
The Burden of Impaired Serum Albumin Antioxidant Properties and Glyco-Oxidation in Coronary Heart Disease Patients with and without Type 2 Diabetes Mellitus


 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
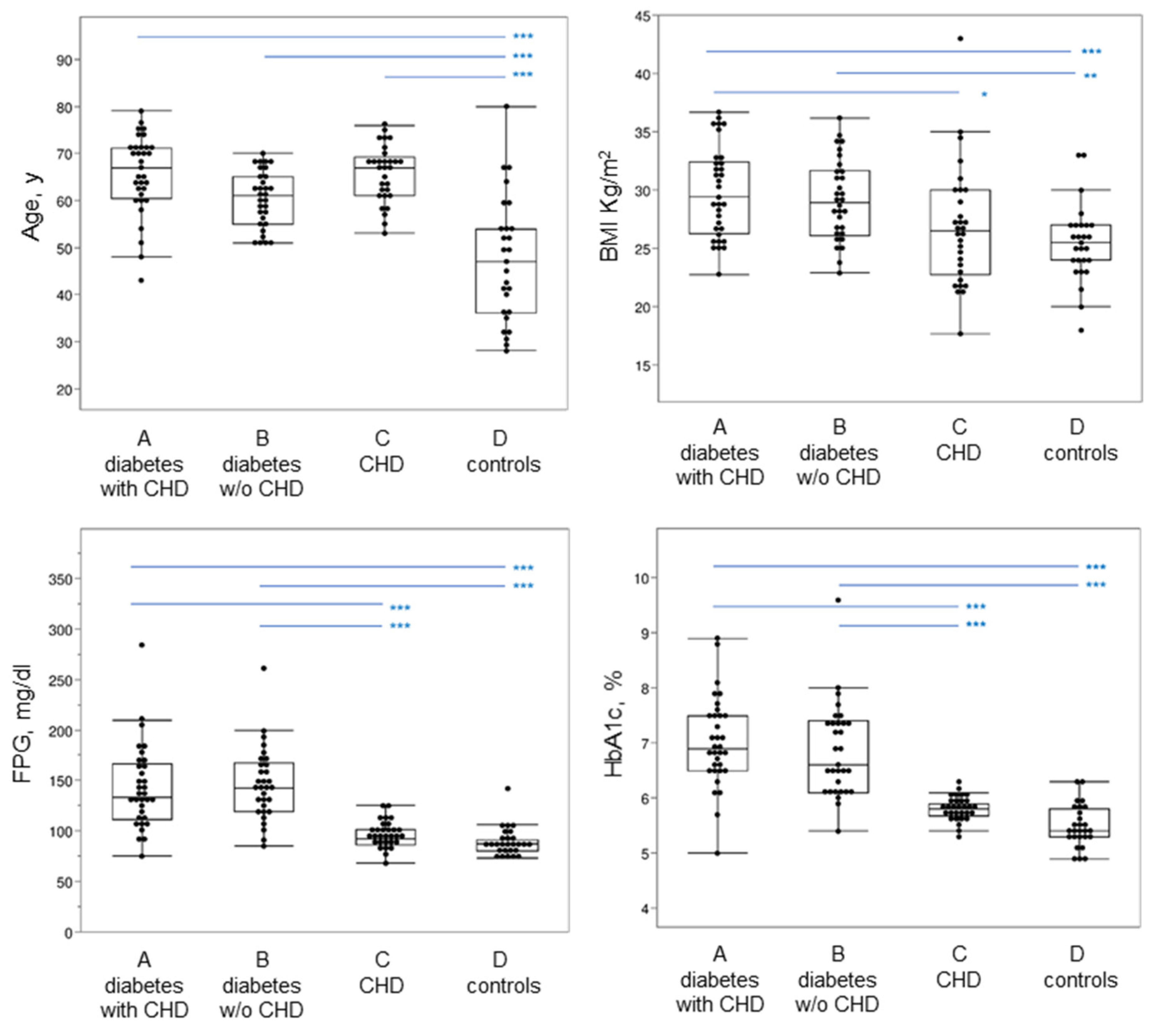
2.1. Patients Recruitment and Clinical Parameters
2.2. Immunoassays
2.3. Albumin Analysis by Mass Spectrometry
2.4. Regeneration of Mercaptoalbumin (HSA-SH)
2.5. Albumin Cysteinylation
2.6. Cell Treatment with Albumin Isoforms
2.7. Real-Time Quantitative Reverse Transcriptase PCR
2.8. TRAP Assay
2.9. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: A systematic literature review of scientific evidence from across the world in 2007-2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [Green Version]
- Lotfy, M.; Adeghate, J.; Kalasz, H.; Singh, J.; Adeghate, E. Chronic Complications of Diabetes Mellitus: A Mini Review. Curr. Diabetes Rev. 2017, 13, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Piarulli, F.; Sartore, G.; Lapolla, A. Glyco-oxidation and cardiovascular complications in type 2 diabetes: A clinical update. Acta Diabetol. 2013, 50, 101–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapolla, A.; Fedele, D.; Traldi, P. Glyco-oxidation in diabetes and related diseases. Clin. Chim. Acta 2005, 357, 236–250. [Google Scholar] [CrossRef] [PubMed]
- Lapolla, A.; Piarulli, F.; Sartore, G.; Ceriello, A.; Ragazzi, E.; Reitano, R.; Baccarin, L.; Laverda, B.; Fedele, B. Advanced Glycation End Products and Antioxidant Status in Type 2 Diabetic Patients with and without Peripheral Artery Disease. Diabetes Care 2007, 30, 670–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrone, A.; Giovino, A.; Benny, J.; Martinelli, F. Advanced Glycation End Products (AGEs): Biochemistry, Signaling, Analytical Methods, and Epigenetic Effects. Oxid. Med. Cell. Longev. 2020, 2020, 3818196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basta, G. Receptor for advanced glycation endproducts and atherosclerosis: From basic mechanisms to clinical implications. Atherosclerosis 2008, 196, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Coughlan, M.T.; Thorburn, D.R.; Penfold, S.A.; Laskowski, A.; Harcourt, B.E.; Sourris, K.C.; Tan, A.L.; Fukami, K.; Thallas-Bonke, V.; Nawroth, P.P.; et al. RAGE-induced cytosolic ROS promote mitochondrial superoxide generation in diabetes. J. Am. Soc. Nephrol. 2009, 20, 742–752. [Google Scholar] [CrossRef] [Green Version]
- Fishman, S.L.; Sonmez, H.; Basman, C.; Singh, V.; Poretsky, L. The role of advanced glycation end-products in the development of coronary artery disease in patients with and without diabetes mellitus: A review. Mol. Med. 2018, 24, 59. [Google Scholar] [CrossRef] [PubMed]
- Falcone, C.; Emanuele, E.; D’Angelo, A.; Buzzi, M.P.; Belvito, C.; Cuccia, M.; Geroldi, D. Plasma levels of soluble receptor for advanced glycation end products and coronary artery disease in nondiabetic men. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1032–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, K.; Yamagishi, S.; Adachi, H.; Kurita-Nakamura, Y.; Matsui, T.; Yoshida, T.; Sato, A.; Imaizumi, T. Elevation of soluble form of receptor for advanced glycation end products (sRAGE) in diabetic subjects with coronary artery disease. Diabetes Metab. Res. Rev. 2007, 23, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Chien, S.C.; Chen, C.Y.; Lin, C.F.; Yeh, H.I. Critical appraisal of the role of serum albumin in cardiovascular disease. Biomark. Res. 2017, 5, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, G.; Clerici, M.; Giustarini, D.; Rossi, R.; Milzani, A.; Dalle-Donne, I. Redox albuminomics: Oxidized albumin in human diseases. Antioxid. Redox Signal. 2012, 17, 1515–1527. [Google Scholar] [CrossRef] [PubMed]
- Roche, M.; Rondeau, P.; Singh, N.R.; Tarnus, E.; Bourdon, E. The antioxidant properties of serum albumin. FEBS Lett. 2008, 582, 1783–1787. [Google Scholar] [CrossRef] [PubMed]
- Brioschi, M.; Gianazza, E.; Mallia, A.; Zoanni, B.; Altomare, A.; Martinez Fernandez, A.; Agostoni, P.; Aldini, G.; Banfi, C. S-Thiolation Targets Albumin in Heart Failure. Antioxidants 2020, 9, 763. [Google Scholar] [CrossRef] [PubMed]
- Perna, A.F.; Satta, E.; Acanfora, F.; Lombardi, C.; Ingrosso, D.; de Santo, N.G. Increased plasma protein homocysteinylation in hemodialysis patients. Kidney Int. 2006, 69, 869–876. [Google Scholar] [CrossRef] [Green Version]
- D’Aronco, S.; Crotti, S.; Agostini, M.; Traldi, P.; Chilelli, N.C.; Lapolla, A. The role of mass spectrometry in studies of glycation processes and diabetes management. Mass Spectrom. Rev. 2019, 38, 112–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapolla, A.; Fedele, D.; Seraglia, R.; Catinella, S.; Baldo, L.; Aronica, R.; Traldi, P. A new effective method for the evaluation of glycated intact plasma proteins in diabetic subjects. Diabetologia 1995, 38, 1076–1081. [Google Scholar] [CrossRef] [PubMed]
- Martinez Fernandez, A.; Regazzoni, L.; Brioschi, M.; Gianazza, E.; Agostoni, P.; Aldini, G.; Banfi, C. Pro-oxidant and pro-inflammatory effects of glycated albumin on cardiomyocytes. Free Radic. Biol. Med. 2019, 144, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Li, G.Y.; Li, H.Y.; Li, Q. Use of glycated albumin for the identification of diabetes in subjects from northeast China. World J. Diabetes 2021, 12, 149–157. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes, A. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef] [PubMed]
- Giglio, R.V.; Lo Sasso, B.; Agnello, L.; Bivona, G.; Maniscalco, R.; Ligi, D.; Mannello, F.; Ciaccio, M. Recent Updates and Advances in the Use of Glycated Albumin for the Diagnosis and Monitoring of Diabetes and Renal, Cerebro-and Cardio-Metabolic Diseases. J. Clin. Med. 2020, 9, 3634. [Google Scholar] [CrossRef]
- Huggett, A.S.; Nixon, D.A. Use of glucose oxidase, peroxidase, and O-dianisidine in determination of blood and urinary glucose. Lancet 1957, 273, 368–370. [Google Scholar] [CrossRef]
- Mosca, A.; Paleari, R.; Dalfra, M.G.; Di Cianni, G.; Cuccuru, I.; Pellegrini, G.; Malloggi, L.; Bonomo, M.; Granata, S.; Ceriotti, F.; et al. Reference intervals for hemoglobin A1c in pregnant women: Data from an Italian multicenter study. Clin. Chem. 2006, 52, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Dastych, M.; Wiewiorka, O.; Benovska, M. Ethamsylate (Dicynone) interference in determination of serum creatinine, uric acid, triglycerides, and cholesterol in assays involving the Trinder reaction; in vivo and in vitro. Clin. Lab. 2014, 60, 1373–1376. [Google Scholar] [CrossRef] [PubMed]
- Goh, S.Y.; Cooper, M.E. Clinical review: The role of advanced glycation end products in progression and complications of diabetes. J. Clin. Endocrinol. Metab. 2008, 93, 1143–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altomare, A.; Baron, G.; Brioschi, M.; Longoni, M.; Butti, R.; Valvassori, E.; Tremoli, E.; Carini, M.; Agostoni, P.; Vistoli, G.; et al. N-Acetyl-Cysteine Regenerates Albumin Cys34 by a Thiol-Disulfide Breaking Mechanism: An Explanation of Its Extracellular Antioxidant Activity. Antioxidants 2020, 9, 367. [Google Scholar] [CrossRef] [PubMed]
- Banfi, C.; Brioschi, M.; Barcella, S.; Pignieri, A.; Parolari, A.; Biglioli, P.; Tremoli, E.; Mussoni, L. Tissue factor induction by protease-activated receptor 1 requires intact caveolin-enriched membrane microdomains in human endothelial cells. J. Thromb. Haemost. 2007, 5, 2437–2444. [Google Scholar] [CrossRef] [PubMed]
- Burke, A.P.; Kolodgie, F.D.; Zieske, A.; Fowler, D.R.; Weber, D.K.; Varghese, P.J.; Farb, A.; Virmani, R. Morphologic findings of coronary atherosclerotic plaques in diabetics: A postmortem study. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1266–1271. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J.; Baek, J.Y.; Shin, W.S.; Kim, D.B.; Jang, S.W.; Shin, D.I.; Koh, Y.S.; Seo, S.M.; Uhm, J.S.; Kim, T.H.; et al. Soluble receptor of advanced glycated endproducts is associated with plaque vulnerability in patients with acute myocardial infarction. Circ. J. 2011, 75, 1685–1690. [Google Scholar] [CrossRef] [Green Version]
- Prasad, K. AGE-RAGE Stress and Coronary Artery Disease. Int. J. Angiol. 2021, 30, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Roohk, H.V.; Zaidi, A.R.; Patel, D. Glycated albumin (GA) and inflammation: Role of GA as a potential marker of inflammation. Inflamm. Res. 2018, 67, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, F.; Shibata, T.; Kamiya, K.; Yoshitake, J.; Kikuchi, R.; Matsushita, T.; Ishii, I.; Giménez-Bastida, J.A.; Schneider, C.; Uchida, K. Structural and functional insights into S-thiolation of human serum albumins. Sci. Rep. 2018, 8, 932. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
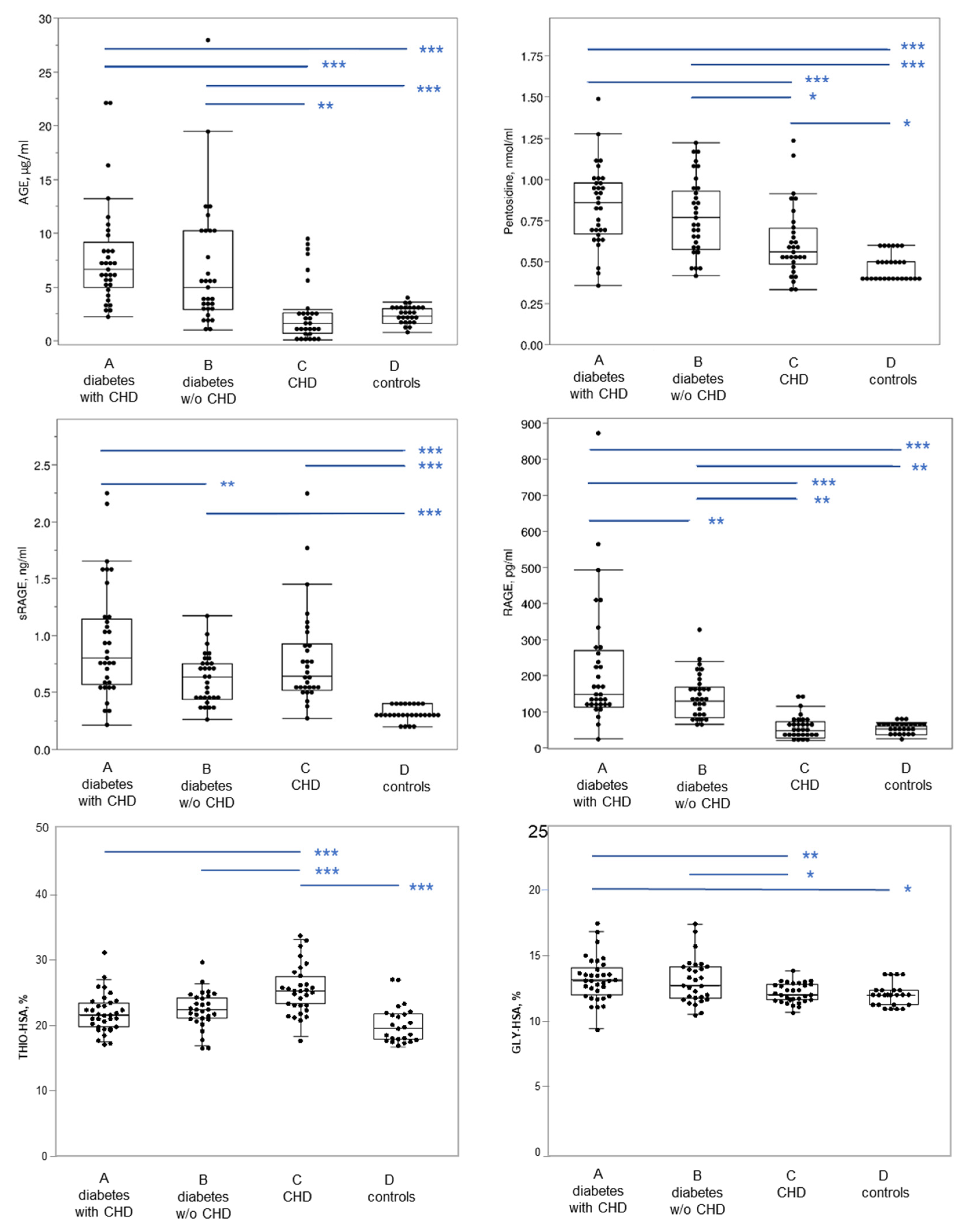
| Parameter | A: Diabetics with CHD (n = 33) | B: Diabetics without CHD (n = 31) | C: Non-diabetics with CHD (n = 30) | D: Controls (n = 27) |
|---|---|---|---|---|
| AGE (µg/mL) | 7.8 ± 4.8 a | 6.7 ± 5.8 a | 2.6 ± 2.8 b | 2.3 ± 0.8 b |
| Pentosidine (nmol/mL) | 0.84 ± 0.24 a | 0.78 ± 0.23 a | 0.62 ± 0.22 b | 0.47 ± 0.08 c |
| sRAGE (ng/mL) | 0.95 ± 0.50 a | 0.62 ± 0.22 b | 0.79 ± 0.42 ab | 0.31 ± 0.07 c |
| RAGE (pg/mL) | 217 ± 171 a | 140 ± 61 b | 54 ± 33 c | 51 ± 13 c |
| GLY-HSA (%) | 13.2 ± 1.6 a | 13.1 ± 1.7 a | 12.1 ± 0.7 b | 12.02 ± 0.9 b |
| THIO-HSA (%) | 21.8 ± 2.9 a | 22.4 ± 2.9 a | 25.3 ± 3.7 b | 20.98 ± 3.4 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piarulli, F.; Banfi, C.; Brioschi, M.; Altomare, A.; Ragazzi, E.; Cosma, C.; Sartore, G.; Lapolla, A. The Burden of Impaired Serum Albumin Antioxidant Properties and Glyco-Oxidation in Coronary Heart Disease Patients with and without Type 2 Diabetes Mellitus. Antioxidants 2022, 11, 1501. https://doi.org/10.3390/antiox11081501
Piarulli F, Banfi C, Brioschi M, Altomare A, Ragazzi E, Cosma C, Sartore G, Lapolla A. The Burden of Impaired Serum Albumin Antioxidant Properties and Glyco-Oxidation in Coronary Heart Disease Patients with and without Type 2 Diabetes Mellitus. Antioxidants. 2022; 11(8):1501. https://doi.org/10.3390/antiox11081501
Chicago/Turabian StylePiarulli, Francesco, Cristina Banfi, Maura Brioschi, Alessandra Altomare, Eugenio Ragazzi, Chiara Cosma, Giovanni Sartore, and Annunziata Lapolla. 2022. "The Burden of Impaired Serum Albumin Antioxidant Properties and Glyco-Oxidation in Coronary Heart Disease Patients with and without Type 2 Diabetes Mellitus" Antioxidants 11, no. 8: 1501. https://doi.org/10.3390/antiox11081501