
Effect of Alpha Lipoic Acid Supplementation on Oxidative Stress and Lipid Parameters in Women Diagnosed with Low-Grade Squamous Intraepithelial Lesions (LSILs): A Double-Blind, Randomized, Placebo-Controlled Trial
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Assessment of Biochemical Parameters
2.3. Assessment of Oxidative Status Parameters
2.3.1. Assessment of Total Antioxidant Capacity of Serum
2.3.2. Assessment of the Activity of the Endogenous Antioxidant System
2.3.3. Assessment of Lipid Peroxidation
2.4. Analysis of Dietary Characteristics and Calculation of Diet Quality Indexes
2.5. Statistical Analysis
3. Results
3.1. The Baseline Characteristics of the Participants
3.2. Impact of ALA Supplementation on Oxidative and Lipid Status Parameters
4. Discussion
4.1. Dietary Characteristics of Participants
4.2. Impact of ALA Supplementation on Oxidative Status Parameters
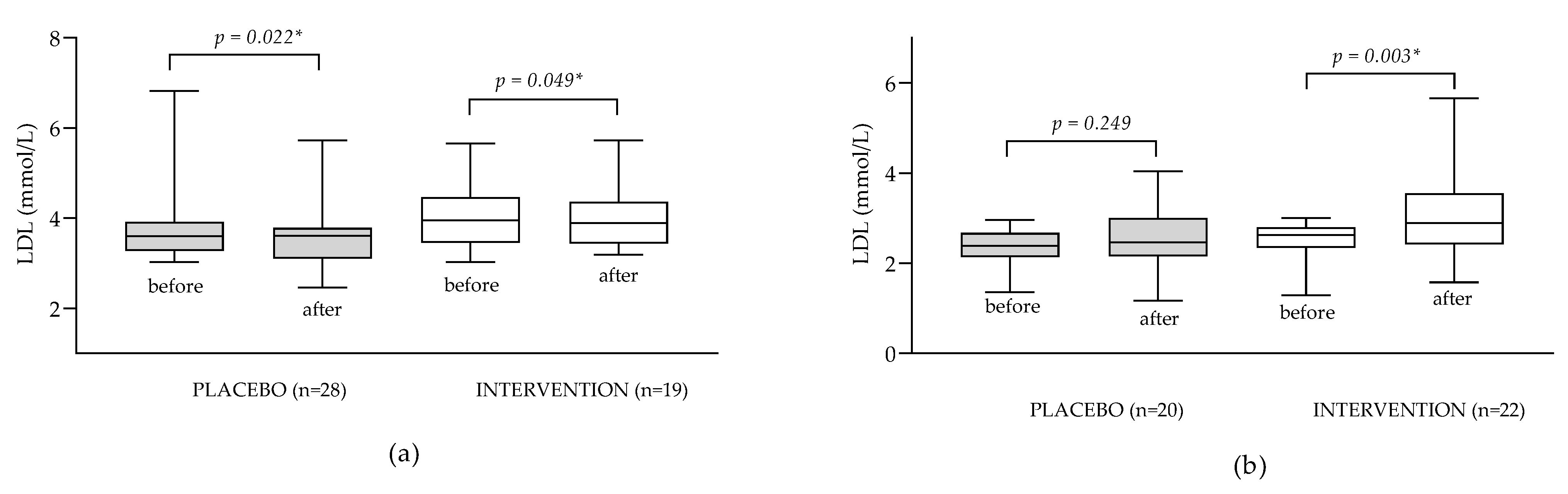
4.3. Impact of ALA Supplementation on Lipid Parameters
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shay, K.P.; Moreau, R.F.; Smith, E.J.; Smith, A.R.; Hagen, T.M. Alpha-lipoic acid as a dietary supplement: Molecular mechanisms and therapeutic potential. Biochim. Biophys. Acta BBA-Gen. Subj. 2009, 1790, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Fu, J.; Zhao, Y.; Ji, K.; Luan, T.; Zang, B. Alpha-Lipoic Acid Exerts Anti-Inflammatory Effects on Lipopolysaccharide-Stimulated Rat Mesangial Cells via Inhibition of Nuclear Factor Kappa B (NF-κB) Signaling Pathway. Inflammation 2014, 38, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Han, P.; Wu, N.; He, B.; Lu, Y.; Li, S.; Liu, Y.; Zhao, S.; Liu, L.; Li, Y. Amelioration of Lipid Abnormalities by α-Lipoic acid Through Antioxidative and Anti-Inflammatory Effects. Obesity 2011, 19, 1647–1653. [Google Scholar] [CrossRef] [PubMed]
- Theodosis-Nobelos, P.; Papagiouvannis, G.; Tziona, P.; Rekka, E.A. Lipoic acid. Kinetics and pluripotent biological properties and derivatives. Mol. Biol. Rep. 2021, 48, 6539–6550. [Google Scholar] [CrossRef] [PubMed]
- Abubaker, S.A.; Alonazy, A.M.; Abdulrahman, A. Effect of Alpha-Lipoic Acid in the Treatment of Diabetic Neuropathy: A Systematic Review. Cureus 2022, 14, e25750. [Google Scholar] [CrossRef] [PubMed]
- Haghighatdoost, F.; Hariri, M. Does alpha-lipoic acid affect lipid profile? A meta-analysis and systematic review on randomized controlled trials. Eur. J. Pharmacol. 2019, 847, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Namazi, N.; Larijani, B.; Azadbakht, L. Alpha-lipoic acid supplement in obesity treatment: A systematic review and meta-analysis of clinical trials. Clin. Nutr. 2017, 37, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Šabanović, M.; Jašić, M.; Odobašić, A.; Aleksovska, E.S.; Pavljašević, S.; Bajraktarević, A.; Čepo, D.V. Alpha Lipoic Acid Reduces Symptoms and Inflammation Biomarkers in Patients with Chronic Hemorrhoidal Illness. Int. J. Vitam. Nutr. Res. 2018, 88, 281–290. [Google Scholar] [CrossRef]
- Hager, K.; Kenklies, M.; McAfoose, J.; Engel, J.; Münch, G. α-Lipoic Acid as a New Treatment Option for Alzheimer’s Disease—A 48 Months Follow-Up Analysis; Springer: Vienna, Austria, 2007; pp. 189–193. [Google Scholar] [CrossRef]
- Dong, L.; Yang, F.; Li, J.; Li, Y.; Yu, X.; Zhang, X. Effect of oral alpha-lipoic acid (ALA) on sperm parameters: A systematic review and meta-analysis. Basic Clin. Androl. 2022, 32, 23. [Google Scholar] [CrossRef]
- Divković, A.; Radić, K.; Sabitović, D.; Golub, N.; Rajković, M.G.; Samarin, I.R.; Karasalihović, Z.; Šerak, A.; Trnačević, E.; Turčić, P.; et al. Effect of Alpha-Lipoic Acid Supplementation on Low-Grade Squamous Intraepithelial Lesions—Double-Blind, Randomized, Placebo-Controlled Trial. Healthcare 2022, 10, 2434. [Google Scholar] [CrossRef]
- Halliwell, B. The antioxidant paradox: Less paradoxical now? Br. J. Clin. Pharmacol. 2012, 75, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Rabić, D.; Sindik, J.; Missoni, S. Development and validation of a self-administered food frequency questionnaire to assess habitual dietary intake and quality of diet in healthy adults in the Republic of Croatia. Coll. Antropol. 2014, 38, 1017–1026. [Google Scholar] [PubMed]
- Ou, B.; Chang, T.; Huang, D.; Prior, R.L. Determination of Total Antioxidant Capacity by Oxygen Radical Absorbance Capacity (ORAC) Using Fluorescein as the Fluorescence Probe: First Action 2012.23. J. AOAC Intern. 2013, 96, 1372–1376. [Google Scholar] [CrossRef] [PubMed]
- Re, R.; Pellegrini, N.; Proteggente, A.; Pannala, A.; Yang, M.; Rice-Evans, C. Antioxidant activity applying an improved ABTS radical cation decolorization assay. Free Radic. Biol. Med. 1999, 26, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, E.A.; Gillespie, K.M. Estimation of total phenolic content and other oxidation substrates in plant tissues using Folin–Ciocalteu reagent. Nat. Protoc. 2007, 2, 875–877. [Google Scholar] [CrossRef] [PubMed]
- Benzie, I.F.F.; Strain, J.J. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: The FRAP assay. Anal. Biochem. 1996, 239, 70–76. Available online: http://linkinghub.elsevier.com/retrieve/pii/S0003269796902924 (accessed on 24 July 2023). [CrossRef] [PubMed]
- Machado, M.D.; Soares, E.V. Assessment of cellular reduced glutathione content in Pseudokirchneriella subcapitata using monochlorobimane. J. Appl. Phycol. 2012, 24, 1509–1516. [Google Scholar] [CrossRef]
- Drury, J.A.; Nycyk, J.A.; Cooke, R.W. Comparison of urinary and plasma malondialdehyde in preterm infants. Clin. Chim. Acta 1997, 263, 177–185. [Google Scholar] [CrossRef]
- Al-Shaar, L.; Yuan, C.; Rosner, B.; Dean, S.B.; Ivey, K.L.; Clowry, C.M.; A Sampson, L.; Barnett, J.B.; Rood, J.; Harnack, L.J.; et al. Reproducibility and Validity of a Semiquantitative Food Frequency Questionnaire in Men Assessed by Multiple Methods. Am. J. Epidemiol. 2020, 190, 1122–1132. [Google Scholar] [CrossRef]
- Kaić-Rak, A.; Antonić, K. Tablice o Sastavu Namirnica i Pica; Zavod Za Zaštitu Zdravlja SR Hrvatske: Zagreb, Croatia, 1990. [Google Scholar]
- Dietary Guidelines for Americans, 9th ed; U.S. Department of Agriculture and U.S. Department of Health and Human Services: Washington, DC, USA, 2020; pp. 2020–2025.
- Kim, S.; Haines, P.S.; Siega-Riz, A.M.; Popkin, B.M. The Diet Quality Index-International (DQI-I) Provides an Effective Tool for Cross-National Comparison of Diet Quality as Illustrated by China and the United States. J. Nutr. 2003, 133, 3476–3484. [Google Scholar] [CrossRef]
- Gerber, M. Qualitative methods to evaluate Mediterranean diet in adults. Public Health Nutr. 2006, 9, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Baldini, M.; Pasqui, F.; Bordoni, A.; Maranesi, M. Is the Mediterranean lifestyle still a reality? Evaluation of food consumption and energy expenditure in Italian and Spanish university students. Public Health Nutr. 2009, 12, 148–155. [Google Scholar] [CrossRef] [PubMed]
- DeRosa, G.; D’Angelo, A.; Romano, D.; Maffioli, P. A Clinical Trial about a Food Supplement Containing α-Lipoic Acid on Oxidative Stress Markers in Type 2 Diabetic Patients. Int. J. Mol. Sci. 2016, 17, 1802. [Google Scholar] [CrossRef]
- Huang, E.A.; Gitelman, S.E. The effect of oral alpha-lipoic acid on oxidative stress in adolescents with type 1 diabetes mellitus. Pediatr. Diabetes 2008, 9, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Khalili, M.; Eghtesadi, S.; Mirshafiey, A.; Eskandari, G.; Sanoobar, M.; Sahraian, M.A.; Motevalian, A.; Norouzi, A.; Moftakhar, S.; Azimi, A. Effect of lipoic acid consumption on oxidative stress among multiple sclerosis patients: A randomized controlled clinical trial. Nutr. Neurosci. 2013, 17, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Amirkhizi, F.; Hamedi-Shahraki, S.; Hosseinpour-Arjmand, S.; Vaghef-Mehrabany, E.; Ebrahimi-Mameghani, M. Effects of Alpha-Lipoic Acid Supplementation on Oxidative Stress Status in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double Blind, Placebo-Controlled Clinical Trial. Iran. Red Crescent Med. J. 2018, 20, 11. [Google Scholar] [CrossRef]
- Ahmadi, A.; Mazooji, N.; Roozbeh, J.; Mazloom, Z.; Hassanzadeh, J. Effect of alpha-lipoic acid and vitamin E supplementation on oxidative stress, inflammation, and malnutrition in hemodialysis patients. Iran. J. Kidney Dis. 2013, 7, 461. [Google Scholar]
- Khabbazi, T.; Mahdavi, R.; Safa, J.; Pour-Abdollahi, P. Effects of Alpha-Lipoic Acid Supplementation on Inflammation, Oxidative Stress, and Serum Lipid Profile Levels in Patients with End-Stage Renal Disease on Hemodialysis. J. Ren. Nutr. 2012, 22, 244–250. [Google Scholar] [CrossRef]
- Draeger, C.L.; Naves, A.; Marques, N.; Baptistella, A.B.; Carnauba, R.A.; Paschoal, V.; Nicastro, H. Controversies of antioxidant vitamins supplementation in exercise: Ergogenic or ergolytic effects in humans? J. Int. Soc. Sports Nutr. 2014, 11, 4. [Google Scholar] [CrossRef]
- Bettermann, E.L.; Hartman, T.J.; A Easley, K.; Ferranti, E.P.; Jones, D.P.; A Quyyumi, A.; Vaccarino, V.; Ziegler, T.R.; A Alvarez, J. Higher Mediterranean Diet Quality Scores and Lower Body Mass Index Are Associated with a Less-Oxidized Plasma Glutathione and Cysteine Redox Status in Adults. J. Nutr. 2018, 148, 245–253. [Google Scholar] [CrossRef]
- Kim, J.Y.; Yang, Y.J.; Yang, Y.K.; Oh, S.-Y.; Hong, Y.-C.; Lee, E.-K.; Kwon, O. Diet quality scores and oxidative stress in Korean adults. Eur. J. Clin. Nutr. 2011, 65, 1271–1278. [Google Scholar] [CrossRef]
- Fung, T.T.; McCullough, M.L.; Newby, P.; E Manson, J.; Meigs, J.B.; Rifai, N.; Willett, W.C.; Hu, F.B. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2005, 82, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Bahadoran, Z.; Gaeini, Z. Common Limitations and Challenges of Dietary Clinical Trials for Translation into Clinical Practices. Int. J. Endocrinol. Metab. 2021, 19, e108170. [Google Scholar] [CrossRef] [PubMed]
- Boylan, S.; Welch, A.; Pikhart, H.; Malyutina, S.; Pajak, A.; Kubinova, R.; Bragina, O.; Simonova, G.; Stepaniak, U.; Gilis-Januszewska, A.; et al. Dietary habits in three Central and Eastern European countries: The HAPIEE study. BMC Public Health 2009, 9, 439. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.; Stuetz, W.; Toussaint, O.; Debacq-Chainiaux, F.; Dollé, M.E.T.; Jansen, E.; Gonos, E.S.; Franceschi, C.; Sikora, E.; Hervonen, A.; et al. Associations between Specific Redox Biomarkers and Age in a Large European Cohort: The MARK-AGE Project. Oxidative Med. Cell. Longev. 2017, 2017, 1401452. [Google Scholar] [CrossRef] [PubMed]
- Pinchuk, I.; Weber, D.; Kochlik, B.; Stuetz, W.; Toussaint, O.; Debacq-Chainiaux, F.; Dollé, M.E.; Jansen, E.H.; Gonos, E.S.; Sikora, E.; et al. Gender- and age-dependencies of oxidative stress, as detected based on the steady state concentrations of different biomarkers in the MARK-AGE study. Redox Biol. 2019, 24, 101204. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, A.H.; McKenzie, M.J.; Bloomer, R.J. Gender comparisons of exercise-induced oxidative stress: Influence of antioxidant supplementation. Appl. Physiol. Nutr. Metab. 2007, 32, 1124–1131. [Google Scholar] [CrossRef]
- Actis-Goretta, L.; Carrasquedo, F.; Fraga, C.G. The regular supplementation with an antioxidant mixture decreases oxidative stress in healthy humans. Gender effect. Clin. Chim. Acta 2004, 349, 97–103. [Google Scholar] [CrossRef]
- Fayez, A.M.; Zakaria, S.; Moustafa, D. Alpha lipoic acid exerts antioxidant effect via Nrf2/HO-1 pathway activation and suppresses hepatic stellate cells activation induced by methotrexate in rats. Biomed. Pharmacother. 2018, 105, 428–433. [Google Scholar] [CrossRef]
- Jibril, A.T.; Jayedi, A.; Shab-Bidar, S. Efficacy and safety of oral alpha-lipoic acid supplementation for type 2 diabetes management: A systematic review and dose–response meta-analysis of randomized trials. Endocr. Connect. 2022, 11, e220322. [Google Scholar] [CrossRef]
- Ordovas, J.M.; Shen, H. Pharmacogenetics of lipid-lowering therapies. Curr. Atheroscler. Rep. 2002, 4, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Cangemi, R.; Romiti, G.F.; Campolongo, G.; Ruscio, E.; Sciomer, S.; Gianfrilli, D.; Raparelli, V. Gender related differences in treatment and response to statins in primary and secondary cardiovascular prevention: The never-ending debate. Pharmacol. Res. 2017, 117, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zhao, L.; Liang, L.; Xie, G.; Wu, Y. Factors explaining the gender disparity in lipid-lowering treatment goal attainment rate in Chinese patients with statin therapy. Lipids Health Dis. 2012, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Marangon, K.; Devaraj, S.; Tirosh, O.; Packer, L.; Jialal, I. Comparison of the effect of α-lipoic acid and α-tocopherol supplementation on measures of oxidative stress. Free. Radic. Biol. Med. 1999, 27, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, T.; Liang, J.; Kitajima, S.; Koike, T.; Wang, X.; Sun, H.; Morimoto, M.; Shikama, H.; Watanabe, T.; Yamada, N.; et al. Macrophage-derived lipoprotein lipase increases aortic atherosclerosis in cholesterol-fed Tg rabbits. Atherosclerosis 2005, 179, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Matsugo, S.; Yan, L.J.; Konishi, T. An antioxidant inhibits protein oxidative modification of human low density lipoprotein and reduces plasma cholesterol levels by the inhibition of HMG-CoA reductas. BBRC 1997, 243, 819–824. [Google Scholar]
- Gosselin, L.E.; Chrapowitzky, L.; Rideout, T.C. Metabolic effects of α-lipoic acid supplementation in pre-diabetics: A randomized, placebo-controlled pilot study. Food Funct. 2019, 10, 5732–5738. [Google Scholar] [CrossRef]
- Iannuzzo, F.; Basile, G.A.; Campolo, D.; Genovese, G.; Pandolfo, G.; Giunta, L.; Ruggeri, D.; Di Benedetto, A.; Bruno, A. Metabolic and clinical effect of alpha-lipoic acid administration in schizophrenic subjects stabilized with atypical antipsychotics: A 12-week, open-label, uncontrolled study. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100116. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Placebo Group (n = 48) | Intervention Group (n = 41) | p | |
|---|---|---|---|
| Lifestyle characteristics | |||
| Age (years) | 37 (28–46) | 43 (34–47) | 0.082 |
| Cigarette smoking * (cigarettes per day) | 14 | 8 | 0.333 |
| Compliance * (returned tablets) | 35 | 28 | 0.405 |
| Diet characteristics ** | |||
| Energy (kcal) | 3104 (1937–4249) | 3530 (2015–4404) | 0.374 |
| Fruits (servings per week) | 2.78 (1.90–5.45) | 3.66 (1.56–5.88) | 0.365 |
| Vegetables (servings per week) | 3.49 (2.21–4.67) | 4.17 (2.83–5.86) | 0.252 |
| Animal protein (g/day) | 40.61 (24.33–62.90) | 36.05 (23.29–54.07) | 0.315 |
| Meat (servings per week) | 3.95 (2.25–7.37) | 4.20 (2.54–7.24) | 0.558 |
| Red meat (servings per week) | 2.66 (0.00–14.36) | 4.05 (0.00–33.76) | 0.852 |
| Fat (g) | 167.9 (99.7–252.5) | 190.6 (103.6–293.8) | 0.176 |
| Saturated fat (g) | 53.4 (29.6–85.5) | 69.75 (34.26–103.7) | 0.202 |
| Cholesterol (mg) | 290.4 (178.3–473.4) | 291.6 (188.8–422.4) | 0.809 |
| Vitamin C (mg) | 199.3 (139.0–302.4) | 175.7 (95.91–321.1) | 0.570 |
| Vitamin E (mg) | 21.44 (12.5–44.4) | 33.61 (17.17–48.06) | 0.262 |
| Carotenoids (mg) # | 7.58 (4.54–15.0) | 14.43 (6.363–18.65) | 0.064 |
| DQI-I *** | 63.55 (57.4–67.7) | 63.64 (55.00–68.79) | 0.308 |
| Med-DQI *** | 9.00 (7.25–10.0) | 9.00 (7.00–10.00) | 0.516 |
| Placebo (n = 48) | Intervention (n = 41) | p * | Placebo (n = 48) | Intervention (n = 41) | p ** | |
|---|---|---|---|---|---|---|
| initial measurement | 3-month follow-up measurement | |||||
| MDA (µmol L−1) | 0.566 (0.373–0.819) | 0.604 (0.444–1.011) | 0.151 | 0.546 (0.346–1.072) | 0.617 (0.462–1.13) | 0.472 |
| FRAP (µmol L−1 TE) | 395.5 (336.2–445.1) | 398.3 (360.9–449.1) | 0.381 | 403.9 (345.0–462.8) | 392.7 (374.6–428.8) | 0.768 |
| SOD (inhibition (%)) | 58.35 (51.64–64.16) | 59.21 (54.23–66.31) | 0.180 | 59.45 (52.15–63.89) | 59.43 (53.15–64.12) | 0.348 |
| ORAC (mg L−1 TE) | 5471 (4583–6295) | 4741 (3600–6447) | 0.488 | 4759 (3978–6310) | 5222 (4145–6119) | 0.184 |
| TEAC (mg L−1 TE) | 296.7 (272.1–328.5) | 322.7 (282.5–352.8) | 0.048 | 299.7 (273.4–326.0) | 321.9 (298.3–351.0) | 0.003 |
| FC (mg L−1GAE) | 1316 (1181–1426) | 1028 (697.3–1289) | 0.005 | 1310 (1164–1454) | 1157 (710.3–1291) | 0.047 |
| GSH (µmol L−1) | 48.33 (44.54–54.60) | 47.19 (44.21–51.63) | 0.389 | 48.46 (45.37–54.29) | 45.72 (42.04–50.57) | 0.050 |
| CHO (mmol L−1) | 5.295 (4.658–6.110) | 5.190 (4.680–6.220) | 0.502 | 5.240 (4.753–6.083) | 5.690 (5.225–6.650) | 0.057 |
| LDL (mmol L−1) | 3.160 (2.473–3.700) | 2.890 (2.600–3.895) | 0.712 | 3.115 (2.543–3.668) | 3.460 (2.840–4.080) | 0.033 |
| HDL (mmol L−1) | 1.400 (1.270–1.633) | 1.420 (1.185–1.740) | 0.941 | 1.435 (1.200–1.620) | 1.450 (1.235–1.890) | 0.118 |
| TG (mmol L−1) | 1.120 (0.850–1.785) | 1.260 (0.795–1.945) | 0.320 | 1.040 (0.843–1.750) | 1.180 (0.820–2.050) | 0.402 |
| Placebo Initial | Placebo 3-Month Follow-Up | p * | Intervention Initial | Intervention 3-Month Follow-Up | p ** | |
|---|---|---|---|---|---|---|
| MDA (µmol L−1) | 0.566 (0.373–0.819) | 0.546 (0.346–1.072) | 0.420 | 0.604 (0.444–1.011) | 0.617 (0.462–1.13) | 0.327 |
| FRAP (µmol L−1 TE) | 395.5 (336.2–445.1) | 403.9 (345.0–462.8) | 0.207 | 398.3 (360.9–449.1) | 392.7 (374.6–428.8) | 0.972 |
| SOD (inhibition (%)) | 58.35 (51.64–64.16) | 59.45 (52.15–63.89) | 0.875 | 59.21 (54.23–66.31) | 59.43 (53.15–64.12) | 0.291 |
| ORAC (mg L−1 TE) | 5471 (4583–6295) | 4759 (3978–6310) | 0.264 | 4741 (3600–6447) | 5222 (4145–6119) | 0.226 |
| TEAC (mg L−1 TE) | 296.7 (272.1–328.5) | 299.7 (273.4–326.0) | 0.593 | 322.7 (282.5–352.8) | 321.9 (298.3–351.0) | 0.581 |
| FC (mg L−1 GAE) | 1316 (1181–1426) | 1310 (1164–1454) | 0.996 | 1028 (697.3–1289) | 1157 (710.3–1291) | 0.888 |
| GSH (µmol L−1) | 48.33 (44.54–54.60) | 48.46 (45.37–54.29) | 0.703 | 47.19 (44.21–51.63) | 45.72 (42.04–50.57) | 0.411 |
| CHO (mmol L−1) | 5.295 (4.658–6.110) | 5.240 (4.753–6.083) | 0.941 | 5.190 (4.680–6.220) | 5.690 (5.225–6.650) | 0.001 |
| LDL (mmol L−1) | 3.160 (2.473–3.700) | 3.115 (2.543–3.668) | 0.277 | 2.890 (2.600–3.895) | 3.460 (2.840–4.080) | 0.006 |
| HDL (mmol L−1) | 1.400 (1.270–1.633) | 1.435 (1.200–1.620) | 0.020 | 1.420 (1.185–1.740) | 1.450 (1.235–1.890) | 0.002 |
| TGC (mmol L−1) | 1.120 (0.850–1.785) | 1.040 (0.843–1.750) | 0.301 | 1.260 (0.795–1.945) | 1.180 (0.820–2.050) | 0.447 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Divković, A.; Karasalihović, Z.; Rumora Samarin, I.; Sabitović, D.; Radić, K.; Golub, N.; Vujić, L.; Rajković, M.G.; Vitali Čepo, D. Effect of Alpha Lipoic Acid Supplementation on Oxidative Stress and Lipid Parameters in Women Diagnosed with Low-Grade Squamous Intraepithelial Lesions (LSILs): A Double-Blind, Randomized, Placebo-Controlled Trial. Antioxidants 2023, 12, 1670. https://doi.org/10.3390/antiox12091670
Divković A, Karasalihović Z, Rumora Samarin I, Sabitović D, Radić K, Golub N, Vujić L, Rajković MG, Vitali Čepo D. Effect of Alpha Lipoic Acid Supplementation on Oxidative Stress and Lipid Parameters in Women Diagnosed with Low-Grade Squamous Intraepithelial Lesions (LSILs): A Double-Blind, Randomized, Placebo-Controlled Trial. Antioxidants. 2023; 12(9):1670. https://doi.org/10.3390/antiox12091670
Chicago/Turabian StyleDivković, Anja, Zinaida Karasalihović, Ivana Rumora Samarin, Damir Sabitović, Kristina Radić, Nikolina Golub, Lovorka Vujić, Marija Grdić Rajković, and Dubravka Vitali Čepo. 2023. "Effect of Alpha Lipoic Acid Supplementation on Oxidative Stress and Lipid Parameters in Women Diagnosed with Low-Grade Squamous Intraepithelial Lesions (LSILs): A Double-Blind, Randomized, Placebo-Controlled Trial" Antioxidants 12, no. 9: 1670. https://doi.org/10.3390/antiox12091670