y.-D.; Yu, Y.; Xie, Y.; Luo, P.; et al. Activation of Nrf2/HO-1 Pathway by Nardochinoid C Inhibits Inflammation and Oxidative Stress in Lipopolysaccharide-Stimulated Macrophages. Front. Pharmacol. 2018, 9, 911. [Google Scholar] [CrossRef] [PubMed]
- Rakariyatham, K.; Wu, X.; Tang, Z.; Han, Y.; Wang, Q.; Xiao, H. Synergism between Luteolin and Sulforaphane in Anti-Inflammation. Food Funct. 2018, 9, 5115–5123. [Google Scholar] [CrossRef]
- Greaney, A.J.; Maier, N.K.; Leppla, S.H.; Moayeri, M. Sulforaphane Inhibits Multiple Inflammasomes through an Nrf2-Independent Mechanism. J. Leukoc. Biol. 2016, 99, 189–199. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Ahn, H.; Hong, E.-J.; An, B.-S.; Jeung, E.-B.; Lee, G.-S. Sulforaphane Attenuates Activation of NLRP3 and NLRC4 Inflammasomes but not AIM2 Inflammasome. Cell. Immunol. 2016, 306, 53–60. [Google Scholar] [CrossRef]
- Zhao, C.; Gillette, D.D.; Li, X.; Zhang, Z.; Wen, H. Nuclear Factor E2-Related Factor-2 (Nrf2) Is Required for NLRP3 and AIM2 Inflammasome Activation. J. Boil. Chem. 2014, 289, 17020–17029. [Google Scholar] [CrossRef] [Green Version]
- Dwivedi, S.; Rajasekar, N.; Hanif, K.; Nath, C.; Shukla, R. Sulforaphane Ameliorates Okadaic Acid-Induced Memory Impairment in Rats by Activating the Nrf2/HO-1 Antioxidant Pathway. Mol. Neurobiol. 2016, 53, 5310–5323. [Google Scholar] [CrossRef]
- Nadeem, A.; Ahmad, S.F.; Al-Harbi, N.O.; Attia, S.M.; Bakheet, S.A.; Ibrahim, K.E.; Alqahtani, F.; Alqinyah, M. Nrf2 Activator, Sulforaphane Ameliorates Autism-Like Symptoms through Suppression of Th17 Related Signaling and Rectification of Oxidant-Antioxidant Imbalance in Periphery and Brain of BTBR T+tf/J mice. Behav. Brain Res. 2019, 364, 213–224. [Google Scholar] [CrossRef]
- Fernandes, J.; Gupta, G.L. N-acetylcysteine Attenuates Neuroinflammation Associated Depressive Behavior Induced by Chronic Unpredictable Mild Stress in Rat. Behav. Brain Res. 2019, 364, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Panizzutti, B.; Bortolasci, C.; Hasebe, K.; Kidnapillai, S.; Gray, L.; Walder, K.; Berk, M.; Mohebbi, M.; Dodd, S.; Gama, C.; et al. Mediator Effects of Parameters of Inflammation and Neurogenesis from a N-Acetyl Cysteine Clinical-Trial for Bipolar Depression. Acta Neuropsychiatr. 2018, 30, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Garcia, R.J.; Francis, L.; Dawood, M.; Lai, Z.-W.; Faraone, S.V.; Perl, A. Attention Deficit and Hyperactivity Disorder Scores Are Elevated and Respond to N-Acetylcysteine Treatment in Patients with Systemic Lupus Erythematosus. Arthritis Rheum. 2013, 65, 1313–1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, Z.-W.; Hanczko, R.; Bonilla, E.; Caza, T.N.; Clair, B.; Bartos, A.; Miklóssy, G.; Jimah, J.; Doherty, E.; Tily, H.; et al. N-Acetylcysteine Reduces Disease Activity by Blocking Mammalian Target of Rapamycin in T Cells from Systemic Lupus Erythematosus Patients: A Randomized, Double-Blind, Placebo-Controlled Trial. Arthritis Rheum. 2012, 64, 2937–2946. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Chen, F.; Wang, W.; Zhang, X.-D. Hydrogen Sulfide Attenuates High Glucose-Induced Human Retinal Pigment Epithelial Cell Inflammation by Inhibiting ROS Formation and NLRP3 Inflammasome Activation. Mediat. Inflamm. 2019, 2019, 8908960. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Wahab, W.M.; I Moussa, F. Neuroprotective Effect of N-Acetylcysteine against Cisplatin-Induced Toxicity in Rat Brain by Modulation of Oxidative Stress and Inflammation. Drug Des. Dev. Ther. 2019, 13, 1155–1162. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.W.; Kwon, M.-J.; Choi, A.M.K.; Kim, H.-P.; Nakahira, K.; Hwang, D.H. Fatty Acids Modulate Toll-like Receptor 4 Activation through Regulation of Receptor Dimerization and Recruitment into Lipid Rafts in a Reactive Oxygen Species-dependent Manner. J. Boil. Chem. 2009, 284, 27384–27392. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, J.A.; Wold, A.E.; Sandberg, A.S.; Ostman, S.M. The Polyunsaturated Fatty Acids Arachidonic Acid and Docosahexaenoic Acid Induce Mouse Dendritic Cells Maturation but Reduce T-Cell Responses in Vitro. PLoS ONE 2015, 10, e0143741. [Google Scholar] [CrossRef]
- Kim, W.; Barhoumi, R.; McMurray, D.N.; Chapkin, R.S. Dietary Fish Oil and DHA Down-Regulate Antigen-Activated CD4+ T-Cells While Promoting the Formation of Liquid-Ordered Mesodomains. Br. J. Nutr. 2014, 111, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Monk, J.M.; Hou, T.Y.; Turk, H.F.; McMurray, D.N.; Chapkin, R.S. n3 PUFAs Reduce Mouse CD4+ T-cell Ex Vivo Polarization into Th17 Cells. J. Nutr. 2013, 143, 1501–1508. [Google Scholar] [CrossRef]
- Hariri, M.; Djazayery, A.; Djalali, M.; Saedisomeolia, A.; Rahimi, A.; Abdolahian, E. Effect of n-3 Supplementation on Hyperactivity, Oxidative Stress and Inflammatory Mediators in Children with Attention-Deficit-Hyperactivity Disorder. Malays. J. Nutr. 2012, 18, 329–335. [Google Scholar] [PubMed]
- Chen, H.; Wu, J.; Zhang, J.; Fujita, Y.; Ishima, T.; Iyo, M.; Hashimoto, K. Protective Effects of the Antioxidant Sulforaphane on Behavioral Changes and Neurotoxicity in Mice after the Administration of Methamphetamine. Psychopharmacology 2012, 222, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Pauletti, A.; Terrone, G.; Shekh-Ahmad, T.; Salamone, A.; Ravizza, T.; Rizzi, M.; Pastore, A.; Pascente, R.; Liang, L.-P.; Villa, B.R.; et al. Targeting Oxidative Stress Improves Disease Outcomes in a Rat Model of Acquired Epilepsy. Brain 2019, 142, e39. [Google Scholar] [CrossRef] [PubMed]
- Wan, F.J.; Tung, C.S.; Shiah, I.S.; Lin, H.C. Effects of Alpha-phenyl-N-tert-butyl Nitrone and N-Acetylcysteine on Hydroxyl Radical Formation and Dopamine Depletion in the Rat Striatum Produced by d-Amphetamine. Eur. Neuropsychopharmacol. 2006, 16, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Bloch, M.H.; Panza, K.E.; Yaffa, A.; Alvarenga, P.G.; Jakubovski, E.; Mulqueen, J.M.; Landeros-Weisenberger, A.; Leckman, J.F. N-Acetylcysteine in the Treatment of Pediatric Tourette Syndrome: Randomized, Double-Blind, Placebo-Controlled Add-On Trial. J. Child Adolesc. Psychopharmacol. 2016, 26, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Rus, C.P. [A Girl with Self-Harm Treated with N-Acetylcysteine (NAC)]. Tijdschr. Psychiatr. 2017, 59, 181–184. [Google Scholar]
- Yan, Y. [Effect of N-Acetylcysteine on Cognitive Function and Nuclear Factor Erythroid 2 Related Factor 2/Heme Oxygenase-1 Pathway in Mouse Models of Postoperative Cognitive Dysfunction]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2019, 41, 529–535. [Google Scholar]
- Milte, C.M.; Parletta, N.; Buckley, J.D.; Coates, A.M.; Young, R.M.; Howe, P.R. Eicosapentaenoic and Docosahexaenoic Acids, Cognition, and Behavior in Children with Attention-Deficit/Hyperactivity Disorder: A Randomized Controlled Trial. Nutrition 2012, 28, 670–677. [Google Scholar] [CrossRef]
- Stevens, L.; Zhang, W.; Peck, L.; Kuczek, T.; Grevstad, N.; Mahon, A.; Zentall, S.S.; Arnold, L.E.; Burgess, J.R. EFA Supplementation in Children with Inattention, Hyperactivity, and Other Disruptive Behaviors. Lipids 2003, 38, 1007–1021. [Google Scholar] [CrossRef]
- Matsudaira, T.; Gow, R.V.; Kelly, J.; Murphy, C.; Potts, L.; Sumich, A.; Ghebremeskel, K.; Crawford, M.A.; Taylor, E. Biochemical and Psychological Effects of Omega-3/6 Supplements in Male Adolescents with Attention-Deficit/Hyperactivity Disorder: A Randomized, Placebo-Controlled, Clinical Trial. J. Child Adolesc. Psychopharmacol. 2015, 25, 775–782. [Google Scholar] [CrossRef] [Green Version]
- Joshi, K.; Lad, S.; Kale, M.; Patwardhan, B.; Mahadik, S.P.; Patni, B.; Chaudhary, A.; Bhave, S.; Pandit, A. Supplementation with Flax Oil and Vitamin C Improves the Outcome of Attention Deficit Hyperactivity Disorder (ADHD). Prostaglandins Leukot. Essent. Fat. Acids 2006, 74, 17–21. [Google Scholar] [CrossRef]
- Sorgi, P.J.; Hallowell, E.M.; Hutchins, H.L.; Sears, B. Effects of an Open-Label Pilot Study with High-Dose EPA/DHA Concentrates on Plasma Phospholipids and Behavior in Children with Attention Deficit Hyperactivity Disorder. Nutr. J. 2007, 6, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widenhorn-Muller, K.; Schwanda, S.; Scholz, E.; Spitzer, M.; Bode, H. Effect of Supplementation with Long-Chain Omega-3 Polyunsaturated Fatty Acids on Behavior and Cognition in Children with Attention Deficit/Hyperactivity Disorder (ADHD): A Randomized Placebo-Controlled Intervention Trial. Prostaglandins Leukot. Essent. Fat. Acids 2014, 91, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Bos, D.J.; Oranje, B.; Veerhoek, E.S.; Van Diepen, R.M.; Weusten, J.M.; Demmelmair, H.; Koletzko, B.; Velden, M.G.D.S.-V.D.; Eilander, A.; Hoeksma, M.; et al. Reduced Symptoms of Inattention after Dietary Omega-3 Fatty Acid Supplementation in Boys with and without Attention Deficit/Hyperactivity Disorder. Neuropsychopharmacology 2015, 40, 2298–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zgórzyńska, E.; Dziedzic, B.; Gorzkiewicz, A.; Stulczewski, D.; Bielawska, K.; Su, K.-P.; Walczewska, A. Omega-3 Polyunsaturated Fatty Acids Improve the Antioxidative Defense in Rat Astrocytes via an Nrf2-Dependent Mechanism. Pharmacol. Rep. 2017, 69, 935–942. [Google Scholar] [CrossRef]
- Šalamon, Š.; Kramar, B.; Marolt, T.P.; Poljšak, B.; Milisav, I. Medical and Dietary Uses of N-Acetylcysteine. Antioxidants 2019, 8, 111. [Google Scholar] [CrossRef] [Green Version]
- Ooi, S.L.; Green, R.; Pak, S.C. N-Acetylcysteine for the Treatment of Psychiatric Disorders: A Review of Current Evidence. BioMed Res. Int. 2018, 2018, 2469486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slattery, J.; Kumar, N.; Delhey, L.; Berk, M.; Dean, O.; Spielholz, C.; Frye, R. Clinical trials of N-acetylcysteine in psychiatry and neurology: A systematic review. Neurosci. Biobehav. Rev. 2015, 55, 294–321. [Google Scholar]
- Duailibi, M.S.; Cordeiro, Q.; Brietzke, E.; Ribeiro, M.; LaRowe, S.; Berk, M.; Trevizol, A.P. N-acetylcysteine in the treatment of craving in substance use disorders: Systematic review and meta-analysis. Am. J. Addict. 2017, 26, 660–666. [Google Scholar] [CrossRef]
- Chen, A.T.; Chibnall, J.T.; A Nasrallah, H. Placebo-Controlled Augmentation Trials of the Antioxidant NAC in Schizophrenia: A Review. Ann. Clin. Psychiatry 2016, 28, 190–196. [Google Scholar]
- Zheng, W.; Qiu, Y.; Berk, M.; Zhang, Q.-E.; Cai, D.-B.; Yang, X.-H.; Ungvari, G.S.; Ng, C.H.; Ning, Y.-P.; Xiang, Y.-T. N-acetylcysteine for Major Mental Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Acta Psychiatr. Scand. 2018, 137, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Oliver, G.; Dean, O.; Camfield, D.; Blair-West, S.; Ng, C.; Berk, M.; Sarris, J. N-Acetyl Cysteine in the Treatment of Obsessive Compulsive and Related Disorders: A Systematic Review. Clin. Psychopharmacol. Neurosci. 2015, 13, 12–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikoo, M.; Radnia, H.; Farokhnia, M.; Mohammadi, M.R.; Akhondzadeh, S. N-acetylcysteine as an Adjunctive Therapy to Risperidone for Treatment of Irritability in Autism: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of Efficacy and Safety. Clin. Neuropharmacol. 2015, 38, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Keller, C.; Smiley, C.; Monforton, C.; Melton, S.; Kalivas, P.W.; Gass, J. N-Acetylcysteine Treatment during Acute Stress Prevents Stress-Induced Augmentation of Addictive Drug Use and Relapse. Addict. Boil. 2019, e12798. [Google Scholar] [CrossRef]
- Healy-Stoffel, M.; Levant, B. N-3 (Omega-3) Fatty Acids: Effects on Brain Dopamine Systems and Potential Role in the Etiology and Treatment of Neuropsychiatric Disorders. CNS Neurol. Disord. Drug Targets 2018, 17, 216–232. [Google Scholar] [CrossRef]
- Avallone, R.; Vitale, G.; Bertolotti, M. Omega-3 Fatty Acids and Neurodegenerative Diseases: New Evidence in Clinical Trials. Int. J. Mol. Sci. 2019, 20, 4256. [Google Scholar] [CrossRef] [Green Version]
- Nasir, M.; Bloch, M.H. Trim the Fat: The Role of Omega-3 Fatty Acids in Psychopharmacology. Ther. Adv. Psychopharmacol. 2019, 9, 2045125319869791. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 Fatty Acids and Inflammatory Processes: From Molecules to Man. Biochem. Soc. Trans. 2017, 45, 1105–1115. [Google Scholar] [CrossRef] [Green Version]
- Endres, S.; Ghorbani, R.; Kelley, V.E.; Georgilis, K.; Lonnemann, G.; Van Der Meer, J.W.M.; Cannon, J.G.; Rogers, T.S.; Klempner, M.S.; Weber, P.C.; et al. The Effect of Dietary Supplementation with n-3 Polyunsaturated Fatty Acids on the Synthesis of Interleukin-1 and Tumor Necrosis Factor by Mononuclear Cells. N. Engl. J. Med. 1989, 320, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Zhao, L.; Youn, H.S.; Weatherill, A.R.; Tapping, R.; Feng, L.; Lee, W.H.; Fitzgerald, K.A.; Hwang, D.H. Saturated Fatty Acid Activates but Polyunsaturated Fatty Acid Inhibits Toll-Like Receptor 2 Dimerized with Toll-like Receptor 6 or 1. J. Boil. Chem. 2004, 279, 16971–16979. [Google Scholar] [CrossRef] [Green Version]
- Mohammadzadeh, S.; Baghi, N.; Yousefi, F.; Yousefzamani, B. Effect of Omega-3 plus Methylphenidate as an Alternative Therapy to Reduce Attention Deficit-Hyperactivity Disorder in Children. Korean J. Pediatr. 2019, 62, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Öztop, D.; Altun, H.; Baskol, G.; Ozsoy, S. Oxidative Stress in Children with Attention Deficit Hyperactivity Disorder. Clin. Biochem. 2012, 45, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Spahis, S.; Vanasse, M.; Bélanger, S.A.; Ghadirian, P.; Grenier, E.; Levy, E. Lipid Profile, Fatty Acid Composition and Pro- and Anti-Oxidant Status in Pediatric Patients with Attention-Deficit/Hyperactivity Disorder. Prostaglandins Leukot. Essent. Fat. Acids 2008, 79, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Naeini, A.A.; Nasim, S.; Najafi, M.; Ghazvini, M.; Hassanzadeh, A. Relationship between Antioxidant Status and Attention Deficit Hyperactivity Disorder among Children. Int. J. Prev. Med. 2019, 10, 41. [Google Scholar] [CrossRef] [PubMed]
- Bulut, M.; Selek, S.; Gergerlioglu, H.S.; Savas, H.A.; Yilmaz, H.R.; Yuce, M.; Ekici, G. Malondialdehyde Levels in Adult Attention-Deficit Hyperactivity Disorder. J. Psychiatry Neurosci. 2007, 32, 435–438. [Google Scholar]
- Bulut, M.; Selek, S.; Bez, Y.; Kaya, M.C.; Günes, M.; Karababa, F.; Çelik, H.; Savaş, H.A. Lipid Peroxidation Markers in Adult Attention Deficit Hyperactivity Disorder: New Findings for Oxidative Stress. Psychiatry Res. Neuroimaging 2013, 209, 638–642. [Google Scholar] [CrossRef]
- Ceylan, M.; Sener, S.; Bayraktar, A.C.; Kavutcu, M.; Bayraktar, A.C. Oxidative Imbalance in Child and Adolescent Patients with Attention-Deficit/Hyperactivity Disorder. Prog. Neuro-Psychopharmacol. Boil. Psychiatry 2010, 34, 1491–1494. [Google Scholar] [CrossRef]
- Verlaet, A.A.J.; Breynaert, A.; Ceulemans, B.; De Bruyne, T.; Fransen, E.; Pieters, L.; Savelkoul, H.F.J.; Hermans, N. Oxidative Stress and Immune Aberrancies in Attention-Deficit/Hyperactivity Disorder (ADHD): A Case-Control Comparison. Eur. Child Adolesc. Psychiatry 2019, 28, 719–729. [Google Scholar] [CrossRef]
- Dvorakova, M.; Sivoňová, M.; Trebatická, J.; Škodáček, I.; Waczulikova, I.; Muchová, J.; Ďuračková, Z. The Effect of Polyphenolic Extract from Pine Bark, Pycnogenol® on the Level of Glutathione in Children Suffering from Attention Deficit Hyperactivity Disorder (ADHD). Redox Rep. 2006, 11, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Leffa, D.T.; Bellaver, B.; De Oliveira, C.; De Macedo, I.C.; De Freitas, J.S.; Grevet, E.H.; Caumo, W.; Rohde, L.A.; Quincozes-Santos, A.; Torres, I.L.S. Increased Oxidative Parameters and Decreased Cytokine Levels in an Animal Model of Attention-Deficit/Hyperactivity Disorder. Neurochem. Res. 2017, 42, 3084–3092. [Google Scholar] [CrossRef]
- Sezen, H.; Kandemir, H.; Savik, E.; Kandemir, S.B.; Kilicaslan, F.; Bilinc, H.; Aksoy, N. Increased Oxidative Stress in Children with Attention Deficit Hyperactivity Disorder. Redox Rep. 2016, 21, 248–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avcil, S.; Uysal, P.; Yenisey, Ç.; Abas, B.I. Elevated Melatonin Levels in Children with Attention Deficit Hyperactivity Disorder: Relationship to Oxidative and Nitrosative Stress. J. Atten. Disord. 2019, 1087054719829816. [Google Scholar] [CrossRef] [PubMed]
- Selek, S.; Savaş, H.A.; Gergerlioglu, H.S.; Bulut, M.; Yilmaz, H.R.; Yılmaz, H.R. Oxidative Imbalance in Adult Attention deficit/hyperactivity disorder. Boil. Psychol. 2008, 79, 256–259. [Google Scholar] [CrossRef]
- Ceylan, M.F.; Sener, S.; Bayraktar, A.C.; Kavutcu, M. Changes in Oxidative Stress and Cellular Immunity Serum Markers in Attention-Deficit/Hyperactivity Disorder. Psychiatry Clin. Neurosci. 2012, 66, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S.; Kopin, I.J.; Sharabi, Y. Catecholamine autotoxicity. Implications for Pharmacology and Therapeutics of Parkinson Disease and Related Disorders. Pharmacol. Ther. 2014, 144, 268–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napolitano, A.; Manini, P.; D’Ischia, M. Oxidation Chemistry of Catecholamines and Neuronal Degeneration: An Update. Curr. Med. Chem. 2011, 18, 1832–1845. [Google Scholar] [CrossRef] [Green Version]
- Neri, M.; Cerretani, D.; Fiaschi, A.I.; Laghi, P.F.; Lazzerini, P.E.; Maffione, A.B.; Micheli, L.; Bruni, G.; Nencini, C.; Giorgi, G.; et al. Correlation between Cardiac Oxidative Stress and Myocardial Pathology due to Acute and Chronic Norepinephrine Administration in Rats. J. Cell. Mol. Med. 2007, 11, 156–170. [Google Scholar] [CrossRef]
- Spencer, W.A.; Jeyabalan, J.; Kichambre, S.; Gupta, R.C. Oxidatively Generated DNA Damage after Cu(II) Catalysis of Dopamine and Related Catecholamine Neurotransmitters and Neurotoxins: Role of Reactive Oxygen Species. Free Radic. Biol. Med. 2011, 50, 139–147. [Google Scholar] [CrossRef] [Green Version]
- Swanson, C.J.; Perry, K.W.; Koch-Krueger, S.; Katner, J.; Svensson, K.A.; Bymaster, F.P. Effect of the Attention Deficit/Hyperactivity Disorder Drug Atomoxetine on Extracellular Concentrations of Norepinephrine and Dopamine in Several Brain Regions of the Rat. Neuropharmacology. 2006, 50, 755–760. [Google Scholar] [CrossRef]
- Corona, J.C.; Carreón-Trujillo, S.; González-Pérez, R.; Gómez-Bautista, D.; Vázquez-González, D.; Salazar-García, M. Atomoxetine Produces Oxidative Stress and Alters Mitochondrial Function in Human Neuron-Like Cells. Sci. Rep. 2019, 9, 13011–13019. [Google Scholar] [CrossRef]
- Cobley, J.N.; Fiorello, M.L.; Bailey, D.M. 13 Reasons Why the Brain is Susceptible to Oxidative Stress. Redox Boil. 2018, 15, 490–503. [Google Scholar] [CrossRef] [PubMed]
- Corona, J.C.; Duchen, M.R. Impaired Mitochondrial Homeostasis and Neurodegeneration: Towards New Therapeutic Targets? J. Bioenerg. Biomembr. 2015, 47, 89–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreazza, A.C.; Frey, B.N.; Valvassori, S.S.; Zanotto, C.; Gomes, K.M.; Comim, C.M.; Cassini, C.; Stertz, L.; Ribeiro, L.C.; Quevedo, J.; et al. DNA Damage in Rats after Treatment with Methylphenidate. Prog. Neuro-Psychopharmacol. Boil. Psychiatry 2007, 31, 1282–1288. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.R.; Reinke, A.; Petronilho, F.C.; Gomes, K.M.; Dal-Pizzol, F.; Quevedo, J. Methylphenidate Treatment Induces Oxidative Stress in Young Rat Brain. Brain Res. 2006, 1078, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Gomes, K.M.; Petronilho, F.C.; Mantovani, M.; Garbelotto, T.; Boeck, C.R.; Dal-Pizzol, F.; Quevedo, J. Antioxidant Enzyme Activities Following Acute or Chronic Methylphenidate Treatment in Young Rats. Neurochem. Res. 2008, 33, 1024–1027. [Google Scholar] [CrossRef] [PubMed]
- Comim, C.M.; Gomes, K.M.; Reus, G.Z.; Petronilho, F.; Ferreira, G.K.; Streck, E.L.; Dal-Pizzol, F.; Quevedo, J. Methylphenidate Treatment Causes Oxidative Stress and Alters Energetic Metabolism in an Animal Model of Attention-Deficit Hyperactivity Disorder. Acta Neuropsychiatr. 2014, 26, 96–103. [Google Scholar] [CrossRef]
- Motaghinejad, M.; Motevalian, M.; Shabab, B.; Fatima, S. Effects of Acute Doses of Methylphenidate on Inflammation and Oxidative Stress in Isolated Hippocampus and Cerebral Cortex of Adult Rats. J. Neural Transm. 2017, 124, 121–131. [Google Scholar] [CrossRef]
- Smith, R.E.; Ozben, T.; Saso, L. Modulation of Oxidative Stress: Pharmaceutical and Pharmacological Aspects 2018. Oxidative Med. Cell. Longev. 2019, 2019, 6380473. [Google Scholar] [CrossRef]
- Sun, Y.; Yang, T.; Leak, R.K.; Chen, J.; Zhang, F. Preventive and Protective Roles of Dietary Nrf2 Activators against Central Nervous System Diseases. CNS Neurol. Disord. Drug Targets 2017, 16, 326–338. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wu, J.; Chen, D.; Jin, J.; Wu, Y.; Chen, Z. Effects of Sulforaphane in the Central Nervous System. Eur. J. Pharmacol. 2019, 853, 153–168. [Google Scholar] [CrossRef]
- Shahripour, R.B.; Harrigan, M.R.; Alexandrov, A.V. N-Acetylcysteine (NAC) in Neurological Disorders: Mechanisms of Action and Therapeutic Opportunities. Brain Behav. 2014, 4, 108–122. [Google Scholar] [CrossRef] [PubMed]
- Heshmati, J.; Morvaridzadeh, M.; Maroufizadeh, S.; Akbari, A.; Yavari, M.; Amirinejad, A.; Maleki-Hajiagha, A.; Sepidarkish, M.; Amirinejhad, A. Omega-3 Fatty Acids Supplementation and Oxidative Stress Parameters: A Systematic Review and Meta-Analysis of Clinical Trials. Pharmacol. Res. 2019, 149, 104462. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Against Inflammation | Type of Study | Outcome |
| SFN | Mouse model of atopic dermatitis [61] | Reduced inflammation, suppressed JAK1/STAT3 signaling and activated Nrf2/HO-1 pathway |
| SFN | Microglial cells [62] | Reduced inflammatory mediators (iNOS, COX-2, NO, and PGE2) and proinflammatory cytokines (TNF-α, IL-6, and IL-1β), increased anti-inflammatory cytokines (IL-10 and IL-4) and increased the expression of Nrf2 and HO-1. |
| SFN | Mouse model of acute lung injury and Macrophages [63,65] | Decreased lactate dehydrogenase, IL-6, TNF-α, NF-kB, PGE2 production, COX-2, MMP-9 and iNOS protein expression |
| SFN | Mouse model of peritonitis [66] | Inhibited inflammasome activation and IL-1β secretion and inhibited cell recruitment to peritoneum. |
| SFN | Mouse macrophages [67] | Blocked activation of NLRP3 and NLRC4 inflammasomes and IL-1β secretion |
| SFN | Rat [69] | Inhibited NF-kB activity and TNF-α secretion and prevent decreased IL-10 |
| SFN | Mouse model of autism and Autism patients [27,70] | Reduced Th17 response and expression of NF-kB and iNOS Randomized double-blind study; decreased symptoms |
| NAC | Mild-stress rat model [71] | Inhibited pro-inflammatory cytokines (IL-1β, IL-6 and TNF-α) |
| NAC | Bipolar depression patients [72] | Randomized placebo-controlled trial; no effects on the biological parameters evaluated |
| NAC | Systemic lupus erythematosus patients [73,74] | Randomized double-blind placebo-controlled trial and randomized controlled trial; reduced the ADHD symptoms and also inhibited the autoimmune inflammatory process by suppression of the mammalian target of rapamycin (mTOR) and increased regulatory T cells |
| NAC | Human retinal pigment epithelial cell line [75] | Decreased IL-18, IL-1β mRNA, ROS and blocked inflammasome activation |
| NAC | Rat [76] | Improved brain oxidant/antioxidant status and reversed the overproduction of pro-inflammatory cytokines in brain and serum |
| Omega-3 FAs | Macrophage and mouse dendritic cell lines [77,78] | Inhibited dimerization and recruitment of TLR2 and TLR4 recruitment to lipid rafts and reduced T-cell proliferation and increased the proportion of T cells expressing FoxP3 |
| Omega-3 FAs | Mouse [79,80] | Regulated CD4+ T-cell function and reduced Th17cell polarazation |
| Omega-3 FAs | Children with ADHD [81] | Double-blind study; decreased plasma inflammatory mediators |
| Against Oxidative Stress | Type of Study | Outcome |
| SFN | Mouse [82] | Increased dopamine, DOPAC and dopamine transporter immunoreactivity in the striatum |
| SFN | Rat [69] | Activation of HO-1, glutamate-cysteine ligase catalytic subunit and Nrf2 and protected against memory impairment |
| SFN | Mouse model of autism [70] | Improved the autism-like symptoms and upregulated SOD, glutathione reductase and GPx |
| SFN and NAC | Rat with epilepsy [83] | Reduced oxidative stress, delayed the onset of epilepsy, blocked disease progression and reduced the frequency of spontaneous seizures |
| SFN | Healthy subjects [26] | Clinical pilot study; increased GSH |
| NAC | Rats [84] | Protected against amphetamine-induced damage |
| NAC | Paediatric Tourette’s syndrome [85] | Randomized double-blind placebo-controlled trial; did not show a significant difference with placebo |
| NAC | A girl with ADHD [86] | A case-study; reduced the frequency of self-cutting and reduced the symptoms and depression |
| NAC | Mouse model of postoperative cognitive dysfunction [87] | Reduced oxidative stress and inflammation in the hippocampus and improved cognitive function by activation of the Nrf2/HO-1 pathway |
| Omega-3 FAs | Children with ADHD [81] | Double-blind study; decreased oxidative stress |
| Omega-3 FAs | Children with ADHD [88] | Randomized controlled trial; no significant differences among the treatments. One subgroup improved spelling, reading and attention and decreased hyperactivity |
| Omega-3 FAs | Children with ADHD [89,90] | Randomized pilot study and placebo-controlled trial; no significant improvement |
| Omega-3 FAs | Children with ADHD [91,92,93,94] | Pilot studies and randomized placebo-controlled trials; improved working memory function and improved symptoms and behaviour |
| Omega-3 FAs | Rat astrocytes [95] | Increased glutamate-cysteine ligase, Nrf2, glutathione synthetase and glutathione peroxidase-4 proteins |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarez-Arellano, L.; González-García, N.; Salazar-García, M.; Corona, J.C. Antioxidants as a Potential Target against Inflammation and Oxidative Stress in Attention-Deficit/Hyperactivity Disorder. Antioxidants 2020, 9, 176. https://doi.org/10.3390/antiox9020176
Alvarez-Arellano L, González-García N, Salazar-García M, Corona JC. Antioxidants as a Potential Target against Inflammation and Oxidative Stress in Attention-Deficit/Hyperactivity Disorder. Antioxidants. 2020; 9(2):176. https://doi.org/10.3390/antiox9020176
Chicago/Turabian StyleAlvarez-Arellano, Lourdes, Nadia González-García, Marcela Salazar-García, and Juan Carlos Corona. 2020. "Antioxidants as a Potential Target against Inflammation and Oxidative Stress in Attention-Deficit/Hyperactivity Disorder" Antioxidants 9, no. 2: 176. https://doi.org/10.3390/antiox9020176