
Vitamin D3 and COVID-19 Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses

 , ,
, ,
Abstract
:1. Introduction
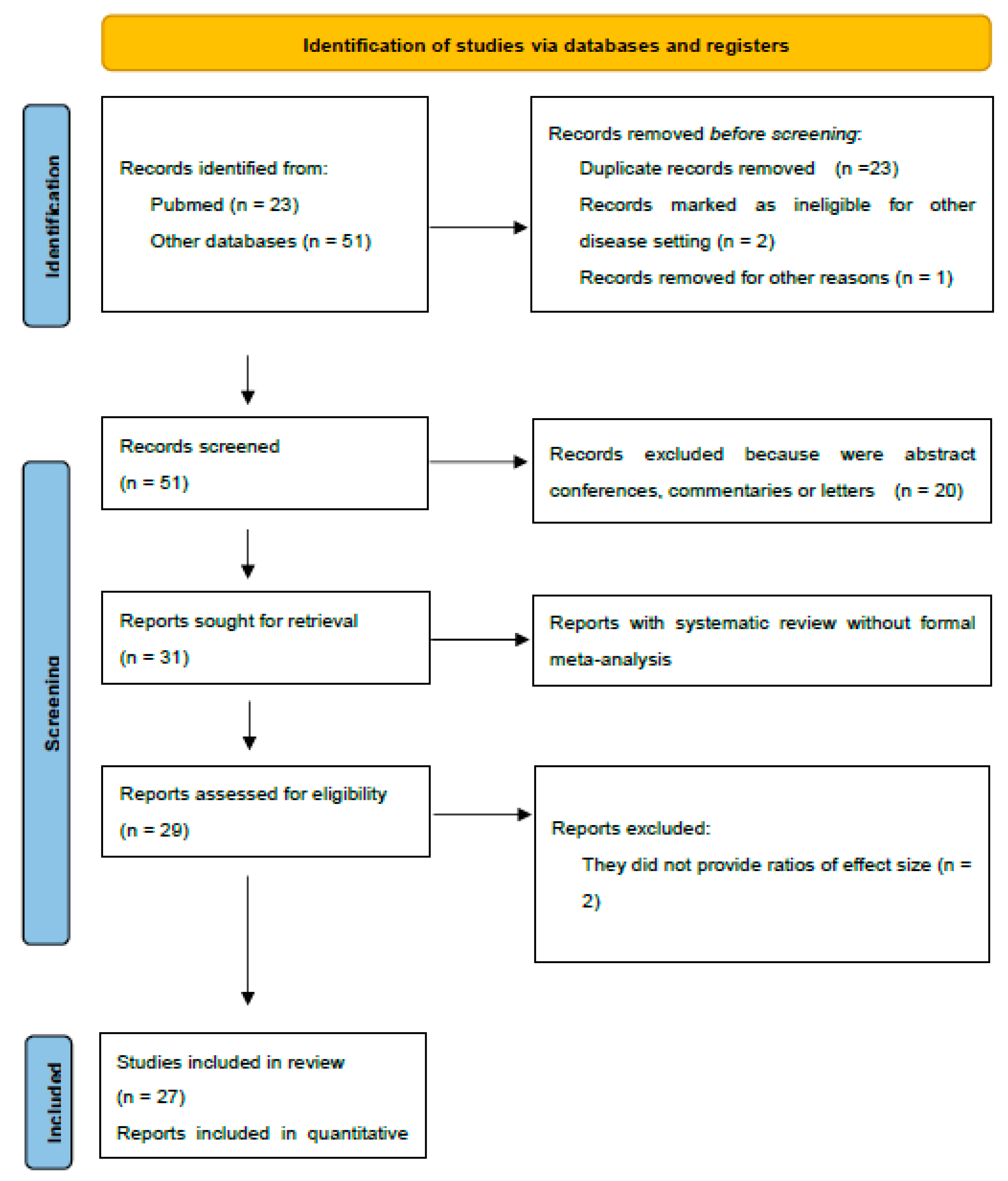
2. Material and Methods
2.1. Literature Search
2.2. Selection Criteria
2.3. Data Extraction
2.4. Assessment of Methodological Quality
2.5. Grading of the Evidence
2.6. Data Analysis
3. Results
4. Grading of Evidence
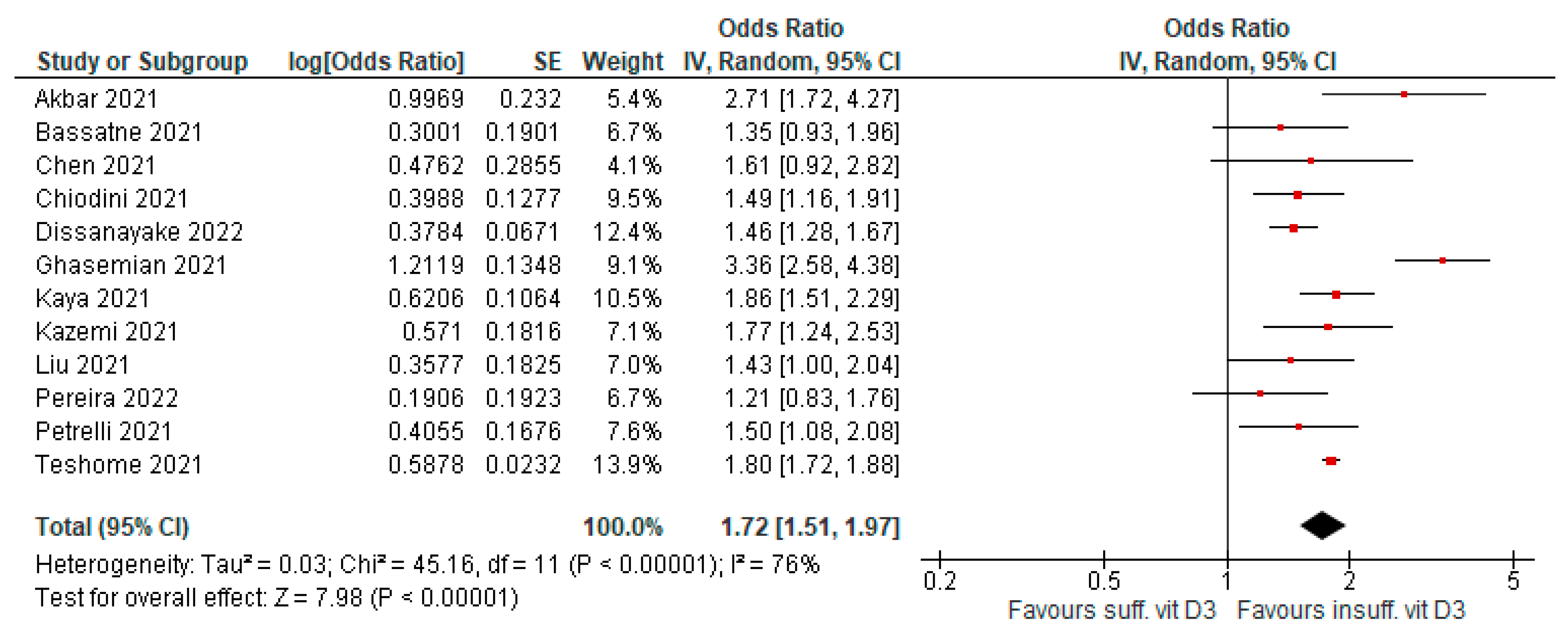
4.1. Susceptibility to Infection
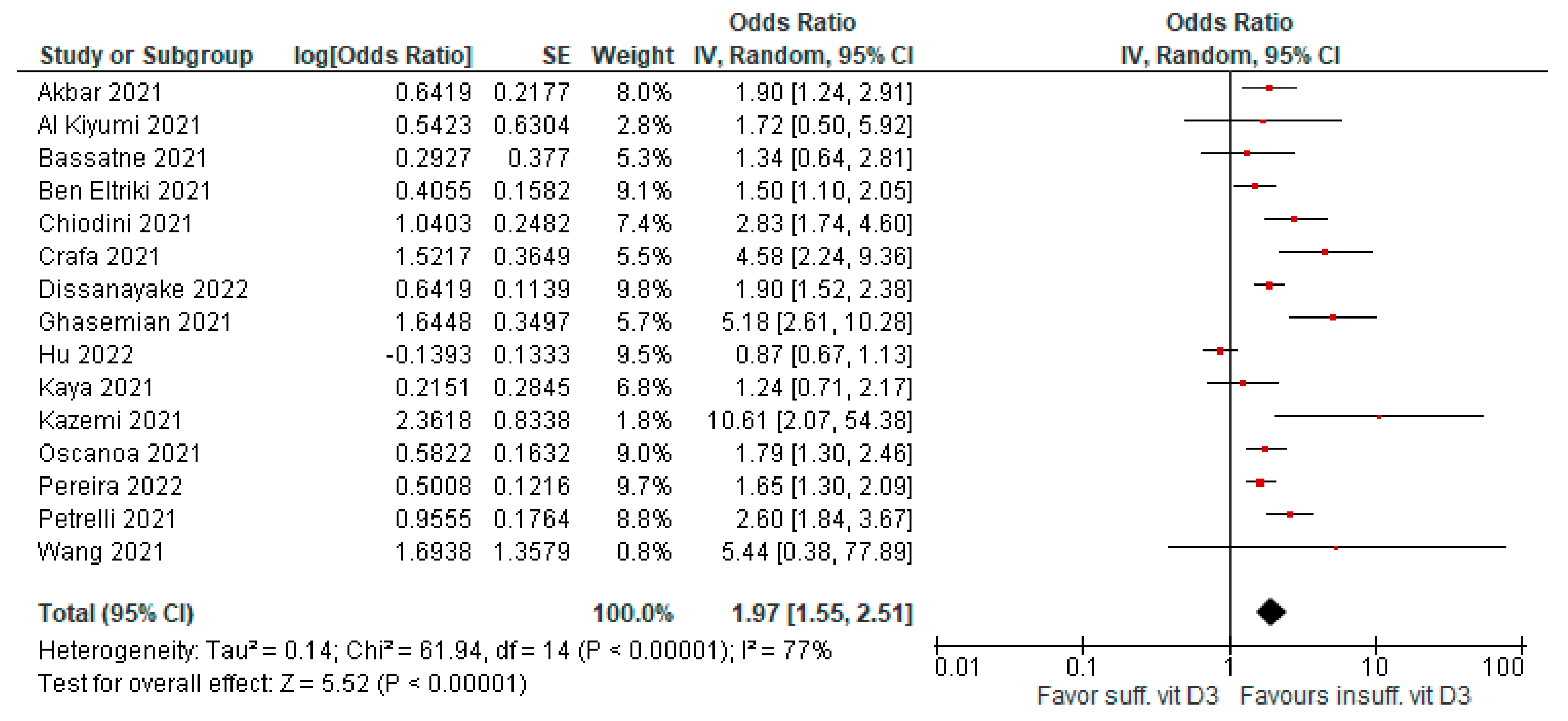
4.2. Risk of Severe Infection (ICU Admission)
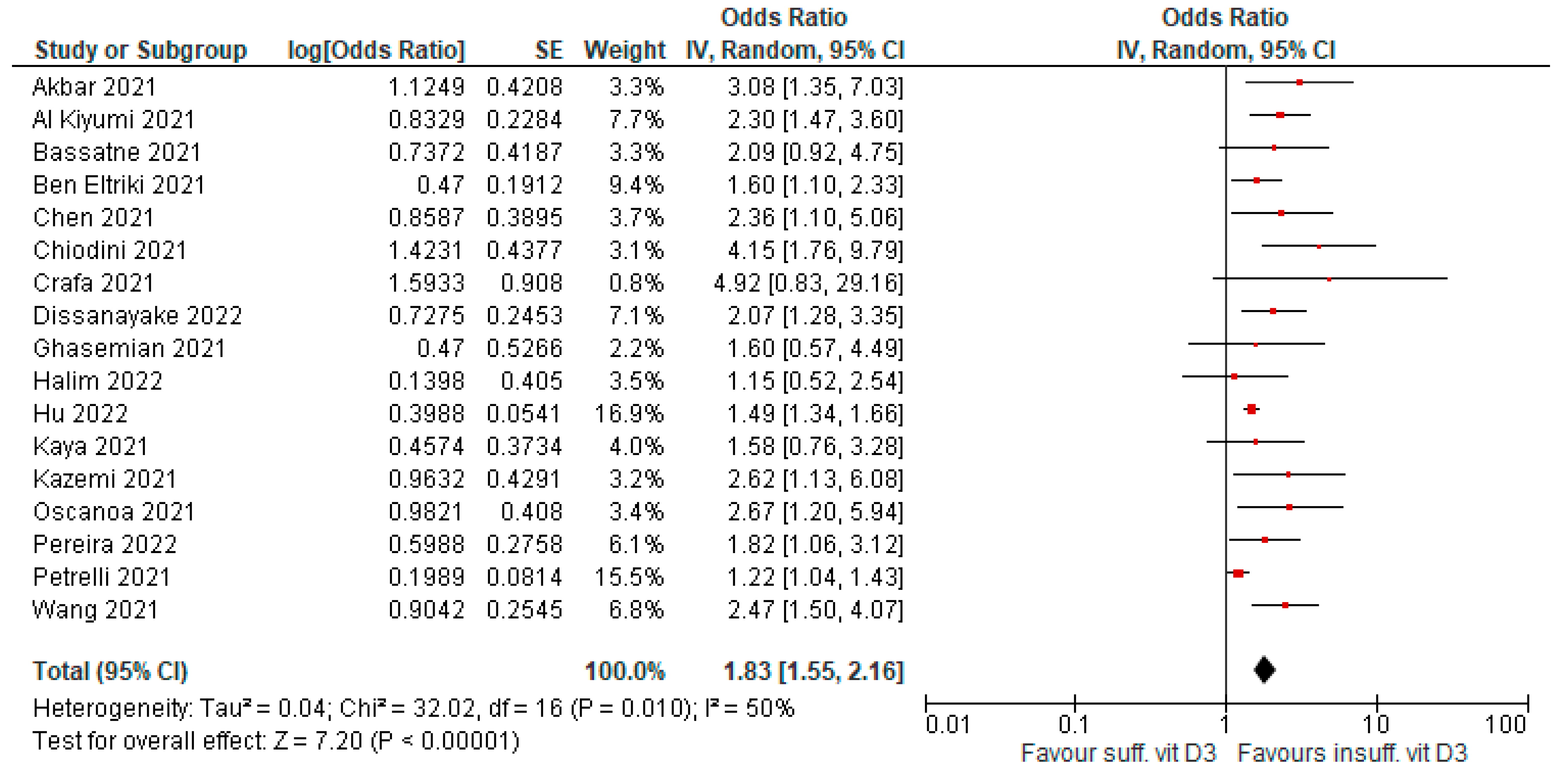
4.3. Risk of Death
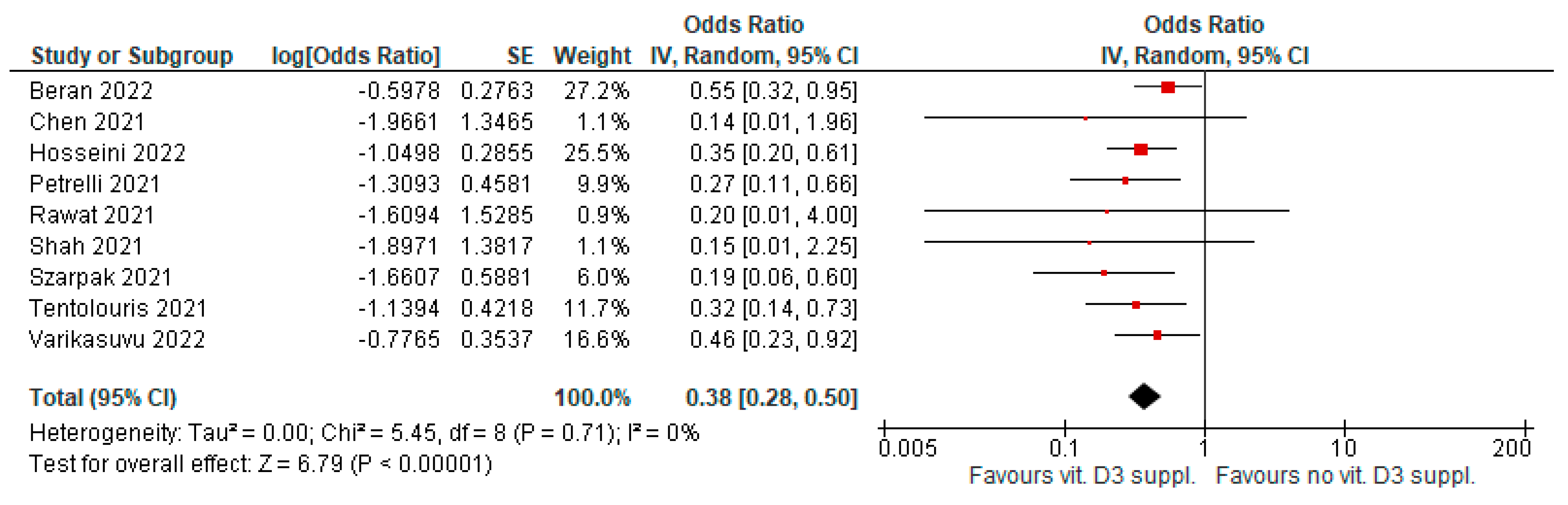
4.4. Supplementation to Improve Infection Severity
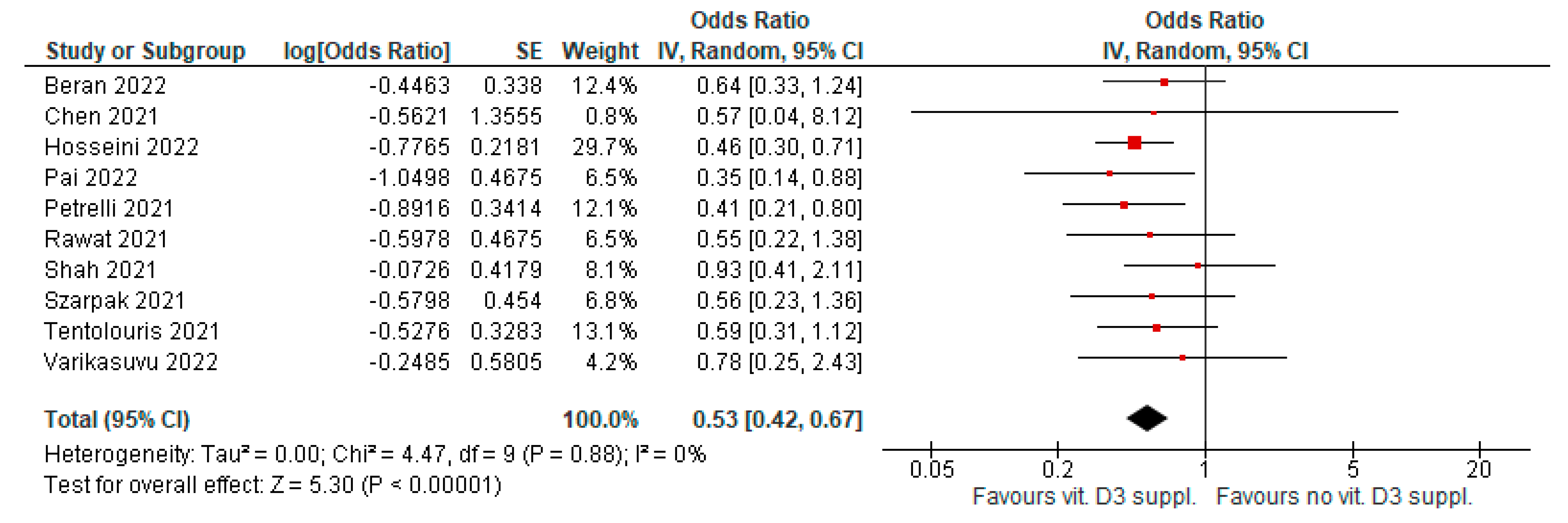
4.5. Supplementation to Improve Infection Mortality
4.6. Sensitivity Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Heath, A.K.; Kim, I.Y.; Hodge, A.M.; English, D.R.; Muller, D.C. Vitamin D Status and Mortality: A Systematic Review of Observational Studies. Int. J. Environ. Res. Public Health 2019, 16, 383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Fang, F.; Tang, J.; Jia, L.; Feng, Y.; Xu, P.; Faramand, A. Association between vitamin D supplementation and mortality: Systematic review and meta-analysis. BMJ 2019, 366, l4673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martineau, A.R.; Jolliffe, D.A.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; Goodall, E.C.; et al. Vitamin D supplementation to prevent acute respiratory infections: Individual participant data meta-analysis. Health Technol. Assess. 2019, 23, 1–44. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Theodoratou, E.; Tzoulaki, I.; Zgaga, L.; Ioannidis, J.P.A. Vitamin D and multiple health outcomes: Umbrella review of systematic reviews and meta-analyses of observational studies and randomised trials. BMJ 2014, 348, g2035. [Google Scholar] [CrossRef] [Green Version]
- Akbar, M.R.; Wibowo, A.; Pranata, R.; Setiabudiawan, B. Low Serum 25-hydroxyvitamin D (Vitamin D) Level Is Associated with Susceptibility to COVID-19, Severity, and Mortality: A Systematic Review and Meta-Analysis. Front. Nutr. 2021, 8, 660420. [Google Scholar] [CrossRef]
- Al Kiyumi, M.; Kalra, S.; Davies, J.; Kalhan, A. The impact of vitamin d deficiency on the severity of symptoms and mortality rate among adult patients with Covid-19: A systematic review and meta-analysis. Indian J. Endocrinol. Metab. 2021, 25, 261. [Google Scholar] [CrossRef]
- Kaya, M.O.; Pamukçu, E.; Yakar, B. The role of vitamin D deficiency on COVID-19: A systematic review and meta-analysis of observational studies. Epidemiology Health 2021, 43, e2021074. [Google Scholar] [CrossRef]
- Kazemi, A.; Mohammadi, V.; Aghababaee, S.K.; Golzarand, M.; Clark, C.C.T.; Babajafari, S. Association of Vitamin D Status with SARS-CoV-2 Infection or COVID-19 Severity: A Systematic Review and Meta-analysis. Adv. Nutr. Int. Rev. J. 2021, 12, 1636–1658. [Google Scholar] [CrossRef]
- Liu, N.; Sun, J.; Wang, X.; Zhang, T.; Zhao, M.; Li, H. Low vitamin D status is associated with coronavirus disease 2019 outcomes: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 104, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Oscanoa, T.J.; Amado, J.; Vidal, X.; Laird, E.; Ghashut, A.R.; Romero-Ortuno, R. The Relationship Between the Severity and Mortality of SARS-CoV-2 Infection and 25-hydroxyvitamin D Concentration—A Metaanalysis. Adv. Respir. Med. 2021, 89, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Dantas Damascena, A.D.; Galvão Azevedo, L.M.G.; de Almeida Oliveira, T.D.A.; da Mota Santana, J.D.M. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2022, 62, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Luciani, A.; Perego, G.; Dognini, G.; Colombelli, P.L.; Ghidini, A. Therapeutic and prognostic role of vitamin D for COVID-19 infection: A systematic review and meta-analysis of 43 observational studies. J. Steroid Biochem. Mol. Biol. 2021, 211, 105883. [Google Scholar] [CrossRef]
- Shah, K.; Saxena, D.; Mavalankar, D. Vitamin D supplementation, COVID-19 and disease severity: A meta-analysis. QJM Int. J. Med. 2021, 114, 175–181. [Google Scholar] [CrossRef]
- Szarpak, L.; Filipiak, K.J.; Gasecka, A.; Gawel, W.; Koziel, D.; Jaguszewski, M.J.; Chmielewski, J.; Gozhenko, A.; Bielski, K.; Wroblewski, P.; et al. Vitamin D supplementation to treat SARS-CoV-2 positive patients. Evidence from meta-analysis. Cardiol. J. 2022, 29, 188–196. [Google Scholar] [CrossRef]
- Tentolouris, N.; Samakidou, G.; Eleftheriadou, I.; Tentolouris, A.; Jude, E.B. The effect of vitamin D supplementation on mortality and intensive care unit admission of COVID-19 patients. A systematic review, meta-analysis and meta-regression. Diabetes/Metab. Res. Rev. 2022, 38, e3517. [Google Scholar] [CrossRef]
- Teshome, A.; Adane, A.; Girma, B.; Mekonnen, Z.A. The Impact of Vitamin D Level on COVID-19 Infection: Systematic Review and Meta-Analysis. Front. Public Health 2021, 9, 624559. [Google Scholar] [CrossRef]
- Ben-Eltriki, M.; Hopefl, R.; Wright, J.M.; Deb, S. Association between Vitamin D Status and Risk of Developing Severe COVID-19 Infection: A Meta-Analysis of Observational Studies. J. Am. Coll. Nutr. 2022, 41, 679–689. [Google Scholar] [CrossRef]
- Varikasuvu, S.R.; Thangappazham, B.; Vykunta, A.; Duggina, P.; Manne, M.; Raj, H.; Aloori, S. COVID-19 and vitamin D (Co-VIVID study): A systematic review and meta-analysis of randomized controlled trials. Expert Rev. Anti-infective Ther. 2022, 20, 907–913. [Google Scholar] [CrossRef]
- Wang, Z.; Joshi, A.; Leopold, K.; Jackson, S.; Christensen, S.; Nayfeh, T.; Mohammed, K.; Creo, A.; Tebben, P.; Kumar, S. Association of vitamin D deficiency with COVID-19 infection severity: Systematic review and meta-analysis. Clin. Endocrinol. 2021, 96, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Banerjee, M.; Bhadada, S.K.; Shetty, A.J.; Singh, B.; Vyas, A. Vitamin D supplementation and clinical outcomes in COVID-19: A systematic review and meta-analysis. J. Endocrinol. Investig. 2022, 45, 53–68. [Google Scholar] [CrossRef] [PubMed]
- Bassatne, A.; Basbous, M.; Chakhtoura, M.; El Zein, O.; Rahme, M.; Fuleihan, G.E.-H. The link between COVID-19 and VItamin D (VIVID): A systematic review and meta-analysis. Metabolism 2021, 119, 154753. [Google Scholar] [CrossRef] [PubMed]
- Dissanayake, H.A.; de Silva, N.L.; Sumanatilleke, M.; de Silva, S.D.N.; Gamage, K.K.K.; Dematapitiya, C.; Kuruppu, D.C.; Ranasinghe, P.; Pathmanathan, S.; Katulanda, P. Prognostic and Therapeutic Role of Vitamin D in COVID-19: Systematic Review and Meta-analysis. J. Clin. Endocrinol. Metab. 2021, 107, 1484–1502. [Google Scholar] [CrossRef]
- Rawat, D.; Roy, A.; Maitra, S.; Shankar, V.; Khanna, P.; Baidya, D.K. “Vitamin D supplementation and COVID-19 treatment: A systematic review and meta-analysis”. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102189. [Google Scholar] [CrossRef]
- Hosseini, B.; El Abd, A.; Ducharme, F.M. Effects of Vitamin D Supplementation on COVID-19 Related Outcomes: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2134. [Google Scholar] [CrossRef]
- Beran, A.; Mhanna, M.; Srour, O.; Ayesh, H.; Stewart, J.M.; Hjouj, M.; Khokher, W.; Mhanna, A.S.; Ghazaleh, D.; Khader, Y.; et al. Clinical significance of micronutrient supplements in patients with coronavirus disease 2019: A comprehensive systematic review and meta-analysis. Clin. Nutr. ESPEN 2022, 48, 167–177. [Google Scholar] [CrossRef]
- Chen, J.; Mei, K.; Xie, L.; Yuan, P.; Ma, J.; Yu, P.; Zhu, W.; Zheng, C.; Liu, X. Low vitamin D levels do not aggravate COVID-19 risk or death, and vitamin D supplementation does not improve outcomes in hospitalized patients with COVID-19: A meta-analysis and GRADE assessment of cohort studies and RCTs. Nutr. J. 2021, 20, 89. [Google Scholar] [CrossRef]
- Chiodini, I.; Gatti, D.; Soranna, D.; Merlotti, D.; Mingiano, C.; Fassio, A.; Adami, G.; Falchetti, A.; Eller-Vainicher, C.; Rossini, M.; et al. Vitamin D Status and SARS-CoV-2 Infection and COVID-19 Clinical Outcomes. Front. Public Health 2021, 9, 736665. [Google Scholar] [CrossRef]
- Crafa, A.; Cannarella, R.; Condorelli, R.A.; Mongioì, L.M.; Barbagallo, F.; Aversa, A.; La Vignera, S.; Calogero, A.E. Influence of 25-hydroxy-cholecalciferol levels on SARS-CoV-2 infection and COVID-19 severity: A systematic review and meta-analysis. Eclinicalmedicine 2021, 37, 100967. [Google Scholar] [CrossRef]
- Ghasemian, R.; Shamshirian, A.; Heydari, K.; Malekan, M.; Alizadeh-Navaei, R.; Ebrahimzadeh, M.A.; Warkiani, M.E.; Jafarpour, H.; Bazaz, S.R.; Shahmirzadi, A.R.; et al. The role of vitamin D in the age of COVID-19: A systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e14675. [Google Scholar] [CrossRef] [PubMed]
- Halim, C.; Mirza, A.F.; Sari, M.I. The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 195. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Kung, J.; Cave, A.; Banh, H.L. Effects of Vitamin D Serum Level on Morbidity and Mortality in Patients with COVID-19: A Systematic Review and Meta-Analysis. J. Pharm. Pharm. Sci. 2022, 25, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocr. Rev. 2018, 40, 1109–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopefl, R.; Ben-Eltriki, M.; Deb, S. Association Between Vitamin D Levels and Inflammatory Markers in COVID-19 Patients: A Meta-Analysis of Observational Studies. J. Pharm. Pharm. Sci. 2022, 25, 124–136. [Google Scholar] [CrossRef]
- Zdrenghea, M.T.; Makrinioti, H.; Bagacean, C.; Bush, A.; Johnston, S.L.; Stanciu, L.A. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev. Med. Virol. 2017, 27, e1909. [Google Scholar] [CrossRef]
- Arboleda, J.F.; Urcuqui-Inchima, S. Vitamin D Supplementation: A Potential Approach for Coronavirus/COVID-19 Therapeutics? Front. Immunol. 2020, 11, 1523. [Google Scholar] [CrossRef]
- Ahmed, F. A Network-Based Analysis Reveals the Mechanism Underlying Vitamin D in Suppressing Cytokine Storm and Virus in SARS-CoV-2 Infection. Front. Immunol. 2020, 11, 590459. [Google Scholar] [CrossRef]
- Wang, T.-T.; Dabbas, B.; Laperriere, D.; Bitton, A.J.; Soualhine, H.; Tavera-Mendoza, L.E.; Dionne, S.; Servant, M.J.; Bitton, A.; Seidman, E.G.; et al. Direct and Indirect Induction by 1,25-Dihydroxyvitamin D3 of the NOD2/CARD15-Defensin β2 Innate Immune Pathway Defective in Crohn Disease. J. Biol. Chem. 2010, 285, 2227–2231. [Google Scholar] [CrossRef] [Green Version]
- Bacchetta, J.; Zaritsky, J.J.; Sea, J.L.; Chun, R.; Lisse, T.S.; Zavala, K.; Nayak, A.; Wesseling-Perry, K.; Westerman, M.; Hollis, B.W.; et al. Suppression of Iron-Regulatory Hepcidin by Vitamin D. J. Am. Soc. Nephrol. 2014, 25, 564–572. [Google Scholar] [CrossRef]
- Kong, J.; Zhang, Z.; Musch, M.W.; Ning, G.; Sun, J.; Hart, J.; Bissonnette, M.; Li, Y.C. Novel role of the vitamin D receptor in maintaining the integrity of the intestinal mucosal barrier. Am. J. Physiol. Gastrointest. Liver Physiol. 2008, 294, G208–G216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.-Y.; Liu, T.-J.; Fu, J.-H.; Xu, W.; Wu, L.-L.; Hou, A.-N.; Xue, X.-D. Vitamin D/VDR signaling attenuates lipopolysaccharide-induced acute lung injury by maintaining the integrity of the pulmonary epithelial barrier. Mol. Med. Rep. 2016, 13, 1186–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gough, M.E.; Graviss, E.A.; May, E.E. The dynamic immunomodulatory effects of vitamin D3 during Mycobacterium infection. Innate Immun. 2017, 23, 506–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramanian, K.; Bergman, P.; Henriques-Normark, B. Vitamin D Promotes Pneumococcal Killing and Modulates Inflammatory Responses in Primary Human Neutrophils. J. Innate Immun. 2017, 9, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Mushegian, A.A. Autophagy and vitamin D. Sci. Signal. 2017, 10, eaan2526. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Siman-Tov, G.; Hall, G.; Bhalla, N.; Narayanan, A. Human Antimicrobial Peptides as Therapeutics for Viral Infections. Viruses 2019, 11, 704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, J.; Lin, E.; He, L.; Yu, J.; Tan, P.; Zhou, Y. Autophagy and Viral Infection. Adv. Exp. Med. Biol. 2019, 1209, 55–78. [Google Scholar] [CrossRef] [PubMed]
- van Etten, E.; Mathieu, C. Immunoregulation by 1,25-dihydroxyvitamin D3: Basic concepts. J. Steroid Biochem. Mol. Biol. 2005, 97, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Daniel, C.; Sartory, N.A.; Zahn, N.; Radeke, H.H.; Stein, J.M. Immune Modulatory Treatment of Trinitrobenzene Sulfonic Acid Colitis with Calcitriol Is Associated with a Change of a T Helper (Th) 1/Th17 to a Th2 and Regulatory T Cell Profile. J. Pharmacol. Exp. Ther. 2008, 324, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Laplana, M.; Royo, J.L.; Fibla, J. Vitamin D Receptor polymorphisms and risk of enveloped virus infection: A meta-analysis. Gene 2018, 678, 384–394. [Google Scholar] [CrossRef]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Deng, W.; et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus–induced lung injury. Nat. Med. 2005, 11, 875–879. [Google Scholar] [CrossRef] [PubMed]
- Imai, Y.; Kuba, K.; Rao, S.; Huan, Y.; Guo, F.; Guan, B.; Yang, P.; Sarao, R.; Wada, T.; Leong-Poi, H.; et al. Angiotensin-converting enzyme 2 protects from severe acute lung failure. Nature 2005, 436, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Asperen, R.M.W.-V.; Lutter, R.; Specht, P.A.; Moll, G.N.; Van Woensel, J.B.; Van Der Loos, C.M.; Van Goor, H.; Kamilic, J.; Florquin, S.; Bos, A.P. Acute respiratory distress syndrome leads to reduced ratio of ACE/ACE2 activities and is prevented by angiotensin-(1-7) or an angiotensin II receptor antagonist. J. Pathol. 2011, 225, 618–627. [Google Scholar] [CrossRef]
- Grace, J.A.; Klein, S.; Herath, C.B.; Granzow, M.; Schierwagen, R.; Masing, N.; Walther, T.; Sauerbruch, T.; Burrell, L.M.; Angus, P.W.; et al. Activation of the Mas Receptor by Angiotensin-(1–7) in the Renin–Angiotensin System Mediates Mesenteric Vasodilatation in Cirrhosis. Gastroenterology 2013, 145, 874–884.e5. [Google Scholar] [CrossRef]
- Xu, J.; Yang, J.; Chen, J.; Luo, Q.; Zhang, Q.; Zhang, H. Vitamin D alleviates lipopolysaccharide-induced acute lung injury via regulation of the renin-angiotensin system. Mol. Med. Rep. 2017, 16, 7432–7438. [Google Scholar] [CrossRef] [Green Version]
- Bilezikian, J.P.; Bikle, D.; Hewison, M.; Lazaretti-Castro, M.; Formenti, A.M.; Gupta, A.; Madhavan, M.V.; Nair, N.; Babalyan, V.; Hutchings, N.; et al. Mechanisms in Endocrinology: Vitamin D and COVID-19. Eur. J. Endocrinol. 2020, 183, R133–R147. [Google Scholar] [CrossRef]
- Song, Y.; Qayyum, S.; Greer, R.A.; Slominski, R.M.; Raman, C.; Slominski, A.T.; Song, Y. Vitamin D3 and its hydroxyderivatives as promising drugs against COVID-19: A computational study. J. Biomol. Struct. Dyn. 2022, 40, 11594–11610. [Google Scholar] [CrossRef]
- Ulivieri, F.M.; Banfi, G.; Camozzi, V.; Colao, A.; Formenti, A.M.; Frara, S.; Lombardi, G.; Napoli, N.; Giustina, A. Vitamin D in the Covid-19 era: A review with recommendations from a G.I.O.S.E.G. expert panel. Endocrine 2021, 72, 597–603. [Google Scholar] [CrossRef]
- Albergamo, A.; Apprato, G.; Silvagno, F. The Role of Vitamin D in Supporting Health in the COVID-19 Era. Int. J. Mol. Sci. 2022, 23, 3621. [Google Scholar] [CrossRef]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.C.; Silva, C.B.R.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.H.; et al. Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients with Moderate to Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. Med. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginde, A.A.; Blatchford, P.; Breese, K.; Zarrabi, L.; Linnebur, S.A.; Wallace, J.I.; Schwartz, R.S. High-Dose Monthly Vitamin D for Prevention of Acute Respiratory Infection in Older Long-Term Care Residents: A Randomized Clinical Trial. J. Am. Geriatr. Soc. 2017, 65, 496–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guidelines. Available online: https://www.nice.org.uk/guidance/ng187 (accessed on 15 June 2022).
- Balla, M.; Merugu, G.P.; Konala, V.M.; Sangani, V.; Kondakindi, H.; Pokal, M.; Gayam, V.; Adapa, S.; Naramala, S.; Malayala, S.V. Back to basics: Review on vitamin D and respiratory viral infections including COVID-19. J. Community Hosp. Intern. Med. Perspect. 2020, 10, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Maghbooli, Z.; Sahraian, M.A.; Ebrahimi, M.; Pazoki, M.; Kafan, S.; Tabriz, H.M.; Hadadi, A.; Montazeri, M.; Nasiri, M.; Shirvani, A.; et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS ONE 2020, 15, e0239799. [Google Scholar] [CrossRef] [PubMed]
- Murai, I.H.; Fernandes, A.L.; Antonangelo, L.; Gualano, B.; Pereira, R.M.R. Effect of a Single High-Dose Vitamin D3 on the Length of Hospital Stay of Severely 25-Hydroxyvitamin D-Deficient Patients with COVID-19. Clinics 2021, 76, e3549. [Google Scholar] [CrossRef] [PubMed]
- Slominski, R.M.; Stefan, J.; Athar, M.; Holick, M.F.; Jetten, A.M.; Raman, C.; Slominski, A.T. COVID-19 and Vitamin D: A lesson from the skin. Exp. Dermatol. 2020, 29, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Qayyum, S.; Slominski, R.M.; Raman, C.; Slominski, A.T. Novel CYP11A1-Derived Vitamin D and Lumisterol Biometabolites for the Management of COVID-19. Nutrients 2022, 14, 4779. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/ Year | N° Studies/ N° pts | Type of Studies | Time of Search | Vitamina D3 Cutoff (ng/mL) | Vitamin D3 Dose/Timing | Outcome Evaluated | Severity Definition | Type of Metric/ Type of Analysis | Small Study Effect (p Egger Test) | Overall Quality Assessment (AMSTAR2) |
|---|---|---|---|---|---|---|---|---|---|---|
| Akbar/2021 | 14/999,179 | 9 Retrosp observational | Up to 9 December 2020 | 20–30 | - | - Risk of infection and VitD levels | Criteria for severe CAP (ICU, MV) | OR/- | Severity (p 0.047) Mortality (p 0.046) | Moderate |
| 2 Prosp Observational | - Risk of severity and VitD levels | |||||||||
| 2 Cross-Sect | - Risk of death and VitD levels | |||||||||
| 1 Observational study | ||||||||||
| Al Kiyumi/2021 | 43/254,963 | 18 Retrosp | Until 20 December 2020 | 20 | - | - Prevalence of VDD/VDI in patients with COVID-19 | ARDS, severe radiology, ICU admission, O2 therapy, ventilator support | OR/MVA | Severity (p 0.071) Mortality (p 0.023) | Moderate |
| 11 Cross-Sect | - Severity of COVID-19 | |||||||||
| 8 Prosp | - Case-fatality rate | |||||||||
| 3 Case-control | ||||||||||
| 1 Observational study | ||||||||||
| 1 pilot study | ||||||||||
| 1 Case series | ||||||||||
| Bassatne/2021 | 31/8209 | 15 Cross-Sect | Until 20 January 2021 | 20 | 357 to 60,000 IU die/from one week to 12 months | Association of low serum 25(OH)D with COVID-19 related health outcomes: | - | RR/- | Not performed | High |
| 11 Cohort | - Mortality | |||||||||
| 4 Case-control | - ICU admission | |||||||||
| - Invasive ventilation | ||||||||||
| - Non-invasive ventilation | ||||||||||
| - Hospitalization | ||||||||||
| - Length of hospital stay | ||||||||||
| - Disease severity | ||||||||||
| - ARDS | ||||||||||
| Serum 25(OH)D levels in COVID-19 infected patients compared to those not infected | ||||||||||
| Ben-Eltriki/ 2021 | 24/3637 | 7 Retrosp observational | Up to 30 March 2021 | 30 | - | - All-cause mortality | Total number of severe cases, hospital duration, MV | RR/- | Not reported | Critically low |
| 6 Prosp cohort | - COVID-19 severity | |||||||||
| 3 Cross-Sect | - Difference in biological markers and disease severity | |||||||||
| 2 Retrosp | ||||||||||
| 2 Prosp observational | ||||||||||
| 2 Cohort | ||||||||||
| 2 Case-control | ||||||||||
| Beran/2022 | 14/3497 | 4 Retrosp cohort | Through 5 December 2021 | - | Various | -Risk of mortality | - | RR/- | (p 0.047) | High |
| 4 RCT | - Intubation rate | |||||||||
| 3 Non-RCT | ||||||||||
| 2 Cross-Sect | ||||||||||
| 1 Case-control | ||||||||||
| Chen/2021 | 13/536,338 | 10 Retrosp cohort | Up to 5 June 2021 | 20–30 | Various | - Effect of low VitD level on COVID-19 | ICU admission | OR/MVA | Not performed | Moderate |
| 2 RCT | - Effect of VitD supplements on ICU admission or death | |||||||||
| 1 Prosp C | ||||||||||
| Chiodini/ 2021 | 54/ 1,403,715 | 37 Retrosp | Until 31 March 2021 | 25 | - | - VitD status as a predictor of in-hospital COVID-19 severity | ICU admission | OR/- | Severity (p 0.816) Mortality (p 0.110) | Moderate |
| 17 Prosp | - VitD and SARS-CoV-2 infection or COVID-19 related hospitalization | |||||||||
| Crafa/2021 | 29/380,172 | 11 Retrosp | Up to January 2021 | 20 | - | - 25(OH)D levels in patients SARS-CoV-2 pos or neg | Severe pneumonia, ICU, severe radiology or combo | OR/- | Not reported | Moderate |
| 6 Prosp | - 25(OH)D levels in patients with severe or non-severe COVID-19 | |||||||||
| 5 Case-control | - 25(OH)D levels in COVID-19 patients who died compared to those discharged | |||||||||
| 3 Observational study | - Risk of severe COVID-19 in patients with VitD deficiency | |||||||||
| 1 pilot study | - Mortality risk in patients with VitD deficiency | |||||||||
| 1 Cohort | ||||||||||
| 1 Cross-Sect | ||||||||||
| 1 Popul-based | ||||||||||
| Dissanayake/ 2022 | 72/ 1,975,551 | 28 Retrosp cohort | - | Various | - | - Susceptibility to infection | Hospitalization, hypoxia (O2, non/invasive ventilation, ARDS or combo), death or composite | OR/- | (p 0.0001) | Moderate |
| 26 Case-control | - Risk of developing severe COVID-19 | |||||||||
| 17 Prosp cohort | - Mortality | |||||||||
| - VitD in the treatment of COVID-19 | ||||||||||
| Ghasemian/ 2021 | 23/11,901 | 9 Retrosp cohort | Up to 18 December 2020 | 20–30 | - | - Frequency of VitD status in | - | OR/- | Severity (p 0.14) Mortality (p 0.62) | Critically low |
| 5 Case-control | COVID-19 patients | |||||||||
| 4 Cross-Sect | - Mean serum 25(OH)D concentration | |||||||||
| 4 Prosp cohort | - VitD deficiency and SARS-CoV-2 infection | |||||||||
| 1 RCT | - VitD deficiency and COVID-19 severity | |||||||||
| - VitD deficiency and | ||||||||||
| COVID-19 mortality | ||||||||||
| Halim/2022 | 11/1424 | 4 Retrosp cohort | Up to the year 2021 | 20 | - | - VitD and COVID-19 severity | Various | OR/- | Not reported | Critically low |
| 4 Cohort | - VitD and COVID-19 mortality | |||||||||
| 3 Cross-Sect | ||||||||||
| Hosseini/2022 | 23/ 5,870,189 | 9 RCT | Up until January 2022 | 25 | Various | - Risk of COVID-19 infection (primary prevention | - | RR/- | Risk of bias detected in some studies | High |
| 6 Retrosp cohort | studies on uninfected individuals) | |||||||||
| 4 Prosp cohort | - Hospital admission (secondary prevention studies on mild COVID-19 cases) | |||||||||
| 3 Retrosp | - ICU admission and mortality rate (tertiary prevention studies on hospitalized | |||||||||
| 1 Case-control | COVID-19 patients) | |||||||||
| Hu/2022 | 20/12,806 | 6 Retrosp | On 1 May 2021 | 25 | - | - Effect of VitD serum concentration on mortality | ICU admission, ventilator support, length of hospital stay | RR/- | High risk | Low |
| 4 Retrosp observational | - Effect of VitD serum concentration on ICU admission | |||||||||
| 4 Prosp observational | - Effect of VitD serum concentration on ventilator support requirement | |||||||||
| 2 Retrosp cohort | - Length of hospital stay | |||||||||
| 2 Cross-Sect | ||||||||||
| 1 Prosp | ||||||||||
| 1 Prosp cohort | ||||||||||
| Kaya/2021 | 21/205,869 | 11 Case-control | Between 1 January and 15 December 2020 | 20 | - | - VitD and COVID-19 infection | - | OR/- | Severity (p 0.064) Mortality (p 0.911) | Low |
| 9 Cohort | - VitD and COVID-19 severity | |||||||||
| 6 Cross-Sect | - VitD and COVID-19 mortality | |||||||||
| Kazemi/2021 | 39/13,333 | 11 Case-control | Up to 26 November 2020 | Various | - | - Association of 25(OH)D status with SARS-CoV-2 infection | Various | OR/- | (p 0.002) | High |
| 9 Cross-Sect | - Association of VitD status with COVID-19 severity | |||||||||
| 6 Retrosp cohort | - Composite severity | |||||||||
| 4 Retrosp observational | - ICU admission or stay | |||||||||
| 3 Retrosp | - Pulmonary complications | |||||||||
| 3 Prosp | - Hospitalization | |||||||||
| 3 Descriptive | - Concentration of 25(OH)D between severe and less | |||||||||
| 3 Cohort | - severe status of disease | |||||||||
| 2 Prosp cohort | - Inflammatory markers | |||||||||
| 2 Quasi-exp | - Mortality | |||||||||
| 2 RCT | ||||||||||
| Liu/2021 | 10/361,934 | 10 Case-control | To 25 September 2020 | Various | - | - Association between | - | OR/- | (p 0.001; p 0.009) | Moderate |
| VitD deficiency or insufficiency and COVID-19 infection | ||||||||||
| - VitD levels in COVID-19-positive and-negative participants | ||||||||||
| Oscanoa/2021 | 23/2692 | 11 Case-control | Between December 2019 and December 2020 | Various | - | - Mortality and severity | ICU admission, ARDS and/or need for MV | RR/- | Not reported | Critically low |
| 5 Cross-Sect | - proportions in COVID-19 patients with 25(OH)D deficiency | |||||||||
| 5 Cohort | ||||||||||
| 2 Observational study | ||||||||||
| Pai/2022 | 13/2933 | 10 Observational study | Until 8 June 2021 | Various | Various | - ICU admission and/or mortality in COVID-19 patients receiving VitD supplementation | - | OR/- | Risk of bias detected in some studies | High |
| 3 RCT | ||||||||||
| Pereira/2022 | 25/8176 | 9 Cohort | Up to 9 October 2020 | 50 | - | - Prevalence of VitD deficiency in severe cases of COVID-19 | - | OR/- | Risk of bias detected in some studies | Critically low |
| 7 Retrosp | ||||||||||
| 6 Cross-Sect | ||||||||||
| 1 Prosp cohort | ||||||||||
| 1 Popul-based | ||||||||||
| 1 Case series | ||||||||||
| Petrelli/2021 | 43/612,601 | 24 Retrosp | Until 31 January 2021 | 15–30 | Various | - Association between VitD and risk, severity, and mortality for COVID-19 infection | Various | OR/MVA | (p 0.04) | Critically low |
| 7 Prosp | ||||||||||
| 4 Case-control | ||||||||||
| 2 Prosp cohort | ||||||||||
| 2 Cross-Sect | ||||||||||
| 1 Observational | ||||||||||
| 1 Registry data | ||||||||||
| 1 Popul-based | ||||||||||
| 1 RCT | ||||||||||
| Rawat/2021 | 5/467 | 3 RCT | Until 18 May 2021 | - | Various | - Mortality | ICU admission, MV | RR/- | Risk of bias detected in some studies | Critically low |
| 2 Quasi-Exp | - Mechanical ventilation | |||||||||
| - Admission to ICU | ||||||||||
| - Acute markers | ||||||||||
| Shah/2021 | 3/532 | 2 RCT | Between December 2019 and 17 December 2020 | - | Various | - ICU admission | ICU admission, need for MV, mortality | OR/MVA | Severity (p 0.253) Mortality (p 0.138) | Critically low |
| 1 Retrosp case-control | - Death | |||||||||
| - Hospital length of stay | ||||||||||
| - Mechanical ventilation requirement | ||||||||||
| - Serum level of VitD and | ||||||||||
| - biomarkers | ||||||||||
| Szarpak/2022 | 8/2322 | 3 Observational | Until 10 July 2021 | - | Various | - Primary end points were 14-day and in-hospital mortality. | - | OR/- | Risk of bias detected in some studies | Critically low |
| 1 Retrosp cohort | - Secondary end points were ICU admission, need of mechanical ventilation, | |||||||||
| 1 Retrosp case-control | - radiological improvement and secondary infection incidence | |||||||||
| 1 Quasi-exp | ||||||||||
| 1 Pilot study random | ||||||||||
| 1 RCT | ||||||||||
| Tentolouris/ 2021 | 9/278 | 2 Cohort | On 26 March 2021 | - | Various | - Mortality | Various | OR/- | Severity (p 0.011) Mortality (p 0.676) | Moderate |
| 1 RCT | - ICU admissions | |||||||||
| 1 pilot study random | ||||||||||
| 1 Quasi-exp | ||||||||||
| 1 Prosp observ. study | ||||||||||
| 1 Prosp cross-Sect | ||||||||||
| 1 Case-control | ||||||||||
| 1 Retrosp cross-Sect | ||||||||||
| 1 Retrosp | ||||||||||
| Teshome/ 2021 | 14/91,120 | 5 Cohort | From 15 May 2020 to 20 December 2020 | - | - | - Risk of developing COVID-19 infection among VDD and normal VitD levels | - | OR/- | (p 0.764) * | Critically low |
| 5 Case-control | ||||||||||
| 3 Cross-Sect | ||||||||||
| 1 Interim audit | ||||||||||
| Varikasuvu/ 2022 | 6/551 | 6 RCT | To 5 August 2021 | - | Various | - Severity | - | RR/- | (p 0.14) | Moderate |
| - ICU care | ||||||||||
| - Mortality | ||||||||||
| - Seropositivity | ||||||||||
| - RT-PCR positivity | ||||||||||
| Wang/2021 | 17/2756 | 17 Observational | From 1 January 2019 to 3 December 2020 | 12–25 | - | - Mortality | Mortality, hospital admission, lenght of hospital stay | OR/- | High risk | Critically low |
| - Hospital admission | ||||||||||
| - Length of hospital stay | ||||||||||
| - ICU admission |
| Endpoint | Author/Year | N° Studies | Effect Size (95% CI) | Heterogenity (I2, p) | Overall Effect |
|---|---|---|---|---|---|
| COVID-19 infection | Akbar/2021 | 6 | OR = 2.71 [1.72, 4.29] | 92.6%, 0.001 | OR = 1.72 (95% CI 1.51–1.97) p < 0.01; I2 = 76%, p for heterogeneity < 0.01 Highly suggestive association |
| Bassatne/2021 | 3 | RR = 1.35 (0.93–1.96) | 76%, 0.11 | ||
| Chen/2021 | 3 | RR = 1.61 (0.92–1.8) | 92%, 0.09 | ||
| Chiodini/2021 | 7 | OR = 1.49 (1.16–1.91) | 79%, 0.1 | ||
| Dissanayake/2022 | 19 | OR = 1.46 (1.28–1.65) | 92%, <0.001 | ||
| Gasemian/2021 | 3 | OR = 3.36 (2.58–4.37) | NR | ||
| Kaya/2021 | 8 | OR = 1.64 (1.32–2.04) | 85%, <0.01 | ||
| Kazemi/2021 | 3 | OR = 1.77 (1.24–2.53) | 44%, 0.16 | ||
| Liu/2021 | 4 | OR = 1.43 (1–2.05) | 64%, 0.03 | ||
| Pereira/2022 | 4 | OR = 1.21 (0.83–1.6) | 78%, 0.003 | ||
| Petrelli/2021 | 7 | OR = 1.5 (1.08–2.08) | 95%, <0.001 | ||
| Teshome/2021 | 8 | OR = 1.8 (1.72–1.88) | 71%, <0.001 | ||
| Severe COVID-19 infection | Akbar/2021 | 5 | OR = 1.90 [1.24, 2.93] | 64.2%, 0.02 | OR = 1.97 (95% CI 1.55–2.51) p < 0.01; I2 = 77%, p for heterogeneity < 0.01 Highly suggestive association |
| Al Kiyumi/2021 | 5 | OR = 3.38 (1.94–5.87) | 67%, <0.01 | ||
| Bassatne/2021 | 7 | RR = 1.34 (0.64–2.79) | 0, 0.43 | ||
| Ben Eltriki/2021 | 12 | RR = 1.5 (1.1–2.05) | 92%, 0.01 | ||
| Chiodini/2021 | 10 | OR = 2.83 (1.74–4.6) | 84%, 0.94 | ||
| Crafa/2021 | 8 | OR = 4.58 (2.24–9.36) | 81%, 0.001 | ||
| Dissanayake/2022 | 36 | OR = 1.9 (1.52–2.38) | 81%, <0.001 | ||
| Gasemian/2021 | 13 | OR = 5.18 (2.61–10.31) | NR | ||
| Hu/2022 | 3 | RR = 0.87 (0.67–1.14) | 0, 0.31 | ||
| Kaya/2021 | 9 | OR = 1.24 (0.71–2.17) | 92%, <0.01 | ||
| Kazemi/2021 | 6 | OR = 10.61 (2.07–54.38) | 90, <0.01 | ||
| Oscanoa/2021 | 4 | RR = 1.79 (1.3–2.46) | 81%, <0.001 | ||
| Pereira/2022 | 10 | OR = 1.65 (1.3–2.09) | 35%, 0.12 | ||
| Petrelli/2021 | 17 | OR = 2.6 (1.84–3.67) | 87%, <0.001 | ||
| Wang/2021 | 4 | OR = 5.44 (0.38–78.42) | 83%, NR | ||
| COVID-19 mortality | Akbar/2021 | 8 | OR = 3.08 [1.35, 7.00] | 80.3%, 0.001 | OR = 1.83 (95% CI 1.55–2.16) p < 0.01; I2 = 50%, p for heterogeneity = 0.01 Highly suggestive association |
| Al Kiyumi/2021 | 4 | OR = 2.3 [1.47–3.6] | 0, 0.07 | ||
| Bassatne/2021 | 7 | RR = 2.09 (0.92–4.77) | 76%, 0.08 | ||
| Ben Eltriki/2021 | 18 | RR = 1.6 (1.1–2.32) | 68%, 0.01 | ||
| Chen/2021 | 4 | RR = 2.36 (1.1–5.06) | 0%, 0.71 | ||
| Chiodini/2021 | 19 | OR = 4.15 (1.76–9.79) | 44%, 0.33 | ||
| Crafa/2021 | 9 | OR = 4.92 (0.83–29.31) | 94%, <0.001 | ||
| Dissanayake/2022 | 20 | OR = 2.07 (1.28–3.35) | 73%, 0.003 | ||
| Gasemian/2021 | 7 | OR = 1.6 (0.57–4.45) | NR | ||
| Halim/2022 | 5 | OR = 1.15 (0.52–2.49) | 66%, 0.34 | ||
| Hu/2022 | 20 | RR = 1.49 (1.34–1.66) | 83%, 0.88 | ||
| Kaya/2021 | 5 | OR = 1.58 (0.76–3.28) | 83%, <0.01 | ||
| Kazemi/2021 | 8 | OR = 2.62 (1.13–6.08) | 83%, <0.001 | ||
| Oscanoa/2021 | 4 | RR = 2.67 (1.2–5.94) | 83%, <0.001 | ||
| Pereira/2022 | 5 | OR = 1.82 (1.06–2.58) | 59%, 0.04 | ||
| Petrelli/2021 | 19 | OR = 1.22 (1.04–1.43) | 74%, 0.01 | ||
| Wang/2021 | 12 | OR = 2.47 (1.5–4.05) | 30%, NR | ||
| Effect of supplementation of vitamin D3 on COVID-19 infection severity | Beran/2022 | 6 | RR = 0.55 (0.32–0.97) | 48%, 0.04 | OR = 0.38 (95% CI 0.28–0.5) p < 0.01; I2 = 0%, p for heterogeneity = 0.71 Highly suggestive association |
| Chen/2021 | 2 | OR = 0.14 (0–4.9) | 90%, 0.28 | ||
| Hosseini/2022 | 7 | RR = 0.35 (0.20–0.62) | 75%, <0.001 | ||
| Petrelli/2021 | 6 | OR = 0.27 (0.11–0.66) | 49%, 0.004 | ||
| Rawat/2021 | 2 | RR= 0.2 (0.01–4.26) | 89%, 0.3 | ||
| Shah/2021 | 3 | OR = 0.15 (0.01–1.45) | 82%, NR | ||
| Szarpak/2021 | 5 | OR = 0.19 (0.06–0.54) | 77%, 0.002 | ||
| Tentolouris/2021 | 6 | OR = 0.32 (0.14–0.71) | 60%, 0.028 | ||
| Varikasuvu/2022 | 6 | RR = 0.46 (0.23–0.93) | 52%, 0.06 | ||
| Effect of supplementation of vitamin D3 on COVID-19 infection mortality | Beran/2022 | 9 | RR = 0.64 (0.33–1.27) | 77%, 0.25 | OR = 0.53 (95% CI 0.42–0.67) p < 0.01: I2 = 0%, p for heterogeneity = 0.88 Highly suggestive association |
| Chen/2021 | 2 | OR = 0.57 (0.04–7.78) | 64%, 0.67 | ||
| Hosseini/2022 | 11 | RR = 0.46 (0.30–0.7) | 54%, <0.001 | ||
| Pai/2022 | 7 * | OR = 0.35 (0.14–0.85) | 67%, 0.03 | ||
| Petrelli/2021 | 7 | OR = 0.41 (0.21–0.81) | 72%, 0.01 | ||
| Rawat/2021 | 4 | RR= 0.55 (0.22–1.39) | 58%, 0.21 | ||
| Shah/2021 | 3 | OR = 0.93 (0.41–2.11) | 21%, 0.27 | ||
| Szarpak/2021 | 7 | OR = 0.56 (0.23–1.37) | 74%, 0.2 | ||
| Tentolouris/2021 | 9 | OR = 0.59 (0.31–1.12) | 62%, 0.006 | ||
| Varikasuvu/2022 | 4 | RR = 0.78 (0.25–2.4) | 48%, 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrelli, F.; Oldani, S.; Borgonovo, K.; Cabiddu, M.; Dognini, G.; Ghilardi, M.; Parati, M.C.; Petro’, D.; Dottorini, L.; Rea, C.; et al. Vitamin D3 and COVID-19 Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Antioxidants 2023, 12, 247. https://doi.org/10.3390/antiox12020247
Petrelli F, Oldani S, Borgonovo K, Cabiddu M, Dognini G, Ghilardi M, Parati MC, Petro’ D, Dottorini L, Rea C, et al. Vitamin D3 and COVID-19 Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Antioxidants. 2023; 12(2):247. https://doi.org/10.3390/antiox12020247
Chicago/Turabian StylePetrelli, Fausto, Simone Oldani, Karen Borgonovo, Mary Cabiddu, Giuseppina Dognini, Mara Ghilardi, Maria Chiara Parati, Daniela Petro’, Lorenzo Dottorini, Carmen Rea, and et al. 2023. "Vitamin D3 and COVID-19 Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses" Antioxidants 12, no. 2: 247. https://doi.org/10.3390/antiox12020247