
Vitamin D Determinants, Status, and Antioxidant/Anti-inflammatory-Related Effects in Cardiovascular Risk and Disease: Not the Last Word in the Controversy
 , , and
, , and
Abstract
:1. Introduction
2. Vitamin D Metabolism: A Brief Summary
3. Methodological Determinants
3.1. Preanalytical Issues
3.2. Analytical Issues
4. Environmental Determinants, Lifestyle Habits, and Skin Pigmentation Affecting 25(OH)D Status
5. Anthropometric Characteristics
6. Vitamin D and Genetic Determinants
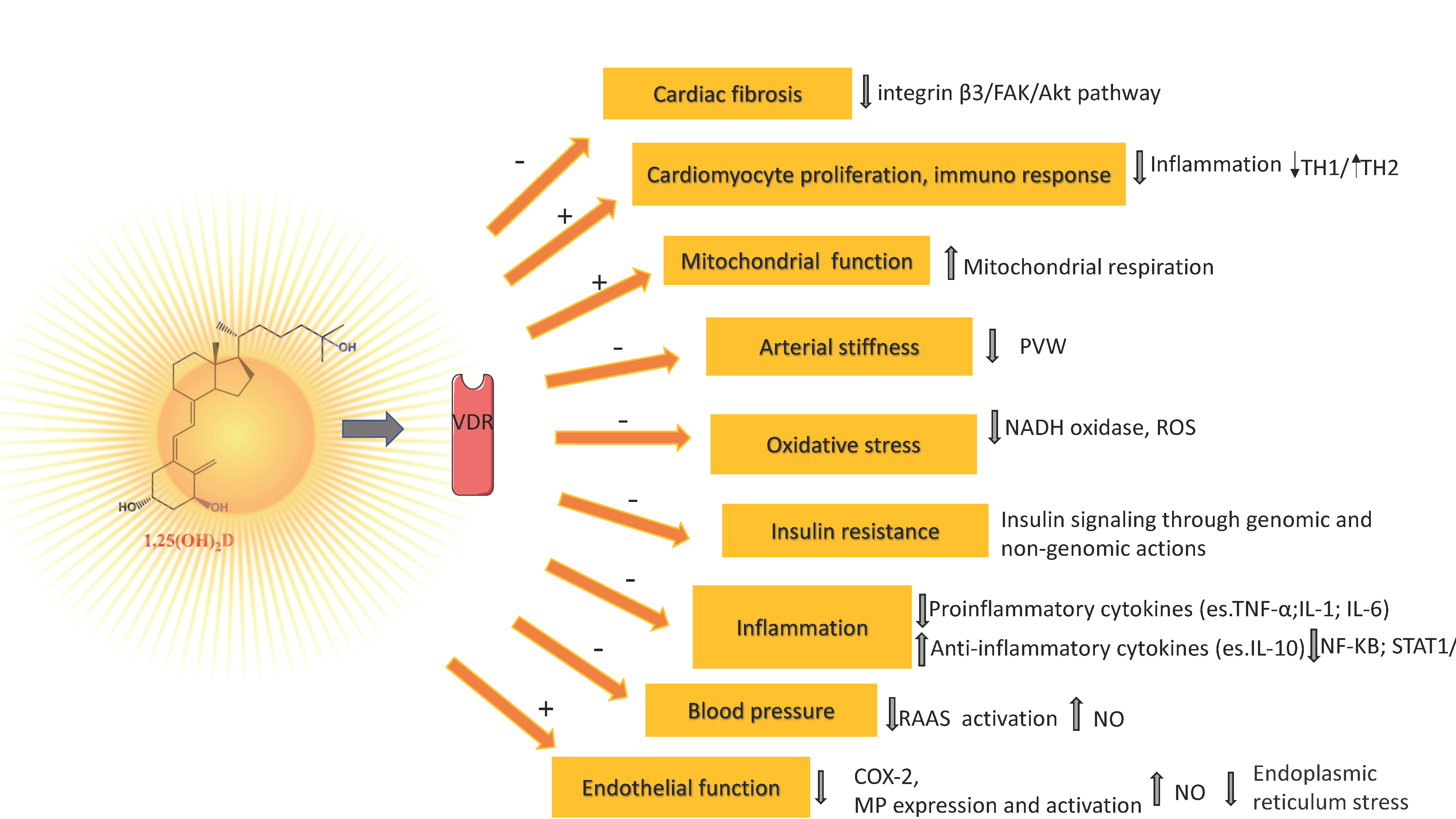
7. Vitamin D Mechanisms Related to Its Antioxidant/Antiinflammatory Action and Vascular Health
8. Observational Studies
9. Randomized Controlled Trials
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silva, I.C.J.; Lazaretti-Castro, M. Vitamin D Metabolism and Extraskeletal Outcomes: An Update. Arch. Endocrinol. Metab. 2022, 66, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Graham, L. IOM Releases Report on Dietary Reference Intakes for Calcium and Vitamin D. Am. Fam. Physician 2011, 83, 1352. [Google Scholar]
- Holick, M.F. The Vitamin D Deficiency Pandemic: Approaches for Diagnosis, Treatment and Prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Huang, S.; Yuan, X.; Wang, Y.; Liu, Y.; Zhou, J. The Role of Vitamin D Deficiency in the Development of Paediatric Diseases. Ann. Med. 2023, 55, 127–135. [Google Scholar] [CrossRef]
- Von Domarus, C.; Brown, J.; Barvencik, F.; Amling, M.; Pogoda, P. How Much Vitamin D Do We Need for Skeletal Health? Clin. Orthop. Relat. Res. 2011, 469, 3127–3133. [Google Scholar] [CrossRef]
- Battault, S.; Whiting, S.J.; Peltier, S.L.; Sadrin, S.; Gerber, G.; Maixent, J.M. Vitamin D Metabolism, Functions and Needs: From Science to Health Claims. Eur. J. Nutr. 2013, 52, 429–441. [Google Scholar] [CrossRef]
- Wacker, M.; Holiack, M.F. Vitamin D-Effects on Skeletal and Extraskeletal Health and the Need for Supplementation. Nutrients 2013, 5, 111–148. [Google Scholar] [CrossRef]
- Valcour, A.; Blocki, F.; Hawkins, D.M.; Rao, S.D. Effects of Age and Serum 25-OH-Vitamin D on Serum Parathyroid Hormone Levels. J. Clin. Endocrinol. Metab. 2012, 97, 3989–3995. [Google Scholar] [CrossRef]
- Norman, A.W. From Vitamin D to Hormone D: Fundamentals of the Vitamin D Endocrine System Essential for Good Health. Am. J. Clin. Nutr. 2008, 88. [Google Scholar] [CrossRef]
- Spedding, S.; Vanlint, S.; Morris, H.; Scragg, R. Does Vitamin D Sufficiency Equate to a Single Serum 25-Hydroxyvitamin D Level or Are Different Levels Required for Non-Skeletal Diseases? Nutrients 2013, 5, 5127–5139. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; et al. Vitamin D Supplementation Guidelines. J. Steroid Biochem. Mol. Biol. 2018, 175, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Cianferotti, L.; Marcocci, C. Subclinical Vitamin D Deficiency. Best Pract. Res. Clin. Endocrinol. Metab. 2012, 26, 523–537. [Google Scholar] [CrossRef]
- Bianchi, S.; Maffei, S.; Prontera, C.; Battaglia, D.; Vassalle, C. Preanalytical, Analytical (DiaSorin LIAISON) and Clinical Variables Potentially Affecting the 25-OH Vitamin D Estimation. Clin. Biochem. 2012, 45, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.M.; Murphy, V.E.; Gibson, P.G.; Clarke, M.; Jensen, M.E. The Impact of Sample Type on Vitamin d Quantification and Clinical Classification during Pregnancy. Nutrients 2020, 12, 3872. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.L.; Falk, R.T.; Kimlin, M.G.; Rajaraman, P.; Sigurdson, A.J.; Horst, R.L.; Cosentino, L.M.; Linet, M.S.; Freedman, D.M. The Impact of Delayed Blood Centrifuging, Choice of Collection Tube, and Type of Assay on 25-Hydroxyvitamin D Concentrations. Cancer Causes Control 2010, 21, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Wielders, J.P.M.; Wijnberg, F.A. Preanalytical Stability of 25(OH)-Vitamin D3 in Human Blood or Serum at Room Temperature: Solid as a Rock. Clin. Chem. 2009, 55, 1584–1585. [Google Scholar] [CrossRef]
- Borai, A.; Khalil, H.; Alghamdi, B.; Alhamdi, R.; Ali, N.; Bahijri, S.; Ferns, G. The Pre-Analytical Stability of 25-Hydroxyvitamin D: Storage and Mixing Effects. J. Clin. Lab. Anal. 2020, 34, e23037. [Google Scholar] [CrossRef]
- Colak, A.; Toprak, B.; Dogan, N.; Ustuner, F. Effect of Sample Type, Centrifugation and Storage Conditions on Vitamin D Concentration. Biochem. Med. 2013, 23, 321–325. [Google Scholar] [CrossRef]
- Zelzer, S.; Meinitzer, A.; Enko, D.; Simstich, S.; Le Goff, C.; Cavalier, E.; Herrmann, M.; Goessler, W. Simultaneous Determination of 24,25- and 25,26-Dihydroxyvitamin D3 in Serum Samples with Liquid-Chromatography Mass Spectrometry–A Useful Tool for the Assessment of Vitamin D Metabolism. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2020, 1158, 122394. [Google Scholar] [CrossRef]
- Cavalier, E. Long-Term Stability of 25-Hydroxyvitamin D: Importance of the Analytical Method and of the Patient Matrix. Clin. Chem. Lab. Med. 2021, 59, E389–E391. [Google Scholar] [CrossRef] [PubMed]
- Carter, G.D. 25-Hydroxyvitamin D Assays: The Quest for Accuracy. Clin. Chem. 2009, 55, 1300–1302. [Google Scholar] [CrossRef] [PubMed]
- Fraser, W.D.; Milan, A.M. Vitamin D Assays: Past and Present Debates, Difficulties, and Developments. Calcif. Tissue Int. 2013, 92, 118–127. [Google Scholar] [CrossRef]
- Sempos, C.T.; Vesper, H.W.; Phinney, K.W.; Thienpont, L.M.; Coates, P.M. Vitamin D Status as an International Issue: National Surveys and the Problem of Standardization. Scand. J. Clin. Lab. Invest. 2012, 72, 32–40. [Google Scholar] [CrossRef]
- Stöckl, D.; Sluss, P.M.; Thienpont, L.M. Specifications for Trueness and Precision of a Reference Measurement System for Serum/Plasma 25-Hydroxyvitamin D Analysis. Clin. Chim. Acta 2009, 408, 8–13. [Google Scholar] [CrossRef]
- Carter, G.D.; Carter, R.; Jones, J.; Berry, J. How Accurate Are Assays for 25-Hydroxyvitamin D? Data from the International Vitamin D External Quality Assessment Scheme. Clin. Chem. 2004, 50, 2195–2197. [Google Scholar] [CrossRef]
- Carter, G.D. Accuracy of 25-Hydroxyvitamin D Assays: Confronting the Issues. Curr. Drug Targets 2010, 12, 19–28. [Google Scholar] [CrossRef]
- CDC Vitamin D Standardization-Certification Program (CDC VDSCP) Certified Total 25-Hydroxyvitamin D Procedures. Available online: https://www.cdc.gov/labstandards/vdscp_participants.html (accessed on 10 February 2023).
- Burdette, C.Q.; Camara, J.E.; Nalin, F.; Pritchett, J.; Sander, L.C.; Carter, G.D.; Jones, J.; Betz, J.M.; Sempos, C.T.; Wise, S.A. Establishing an Accuracy Basis for the Vitamin D External Quality Assessment Scheme (DEQAS). J. AOAC Int. 2017, 100, 1277–1287. [Google Scholar] [CrossRef]
- Nist. Available online: https://www.nist.gov/programs-projects/vitamin-d-metabolites-quality-assurance-program (accessed on 13 February 2023).
- Bianchi, S.; Giovannini, S.; Zucchelli, G.; Clerico, A.; Pierini, M.; Ndreu, R.; Vannucci, A.; Battaglia, D.; Vassalle, C. Analysis of the 2010-2012 Results of the Multicenter External Proficiency Study for 25-Hydroxyvitamin D. Biomark. Med. 2013, 7, 691–699. [Google Scholar] [CrossRef]
- Tai, S.S.C.; Bedner, M.; Phinney, K.W. Development of a Candidate Reference Measurement Procedure for the Determination of 25-Hydroxyvitamin D3 and 25-Hydroxyvitamin D 2 in Human Serum Using Isotope-Dilution Liquid Chromatography Tandem Mass Spectrometry. Anal. Chem. 2010, 82, 1942–1948. [Google Scholar] [CrossRef]
- Binkley, N.; Dawson-Hughes, B.; Durazo-Arvizu, R.; Thamm, M.; Tian, L.; Merkel, J.M.; Jones, J.C.; Carter, G.D.; Sempos, C.T. Vitamin D Measurement Standardization: The Way out of the Chaos. J. Steroid Biochem. Mol. Biol. 2017, 173, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Mineva, E.M.; Schleicher, R.L.; Chaudhary-Webb, M.; Maw, K.L.; Botelho, J.C.; Vesper, H.W.; Pfeiffer, C.M. A Candidate Reference Measurement Procedure for Quantifying Serum Concentrations of 25-Hydroxyvitamin D3 and 25-Hydroxyvitamin D2 Using Isotope-Dilution Liquid Chromatography-Tandem Mass Spectrometry. Anal. Bioanal. Chem. 2015, 407, 5615–5624. [Google Scholar] [CrossRef]
- Carter, G.D. 25-Hydroxyvitamin D: A Difficult Analyte. Clin. Chem. 2012, 58, 486–488. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, F.; Rotundo, S.; Armili, S.; Mimmi, S.; Lucia, F.; Montenegro, N.; Antico, G.C.; Cerra, A.; Gaetano, M.; Galato, F.; et al. Serum 25-Hydroxyvitamin D Measurement: Comparative Evaluation of Three Automated Immunoassays. Pract. Lab. Med. 2021, 26, e00251. [Google Scholar] [CrossRef]
- Henderson, C.M.; Lutsey, P.L.; Misialek, J.R.; Laha, T.J.; Selvin, E.; Eckfeldt, J.H.; Hoofnagle, A.N. Measurement by a Novel LC-MS/MS Methodology Reveals Similar Serum Concentrations of Vitamin D-Binding Protein in Blacks and Whites. Clin. Chem. 2016, 62, 179–187. [Google Scholar] [CrossRef]
- Carter, G.D.; Phinney, K.W. Assessing Vitamin D Status: Time for a Rethink? Clin. Chem. 2014, 60, 809–811. [Google Scholar] [CrossRef]
- Tsiaras, W.G.; Weinstock, M.A. Factors Influencing Vitamin d Status. Acta Derm. Venereol. 2011, 91, 115–124. [Google Scholar] [CrossRef]
- Kimlin, M.G. Geographic Location and Vitamin D Synthesis. Mol. Asp. Med. 2008, 29, 453–461. [Google Scholar] [CrossRef]
- Engelsen, O. The Relationship between Ultraviolet Radiation Exposure and Vitamin D Status. Nutrients 2010, 2, 482–495. [Google Scholar] [CrossRef] [PubMed]
- Spiro, A.; Buttriss, J.L. Vitamin D: An Overview of Vitamin D Status and Intake in Europe. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef]
- Aldrees, T.; Alohali, S.; Albosaily, A.; Almatrafi, S.; Aldhahri, S. Seasonal Variations in Serum Levels of Vitamin D and Other Biochemical Markers among KSA Patients Prior to Thyroid Surgery. J. Taibah Univ. Med. Sci. 2020, 15, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Karagüzel, G.; Dilber, B.; Çan, G.; Ökten, A.; Deǧer, O.; Holick, M.F. Seasonal Vitamin D Status of Healthy Schoolchildren and Predictors of Low Vitamin D Status. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 654–660. [Google Scholar] [CrossRef]
- Bjarnadottir, A.; Kristjansdottir, A.G.; Hrafnkelsson, H.; Johannsson, E.; Magnusson, K.T.; Thorsdottir, I. Insufficient Autumn Vitamin D Intake and Low Vitamin D Status in 7-Year-Old Icelandic Children. Public Health Nutr. 2015, 18, 208–217. [Google Scholar] [CrossRef]
- Petersen, R.A.; Damsgaard, C.T.; Dalskov, S.M.; Sorensen, L.B.; Hjorth, M.F.; Ritz, C.; Kjolbæk, L.; Andersen, R.; Tetens, I.; Krarup, H.; et al. Vitamin D Status and Its Determinants during Autumn in Children at Northern Latitudes: A Cross-Sectional Analysis from the Optimal Well-Being, Development and Health for Danish Children through a Healthy New Nordic Diet (OPUS) School Meal Study. Br. J. Nutr. 2016, 115, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.; Tjønneland, A.; Køster, B.; Brot, C.; Andersen, R.; Cohen, A.S.; Frederiksen, K.; Olsen, A. Vitamin D Status and Seasonal Variation among Danish Children and Adults: A Descriptive Study. Nutrients 2018, 10, 1801. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, C.; Souberbielle, J.C. Is Hypovitaminosis D One of the Environmental Risk Factors for Multiple Sclerosis? Brain 2010, 133, 1869–1888. [Google Scholar] [CrossRef]
- Bhattoa, H.P.; Nagy, E.; More, C.; Kappelmayer, J.; Balogh, A.; Kalina, E.; Antal-Szalmas, P. Prevalence and Seasonal Variation of Hypovitaminosis D and Its Relationship to Bone Metabolism in Healthy Hungarian Men over 50 Years of Age: The HunMen Study. Osteoporos. Int. 2013, 24, 179–186. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D Deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef]
- Ghareghani, M.; Reiter, R.J.; Zibara, K.; Farhadi, N. Latitude, Vitamin D, Melatonin, and Gut Microbiota Act in Concert to Initiate Multiple Sclerosis: A New Mechanistic Pathway. Front. Immunol. 2018, 9, 2484. [Google Scholar] [CrossRef] [PubMed]
- Adami, S.; Bertoldo, F.; Braga, V.; Fracassi, E.; Gatti, D.; Gandolini, G.; Minisola, S.; Battista Rini, G. 25-Hydroxy Vitamin D Levels in Healthy Premenopausal Women: Association with Bone Turnover Markers and Bone Mineral Density. Bone 2009, 45, 423–426. [Google Scholar] [CrossRef]
- Liu, X.; Baylin, A.; Levy, P.D. Vitamin D Deficiency and Insufficiency among US Adults: Prevalence, Predictors and Clinical Implications. Br. J. Nutr. 2018, 119, 928–936. [Google Scholar] [CrossRef] [PubMed]
- Wahl, D.A.; Cooper, C.; Ebeling, P.R.; Eggersdorfer, M.; Hilger, J.; Hoffmann, K.; Josse, R.; Kanis, J.A.; Mithal, A.; Pierroz, D.D.; et al. A Global Representation of Vitamin D Status in Healthy Populations. Arch. Osteoporos. 2012, 7, 155–172. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Pérez-López, F. The Importance of Some Analytical Aspects and Confounding Factors in Relation to Clinical Interpretation of Results. In Vitamin D: Daily Requirements, Dietary Sources and Symptoms of Deficiency; Nova Publisher: New York, NY, USA, 2013; ISBN 978-1-62808-816-8. [Google Scholar]
- Vitale, J.A.; Lombardi, G.; Cavaleri, L.; Graziani, R.; Schoenhuber, H.; La Torre, A.; Banfi, G. Rates of Insufficiency and Deficiency of Vitamin D Levels in Elite Professional Male and Female Skiers: A Chronobiologic Approach. Chronobiol. Int. 2018, 35, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Manios, Y.; Moschonis, G.; Lambrinou, C.P.; Tsoutsoulopoulou, K.; Binou, P.; Karachaliou, A.; Breidenassel, C.; Gonzalez-Gross, M.; Kiely, M.; Cashman, K.D. A Systematic Review of Vitamin D Status in Southern European Countries. Eur. J. Nutr. 2018, 57, 2001–2036. [Google Scholar] [CrossRef] [PubMed]
- Laaksi, I.T.; Ruohola, J.P.S.; Ylikomi, T.J.; Auvinen, A.; Haataja, R.I.; Pihlajamäki, H.K.; Tuohimaa, P.J. Vitamin D Fortification as Public Health Policy: Significant Improvement in Vitamin D Status in Young Finnish Men. Eur. J. Clin. Nutr. 2006, 60, 1035–1038. [Google Scholar] [CrossRef]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L.; Stepan, J.; Fuleihan, G.E.H.; Bouillon, R. Current Vitamin D Status in European and Middle East Countries and Strategies to Prevent Vitamin D Deficiency: A Position Statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, P23–P54. [Google Scholar] [CrossRef]
- Niedermaier, T.; Gredner, T.; Kuznia, S.; Schöttker, B.; Mons, U.; Lakerveld, J.; Ahrens, W.; Brenner, H. Vitamin D Food Fortification in European Countries: The Underused Potential to Prevent Cancer Deaths. Eur. J. Epidemiol. 2022, 37, 309–320. [Google Scholar] [CrossRef]
- Van Schoor, N.M.; Lips, P. Worldwide Vitamin D Status. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 671–680. [Google Scholar] [CrossRef]
- Ames, B.N.; Grant, W.B.; Willett, W.C. Does the High Prevalence of Vitamin d Deficiency in African Americans Contribute to Health Disparities? Nutrients 2021, 13, 499. [Google Scholar] [CrossRef]
- Kramer, H.; Camacho, P.; Aloia, J.; Luke, A.; Bovet, P.; Rhule, J.P.; Forrester, T.; Lambert, V.; Harders, R.; Dugas, L.; et al. Association between 25-Hydroxyvitamin D and Intact Parathyroid Hormone Levels across Latitude among Adults with African Ancestry. Endocr. Pract. 2016, 22, 911–919. [Google Scholar] [CrossRef]
- Batai, K.; Murphy, A.B.; Shah, E.; Ruden, M.; Newsome, J.; Agate, S.; Dixon, M.A.; Chen, H.Y.; Deane, L.A.; Hollowell, C.M.P.; et al. Common Vitamin D Pathway Gene Variants Reveal Contrasting Effects on Serum Vitamin D Levels in African Americans and European Americans. Hum. Genet. 2014, 133, 1395–1405. [Google Scholar] [CrossRef] [PubMed]
- Rozmus, D.; Ciesielska, A.; Płomiński, J.; Grzybowski, R.; Fiedorowicz, E.; Kordulewska, N.; Savelkoul, H.; Kostyra, E.; Cieślińska, A. Vitamin D Binding Protein (VDBP) and Its Gene Polymorphisms—The Risk of Malignant Tumors and Other Diseases. Int. J. Mol. Sci. 2020, 21, 7822. [Google Scholar] [CrossRef] [PubMed]
- Chun, R.F.; Peercy, B.E.; Orwoll, E.S.; Nielson, C.M.; Adams, J.S.; Hewison, M. Vitamin D and DBP: The Free Hormone Hypothesis Revisited. J. Steroid Biochem. Mol. Biol. 2014, 144, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Manicourt, D.H.; Devogelaer, J.P. Urban Tropospheric Ozone Increases the Prevalence of Vitamin d Deficiency among Belgian Postmenopausal Women with Outdoor Activities during Summer. J. Clin. Endocrinol. Metab. 2008, 93, 3893–3899. [Google Scholar] [CrossRef]
- Corrêa, M.P.; Yamamoto, A.L.C.; Moraes, G.R.; Godin-Beekmann, S.; Mahé, E. Changes in the Total Ozone Content over the Period 2006 to 2100 and the Effects on the Erythemal and Vitamin D Effective UV Doses for South America and Antarctica. Photochem. Photobiol. Sci. 2019, 18, 2931–2941. [Google Scholar] [CrossRef]
- Engelsen, O.; Brustad, M.; Aksnes, L.; Lund, E. Daily Duration of Vitamin D Synthesis in Human Skin with Relation to Latitude, Total Ozone, Altitude, Ground Cover, Aerosols and Cloud Thickness. Photochem. Photobiol. 2005, 81, 1287–1290. [Google Scholar] [CrossRef]
- Gao, C.; Qiao, J.; Li, S.S.; Yu, W.J.; He, J.W.; Fu, W.Z.; Zhang, Z.L. The Levels of Bone Turnover Markers 25(OH)D and PTH and Their Relationship with Bone Mineral Density in Postmenopausal Women in a Suburban District in China. Osteoporos. Int. 2017, 28, 211–218. [Google Scholar] [CrossRef]
- Bens, G. Sunscreens. Adv. Exp. Med. Biol. 2014, 810, 429–463. [Google Scholar]
- Buyukuslu, N.; Esin, K.; Hizli, H.; Sunal, N.; Yigit, P.; Garipagaoglu, M. Clothing Preference Affects Vitamin D Status of Young Women. Nutr. Res. 2014, 34, 688–693. [Google Scholar] [CrossRef]
- Datta, P.; Philipsen, P.A.; Olsen, P.; Petersen, B.; Johansen, P.; Morling, N.; Wulf, H.C. Major Inter-Personal Variation in the Increase and Maximal Level of 25-Hydroxy Vitamin D Induced by UVB. Photochem. Photobiol. Sci. 2016, 15, 536–545. [Google Scholar] [CrossRef]
- Meehan, M.; Penckofer, S. The Role of Vitamin D in the Aging Adult. J. Aging Gerontol. 2014, 2, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Kim, S.W. Vitamin D and Chronic Kidney Disease. Korean J. Intern. Med. 2014, 29, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Jean, G.; Souberbielle, J.C.; Chazot, C. Vitamin D in Chronic Kidney Disease and Dialysis Patients. Nutrients 2017, 9, 328. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Di Somma, C.; Laudisio, D.; Salzano, C.; Pugliese, G.; de Alteriis, G.; Colao, A.; Savastano, S. Sex Differences of Vitamin D Status across BMI Classes: An Observational Prospective Cohort Study. Nutrients 2019, 11, 3034. [Google Scholar] [CrossRef]
- Verdoia, M.; Schaffer, A.; Barbieri, L.; Di Giovine, G.; Marino, P.; Suryapranata, H.; De Luca, G. Impact of Gender Difference on Vitamin D Status and Its Relationship with the Extent of Coronary Artery Disease. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 464–470. [Google Scholar] [CrossRef]
- Karacan, M.; Usta, A.; Biçer, S.; Baktır, G.; Gündogan, G.İ.; Usta, C.S.; Akinci, G. Serum Vitamin D Levels in Healthy Urban Population at Reproductive Age: Effects of Age, Gender and Season. Cent. Eur. J. Public Health 2020, 28, 306–312. [Google Scholar] [CrossRef]
- Heaney, R.P.; Recker, R.R.; Grote, J.; Horst, R.L.; Armas, L.A.G. Vitamin D3 Is More Potent than Vitamin D2in Humans. J. Clin. Endocrinol. Metab. 2011, 96, 447–452. [Google Scholar] [CrossRef]
- Nimitphong, H.; Park, E.; Lee, M.J. Vitamin D Regulation of Adipogenesis and Adipose Tissue Functions. Nutr. Res. Pract. 2020, 14, 553–567. [Google Scholar] [CrossRef]
- Pereira-Santos, M.; Costa, P.R.F.; Assis, A.M.O.; Santos, C.A.S.T.; Santos, D.B. Obesity and Vitamin D Deficiency: A Systematic Review and Meta-Analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef]
- Wang, X.; Chang, X.; Zhu, Y.; Wang, H.; Sun, K. Metabolically Obese Individuals of Normal Weight Have a High Risk of 25-Hydroxyvitamin D Deficiency. Am. J. Med. Sci. 2016, 352, 360–367. [Google Scholar] [CrossRef]
- Fiamenghi, V.I.; de Mello, E.D. Vitamin D Deficiency in Children and Adolescents with Obesity: A Meta-Analysis. J. Pediatr. 2021, 97, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Abbas, M.A. Physiological Functions of Vitamin D in Adipose Tissue. J. Steroid Biochem. Mol. Biol. 2017, 165, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Vimaleswaran, K.S.; Berry, D.J.; Lu, C.; Tikkanen, E.; Pilz, S.; Hiraki, L.T.; Cooper, J.D.; Dastani, Z.; Li, R.; Houston, D.K.; et al. Causal Relationship between Obesity and Vitamin D Status: Bi-Directional Mendelian Randomization Analysis of Multiple Cohorts Liisa Hartikainen 38, the Genetic Investigation of Anthropometric Traits (GIANT) Consortium. PLoS Med. 2013, 10, 145–170. [Google Scholar] [CrossRef] [PubMed]
- Verweij, K.J.; Mosing, M.A.; Zietsch, B.P.; Medlan, M. Estimating Heritability from Twin Studies. Stat. Hum. Genet. Methods Protoc. Methods Mol. Biol. 2012, 850, 151–170. [Google Scholar] [CrossRef]
- Karohl, C.; Su, S.; Kumari, M.; Tangpricha, V.; Veledar, E.; Vaccarino, V.; Raggi, P. Heritability and Seasonal Variability of Vitamin D Concentrations in Male Twins. Am. J. Clin. Nutr. 2010, 92, 1393–1398. [Google Scholar] [CrossRef]
- Orton, S.M.; Morris, A.P.; Herrera, B.M.; Ramagopalan, S.V.; Lincoln, M.R.; Chao, M.J.; Vieth, R.; Sadovnick, A.D.; Ebers, G.C. Evidence for Genetic Regulation of Vitamin D Status in Twins with Multiple Sclerosis. Am. J. Clin. Nutr. 2008, 88, 441–447. [Google Scholar] [CrossRef]
- Yu, H.J.; Kwon, M.J.; Woo, H.Y.; Park, H. Analysis of 25-Hydroxyvitamin D Status According to Age, Gender, and Seasonal Variation. J. Clin. Lab. Anal. 2016, 30, 905–911. [Google Scholar] [CrossRef]
- Dastani, Z.; Li, R.; Richards, B. Genetic Regulation of Vitamin D Levels. Calcif. Tissue Int. 2013, 92, 106–117. [Google Scholar] [CrossRef]
- Lander, E.; Kruglyak, L. Genetic Dissection of Complex Traits: Guidelines for Interpreting and Reporting Linkage Results. Nat. Genet. 1995, 11, 241–247. [Google Scholar] [CrossRef]
- Shinkyo, R.; Sakaki, T.; Kamakura, M.; Ohta, M.; Inouye, K. Metabolism of Vitamin D by Human Microsomal CYP2R1. Biochem. Biophys. Res. Commun. 2004, 324, 451–457. [Google Scholar] [CrossRef]
- McGrath, J.J.; Saha, S.; Burne, T.H.J.; Eyles, D.W. A Systematic Review of the Association between Common Single Nucleotide Polymorphisms and 25-Hydroxyvitamin D Concentrations. J. Steroid Biochem. Mol. Biol. 2010, 121, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Sakaki, T.; Kagawa, N.; Yamamoto, K.; Inouye, K. Metabolism of Vitamin D3 by Cytochromes P450. Front. Biosci. 2005, 10, 119–134. [Google Scholar] [PubMed]
- Benjamin, E.J.; Dupuis, J.; Larson, M.G.; Lunetta, K.L.; Booth, S.L.; Govindaraju, D.R.; Kathiresan, S.; Keaney, J.F.; Keyes, M.J.; Lin, J.P.; et al. Genome-Wide Association with Select Biomarker Traits in the Framingham Heart Study. BMC Med. Genet. 2007, 8, S11. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Kiel, D.P.; Kraft, P. The Genetics of Vitamin D. Bone 2019, 126, 59–77. [Google Scholar] [CrossRef]
- Ahn, J.; Yu, K.; Stolzenberg-Solomon, R.; Simon, K.C.; McCullough, M.L.; Gallicchio, L.; Jacobs, E.J.; Ascherio, A.; Helzlsouer, K.; Jacobs, K.B.; et al. Genome-Wide Association Study of Circulating Vitamin D Levels. Hum. Mol. Genet. 2010, 19, 2739–2745. [Google Scholar] [CrossRef]
- Wang, T.J.; Zhang, F.; Richards, J.B.; Kestenbaum, B.; Van Meurs, J.B.; Berry, D.; Kiel, D.P.; Streeten, E.A.; Ohlsson, C.; Koller, D.L.; et al. Common Genetic Determinants of Vitamin D Insufficiency: A Genome-Wide Association Study. Lancet 2010, 376, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; O’Reilly, P.F.; Aschard, H.; Hsu, Y.H.; Richards, J.B.; Dupuis, J.; Ingelsson, E.; Karasik, D.; Pilz, S.; Berry, D.; et al. Genome-Wide Association Study in 79,366 European-Ancestry Individuals Informs the Genetic Architecture of 25-Hydroxyvitamin D Levels. Nat. Commun. 2018, 9, 260. [Google Scholar] [CrossRef]
- Ferrer-Suay, S.; Alonso-Iglesias, E.; Tortajada-Girbés, M.; Carrasco-Luna, J.; Codoñer-Franch, P. Vitamin D Receptor Gene ApaI and FokI Polymorphisms and Its Association with Inflammation and Oxidative Stress in Vitamin D Sufficient Caucasian Spanish Children. Transl. Pediatr. 2021, 10, 103–111. [Google Scholar] [CrossRef]
- Wang, T.T.; Tavera-Mendoza, L.E.; Laperriere, D.; Libby, E.; MacLeod, N.B.; Nagai, Y.; Bourdeau, V.; Konstorum, A.; Lallemant, B.; Zhang, R.; et al. Large-Scale in Silico and Microarray-Based Identification of Direct 1,25-Dihydroxyvitamin D3 Target Genes. Mol. Endocrinol. 2005, 19, 2685–2695. [Google Scholar] [CrossRef]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocr. Rev. 2019, 40, 1109–1151. [Google Scholar] [CrossRef]
- Marino, R.; Misra, M. Extra-Skeletal Effects of Vitamin D. Nutrients 2019, 11, 1460. [Google Scholar] [CrossRef] [PubMed]
- Goncalves-Mendes, N.; Talvas, J.; Dualé, C.; Guttmann, A.; Corbin, V.; Marceau, G.; Sapin, V.; Brachet, P.; Evrard, B.; Laurichesse, H.; et al. Impact of Vitamin D Supplementation on Influenza Vaccine Response and Immune Functions in Deficient Elderly Persons: A Randomized Placebo-Controlled Trial. Front. Immunol. 2019, 10, 65. [Google Scholar] [CrossRef] [PubMed]
- Zmijewski, M.A. Vitamin D and Human Health. Int. J. Mol. Sci. 2019, 20, 145. [Google Scholar] [CrossRef]
- Modarresi-Ghazani, F.; Hejazi, M.E.; Gharekhani, A.; Entezari-Maleki, T. Role of Vitamin D in Cardiovascular Disease. Arch. Iran. Med. 2016, 19, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Doroudi, M.; Cheung, J.; Grozier, A.L.; Schwartz, Z.; Boyan, B.D. Plasma Membrane Pdia3 and VDR Interact to Elicit Rapid Responses to 1α,25(OH)2D3. Cell. Signal. 2013, 25, 2362–2373. [Google Scholar] [CrossRef]
- Zmijewski, M.A.; Carlberg, C. Vitamin D Receptor(s): In the Nucleus but Also at Membranes? Exp. Dermatol. 2020, 29, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Walters, M.R.; Wicker, D.C.; Riggle, P.C. 1,25-Dihydroxyvitamin D3 Receptors Identified in the Rat Heart. J. Mol. Cell. Cardiol. 1986, 18, 67–72. [Google Scholar] [CrossRef]
- Latic, N.; Erben, R.G. Vitamin D and Cardiovascular Disease, with Emphasis on Hypertension, Atherosclerosis, and Heart Failure. Int. J. Mol. Sci. 2020, 21, 6483. [Google Scholar] [CrossRef]
- Cakal, S.; Çakal, B.; Karaca, O. Association of Vitamin D Deficiency with Arterial Stiffness in Newly Diagnosed Hypertension. Blood Press. Monit. 2021, 26, 113–117. [Google Scholar] [CrossRef]
- Barthelmes, J.; Nägele, M.P.; Ludovici, V.; Ruschitzka, F.; Sudano, I.; Flammer, A.J. Endothelial Dysfunction in Cardiovascular Disease and Flammer Syndrome-Similarities and Differences. EPMA J. 2017, 8, 99–109. [Google Scholar] [CrossRef]
- Gallo, G.; Volpe, M.; Savoia, C. Endothelial Dysfunction in Hypertension: Current Concepts and Clinical Implications. Front. Med. 2022, 8, 3022. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Meza, C.A.; Clarke, H.; Kim, J.S.; Hickner, R.C. Vitamin D and Endothelial Function. Nutrients 2020, 12, 575. [Google Scholar] [CrossRef] [PubMed]
- Molinari, C.; Uberti, F.; Grossini, E.; Vacca, G.; Carda, S.; Invernizzi, M.; Cisari, C. 1α,25-Dihydroxycholecalciferol Induces Nitric Oxide Production in Cultured Endothelial Cells. Cell. Physiol. Biochem. 2011, 27, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Andrukhova, O.; Slavic, S.; Zeitz, U.; Riesen, S.C.; Heppelmann, M.S.; Ambrisko, T.D.; Markovic, M.; Kuebler, W.M.; Erben, R.G. Vitamin D Is a Regulator of Endothelial Nitric Oxide Synthase and Arterial Stiffness in Mice. Mol. Endocrinol. 2014, 28, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.K.; Micinski, D.; Huning, L.; Kahlon, G.; Bass, P.F.; Levine, S.N. Vitamin D and L-Cysteine Levels Correlate Positively with GSH and Negatively with Insulin Resistance Levels in the Blood of Type 2 Diabetic Patients. Eur. J. Clin. Nutr. 2014, 68, 1148–1153. [Google Scholar] [CrossRef]
- Nakai, K.; Fujii, H.; Kono, K.; Goto, S.; Kitazawa, R.; Kitazawa, S.; Hirata, M.; Shinohara, M.; Fukagawa, M.; Nishi, S. Vitamin D Activates the Nrf2-Keap1 Antioxidant Pathway and Ameliorates Nephropathy in Diabetic Rats. Am. J. Hypertens. 2014, 27, 586–595. [Google Scholar] [CrossRef]
- Bhat, M.; Ismail, A. Vitamin D Treatment Protects against and Reverses Oxidative Stress Induced Muscle Proteolysis. J. Steroid Biochem. Mol. Biol. 2015, 152, 171–179. [Google Scholar] [CrossRef]
- Calton, E.K.; Keane, K.N.; Newsholme, P.; Soares, M.J. The Impact of Vitamin D Levels on Inflammatory Status: A Systematic Review of Immune Cell Studies. PLoS ONE 2015, 10, e0141770. [Google Scholar] [CrossRef]
- Kunadian, V.; Ford, G.A.; Bawamia, B.; Qiu, W.; Manson, J.E. Vitamin D Deficiency and Coronary Artery Disease: A Review of the Evidence. Am. Heart J. 2014, 167, 283–291. [Google Scholar] [CrossRef]
- Li, Y.C. Molecular Mechanism of Vitamin D in the Cardiovascular System. J. Investig. Med. 2011, 59, 868–871. [Google Scholar] [CrossRef]
- Turin, A.; Bax, J.J.; Doukas, D.; Joyce, C.; Lopez, J.J.; Mathew, V.; Pontone, G.; Shah, F.; Singh, S.; Wilber, D.J.; et al. Interactions Among Vitamin D, Atrial Fibrillation, and the Renin-Angiotensin-Aldosterone System. Am. J. Cardiol. 2018, 122, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Kong, J.; Wei, M.; Chen, Z.-F.; Liu, S.Q.; Cao, L.-P. 1,25-Dihydroxyvitamin D3 Is a Negative Endocrine Regulator of the Renin-Angiotensin System. J. Clin. Investig. 2002, 110, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Pan, W.; Kong, J.; Zheng, W.; Szeto, F.L.; Wong, K.E.; Cohen, R.; Klopot, A.; Zhang, Z.; Yan, C.L. 1,25-Dihydroxyvitamin D3 Suppresses Renin Gene Transcription by Blocking the Activity of the Cyclic AMP Response Element in the Renin Gene Promoter. J. Biol. Chem. 2007, 282, 29821–29830. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Lu, F.; Cao, K.; Xu, D.; Goltzman, D.; Miao, D. Calcium-Independent and 1,25(OH)2D3-Dependent Regulation of the Renin-Angiotensin System in 1α-Hydroxylase Knockout Mice. Kidney Int. 2008, 74, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Chen, L.; Zhang, L.; Xiao, M.; Ding, J.; Goltzman, D.; Miao, D. Administration of Exogenous 1,25(OH)2D3 Normalizes Overactivation of the Central Renin-Angiotensin System in 1α(OH)Ase Knockout Mice. Neurosci. Lett. 2015, 588, 184–189. [Google Scholar] [CrossRef]
- Tomaschitz, A.; Pilz, S.; Ritz, E.; Grammer, T.; Drechsler, C.; Boehm, B.O.; März, W. Independent Association between 1,25-Dihydroxyvitamin D, 25-Hydroxyvitamin D and the Renin-Angiotensin System. The Ludwigshafen Risk and Cardiovascular Health (LURIC) Study. Clin. Chim. Acta 2010, 411, 1354–1360. [Google Scholar] [CrossRef]
- Bernini, G.; Carrara, D.; Bacca, A.; Carli, V.; Virdis, A.; Rugani, I.; Duranti, E.; Ghiadoni, L.; Bernini, M.; Taddei, S. Effect of Acute and Chronic Vitamin D Administration on Systemic Renin Angiotensin Systemin Essential Hypertensives and Controls. J. Endocrinol. Investig. 2013, 36, 216–220. [Google Scholar] [CrossRef]
- McMullan, C.J.; Borgi, L.; Curhan, G.C.; Fisher, N.; Forman, J.P. The Effect of Vitamin D on Renin-Angiotensin System Activation and Blood Pressure: A Randomized Control Trial. J. Hypertens. 2016, 35, 822–829. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Apekey, T.A.; Steur, M. Vitamin D and Risk of Future Hypertension: Meta-Analysis of 283,537 Participants. Eur. J. Epidemiol. 2013, 28, 205–221. [Google Scholar] [CrossRef]
- Zhang, D.; Cheng, C.; Wang, Y.; Sun, H.; Yu, S.; Xue, Y.; Liu, Y.; Li, W.; Li, X. Effect of Vitamin D on Blood Pressure and Hypertension in the General Population: An Update Meta-Analysis of Cohort Studies and Randomized Controlled Trials. Prev. Chronic Dis. 2020, 17, E03. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Burgess, S.; Munroe, P.B.; Khan, H. Vitamin D and High Blood Pressure: Causal Association or Epiphenomenon? Eur. J. Epidemiol. 2014, 29, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Huang, K. Effect of Vitamin D Supplementation on Blood Pressure Parameters in Patients with Vitamin D Deficiency: A Systematic Review and Meta-Analysis. J. Am. Soc. Hypertens. 2018, 12, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; McKenna, W. Hypertrophic Cardiomyopathy: A 50th Anniversary. Heart 2008, 94, 1247–1248. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, A.J.; Scott, D.; Srikanth, V.; Ebeling, P. Effect of Vitamin D Supplementation on Measures of Arterial Stiffness: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Endocrinol. 2016, 84, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.C.; Hsu, C.Y.; Mao, P.C.M.; Dreyer, G.; Wu, F.Z.; Chen, C.L. The Effects of Correction of Vitamin D Deficiency on Arterial Stiffness: A Systematic Review and Updated Meta-Analysis of Randomized Controlled Trials. J. Steroid Biochem. Mol. Biol. 2020, 198. [Google Scholar] [CrossRef]
- Szymczak-Pajor, I.; Śliwińska, A. Analysis of Association between Vitamin d Deficiency and Insulin Resistance. Nutrients 2019, 11, 794. [Google Scholar] [CrossRef]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between Insulin Resistance and the Development of Cardiovascular Disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef]
- Li, Y.X.; Zhou, L. Vitamin D Deficiency, Obesity and Diabetes. Cell. Mol. Biol. 2015, 61, 35–38. [Google Scholar]
- Wang, X.F.; Li, Q.; Sun, X.; Zheng, L.M.; Cheng, S.L.; Zhu, Y.H. Calcitriol Suppressed Isoproterenol-Induced Proliferation of Cardiac Fibroblasts via Integrin Β3/FAK/Akt Pathway. Curr. Med. Sci. 2023, 43, 48–57. [Google Scholar] [CrossRef]
- Yang, S.; Wang, C.; Ruan, C.; Chen, M.; Cao, R.; Sheng, L.; Chang, N.; Xu, T.; Zhao, P.; Liu, X.; et al. Novel Insights into the Cardioprotective Effects of Calcitriol in Myocardial Infarction. Cells 2022, 11, 1676. [Google Scholar] [CrossRef]
- Haas, M.J.; Jafri, M.; Wehmeier, K.R.; Onstead-Haas, L.M.; Mooradian, A.D. Inhibition of Endoplasmic Reticulum Stress and Oxidative Stress by Vitamin D in Endothelial Cells. Free Radic. Biol. Med. 2016, 99, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Reddy, A.M.; Iqbal, M.; Chopra, H.; Urmi, S.; Junapudi, S.; Bibi, S.; Gupta, S.K.; Pangi, V.N.; Singh, I.; Abdel-Daim, M.M. Pivotal Role of Vitamin D in Mitochondrial Health, Cardiac Function, and Human Reproduction. EXCLI J. 2022, 21, 967–990. [Google Scholar] [CrossRef]
- Codoñer-Franch, P.; Tavárez-Alonso, S.; Simó-Jordá, R.; Laporta-Martín, P.; Carratalá-Calvo, A.; Alonso-Iglesias, E. Vitamin D Status Is Linked to Biomarkers of Oxidative Stress, Inflammation, and Endothelial Activation in Obese Children. J. Pediatr. 2012, 161, 848–854. [Google Scholar] [CrossRef]
- Gradinaru, D.; Borsa, C.; Ionescu, C.; Margina, D.; Prada, G.I.; Jansen, E. Vitamin D Status and Oxidative Stress Markers in the Elderly with Impaired Fasting Glucose and Type 2 Diabetes Mellitus. Aging Clin. Exp. Res. 2012, 24, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Asghari, S.; Hamedi-Shahraki, S.; Amirkhizi, F. Vitamin D Status and Systemic Redox Biomarkers in Adults with Obesity. Clin. Nutr. ESPEN 2021, 45, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Cӑtoi, A.F.; Iancu, M.; Pârvu, A.E.; Cecan, A.D.; Bidian, C.; Chera, E.I.; Pop, I.D.; Macri, A.M. Relationship between 25 Hydroxyvitamin d, Overweight/Obesity Status, pro-Inflammatory and Oxidative Stress Markers in Patients with Type 2 Diabetes: A Simplified Empirical Path Model. Nutrients 2021, 13, 2889. [Google Scholar] [CrossRef] [PubMed]
- Dhas, Y.; Banerjee, J.; Damle, G.; Mishra, N. Serum 25(OH)D Concentration and Its Association with Inflammation and Oxidative Stress in the Middle-Aged Indian Healthy and Diabetic Subjects. Steroids 2020, 154, 951–957. [Google Scholar] [CrossRef]
- Jaksic, M.; Martinovic, M.; Gligorovic-Barhanovic, N.; Vujacic, A.; Djurovic, D.; Nedovic-Vukovic, M. Association between Inflammation, Oxidative Stress, Vitamin D, Copper and Zinc with Pre-Obesity and Obesity in School Children from the City of Podgorica, Montenegro. J. Pediatr. Endocrinol. Metab. 2019, 32, 951–957. [Google Scholar] [CrossRef]
- Verdoia, M.; Nardin, M.; Gioscia, R.; Afifeh, A.M.S.; Viglione, F.; Negro, F.; Marcolongo, M.; Luca, G. De Association between Vitamin D Deficiency and Serum Homocysteine Levels and Its Relationship with Coronary Artery Disease. J. Thromb. Thrombolysis 2021, 52, 523–531. [Google Scholar] [CrossRef]
- Danikiewicz, A.; Hudzik, B.; Nowak, J.; Kowalska, J.; Zieleń-Zynek, I.; Szkodzinski, J.; Tun, H.N.; Zubelewicz-Szkodzinska, B. Serum Gamma Glutamyltransferase Is Associated with 25-Hydroxyvitamin d Status in Elderly Patients with Stable Coronary Artery Disease. Int. J. Environ. Res. Public Health 2020, 17, 8980. [Google Scholar] [CrossRef]
- Machulsky, N.F.; Barchuk, M.; Gagliardi, J.; González, D.; Lombardo, M.; Escudero, A.G.; Gigena, G.; Blanco, F.; Schreier, L.; Fabre, B.; et al. Vitamin D Is Related to Markers of Vulnerable Plaque in Acute Myocardial Infarction. Curr. Vasc. Pharmacol. 2017, 15, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Song, Y.; Manson, J.A.E.; Pilz, S.; März, W.; Michaëlsson, K.; Lundqvist, A.; Jassal, S.K.; Barrett-Connor, E.; Zhang, C.; et al. Circulating 25-Hydroxy-Vitamin D and Risk of Cardiovascular Disease: A Meta-Analysis of Prospective Studies. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Brøndum-Jacobsen, P.; Benn, M.; Jensen, G.B.; Nordestgaard, B.G. 25-Hydroxyvitamin D Levels and Risk of Ischemic Heart Disease, Myocardial Infarction, and Early Death: Population-Based Study and Meta-Analyses of 18 and 17 Studies. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2794–2802. [Google Scholar] [CrossRef] [PubMed]
- Tomson, J.; Emberson, J.; Hill, M.; Gordon, A.; Armitage, J.; Shipley, M.; Collins, R.; Clarke, R. Vitamin D and Risk of Death from Vascular and Non-Vascular Causes in the Whitehall Study and Meta-Analyses of 12 000 Deaths. Eur. Heart J. 2013, 34, 1365–1374. [Google Scholar] [CrossRef]
- Gaksch, M.; Jorde, R.; Grimnes, G.; Joakimsen, R.; Schirmer, H.; Wilsgaard, T.; Mathiesen, E.B.; Njølstad, I.; Løchen, M.L.; Maürz, W.; et al. Vitamin D and Mortality: Individual Participant Data Meta-Analysis of Standardized 25-Hydroxyvitamin D in 26916 Individuals from a European Consortium. PLoS ONE 2017, 12, e0170791. [Google Scholar] [CrossRef]
- Yang, J.; Ou-Yang, J.; Huang, J.; Wilhelm, M. Low Serum Vitamin D Levels Increase the Mortality of Cardiovascular Disease in Older Adults: A Dose-Response Meta-Analysis of Prospective Studies. Medicine 2019, 98, 810–819. [Google Scholar] [CrossRef]
- Zhang, R.; Li, B.; Gao, X.; Tian, R.; Pan, Y.; Jiang, Y.; Gu, H.; Wang, Y.; Wang, Y.; Liu, G. Serum 25-HydroxyVitamin D and the Risk of Cardiovascular Disease: Dose-Response Meta-Analysis of Prospective Studies1-3. Am. J. Clin. Nutr. 2017, 105, 810–819. [Google Scholar] [CrossRef]
- Zhou, R.; Wang, M.; Huang, H.; Li, W.; Hu, Y.; Wu, T. Lower Vitamin D Status Is Associated with an Increased Risk of Ischemic Stroke: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 277. [Google Scholar] [CrossRef]
- Gholami, F.; Moradi, G.; Zareei, B.; Rasouli, M.A.; Nikkhoo, B.; Roshani, D.; Ghaderi, E. The Association between Circulating 25-Hydroxyvitamin D and Cardiovascular Diseases: A Meta-Analysis of Prospective Cohort Studies. BMC Cardiovasc. Disord. 2019, 19, 248. [Google Scholar] [CrossRef]
- Dudenkov, D.V.; Mara, K.C.; Maxson, J.A.; Thacher, T.D. Serum 25-Hydroxyvitamin D Values and Risk of Incident Cardiovascular Disease: A Population-Based Retrospective Cohort Study. J. Steroid Biochem. Mol. Biol. 2021, 213, 105953. [Google Scholar] [CrossRef]
- Del Valle, H.B.; Yaktine, A.L.; Taylor, C.L.; Ross, A.C. Dietary Reference Intakes for Calcium and Vitamin. In Institute of Medicine Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Wang, T.; Sun, H.; Ge, H.; Liu, X.; Yu, F.; Han, H.; Wang, J.; Li, W. Association between Vitamin D and Risk of Cardiovascular Disease in Chinese Rural Population. PLoS ONE 2019, 14, e0217311. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Sabour, S.; Sagar, U.N.; Adams, S.; Whellan, D.J. Prevalence of Hypovitaminosis D in Cardiovascular Diseases (from the National Health and Nutrition Examination Survey 2001 to 2004). Am. J. Cardiol. 2008, 102, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, J.; Targher, G.; Smits, G.; Chonchol, M. 25-Hydroxyvitamin D Deficiency Is Independently Associated with Cardiovascular Disease in the Third National Health and Nutrition Examination Survey. Atherosclerosis 2009, 205, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Melamed, M.L.; Muntner, P.; Michos, E.D.; Uribarri, J.; Weber, C.; Sharma, J.; Raggi, P. Serum 25-Hydroxyvitamin D Levels and the Prevalence of Peripheral Arterial Disease Results from NHANES 2001 to 2004. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.; Liu, Y.; Hollis, B.W.; Rimm, E.B. 25-Hydroxyvitamin D and Risk of Myocardial Infarction in Men: A Prospective Study. Arch. Intern. Med. 2008, 168, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; D’Agostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D Deficiency and Risk of Cardiovascular Disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Schaffer, A.; Sartori, C.; Barbieri, L.; Cassetti, E.; Marino, P.; Galasso, G.; Luca, G. De Vitamin D Deficiency Is Independently Associated with the Extent of Coronary Artery Disease. Eur. J. Clin. Investig. 2014, 44, 634–642. [Google Scholar] [CrossRef]
- Lee, J.H.; Gadi, R.; Spertus, J.A.; Tang, F.; O’Keefe, J.H. Prevalence of Vitamin D Deficiency in Patients with Acute Myocardial Infarction. Am. J. Cardiol. 2011, 107, 1636–1638. [Google Scholar] [CrossRef]
- Pingitore, A.; Mastorci, F.; Berti, S.; Sabatino, L.; Palmieri, C.; Iervasi, G.; Vassalle, C. Hypovitaminosis D and Low T3 Syndrome: A Link for Therapeutic Challenges in Patients with Acute Myocardial Infarction. J. Clin. Med. 2021, 10, 5267. [Google Scholar] [CrossRef]
- Leu, M.; Giovannucci, E. Vitamin D: Epidemiology of Cardiovascular Risks and Events. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 633–646. [Google Scholar] [CrossRef]
- Krivošíková, Z.; Gajdoš, M.; Šebeková, K. Vitamin D Levels Decline with Rising Number of Cardiometabolic Risk Factors in Healthy Adults: Association with Adipokines, Inflammation, Oxidative Stress and Advanced Glycation Markers. PLoS ONE 2015, 10, e0131753. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.W.; Siu, P.M.; Pang, M.Y.; Woo, J.; Collins, A.R.; Benzie, I.F.F. Vitamin D Deficiency, Oxidative Stress and Antioxidant Status: Only Weak Association Seen in the Absence of Advanced Age, Obesity or Pre-Existing Disease. Br. J. Nutr. 2017, 118, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Juonala, M.; Voipio, A.; Pahkala, K.; Viikari, J.S.A.; Mikkilä, V.; Kähönen, M.; Hutri-Kähönen, N.; Jula, A.; Burgner, D.; Sabin, M.A.; et al. Childhood 25-OH Vitamin D Levels and Carotid Intima-Media Thickness in Adulthood: The Cardiovascular Risk in Young Finns Study. J. Clin. Endocrinol. Metab. 2015, 100, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Elamin, M.B.; Elnour, N.O.A.; Elamin, K.B.; Fatourechi, M.M.; Alkatib, A.A.; Almandoz, J.P.; Liu, H.; Lane, M.A.; Mullan, R.J.; Hazem, A.; et al. Vitamin D and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2011, 96, 1931–1942. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.; Gamble, G.D.; Reid, I.R. The Effect of Vitamin D Supplementation on Skeletal, Vascular, or Cancer Outcomes: A Trial Sequential Meta-Analysis. Lancet Diabetes Endocrinol. 2014, 2, 307–320. [Google Scholar] [CrossRef]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L.; et al. Vitamin D Supplementation and Cardiovascular Disease Risks in More Than 83000 Individuals in 21 Randomized Clinical Trials: A Meta-Analysis. JAMA Cardiol. 2019, 4, 765–775. [Google Scholar] [CrossRef]
- Pei, Y.Y.; Zhang, Y.; Peng, X.C.; Liu, Z.R.; Xu, P.; Fang, F. Association of Vitamin D Supplementation with Cardiovascular Events: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 3158. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Wetterslev, J.; Simonetti, R.G.; Bjelakovic, M.; Gluud, C. Vitamin D Supplementation for Prevention of Mortality in Adults. Cochrane Database Syst. Rev. 2014, 2014, CD007470. [Google Scholar] [CrossRef]
- Rejnmark, L.; Avenell, A.; Masud, T.; Anderson, F.; Meyer, H.E.; Sanders, K.M.; Salovaara, K.; Cooper, C.; Smith, H.E.; Jacobs, E.T.; et al. Vitamin D with Calcium Reduces Mortality: Patient Level Pooled Analysis of 70,528 Patients from Eight Major Vitamin D Trials. J. Clin. Endocrinol. Metab. 2012, 97, 2670–2681. [Google Scholar] [CrossRef]
- Kalvandi, F.; Azarbayjani, M.A.; Azizbeigi, R.; Azizbeigi, K. Elastic Resistance Training Is More Effective than Vitamin D3 Supplementation in Reducing Oxidative Stress and Strengthen Antioxidant Enzymes in Healthy Men. Eur. J. Clin. Nutr. 2022, 76, 610–615. [Google Scholar] [CrossRef]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Esmaillzadeh, A. Vitamin D Supplementation Affects Serum High-Sensitivity C-Reactive Protein, Insulin Resistance, and Biomarkers of Oxidative Stress in Pregnant Women. J. Nutr. 2013, 143, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Timar, A.; Saberi-Karimian, M.; Ghazizadeh, H.; Parizadeh, S.M.R.; Sabbaghzadeh, R.; Emadzadeh, M.; Eshaghi, F.; Tavallaie, S.; Ferns, G.A.; Ghayour-Mobarhan, M. Evaluation of the Serum Prooxidant-Antioxidant Balance before and after Vitamin D Supplementation in Adolescent Iranian Girls. Adv. Med. Sci. 2019, 64, 174–180. [Google Scholar] [CrossRef]
- de Medeiros Cavalcante, I.G.; Silva, A.S.; Costa, M.J.C.; Persuhn, D.C.; Issa, C.T.M.I.; de Luna Freire, T.L.; da Conceição Rodrigues Gonçalves, M. Effect of Vitamin D3 Supplementation and Influence of BsmI Polymorphism of the VDR Gene of the Inflammatory Profile and Oxidative Stress in Elderly Women with Vitamin D Insufficiency Vitamin D3 Megadose Reduces Inflammatory Markers. Exp. Gerontol. 2015, 66, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Scholten, S.; Sergeev, I.; Birger, C.; Song, Q. Effects of Vitamin D and Quercetin, Alone and in Combination, on Cardiorespiratory Fitness and Muscle Function in Physically Active Male Adults. Open Access J. Sport. Med. 2015, 6, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Nikooyeh, B.; Neyestani, T.R.; Tayebinejad, N.; Alavi-Majd, H.; Shariatzadeh, N.; Kalayi, A.; Zahedirad, M.; Heravifard, S.; Salekzamani, S. Daily Intake of Vitamin D- or Calcium-Vitamin D-Fortified Persian Yogurt Drink (Doogh) Attenuates Diabetes-Induced Oxidative Stress: Evidence for Antioxidative Properties of Vitamin D. J. Hum. Nutr. Diet. 2014, 27, 276–823. [Google Scholar] [CrossRef]
- Tamadon, M.R.; Soleimani, A.; Keneshlou, F.; Mojarrad, M.Z.; Bahmani, F.; Naseri, A.; Kashani, H.H.; Hosseini, E.S.; Asemi, Z. Clinical Trial on the Effects of Vitamin D Supplementation on Metabolic Profiles in Diabetic Hemodialysis. Horm. Metab. Res. 2018, 50, 50–55. [Google Scholar] [CrossRef]
- Johny, E.; Jala, A.; Nath, B.; Alam, M.J.; Kuladhipati, I.; Das, R.; Borkar, R.M.; Adela, R. Vitamin D Supplementation Modulates Platelet-Mediated Inflammation in Subjects With Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Front. Immunol. 2022, 13, 869591. [Google Scholar] [CrossRef]
- Pasupuleti, P.; Suchitra, M.M.; Bitla, A.R.; Sachan, A. Attenuation of Oxidative Stress, Interleukin-6, High-Sensitivity C-Reactive Protein, Plasminogen Activator Inhibitor-1, and Fibrinogen with Oral Vitamin D Supplementation in Patients with T2DM Having Vitamin D Deficiency. J. Lab. Physicians 2022, 14, 190–196. [Google Scholar] [CrossRef]
- Thethi, T.K.; Bajwa, M.A.; Ghanim, H.; Jo, C.; Weir, M.; Goldfine, A.B.; Umpierrez, G.; Desouza, C.; Dandona, P.; Fang-Hollingsworth, Y.; et al. Effect of Paricalcitol on Endothelial Function and Inflammation in Type 2 Diabetes and Chronic Kidney Disease. J. Diabetes Complicat. 2015, 29, 433–437. [Google Scholar] [CrossRef]
- Yiu, Y.F.; Yiu, K.H.; Siu, C.W.; Chan, Y.H.; Li, S.W.; Wong, L.Y.; Lee, S.W.L.; Tam, S.; Wong, E.W.K.; Lau, C.P.; et al. Randomized Controlled Trial of Vitamin D Supplement on Endothelial Function in Patients with Type 2 Diabetes. Atherosclerosis 2013, 227, 140–146. [Google Scholar] [CrossRef]
- Sokol, S.I.; Srinivas, V.; Crandall, J.P.; Kim, M.; Tellides, G.; Lebastchi, A.; Yu, Y.; Gupta, A.K.; Alderman, M.H. The Effects of Vitamin D Repletion on Endothelial Function and Inflammation in Patients with Coronary Artery Disease. Vasc. Med. 2012, 17, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Wang, T.; Zhu, S.; Li, L. Effects of Vitamin D Supplementation as an Adjuvant Therapy in Coronary Artery Disease Patients. Scand. Cardiovasc. J. 2016, 50, 9–16. [Google Scholar] [CrossRef]
- Aslanabadi, N.; Jafaripor, I.; Sadeghi, S.; Hamishehkar, H.; Ghaffari, S.; Toluey, M.; Azizi, H.; Entezari-Maleki, T. Effect of Vitamin D in the Prevention of Myocardial Injury Following Elective Percutaneous Coronary Intervention: A Pilot Randomized Clinical Trial. J. Clin. Pharmacol. 2018, 58, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, L.S.; Ranjbar, G.; Norouzy, A.; Arabi, S.M. Vitamin D Supplementation Effects on the Clinical Outcomes of Patients with Coronary Artery Disease: A Systematic Review and Meta-Analysis. Sci. Rep. 2020, 10, 12923. [Google Scholar] [CrossRef]
- Renke, G.; Starling-Soares, B.; Baesso, T.; Petronio, R.; Aguiar, D.; Paes, R. Effects of Vitamin D on Cardiovascular Risk and Oxidative Stress. Nutrients 2023, 15, 769. [Google Scholar] [CrossRef]
- Saponaro, F.; Marcocci, C.; Zucchi, R. Vitamin D Status and Cardiovascular Outcome. J. Endocrinol. Investig. 2019, 42, 1285–1290. [Google Scholar] [CrossRef]
- Simsek, B.; Selte, A.; Egeli, B.H.; Çakatay, U. Effects of vitamin supplements on clinical cardiovascular outcomes: Time to move on!–A comprehensive review. Clin. Nutr. ESPEN 2021, 42, 1–14. [Google Scholar] [CrossRef]
- Milazzo, V.; De Metrio, M.; Cosentino, N.; Marenzi, G.; Tremoli, E. Vitamin D and acute myocardial infarction. World J. Cardiol. 2017, 9, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Genzen, J.R.; Gosselin, J.T.; Wilson, T.C.; Racila, E.; Krasowski, M.D. Analysis of vitamin D status at two academic medical centers and a national reference laboratory: Result patterns vary by age, gender, season, and patient location. BMC Endocr. Disord. 2013, 3, 52. [Google Scholar] [CrossRef]
- Płudowski, P.; Kos-Kudła, B.; Walczak, M.; Fal, A.; Zozulińska-Ziółkiewicz, D.; Sieroszewski, P.; Peregud-Pogorzelski, J.; Lauterbach, R.; Targowski, T.; Lewiński, A.; et al. Guidelines for Preventing and Treating Vitamin D Deficiency: A 2023 Update in Poland. Nutrients 2023, 15, 695. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Preanalytical Issues | Analytical Issues | |||
|---|---|---|---|---|
| High-Performance Liquid Chromatography (HPLC), Liquid Chromatography-Mass Spectrometry (LC-MS) | IMMUNOASSAY (Enzyme-Linked Immunosorbent Assay-ELISA, Radioimmunoassay-RIA, Chemiluminescence Immunoassay-CLIA) | |||
| Advantages | Disadvantages | Advantages | Disadvantages | |
|
|
|
|
|
| Environmental Determinants | Anthropometric Determinants | Life-Style Determinants |
|---|---|---|
sunlight exposure: intensity and duration season latitude length of day presence of clouds air pollution/ozone | aging race/phototype gender body mass index/obesity genetic asset: presence of specific polymorphisms hepatic/renal dysfunction pregnancy | dietary intake supplementation/fortified foods sunscreen/clothes time spent outdoor/outdoor sports |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Della Nera, G.; Sabatino, L.; Gaggini, M.; Gorini, F.; Vassalle, C. Vitamin D Determinants, Status, and Antioxidant/Anti-inflammatory-Related Effects in Cardiovascular Risk and Disease: Not the Last Word in the Controversy. Antioxidants 2023, 12, 948. https://doi.org/10.3390/antiox12040948
Della Nera G, Sabatino L, Gaggini M, Gorini F, Vassalle C. Vitamin D Determinants, Status, and Antioxidant/Anti-inflammatory-Related Effects in Cardiovascular Risk and Disease: Not the Last Word in the Controversy. Antioxidants. 2023; 12(4):948. https://doi.org/10.3390/antiox12040948
Chicago/Turabian StyleDella Nera, Giulia, Laura Sabatino, Melania Gaggini, Francesca Gorini, and Cristina Vassalle. 2023. "Vitamin D Determinants, Status, and Antioxidant/Anti-inflammatory-Related Effects in Cardiovascular Risk and Disease: Not the Last Word in the Controversy" Antioxidants 12, no. 4: 948. https://doi.org/10.3390/antiox12040948