
Walnut Intake Interventions Targeting Biomarkers of Metabolic Syndrome and Inflammation in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
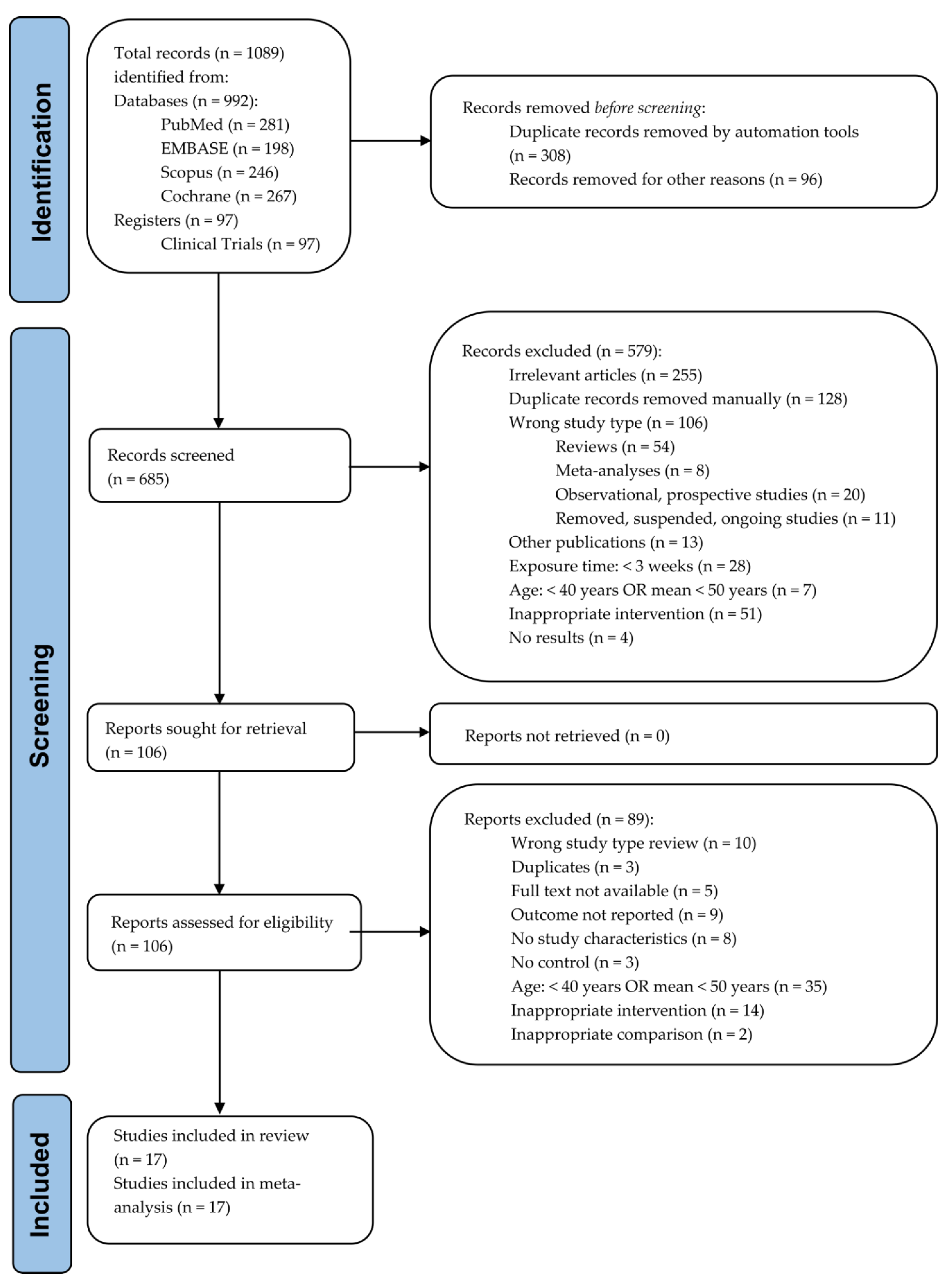
2.4. Selection Process
2.5. Data Items
2.6. Study Risk of Bias Assessment
2.7. Effect Measures
2.8. Synthesis Methods
2.9. Quality Assessment
2.10. Reporting Bias Assessment
3. Results
3.1. Metabolic Syndrome Biomarkers
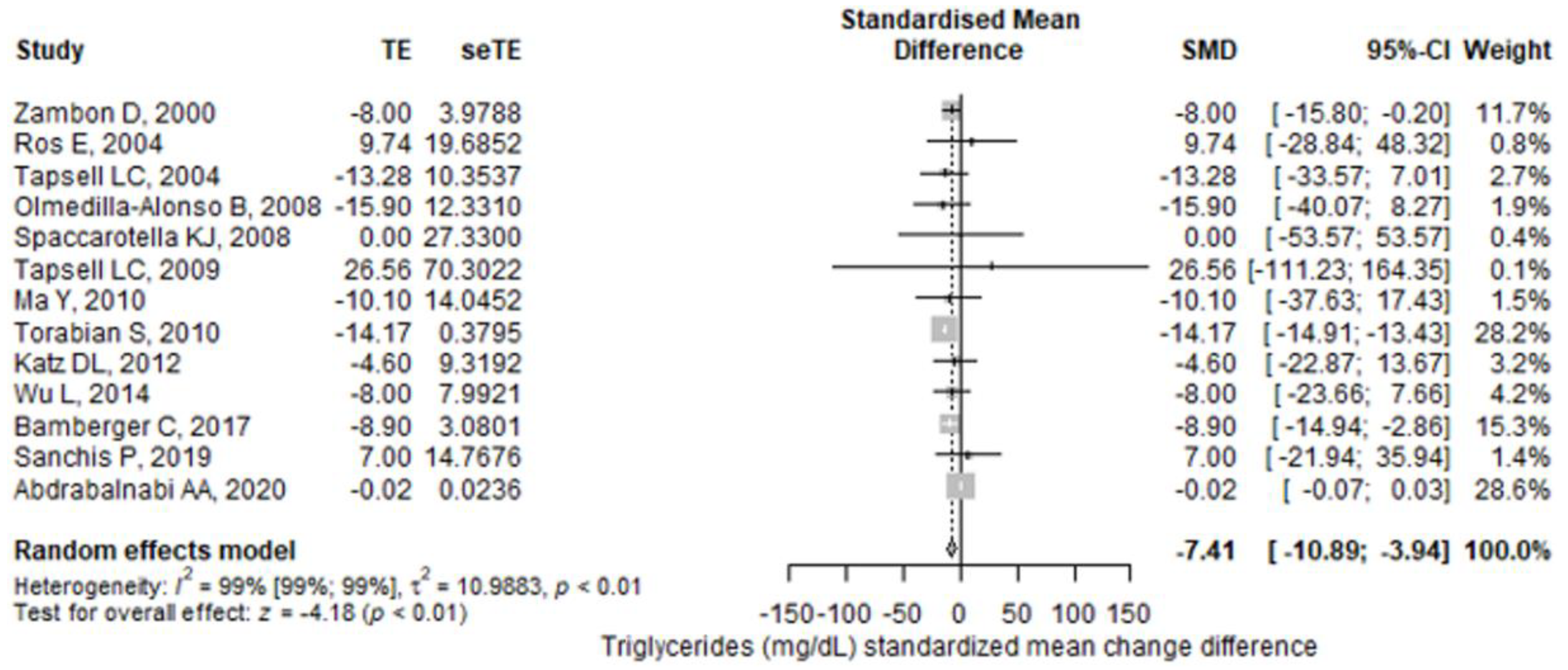
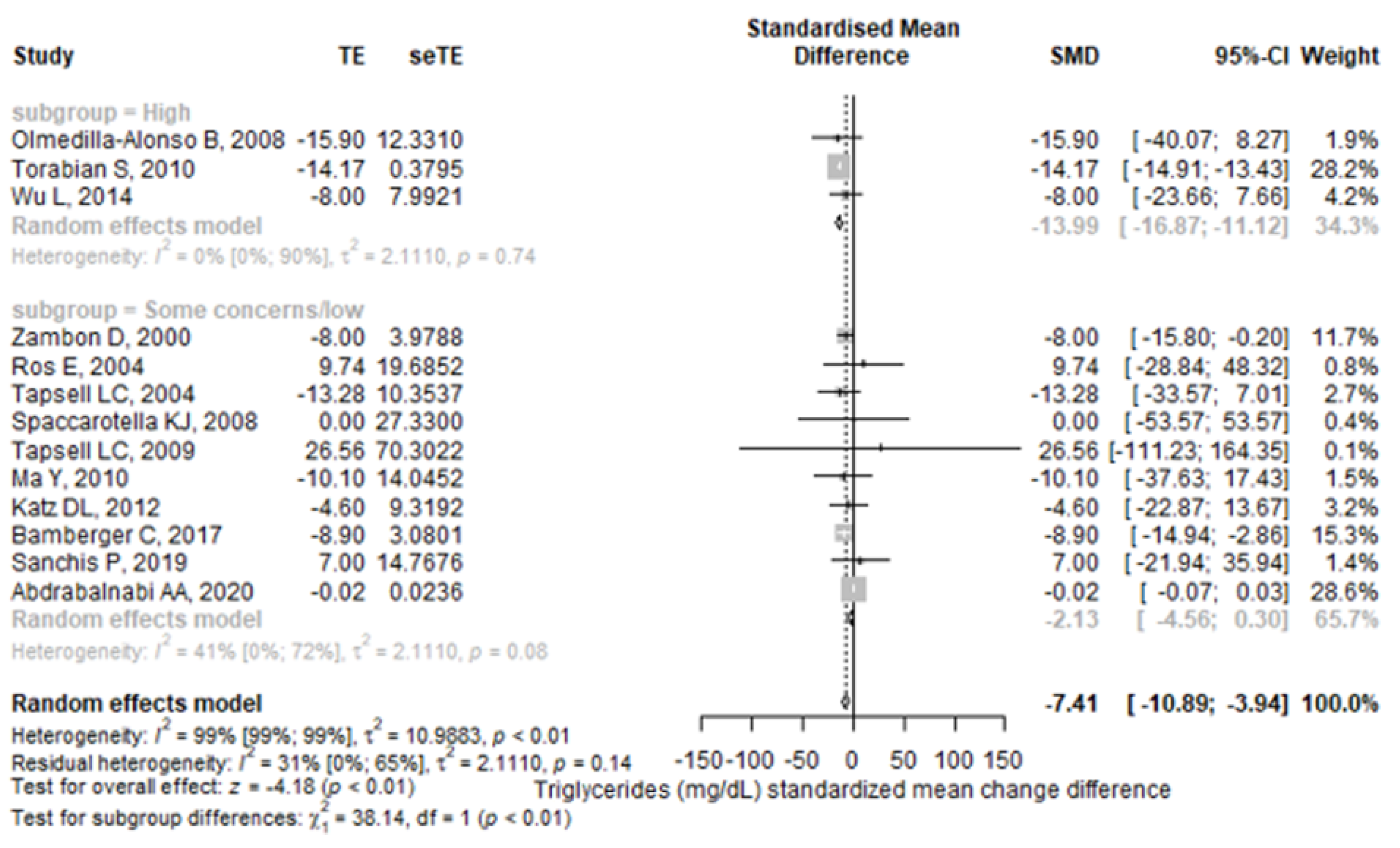
3.1.1. Triglycerides
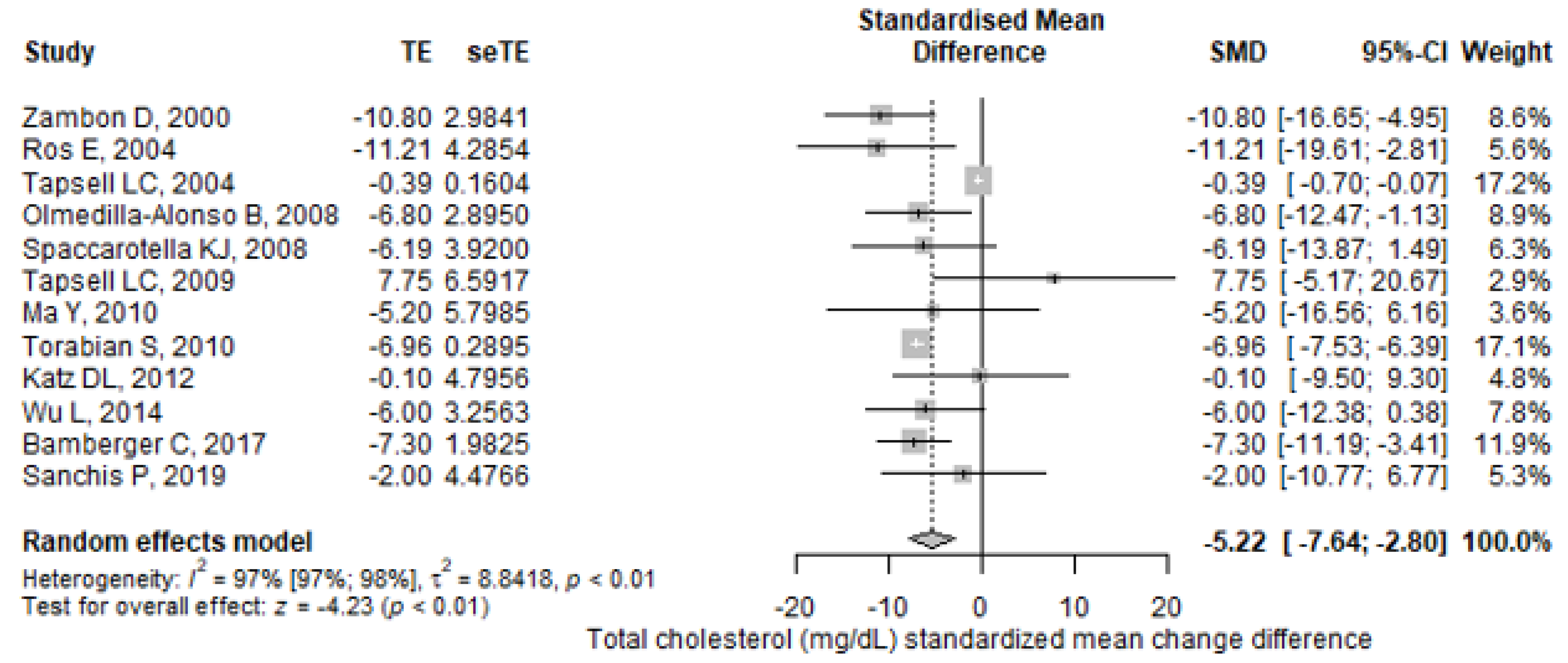
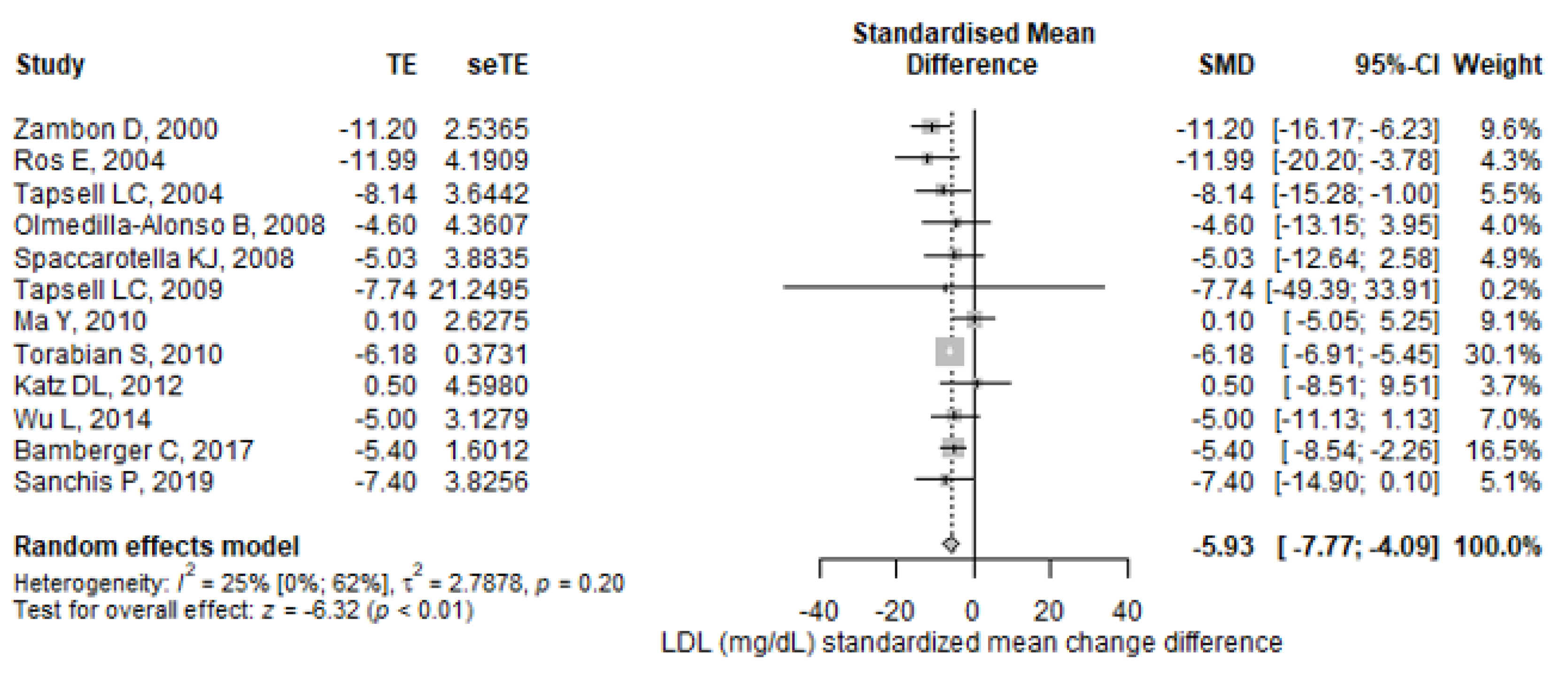
3.1.2. Total Cholesterol, LDL, and HDL Cholesterol
3.1.3. Anthropometric Markers
3.1.4. Blood Pressure
3.1.5. Glycemic Biomarkers
3.2. Inflammatory Biomarkers
3.3. Quality Assessment
3.4. Reporting Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ALA | α-linolenic acid |
| apoB | apolipoprotein B |
| BMI | body mass index |
| BW | body weight |
| CI | confidence interval |
| CI | confidence interval |
| CRP | C-reactive protein |
| CVD | cardiovascular diseases |
| DBP | diastolic blood pressure |
| eTE | the standard error of the treatment effect |
| FBG | fasting blood glucose |
| HbA1c | glycosylated hemoglobin A1c |
| HDL-C | high density lipoprotein-cholesterol |
| HOMA-IR | homeostatic model assessment for insulin resistance |
| hs-CRP | high-sensitivity C-reactive protein |
| ICAM-1 | intercellular adhesion molecule-1 |
| IF | interferon gamma |
| IL-1β | interleukin-1β |
| IL-6 | interleukin-6 |
| IQR | interquartile ranges |
| LDL-C | low density lipoprotein-cholesterol |
| MedD | Mediterranean diet |
| MetS | metabolic syndrome |
| MUFAs | monounsaturated fatty acids |
| NF-кB | nuclear factor kappa B |
| Nrf2/ARE | nuclear factor erythroid 2-related factor 2/antioxidant response element |
| PUFAs | polyunsaturated fatty acids |
| RCT | randomized controlled trial |
| ROS | reactive oxygen species |
| SBP | systolic blood pressure |
| SD | standard deviation |
| SE | standard error |
| SMD | standardized mean difference |
| SMD | standardized mean change difference |
| T2D | type 2 diabetes |
| TC | total cholesterol |
| TE | treatment effect |
| TG | triglycerides |
| TNF-α | tumor necrosis factor-alpha |
| VCAM-1 | vascular cell adhesion molecule-1 |
| W | weight |
| WC | waist circumference |
References
- Rea, I.M.; Gibson, D.S.; McGilligan, V.; McNerlan, S.E.; Denis Alexander, H.; Ross, O.A. Age and Age-Related Diseases: Role of Inflammation Triggers and Cytokines. Front. Immunol. 2018, 9, 586. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Campisi, J. Chronic Inflammation (Inflammaging) and Its Potential Contribution to Age-Associated Diseases. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, S4–S9. [Google Scholar] [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic Inflammation in the Etiology of Disease across the Life Span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, J.L.; Tchkonia, T. Cellular Senescence: A Translational Perspective. EBioMedicine 2017, 21, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapa, S.F.; di Iorio, B.R.; Campiglia, P.; Heidland, A.; Marzocco, S. Inflammation and Oxidative Stress in Chronic Kidney Disease—Potential Therapeutic Role of Minerals, Vitamins and Plant-Derived Metabolites. Int. J. Mol. Sci. 2020, 21, 263. [Google Scholar] [CrossRef] [Green Version]
- Popa, D.S.; Bigman, G.; Rusu, M.E. The Role of Vitamin K in Humans: Implication in Aging and Age-Associated Diseases. Antioxidants 2021, 10, 566. [Google Scholar] [CrossRef]
- Ajabnoor, S.M.; Thorpe, G.; Abdelhamid, A.; Hooper, L. Long-Term Effects of Increasing Omega-3, Omega-6 and Total Polyunsaturated Fats on Inflammatory Bowel Disease and Markers of Inflammation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. J. Nutr. 2021, 60, 2293–2316. [Google Scholar] [CrossRef]
- Kiss, B.; Popa, D.-S.; Crişan, G.; Bojiţă, M.; Loghin, F. The Evaluation of Antioxidant Potential of Veronica Officinalis and Rosmarinus Officinalis Extracts by Monitoring Malondialdehide and Glutathione Levels in Rats. Farmacia 2009, 57, 432–441. [Google Scholar]
- Trautwein, E.A.; McKay, S. The Role of Specific Components of a Plant-Based Diet in Management of Dyslipidemia and the Impact on Cardiovascular Risk. Nutrients 2020, 12, 2671. [Google Scholar] [CrossRef]
- Fizeșan, I.; Rusu, M.E.; Georgiu, C.; Pop, A.; Ștefan, M.G.; Muntean, D.M.; Mirel, S.; Vostinaru, O.; Kiss, B.; Popa, D.S. Antitussive, Antioxidant, and Anti-Inflammatory Effects of a Walnut (Juglans Regia L.) Septum Extract Rich in Bioactive Compounds. Antioxidants 2021, 10, 119. [Google Scholar] [CrossRef]
- Rusu, M.E.; Simedrea, R.; Gheldiu, A.M.; Mocan, A.; Vlase, L.; Popa, D.S.; Ferreira, I.C.F.R. Benefits of Tree Nut Consumption on Aging and Age-Related Diseases: Mechanisms of Actions. Trends Food Sci. Technol. 2019, 88, 104–120. [Google Scholar] [CrossRef]
- de Souza, R.G.M.; Schincaglia, R.M.; Pimente, G.D.; Mota, J.F. Nuts and Human Health Outcomes: A Systematic Review. Nutrients 2017, 9, 1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pop, A.; Fizesan, I.; Vlase, L.; Rusu, M.E.; Cherfan, J.; Babota, M.; Gheldiu, A.-M.; Tomuta, I.; Popa, D.-S. Enhanced Recovery of Phenolic and Tocopherolic Compounds from Walnut (Juglans Regia L.) Male Flowers Based on Process Optimization of Ultrasonic Assisted-Extraction: Phytochemical Profile and Biological Activities. Antioxidants 2021, 10, 607. [Google Scholar] [CrossRef] [PubMed]
- Ros, E.; Singh, A.; O’Keefe, J.H. Nuts: Natural Pleiotropic Nutraceuticals. Nutrients 2021, 13, 3269. [Google Scholar] [CrossRef] [PubMed]
- Rusu, M.E.; Mocan, A.; Ferreira, I.C.F.R.; Popa, D.S. Health Benefits of Nut Consumption in Middle-Aged and Elderly Population. Antioxidants 2019, 8, 302. [Google Scholar] [CrossRef] [Green Version]
- Ros, E.; Izquierdo-Pulido, M.; Sala-Vila, A. Beneficial Effects of Walnut Consumption on Human Health: Role of Micronutrients. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Blondeau, N.; Lipsky, R.H.; Bourourou, M.; Duncan, M.W.; Gorelick, P.B.; Marini, A.M. Alpha-Linolenic Acid: An Omega-3 Fatty Acid with Neuroprotective Properties—Ready for Use in the Stroke Clinic? BioMed Res. Int. 2015, 2015, 519830. [Google Scholar] [CrossRef] [Green Version]
- Hardman, W.E.; Primerano, D.A.; Legenza, M.T.; Morgan, J.; Fan, J.; Denvir, J. Dietary Walnut Altered Gene Expressions Related to Tumor Growth, Survival, and Metastasis in Breast Cancer Patients: A Pilot Clinical Trial. Nutr. Res. 2019, 66, 82–94. [Google Scholar] [CrossRef]
- Borkowski, K.; Yim, S.J.; Holt, R.R.; Hackman, R.M.; Keen, C.L.; Newman, J.W.; Shearer, G.C. Walnuts Change Lipoprotein Composition Suppressing TNFα-Stimulated Cytokine Production by Diabetic Adipocyte. J. Nutr. Biochem. 2019, 68, 51–58. [Google Scholar] [CrossRef]
- Hwang, H.J.; Liu, Y.; Kim, H.S.; Lee, H.; Lim, Y.; Park, H. Daily Walnut Intake Improves Metabolic Syndrome Status and Increases Circulating Adiponectin Levels: Randomized Controlled Crossover Trial. Nutr. Res. Pract. 2019, 13, 105–114. [Google Scholar] [CrossRef]
- Arab, L.; Dhaliwal, S.K.; Martin, C.J.; Larios, A.D.; Jackson, N.J.; Elashoff, D. Association between Walnut Consumption and Diabetes Risk in NHANES. Diabetes/Metab. Res. Rev. 2018, 34, e3031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cahoon, D.; Shertukde, S.P.; Avendano, E.E.; Tanprasertsuk, J.; Scott, T.M.; Johnson, E.J.; Chung, M.; Nirmala, N. Walnut Intake, Cognitive Outcomes and Risk Factors: A Systematic Review and Meta-Analysis. Ann. Med. 2021, 53, 971–997. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Liu, R.; Chang, M.; Huang, J.; Jin, Q.; Wang, X. Effect of Dietary Alpha-Linolenic Acid on Blood Inflammatory Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. J. Nutr. 2018, 57, 877–891. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019; ISBN 9781119536628. [Google Scholar]
- Elbourne, D.R.; Altman, D.G.; Higgins, J.P.; Curtin, F.; Worthington, H.V.; Vail, A. Meta-Analyses Involving Cross-over Trials: Methodological Issues. Int. J. Epidemiol. 2002, 31, 140–149. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide, 1st ed.; CRC Press: Boca Raton, FL, USA, 2021. [Google Scholar] [CrossRef]
- R Core Team R: A Language and Environment for Statistical Computing. Available online: https://www.R_project.org/ (accessed on 4 June 2022).
- Zambón, D.; Sabaté, J.; Muñoz, S.; Campero, B.; Casals, E.; Merlos, M.; Laguna, J.C.; Ros, E. Substituting Walnuts for Monounsaturated Fat Improves the Serum Lipid Profile of Hypercholesterolemic Men and Women A Randomized Crossover Trial. Ann. Intern. Med. 2000, 132, 538–546. [Google Scholar] [CrossRef]
- Ros, E.; Núñez, I.; Pérez-Heras, A.; Serra, M.; Gilabert, R.; Casals, E.; Deulofeu, R. A Walnut Diet Improves Endothelial Function in Hypercholesterolemic Subjects: A Randomized Crossover Trial. Circulation 2004, 109, 1609–1614. [Google Scholar] [CrossRef] [Green Version]
- Tapsell, L.C.; Gillen, L.J.; Patch, C.S.; Batterham, M.; Owen, A.; Baré, M.; Kennedy, M. Including Walnuts in a Low-Fat/Modified-Fat Diet Improves HDL Cholesterol-to-Total Cholesterol Ratios in Patients With Type 2 Diabetes. Diabetes Care 2004, 27, 2777–2783. [Google Scholar] [CrossRef] [Green Version]
- Olmedilla-Alonso, B.; Granado-Lorencio, F.; Herrero-Barbudo, C.; Blanco-Navarro, I.; Blázquez-García, S.; Pérez-Sacristán, B. Consumption of Restructured Meat Products with Added Walnuts Has a Cholesterol-Lowering Effect in Subjects at High Cardiovascular Risk: A Randomised, Crossover, Placebo-Controlled Study. J. Am. Coll. Nutr. 2008, 27, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Spaccarotella, K.J.; Kris-Etherton, P.M.; Stone, W.L.; Bagshaw, D.M.; Fishell, V.K.; West, S.G.; Lawrence, F.R.; Hartman, T.J. The Effect of Walnut Intake on Factors Related to Prostate and Vascular Health in Older Men. Nutr. J. 2008, 7, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tapsell, L.C.; Batterham, M.J.; Teuss, G.; Tan, S.Y.; Dalton, S.; Quick, C.J.; Gillen, L.J.; Charlton, K.E. Long-Term Effects of Increased Dietary Polyunsaturated Fat from Walnuts on Metabolic Parameters in Type II Diabetes. Eur. J. Clin. Nutr. 2009, 63, 1008–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Njike, V.Y.; Millet, J.; Dutta, S.; Doughty, K.; Treu, J.A.; Katz, D.L. Effects of Walnut Consumption on Endothelial Function in Type 2 Diabetic Subjects: A Randomized Controlled Crossover Trial. Diabetes Care 2010, 33, 227–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torabian, S.; Haddad, E.; Cordero-Macintyre, Z.; Tanzman, J.; Fernandez, M.L.; Sabate, J. Long-Term Walnut Supplementation without Dietary Advice Induces Favorable Serum Lipid Changes in Free-Living Individuals. Eur. J. Clin. Nutr. 2010, 64, 274–279. [Google Scholar] [CrossRef] [Green Version]
- Canales, A.; Sánchez-Muniz, F.J.; Bastida, S.; Librelotto, J.; Nus, M.; Corella, D.; Guillen, M.; Benedi, J. Effect of Walnut-Enriched Meat on the Relationship between VCAM, ICAM, and LTB4 Levels and PON-1 Activity in ApoA4 360 and PON-1 Allele Carriers at Increased Cardiovascular Risk. Eur. J. Clin. Nutr. 2011, 65, 703–710. [Google Scholar] [CrossRef] [Green Version]
- Katz, D.L.; Davidhi, A.; Ma, Y.; Kavak, Y.; Bifulco, L.; Njike, V.Y. Effects of Walnuts on Endothelial Function in Overweight Adults with Visceral Obesity: A Randomized, Controlled, Crossover Trial. J. Am. Coll. Nutr. 2012, 6, 415–423. [Google Scholar] [CrossRef]
- Wu, L.; Piotrowski, K.; Rau, T.; Waldmann, E.; Broedl, U.C.; Demmelmair, H.; Koletzko, B.; Stark, R.G.; Nagel, J.M.; Mantzoros, C.S.; et al. Walnut-Enriched Diet Reduces Fasting Non-HDL-Cholesterol and Apolipoprotein B in Healthy Caucasian Subjects: A Randomized Controlled Cross-over Clinical Trial. Metab. Clin. Exp. 2014, 63, 382–391. [Google Scholar] [CrossRef]
- Bamberger, C.; Rossmeier, A.; Lechner, K.; Wu, L.; Waldmann, E.; Stark, R.G.; Altenhofer, J.; Henze, K.; Parhofer, K.G. A Walnut-Enriched Diet Reduces Lipids in Healthy Caucasian Subjects, Independent of Recommended Macronutrient Replacement and Time Point of Consumption: A Prospective, Randomized, Controlled Trial. Nutrients 2017, 9, 1097. [Google Scholar] [CrossRef]
- Bitok, E.; Rajaram, S.; Jaceldo-Siegl, K.; Oda, K.; Sala-Vila, A.; Serra-Mir, M.; Ros, E.; Sabaté, J. Effects of Long-Term Walnut Supplementation on Body Weight in Free-Living Elderly: Results of a Randomized Controlled Trial. Nutrients 2018, 10, 1317. [Google Scholar] [CrossRef] [Green Version]
- Domènech, M.; Serra-Mir, M.; Roth, I.; Freitas-Simoes, T.; Valls-Pedret, C.; Cofán, M.; López, A.; Sala-Vila, A.; Calvo, C.; Rajaram, S.; et al. Effect of a Walnut Diet on Office and 24-Hour Ambulatory Blood Pressure in Elderly Individuals: Findings from the WAHA Randomized Trial. Hypertension 2019, 73, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Sanchis, P.; Molina, M.; Berga, F.; Muñoz, E.; Fortuny, R.; Costa-Bauzá, A.; Grases, F.; Buades, J.M. A Pilot Randomized Crossover Trial Assessing the Safety and Short-Term Effects of Walnut Consumption by Patients with Chronic Kidney Disease. Nutrients 2020, 12, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdrabalnabi, A.; Rajaram, S.; Bitok, E.; Oda, K.; Beeson, W.L.; Kaur, A.; Cofán, M.; Serra-Mir, M.; Roth, I.; Ros, E.; et al. Effects of Supplementing the Usual Diet with a Daily Dose of Walnuts for Two Years on Metabolic Syndrome and Its Components in an Elderly Cohort. Nutrients 2020, 12, 451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cofán, M.; Rajaram, S.; Sala-Vila, A.; Valls-Pedret, C.; Serra-Mir, M.; Roth, I.; Freitas-Simoes, T.M.; Bitok, E.; Sabaté, J.; Ros, E. Effects of 2-Year Walnut-Supplemented Diet on Inflammatory Biomarkers. J. Am. Coll. Cardiol. 2020, 76, 2282–2284. [Google Scholar] [CrossRef]
- Tindall, A.M.; Johnston, E.A.; Kris-Etherton, P.M.; Petersen, K.S. The Effect of Nuts on Markers of Glycemic Control: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2019, 109, 297–314. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Mesas, A.E.; Garrido-Miguel, M.; Martínez-Ortega, I.A.; Jiménez-López, E.; Martínez-Vizcaíno, V. The Relationship of Tree Nuts and Peanuts with Adiposity Parameters: A Systematic Review and Network Meta-Analysis. Nutrients 2021, 13, 2251. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Martínez-Vizcaíno, V.; Garrido-Miguel, M.; Martínez-Ortega, I.A.; Álvarez-Bueno, C.; Eumann Mesas, A. Nut Consumption, Body Weight, and Adiposity in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutr. Rev. 2022, 80, 645–655. [Google Scholar] [CrossRef]
- Neale, E.P.; Guan, V.; Tapsell, L.C.; Probst, Y.C. Effect of Walnut Consumption on Markers of Blood Glucose Control: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2020, 124, 641–653. [Google Scholar] [CrossRef]
- Tarantino, L.M. Qualified Health Claims: Letter of Enforcement Discretion-Walnuts and Coronary Heart Disease; (Docket No 02P-0292); U.S. Food and Drug Administration: Washington, DC, USA, 2004.
- Arabi, S.M.; Bahrami, L.S.; Milkarizi, N.; Nematy, M.; Kalmykov, V.; Sahebkar, A. Impact of Walnut Consumption on Cardio Metabolic and Anthropometric Parameters in Metabolic Syndrome Patients: GRADE-Assessed Systematic Review and Dose-Response Meta-Analysis of Data from Randomized Controlled Trials. Pharmacol. Res. 2022, 178, 106190. [Google Scholar] [CrossRef]
- Liu, X.; Guasch-Ferré, M.; Drouin-Chartier, J.P.; Tobias, D.K.; Bhupathiraju, S.N.; Rexrode, K.M.; Willett, W.C.; Sun, Q.; Li, Y. Changes in Nut Consumption and Subsequent Cardiovascular Disease Risk Among US Men and Women: 3 Large Prospective Cohort Studies. J. Am. Heart Assoc. 2020, 9, e013877. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Li, J.; Hu, F.B.; Salas-Salvadó, J.; Tobias, D.K. Effects of Walnut Consumption on Blood Lipids and Other Cardiovascular Risk Factors: An Updated Meta-Analysis and Systematic Review of Controlled Trials. Am. J. Clin. Nutr. 2018, 108, 174–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becerra-Tomás, N.; Paz-Graniel, I.; Kendall, C.; Kahleova, H.; Rahelić, D.; Sievenpiper, J.L.; Salas-Salvadó, J. Nut Consumption and Incidence of Cardiovascular Diseases and Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies. Nutr. Rev. 2019, 77, 691–709. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Guasch-Ferré, M.; Tobias, D.K.; Li, Y. Association of Walnut Consumption with Total and Cause-Specific Mortality and Life Expectancy in U.S. Adults. Nutrients 2021, 13, 2699. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Rusu, M.E.; Gheldiu, A.M.; Mocan, A.; Vlase, L.; Popa, D.S. Anti-Aging Potential of Tree Nuts with a Focus on the Phytochemical Composition, Molecular Mechanisms and Thermal Stability of Major Bioactive Compounds. Food Funct. 2018, 9, 2554–2575. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Jiang, B.; Santos, H.O.; Santos, D.; Singh, A.; Wang, L. Effects of Walnut Intake on Blood Pressure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phytother. Res. 2020, 34, 2921–2931. [Google Scholar] [CrossRef]
- Banel, D.K.; Hu, F.B. Effects of Walnut Consumption on Blood Lipids and Other Cardiovascular Risk Factors: A Meta-Analysis and Systematic Review. Am. J. Clin. Nutr. 2009, 90, 56–63. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Schulze, M.B.; Fung, T.T.; Meigs, J.B.; Rifai, N.; Manson, J.E.; Hu, F.B. Major Dietary Patterns Are Related to Plasma Concentrations of Markers of Inflammation and Endothelial Dysfunction 1-3. Am. J. Clin. Nutr. 2004, 80, 1029–1064. [Google Scholar] [CrossRef] [Green Version]
- Yu, Z.; Malik, V.S.; Keum, N.N.; Hu, F.B.; Giovannucci, E.L.; Stampfer, M.J.; Willett, W.C.; Fuchs, C.S.; Bao, Y. Associations between Nut Consumption and Inflammatory Biomarkers. Am. J. Clin. Nutr. 2016, 104, 722–728. [Google Scholar] [CrossRef] [Green Version]
- Rusu, M.E.; Fizesan, I.; Pop, A.; Mocan, A.; Gheldiu, A.M.; Babota, M.; Vodnar, D.C.; Jurj, A.; Berindan-Neagoe, I.; Vlase, L.; et al. Walnut (Juglans Regia L.) Septum: Assessment of Bioactive Molecules and in Vitro Biological Effects. Molecules 2020, 25, 2187. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Country | Study (RCT) Design | Exposure Period | Washout Period | Participants (n), Health Status | Age (Years), (SD)/(IQR) (Range) | Female (%) | Walnut Intervention (g/d) | Control Intervention | Outcome of Interest |
|---|---|---|---|---|---|---|---|---|---|---|
| Zambόn et al., 2000 [31] | Spain, USA | Crossover | 6 weeks | 0 | 49 polygenic hypercholesterolemia * | 56 (±11) | 47% | 41–56 g/d (18% of the energy need) | MedD (no walnut) | BW, TC, LDL-C, HDL-C, TG |
| Ros et al., 2004 [32] | Spain | Crossover | 4 weeks | 0 | 20 healthy, non-smokers (hypercholesterolemia) | 55 (±55.9) | 60% | 40–65 g/d (18% of energy need) | MedD (no walnut) | BW, SBP, DBP, TC, LDL-C, HDL-C, CRP, |
| Tapsell et al., 2004 [33] | Australia | Parallel | 6 months | NA | 58 T2D * | 59.3 (±8.1) | 41.37% | 30 g/d—walnut-enriched modified low-fat diet | Modified low-fat diet (no walnuts) | BW, BMI, HbA1c, TC, LDL-C, HDL-C, TG |
| Olmedilla- Alonso et al., 2008 [34] | Spain | Crossover | 5 weeks | 1 month | 25 CV risk, smokers | 54.4 (±8.1) | 40% | 19.4 g/d (20% walnut-enriched meat products) | Restructured meat products (no walnut) | TC, HDL-C, LDL-C, TG, BW, SBP, DBP |
| Spaccarotella et al., 2008 [35] | USA | Crossover | 8 weeks | 2 weeks | 21 healthy, non-smokers | 65.9 (55–75) | 0% | 75 g/d (24% of energy need) | Western-type diet (no walnut) | SBP, DBP, TC, HDL-C, LDL-C |
| Tapsell et al., 2009 [36] | Australia | Parallel | 1 year | NA | 50 T2D * | 54 (±8.7) | NI | 30 g/d (walnut-enriched 2000 kcal diet, 30% fat) | 2000 kcal diet, 30% fat (no walnut) | BW, FBG, TC, HDL-C, LDL-C, TG, HbA1c, insulin |
| Ma et al., 2010 [37] | USA | Crossover | 8 weeks | 8 weeks | 21 T2D, non-smokers | 58.1 (±9.2) | 58.30% | 56 g/d | Habitual diet (no walnut) | TC, HDL-C, LDL-C, TG, FPG, insulin, HOMA-IR, BW, BMI, WC, SBP, DBP |
| Torabian et al., 2010 [38] | USA | Crossover | 6 months | 0 | 87 healthy, non-smokers | 54 (±10.2) | 56% | 28–64 g/d (12% of energy need) | Habitual diet (no walnut) | TC, LDL-C, HDL-C, TG |
| Canales et al., 2011 [39] | Spain | Crossover | 5 weeks | 4–6 weeks | 22 CV risk, smokers | 54.8 (±9.4) | 40% | 34–29 g/d (20% walnut-enriched meat) | Low-fat meat products (no walnut) | VCAM-1, ICAM-1, HDL-C |
| Katz et al., 2012 [40] | USA | Crossover | 8 weeks | 4 weeks | 40 healthy, non-smokers (overweight, MetS risk) | 57.4 (±11.9) | 60.9% | 56 g/d | Habitual diet (no walnut) | TC, HDL-C, LDL-C, TG, FPG, insulin, HOMA-IR, BW, BMI, WC, SBP, DBP |
| Wu et al., 2014 [41] | Germany, USA | Crossover | 8 weeks | 2 weeks | 40 healthy * | 60 (±6.32) | 75% | 43 g/d (replacing 30 g saturated fat in Western-type diet) | Western-type diet (no walnut) | TC, LDL-C, HDL-C, FBG, insulin, HOMA-IR, HbA1c, VCAM-1, ICAM-1 |
| Bamberger et al., 2017 [42] | Germany | Crossover | 8 weeks | 4 weeks | 194 healthy, non-smokers | 63 (±7) | 69% | 43 g/d | Western-type diet (no walnut) | TC, LDL-C, HDL-C, TG |
| Bitok et al., 2018 [43] | USA, Spain | Parallel | 2 years | NA | 307 healthy * | 69.4 (±3.9) | 67% | 28; 42; 56 g/d (15% of energy need) | Habitual diet (no walnut) | BW, WC |
| Domènech et al., 2019 [44] | USA, Spain | Parallel | 2 years | NA | 236 healthy * (60% mild hyper-tension) | 68.8 (±3.3) | 65% | 30–60 g/d, (15% of energy need) | Habitual diet (no walnut) | SBP, DBP |
| Sanchis et al., 2019 [45] | Spain | Crossover | 30 days | 30 days | 13 CKD * | 71 (±10.11) | 46.20% | 30 g/d (walnut-enriched CKD diet) | CKD patients’ diet (no walnut) | BMI, TC, HDL-C, LDL-C, TG, FBG, HbA1c, CRP |
| Abdrabalnabi et al., 2020 [46] | USA, Spain | Parallel | 2 years | NA | 625 healthy * | 69.1 (±3.6) | 67% | 30; 45; 60 g/d (15% of energy need) | Habitual diet (no walnut) | BMI, SBP, DBP, TG, HDL-C, FBG |
| Cofán et al., 2020 [47] | USA, Spain | Parallel | 2 years | NA | 634 healthy * | 69.1 (±3.6) | 66% | 30; 45; 60 g/d (15% of energy need) | Western-type diet (no walnut) | VCAM-1, ICAM-1, IL-6, IFN-γ, IL-1β, TNF-α, E-selectin, hs-CRP |
| Characteristic, Effect Size Type, SMD | Effect Size (95% CI) | p-Value | I2 (95% CI) | p-Value | Egger Test | Studies |
|---|---|---|---|---|---|---|
| CRP (mg/L) | −0.37 (−1.39–0.65) | 0.478 | NC | NC | [32,45] | |
| hs-CRP (mg/L) | −0.01 (−0.12–0.11) | 0.903 | NC | NC | [47] | |
| IFN-γ (pg/mL) | −1.26 (−2.01–−0.51) | <0.001 | NC | NC | [47] | |
| IL-6 (pg/mL) | −0.18 (−0.33–−0.03) | 0.021 | NC | NC | [47] | |
| IL-1β (pg/mL) | −0.1 (−0.16–−0.04) | <0.001 | NC | NC | [47] | |
| TNF-α (pg/mL) | −0.31 (−0.54–−0.08) | 0.009 | NC | NC | [47] | |
| E-selectin (ng/mL) | −2.57 (−4.09–−1.05) | <0.001 | NC | NC | [47] | |
| ICAM-1 (ng/mL) | −0.02 (−0.11–0.07) ANC | 0.672 | - | - | - | [39,41,47] |
| VCAM-1 (ng/mL) | −0.11 (−0.32–0.1) ANC | 0.305 | - | - | - | [39,41,47] |
| WC (cm) | −0.14 (−0.8–0.51) | 0.671 | 0 (0–89.6) | 0.71 | 0.572 | [37,40,43] |
| BMI (kg/m2) | 0.11 (−0.11–0.34) | 0.326 | 63.1 (2.4–86) | 0.028 | 0.683 | [33,37,40,45,46] |
| BW (kg) | 0 (−0.4–0.39) | 0.987 | 22.2 (0–64.1) | 0.253 | 0.537 | [31,32,33,34,36,37,40,43] |
| SBP (mmHg) | −0.85 (−4.48–2.77) | 0.644 | 64.4 (24–83.4) | 0.006 | 0.699 | [32,34,35,37,40,44,45,46] |
| DBP (mmHg) | −0.34 (−1.68–1) | 0.62 | 35.3 (0–71.4) | 0.146 | 0.551 | [32,34,35,37,40,44,45,46] |
| FBG (mg/dL) | 0.01 (0–0.02) | 0.088 | 0 (0–74.6) | 0.692 | 0.57 | [36,37,40,41,45,46] |
| TG (mg/dL) | −7.41 (−10.89–−3.94) | <0.001 | 99.1 (99–99.3) | <0.001 | 0.264 | [31,32,33,34,35,36,37,38,40,41,42,45,46] |
| TC (mg/dL) | −5.22 (−7.64–−2.8) | <0.001 | 97.4 (96.5–98.1) | <0.001 | 0.375 | [31,32,34,35,36,37,38,40,41,42,45] |
| HDL-C (mg/dL) | −0.18 (−0.59–0.22) | 0.375 | 47.4 (0–72.4) | 0.029 | 0.507 | [31,32,33,34,35,36,37,38,39,40,41,42,45,46] |
| LDL-C (mg/dL) | −5.93 (−7.77–−4.09) | <0.001 | 24.8 (0–61.8) | 0.2 | 0.83 | [31,32,33,34,35,36,37,38,40,41,42,45] |
| HbA1c (%) | 0.08 (−0.04–0.2) | 0.196 | 0 (0–84.7) | 0.774 | 0.816 | [33,36,41,45] |
| HOMA-IR | 0.03 (−0.44–0.5) | 0.891 | 57.1 (0–87.8) | 0.097 | 0.95 | [37,40,41] |
| Insulin (mIU/mL) | 0.91 (−2.16–3.98) | 0.561 | 65.4 (0–88.2) | 0.034 | 0.505 | [36,37,40,41] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mateș, L.; Popa, D.-S.; Rusu, M.E.; Fizeșan, I.; Leucuța, D. Walnut Intake Interventions Targeting Biomarkers of Metabolic Syndrome and Inflammation in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants 2022, 11, 1412. https://doi.org/10.3390/antiox11071412
Mateș L, Popa D-S, Rusu ME, Fizeșan I, Leucuța D. Walnut Intake Interventions Targeting Biomarkers of Metabolic Syndrome and Inflammation in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants. 2022; 11(7):1412. https://doi.org/10.3390/antiox11071412
Chicago/Turabian StyleMateș, Letiția, Daniela-Saveta Popa, Marius Emil Rusu, Ionel Fizeșan, and Daniel Leucuța. 2022. "Walnut Intake Interventions Targeting Biomarkers of Metabolic Syndrome and Inflammation in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Antioxidants 11, no. 7: 1412. https://doi.org/10.3390/antiox11071412