

Assessment of Oxidative Stress Markers in Hypertensive Patients under the Use of Renin-Angiotensin-Aldosterone Blockers
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Parameters of 24-h ABPM Collection
2.3. Clinical and Laboratory Baseline Variables
2.4. Assessment of Thiobarbituric Acid Reactive Substances
2.5. Assessment of Reduced Thiols
2.6. Ethics Statement
2.7. Statistical Analysis
3. Results
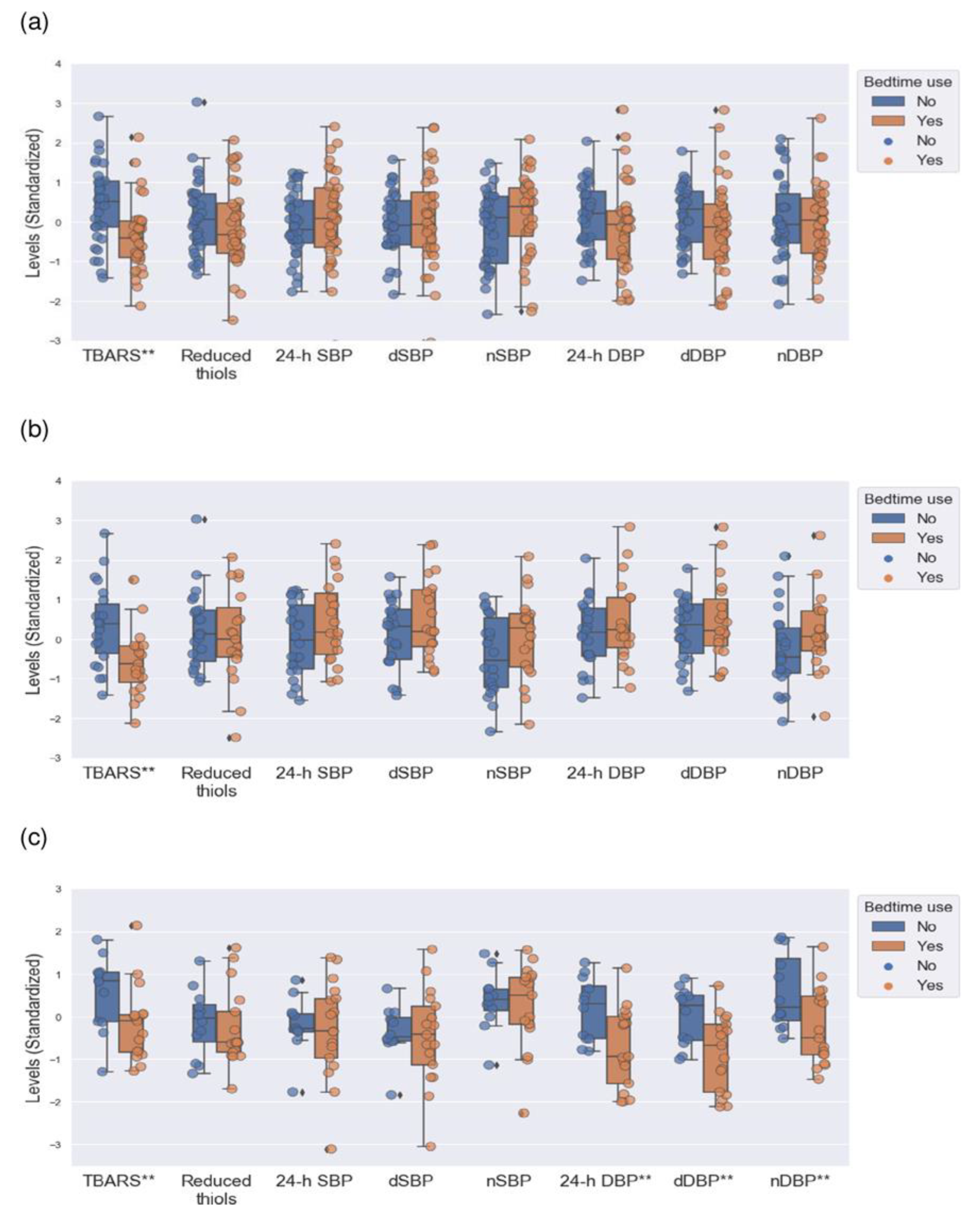
3.1. Comparisons between Hypertensive Patients with Morning and Bedtime Use of RAAS Blockers
3.2. Comparisons between Dipper Patients with Morning and Bedtime Use of RAAS Blockers
3.3. Comparisons between Non-Dipper Patients with Morning and Bedtime Use of RAAS Blockers
3.4. Multivariate Analysis: Association between TBARS Levels and Bedtime Use of RAAS Blockers
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, L.C.; Oliveira-Paula, G.H. Sources and Effects of Oxidative Stress in Hypertension. Curr. Hypertens. Rev. 2020, 16, 166–180. [Google Scholar] [CrossRef] [PubMed]
- Gaschler, M.M.; Stockwell, B.R. Lipid peroxidation in cell death. Biochem. Biophys. Res. Commun. 2017, 482, 419–425. [Google Scholar] [CrossRef]
- Benhar, M. Oxidants, Antioxidants and Thiol Redox Switches in the Control of Regulated Cell Death Pathways. Antioxidants 2020, 9, 309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowles, N.P.; Thosar, S.S.; Herzig, M.X.; Shea, S.A. Chronotherapy for Hypertension. Curr. Hypertens. Rep. 2018, 20, 97. [Google Scholar] [CrossRef]
- Ames, M.K.; Atkins, C.E.; Pitt, B. The renin-angiotensin-aldosterone system and its suppression. J. Vet. Intern. Med. 2019, 33, 363–382. [Google Scholar] [CrossRef] [Green Version]
- Ismail, H.; Mitchell, R.; McFarlane, S.I.; Makaryus, A.N. Pleiotropic effects of inhibitors of the RAAS in the diabetic population: Above and beyond blood pressure lowering. Curr. Diabetes Rep. 2010, 10, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Manrique, C.; Lastra, G.; Gardner, M.; Sowers, J.R. The renin angiotensin aldosterone system in hypertension: Roles of insulin resistance and oxidative stress. Med. Clin. N. Am. 2009, 93, 569–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stergiou, G.S.; Palatini, P.; Parati, G.; O’Brien, E.; Januszewicz, A.; Lurbe, E.; Persu, A.; Mancia, G.; Kreutz, R. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J. Hypertens. 2021, 39, 1293–1302. [Google Scholar] [CrossRef]
- Ben, A.J.; Neumann, C.R.; Mengue, S.S. The Brief Medication Questionnaire and Morisky-Green test to evaluate medication adherence. Rev. Saude Publica 2012, 46, 279–289. [Google Scholar] [CrossRef] [Green Version]
- Twomey, P.J.; Reynolds, T.M. The MDRD formula and validation. QJM 2006, 99, 804–805. [Google Scholar] [CrossRef] [Green Version]
- Ohkawa, H.; Ohishi, N.; Yagi, K. Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Anal. Biochem. 1979, 95, 351–358. [Google Scholar] [CrossRef]
- Hoving, E.B.; Laing, C.; Rutgers, H.M.; Teggeler, M.; van Doormaal, J.J.; Muskiet, F.A. Optimized determination of malondialdehyde in plasma lipid extracts using 1,3-diethyl-2-thiobarbituric acid: Influence of detection method and relations with lipids and fatty acids in plasma from healthy adults. Clin. Chim. Acta 1992, 208, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Ellman, G.L. Tissue sulfhydryl groups. Arch. Biochem. Biophys. 1959, 82, 70–77. [Google Scholar] [CrossRef]
- Turell, L.; Radi, R.; Alvarez, B. The thiol pool in human plasma: The central contribution of albumin to redox processes. Free Radic. Biol. Med. 2013, 65, 244–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kafatos, G.; Verlander, N.Q.; Gelb, D.; Arnold, E.; Charlett, A. A comparison of public domain software for outbreak investigations: Epi Info and EpiData. Euro Surveill. 2007, 12, E070111.4. [Google Scholar] [CrossRef]
- Siti, H.N.; Kamisah, Y.; Kamsiah, J. The role of oxidative stress, antioxidants and vascular inflammation in cardiovascular disease (a review). Vasc. Pharmacol. 2015, 71, 40–56. [Google Scholar] [CrossRef] [PubMed]
- Stanley, C.P.; Stocker, R. Regulation of vascular tone and blood pressure by singlet molecular oxygen in inflammation. Curr. Opin. Nephrol. Hypertens. 2021, 30, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Agra, N.; Cruces-Sande, A.; Mendez-Alvarez, E.; Soto-Otero, R.; Cinza-Sanjurjo, S.; Lopez-Paz, J.-E.; Pose-Reino, A.; Hermida-Ameijeiras, A. Correlation between Blunted Nocturnal Decrease in Diastolic Blood Pressure and Oxidative Stress: An Observational Study. Antioxidants 2022, 11, 2430. [Google Scholar] [CrossRef]
- Fanelli, C.; Zatz, R. Linking oxidative stress, the renin-angiotensin system, and hypertension. Hypertension 2011, 57, 373–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamazaki, T.; Tanimoto, M.; Gohda, T.; Ohara, I.; Hagiwara, S.; Murakoshi, M.; Matsumoto, M.; Kaneko, S.; Aoki, T.; Toyoda, H.; et al. Combination effects of enalapril and losartan on lipid peroxidation in the kidneys of KK-Ay/Ta mice. Nephron Exp. Nephrol. 2009, 113, e66–e76. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Fujioka, S.; Takahashi, R.; Oe, T. Angiotensin II-Induced Oxidative Stress in Human Endothelial Cells: Modification of Cellular Molecules through Lipid Peroxidation. Chem. Res. Toxicol. 2019, 32, 1412–1422. [Google Scholar] [CrossRef] [PubMed]
- Minas, J.N.; Thorwald, M.A.; Conte, D.; Vázquez-Medina, J.-P.; Nishiyama, A.; Ortiz, R.M. Angiotensin and mineralocorticoid receptor antagonism attenuates cardiac oxidative stress in angiotensin II-infused rats. Clin. Exp. Pharmacol. Physiol. 2015, 42, 1178–1188. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Ren, L.; Jiang, M.; Chu, Y. Anti-hypertensive efficacy of amlodipine dosing during morning versus evening: A meta-analysis. Rev. Cardiovasc. Med. 2019, 20, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Prkacin, I.; Balenovic, D.; Djermanovic-Dobrota, V.; Lukac, I.; Drazic, P.; Pranjic, I.-K. Resistant hypertension and chronotherapy. Mater. Sociomed. 2015, 27, 118–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smolensky, M.H.; Hermida, R.C.; Ayala, D.E.; Portaluppi, F. Bedtime hypertension chronotherapy: Concepts and patient outcomes. Curr. Pharm. Des. 2015, 21, 773–790. [Google Scholar] [CrossRef]
- Stranges, P.M.; Drew, A.M.; Rafferty, P.; Shuster, J.E.; Brooks, A.D. Treatment of hypertension with chronotherapy: Is it time of drug administration? Ann. Pharmacother. 2015, 49, 323–334. [Google Scholar] [CrossRef]
- Hermida, R.C.; Ayala, D.E.; Smolensky, M.H.; Fernández, J.R.; Mojón, A.; Portaluppi, F. Chronotherapy with conventional blood pressure medications improves management of hypertension and reduces cardiovascular and stroke risks. Hypertens. Res. 2016, 39, 277–292. [Google Scholar] [CrossRef]
- Craighead, D.H.; Heinbockel, T.C.; Freeberg, K.A.; Rossman, M.J.; Jackman, R.A.; Jankowski, L.R.; Hamilton, M.N.; Ziemba, B.P.; Reisz, J.A.; D’Alessandro, A.; et al. Time-Efficient Inspiratory Muscle Strength Training Lowers Blood Pressure and Improves Endothelial Function, NO Bioavailability, and Oxidative Stress in Midlife/Older Adults With Above-Normal Blood Pressure. J. Am. Heart Assoc. 2021, 10, e020980. [Google Scholar] [CrossRef]
- Wilking, M.; Ndiaye, M.; Mukhtar, H.; Ahmad, N. Circadian rhythm connections to oxidative stress: Implications for human health. Antioxid. Redox Signal. 2013, 19, 192–208. [Google Scholar] [CrossRef] [Green Version]
- Thosar, S.S.; Rueda, J.F.; Berman, A.M.; Lasarev, M.R.; Herzig, M.X.; Clemons, N.A.; Roberts, S.A.; Bowles, N.P.; Emens, J.S.; Ellison, D.H.; et al. Separate and interacting effects of the endogenous circadian system and behaviors on plasma aldosterone in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2019, 316, R157–R164. [Google Scholar] [CrossRef] [PubMed]
- Kario, K.; Shimada, K. Risers and extreme-dippers of nocturnal blood pressure in hypertension: Antihypertensive strategy for nocturnal blood pressure. Clin. Exp. Hypertens. 2004, 26, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Tsikas, D. Assessment of lipid peroxidation by measuring malondialdehyde (MDA) and relatives in biological samples: Analytical and biological challenges. Anal. Biochem. 2017, 524, 13–30. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total n = 70 | All Patients 1 n = 70 | Dippers 2 n = 41 | Non-Dippers 3 n = 29 | |||
|---|---|---|---|---|---|---|---|
| Morning-Time n = 34 | Bedtime n = 36 | Morning-Time n = 22 | Bedtime n = 19 | Morning-Time n = 12 | Bedtime n = 17 | ||
| Age (years) † | 54 (14) | 49 (17) | 57 (13) a | 48 (18) | 58 (12) c | 55 (21) | 57 (15) |
| Sex (women) ‡ | 38 (54) | 20 (59) | 18 (50) | 13 (59) | 7 (37) | 7 (58) | 11 (65) |
| Weight (kg) † | 75 (27) | 70 (34) | 77 (25) | 70 (33) | 75 (22) | 70 (29) | 80 (27) |
| Height (cm) † | 164 (12) | 164 (10) | 164 (16) | 161 (12) | 170 (16) | 165 (10) | 163 (11) |
| BMI (kg/m2) † | 29 (6) | 27 (7) | 29 (6) b | 27 (8) | 29 (5) | 28 (5) | 31 (7) |
| WC (cm) † | 101 (20) | 98 (29) | 104 (13) | 93 (29) | 103 (26) | 101 (31) | 105 (18) |
| Alcohol intake (yes) ‡ | 11 (16) | 5 (15) | 6 (17) | 1 (5) | 2 (10) | 4 (33) | 4 (24) |
| Non-dipper profile (yes) ‡ | 29 (41) | 12 (35) | 17 (47) | ||||
| Compliant patients (yes) ‡ | 66 (94) | 32 (94) | 34 (94) | 21 (96) | 17 (90) | 11 (92) | 17 (100) |
| ACEIs ‡ | 17 (24) | 8 (24) | 9 (25) | 3 (14) | 4 (21) | 5 (41) | 5 (30) |
| ARBs ‡ | 49 (70) | 25 (74) | 24 (67) | 19 (86) | 13 (69) | 6 (50) | 11 (64) |
| MRAs ‡ | 4 (6) | 1 (3) | 3 (8) | 0 (0) | 2 (10) | 1 (8) | 1 (6) |
| Variables | Total n = 70 | All Patients 1 n = 70 | Dippers 2 n = 41 | Non-Dippers 3 n = 29 | |||
|---|---|---|---|---|---|---|---|
| Morning-Time n = 34 | Bedtime n = 36 | Morning-Time n = 22 | Bedtime n = 19 | Morning-Time n = 12 | Bedtime n = 17 | ||
| 24-hSBP (mmHg) † | 125 (15) | 123 (14) | 126 (18) | 125 (20) | 127 (21) | 122 (5) | 121 (18) |
| dSBP (mmHg) † | 129 (15) | 129 (15) | 130 (20) | 135 (18) | 133 (20) | 124 (8) | 125 (21) |
| nSBP (mmHg) † | 116 (19) | 114 (21) | 118 (17) | 107 (22) | 116 (17) | 118 (7) | 119 (14) |
| 24-hDBP (mmHg) † | 76 (14) | 79 (12) | 76 (11) | 78 (12) | 79 (12) | 79 (13) | 68 (16) a |
| dDBP (mmHg) † | 79 (15) | 84 (13) | 80 (15) | 85 (14) | 83 (15) | 84 (12) | 74 (17) b |
| nDBP (mmHg) † | 66 (13) | 66 (13) | 67 (13) | 63 (11) | 67 (9) | 69 (16) | 62 (13) c |
| Variables | Total n = 70 | All Patients 1 n = 70 | Dippers 2 n = 41 | Non-Dippers 3 n = 29 | |||
|---|---|---|---|---|---|---|---|
| Morning-Time n = 34 | Bedtime n = 36 | Morning-Time n = 22 | Bedtime n = 19 | Morning-Time n = 12 | Bedtime n = 17 | ||
| FPG (mg/dL) † | 96 (21) | 95 (17) | 96 (26) | 95 (20) | 97 (26) | 97 (26) | 95 (23) |
| Creatinine (mg/dL) † | 0.83 (0.2) | 0.81 (0.2) | 0.89 (0.2) | 0.82 (0.3) | 0.88 (0.3) | 0.81 (0.1) | 0.86 (0.2) |
| eGFR (ml/min) † | 81 (20) | 85 (17) | 78 (23) | 86 (18) | 79 (19) | 84 (15) | 74 (25) |
| Uric acid (mg/dL) † | 4.9 (2.4) | 4.8 (2.6) | 5.0 (2.1) | 3.9 (2.1) | 5.3 (2.5) | 5.3 (2.2) | 4.8 (2.0) |
| Total proteins (g/dL) † | 7.3 (0.5) | 7.2 (0.6) | 7.3 (0.6) | 7.2 (0.5) | 7.3 (0.5) | 7.2 (0.8) | 7.2 (0.7) |
| TG (mg/dL) † | 88 (43) | 72 (33) | 101 (52) a | 74 (41) | 101 (68) c | 72 (19) | 96 (51) e |
| TC (mg/dL) † | 183 (47) | 180 (45) | 191 (49) | 180 (49) | 200 (64) | 178 (44) | 182 (35) |
| TBARS (nmol/mg Lp) † | 3.1 (1.6) | 3.8 (1.3) | 2.8 (1.0) b | 3.7 (1.6) | 2.6 (1.1) d | 4.1 (1.2) | 3.1 (1.0) f |
| Reduced thiols (mmol/L) † | 0.61 (0.1) | 0.63 (0.1) | 0.59 (0.1) | 0.63 (0.1) | 0.62 (0.1) | 0.62 (0.1) | 0.57 (0.1) |
| Variables | B | p-Value | Exp(B) | 95%CI | |
|---|---|---|---|---|---|
| Inferior | Superior | ||||
| Hypertensive patients a | |||||
| Age (years) | 0.083 | 0.004 | 1.087 | 1.027 | 1.151 |
| TBARS (nmol/mg Lp) | −1.077 | 0.001 | 0.341 | 0.180 | 0.645 |
| Patients with a dipper BP profile b | |||||
| Age (years) | 0.100 | 0.021 | 1.106 | 1.016 | 1.204 |
| TBARS (nmol/mg Lp) | −1.241 | 0.009 | 0.289 | 0.114 | 0.735 |
| Patients with a non-dipper BP profile c | |||||
| nDBP (mmHg) | −0.159 | 0.023 | 0.853 | 0.743 | 0.979 |
| TBARS (nmol/mg Lp) | −1.207 | 0.022 | 0.299 | 0.106 | 0.840 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vazquez-Agra, N.; Marques-Afonso, A.-T.; Cruces-Sande, A.; Mendez-Alvarez, E.; Soto-Otero, R.; Lopez-Paz, J.-E.; Pose-Reino, A.; Hermida-Ameijeiras, A. Assessment of Oxidative Stress Markers in Hypertensive Patients under the Use of Renin-Angiotensin-Aldosterone Blockers. Antioxidants 2023, 12, 802. https://doi.org/10.3390/antiox12040802
Vazquez-Agra N, Marques-Afonso A-T, Cruces-Sande A, Mendez-Alvarez E, Soto-Otero R, Lopez-Paz J-E, Pose-Reino A, Hermida-Ameijeiras A. Assessment of Oxidative Stress Markers in Hypertensive Patients under the Use of Renin-Angiotensin-Aldosterone Blockers. Antioxidants. 2023; 12(4):802. https://doi.org/10.3390/antiox12040802
Chicago/Turabian StyleVazquez-Agra, Nestor, Ana-Teresa Marques-Afonso, Anton Cruces-Sande, Estefania Mendez-Alvarez, Ramon Soto-Otero, Jose-Enrique Lopez-Paz, Antonio Pose-Reino, and Alvaro Hermida-Ameijeiras. 2023. "Assessment of Oxidative Stress Markers in Hypertensive Patients under the Use of Renin-Angiotensin-Aldosterone Blockers" Antioxidants 12, no. 4: 802. https://doi.org/10.3390/antiox12040802