
Comparative Study of the Results of Operations in Patients with Tumor and Non-Tumor Obstructive Jaundice Who Received and Did Not Receive Antioxidant Therapy for the Correction of Endotoxemia, Glycolysis, and Oxidative Stress


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethics
2.3. Methods
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Patients Included in the Study
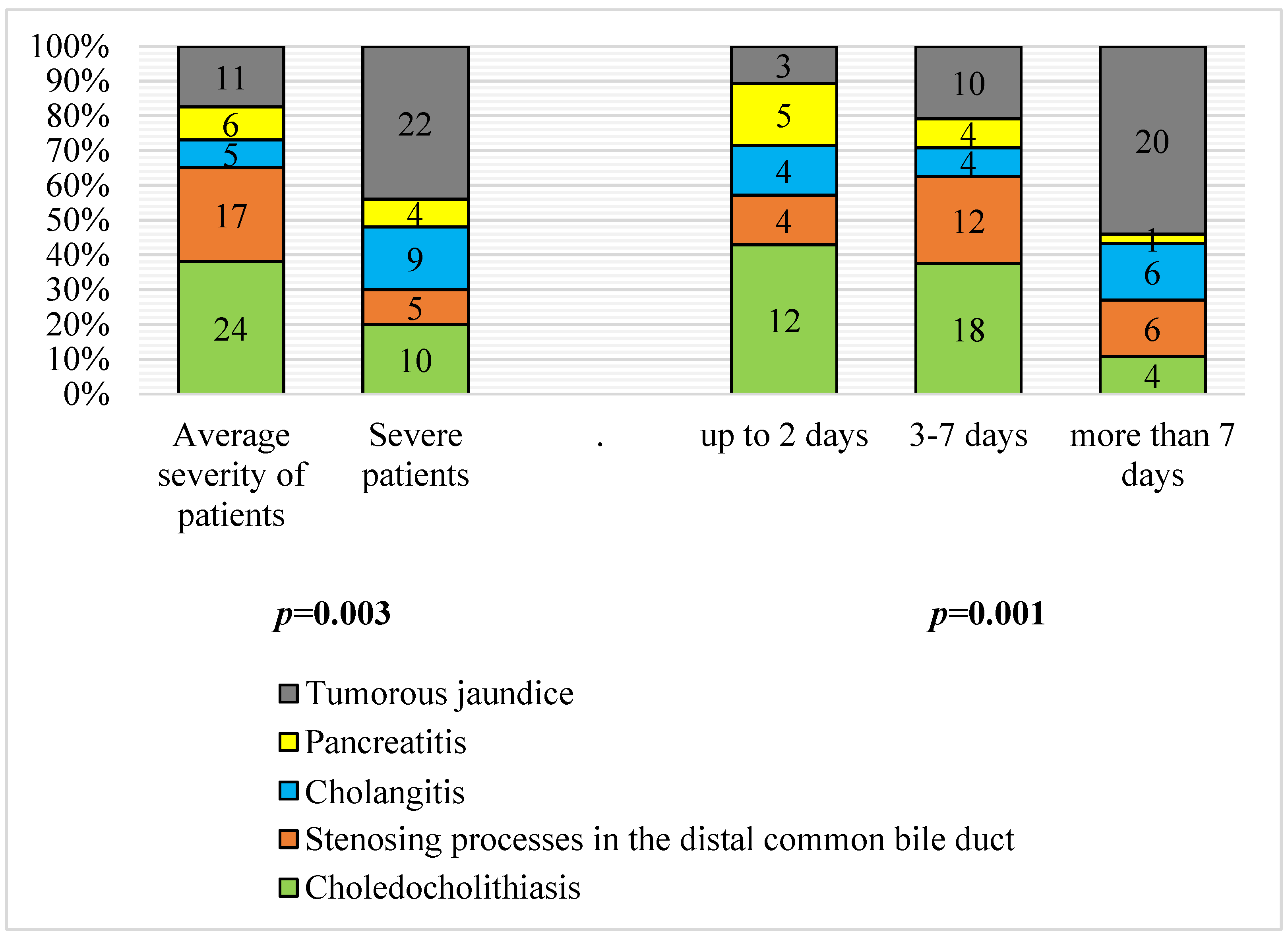
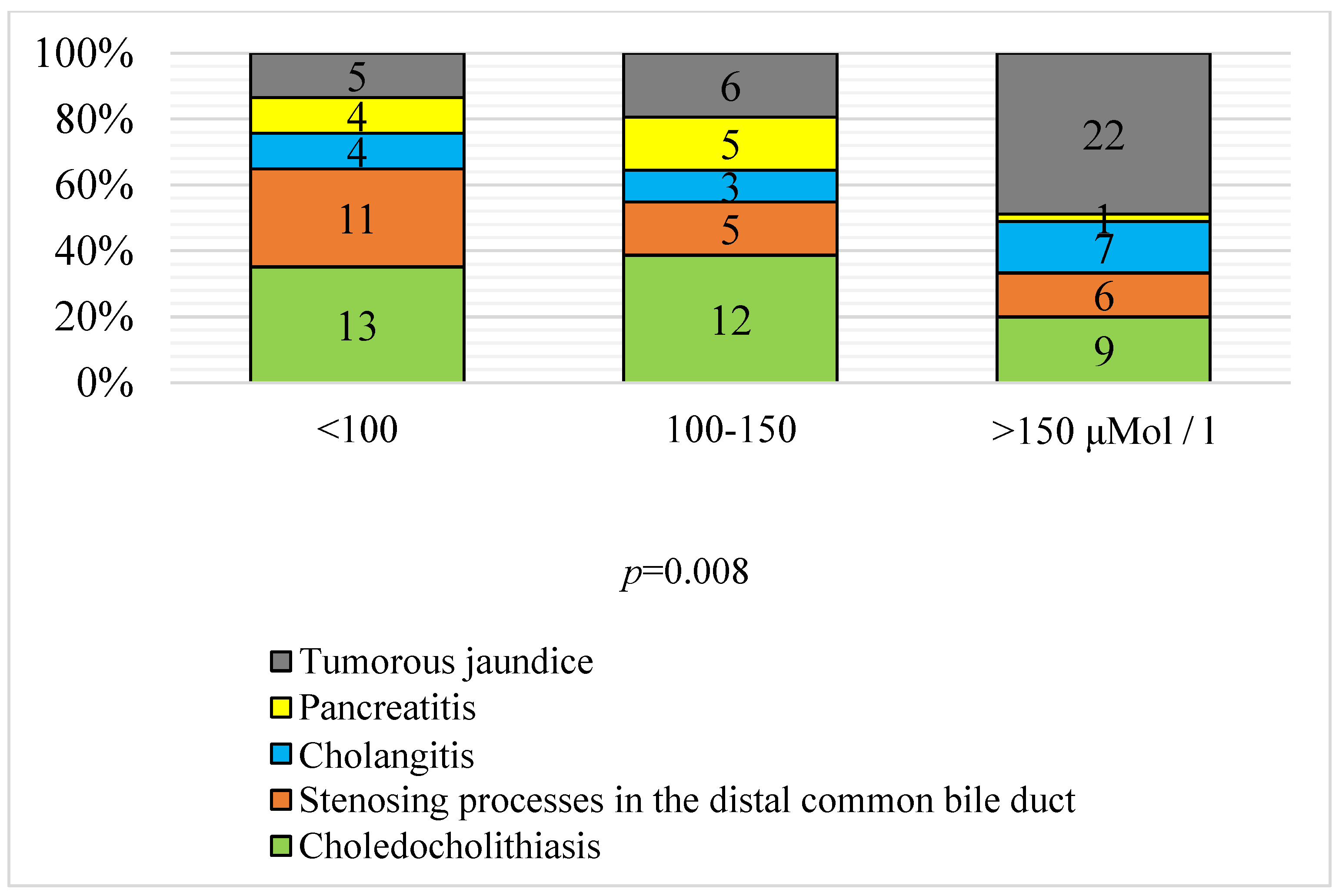
3.2. Severity and Duration of Jaundice according to Etiology
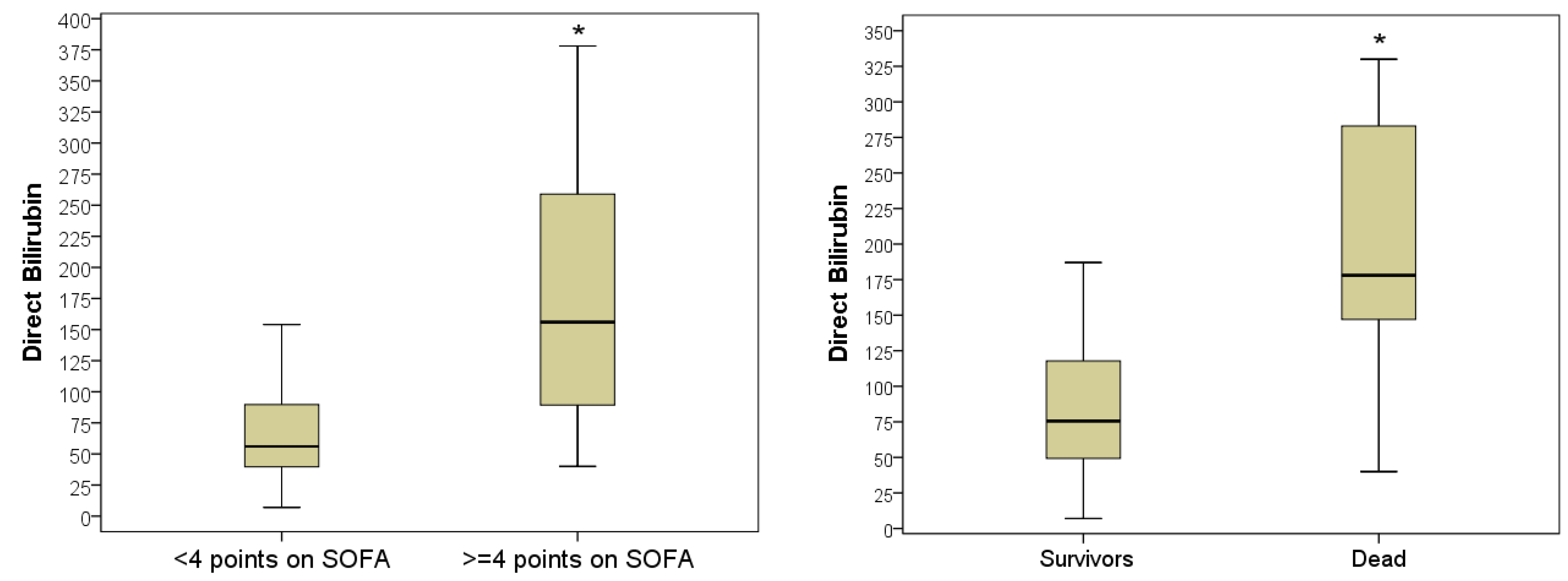
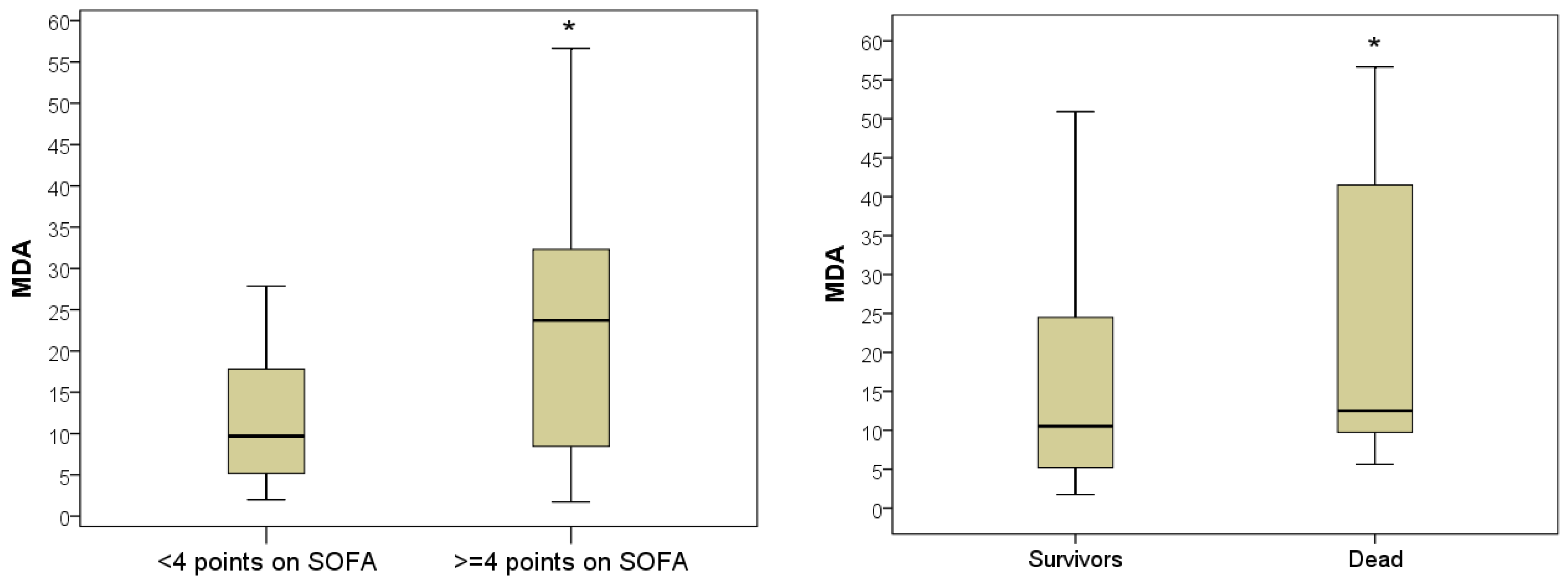
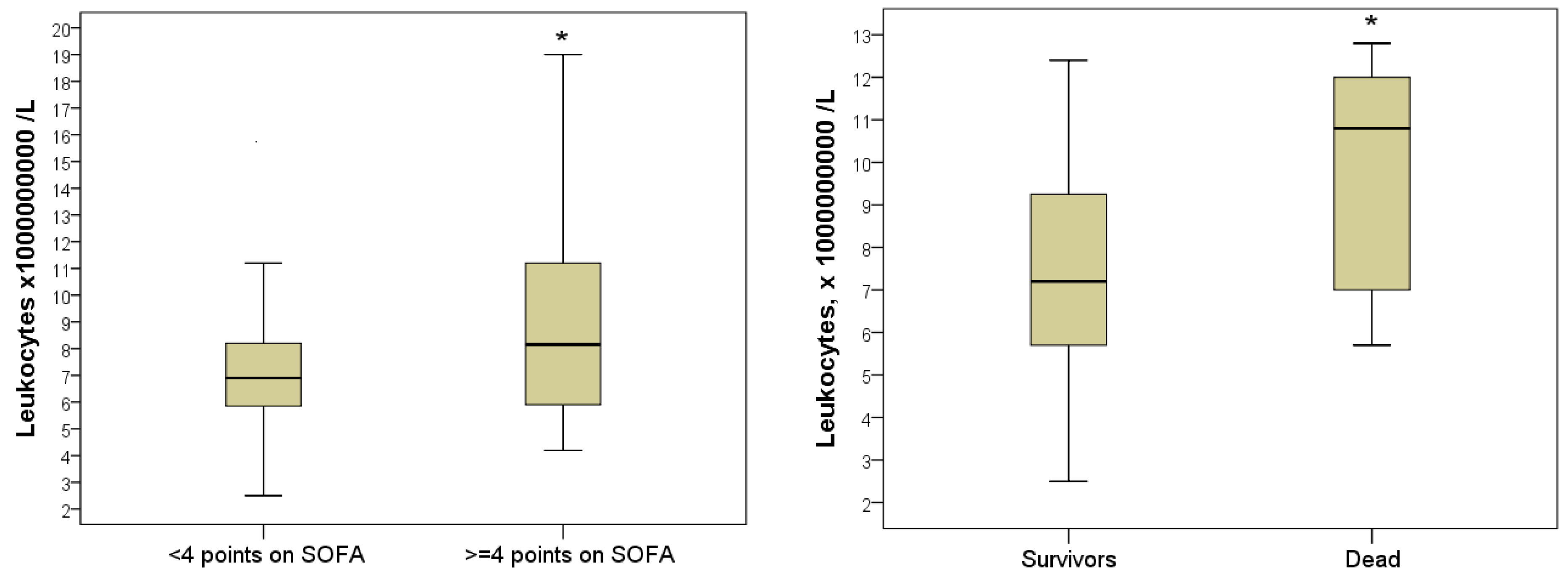
3.3. Predictive Value of the Laboratory Parameters during Hospitalization
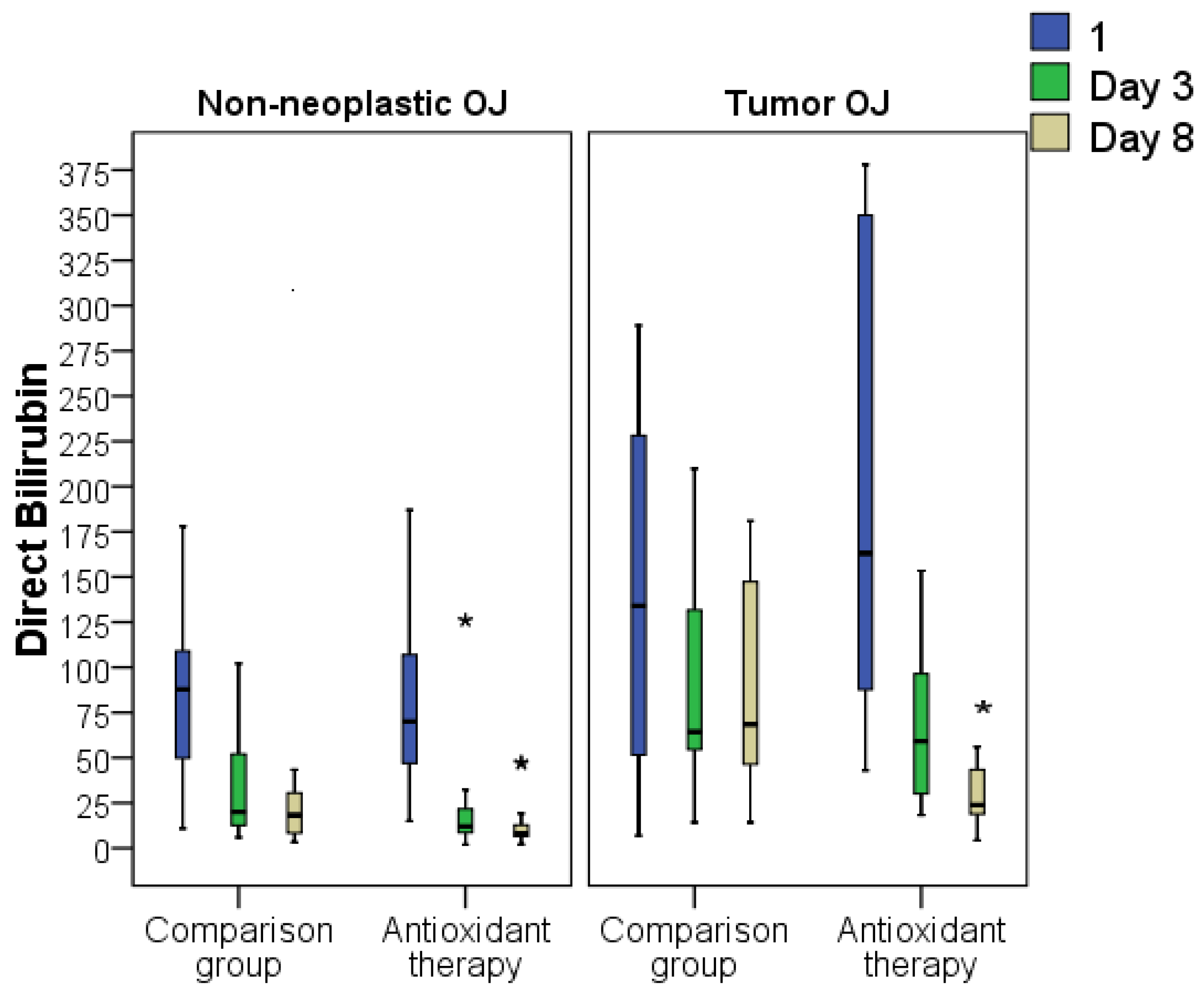
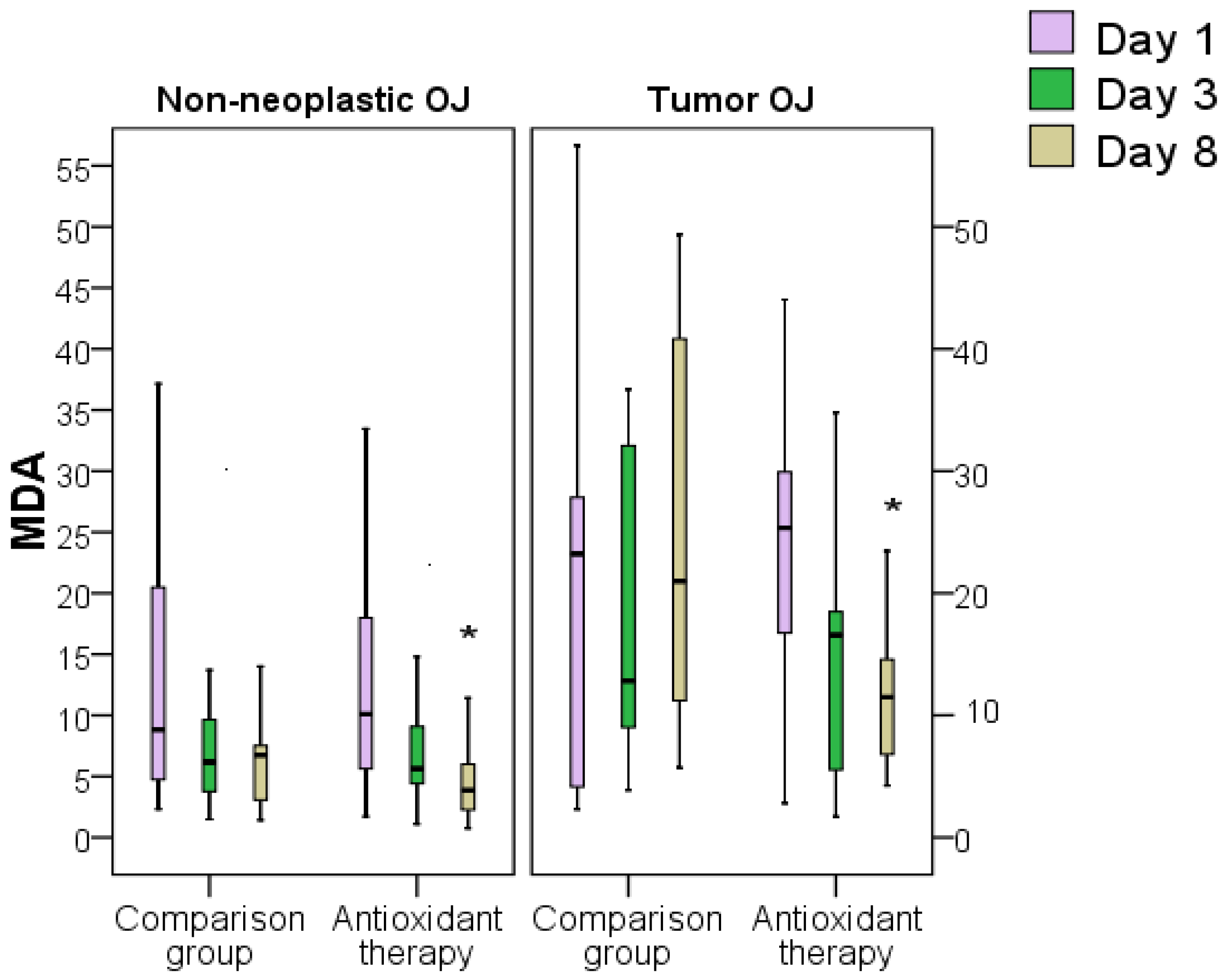
3.4. Influence of Surgical Intervention and Antioxidant Therapy on Laboratory Markers of Severity of Tumor and Non-Tumor Obstructive Jaundice
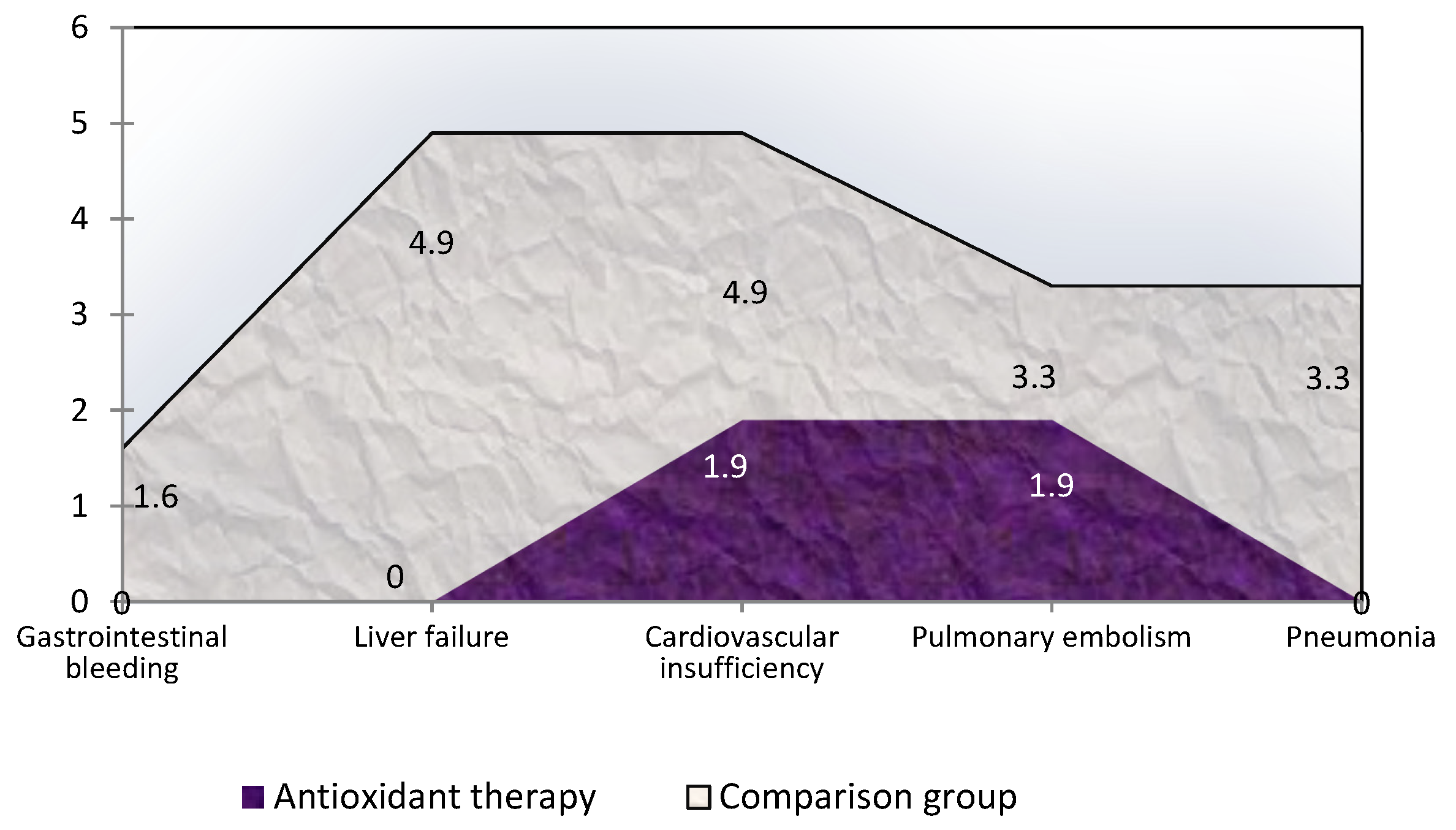
3.5. Influence of Antioxidant Therapy on Treatment Results and Hospital Outcome of Obstructive Jaundice of Tumor and Non-Tumor Origin
4. Discussion
5. Conclusions
6. Research Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soares, P.F.D.C.; Gestic, M.A.; Utrini, M.P.; Callejas-Neto, F.; Chaim, E.A.; Cazzo, E. Epidemiological profile, referral routes and diagnostic accuracy of cases of acute cholangitis among individuals with obstructive jaundice admitted to a tertiary-level university hospital: A cross-sectional study. Sao Paulo Med. J. 2019, 137, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.; Stapley, S.; Hamilton, W. Jaundice in primary care: A cohort study of adults—Aged more 45 years using electronic medical records. Fam. Pract. 2012, 29, 416–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fargo, M.V.; Grogan, S.P.; Saguil, A. Evaluation of Jaundice in Adults. Am. Fam. Physician 2017, 95, 164–168. [Google Scholar] [PubMed]
- Duan, F.; Cui, L.; Bai, Y.; Li, X.; Yan, J.; Liu, X. Comparison of efficacy and complications of endoscopic and percutaneous biliary drainage in malignant obstructive jaundice: A systematic review and meta-analysis. Cancer Imaging 2017, 17, 27. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-L.; Wu, S.-H.; Hsu, S.-H.; Liou, B.-Y.; Chen, H.-L.; Chang, M.-H. Jaundice revisited: Recent advances in the diagnosis and treatment of inherited cholestatic liver diseases. J. Biomed. Sci. 2018, 25, 75. [Google Scholar] [CrossRef] [Green Version]
- Portincasa, P.; Di Ciaula, A.; de Bari, O.; Garruti, G.; Palmieri, V.; Wang, D.-H. Management of gallstones and its related complications. Expert Rev. Gastroenterol. Hepatol. 2015, 10, 93–112. [Google Scholar] [CrossRef]
- Xu, J.; Yang, C. Cholecystectomy outcomes after endoscopic sphincterotomy in patients with choledocholithiasis: A meta-analysis. BMC Gastroenterol. 2020, 20, 229. [Google Scholar] [CrossRef]
- Elmunzer, J.B.; Noureldin, M.; Morgan, K.A.; Adams, D.B.; Coté, G.A.; Waljee, A.K. The Impact of Cholecystectomy After Endoscopic Sphincterotomy for Complicated Gallstone Disease. Am. J. Gastroenterol. 2017, 112, 1596–1602. [Google Scholar] [CrossRef]
- Khan, M.A.; Khan, Z.; Tombazzi, C.R.; Gadiparthi, C.; Lee-Smith, W.; Wilcox, C.M. Role of Cholecystectomy After Endoscopic Sphincterotomy in the Management of Choledocholithiasis in High-risk Patients: A systematic review and meta-analysis. J. Clin. Gastroenterol. 2018, 52, 579–589. [Google Scholar] [CrossRef]
- Modha, K. Clinical Approach to Patients With Obstructive Jaundice. Tech. Vasc. Interv. Radiol. 2015, 18, 197–200. [Google Scholar] [CrossRef]
- Jinfeng, Z.; Yin, Y.; Chi, Z.; Junye, G. Management of impacted common bile duct stones during a laparoscopic procedure: A Retrospective Cohort Study of 377 Consecutive Patients. Int. J. Surg. 2016, 32, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Wan, J.; Xu, S.P.; Liao, L. A retrospective analysis of clinical characteristics and mortality risks in elderly patients with acute cholecystitis and cholangitis. Zhong Hua Nei Ke Za Zhi 2019, 58, 415–418. [Google Scholar]
- Rizzo, A.; Ricci, A.D.; Frega, G.; Palloni, A.; De Lorenzo, S.; Abbati, F.; Mollica, V.; Tavolari, S.; Di Marco, M.; Brandi, G. How to Choose Between Percutaneous Transhepatic and Endoscopic Biliary Drainage in Malignant Obstructive Jaundice: An Updated Systematic Review and Meta-analysis. In Vivo 2020, 34, 1701–1714. [Google Scholar] [CrossRef] [PubMed]
- Perone, J.A.; Riall, T.S.; Olino, K. Palliative Care for Pancreatic and Periampullary Cancer. Surg. Clin. 2016, 96, 1415–1430. [Google Scholar] [CrossRef] [Green Version]
- Coelen, R.J.S.; Roos, E.; Wiggers, J.K.; Besselink, M.G.; Buis, C.I.; Busch, O.R.C.; Dejong, C.H.C.; van Delden, O.M.; van Eijck, C.H.J.; Fockens, P.; et al. Endoscopic versus percutaneous biliary drainage in patients with resectable perihilar cholangiocarcinoma: A multicentre, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2018, 3, 681–690. [Google Scholar] [CrossRef]
- Dasari, B.V.M.; Ionescu, M.I.; Pawlik, T.M.; Hodson, J.; Sutcliffe, R.P.; Roberts, K.J.; Muiesan, P.; Isaac, J.; Marudanayagam, R.; Mirza, D.F. Outcomes of surgical resection of gallbladder cancer in patients presenting with jaundice: A systematic review and meta-analysis. J. Surg. Oncol. 2018, 118, 477–485. [Google Scholar] [CrossRef]
- Popov, A.; Baryshev, A.; Bykov, M.I.; Petrovsky, A.N.; Lishchishin, V.Y.; Vagin, I.V.; Shchava, V.V.; Porkhanov, V.A. Outcomes of minimally invasive biliary decompression in obstructive jaundice. Khirurgiia 2018, 12, 50–56. [Google Scholar] [CrossRef]
- Kurniawan, J.; Hasan, I.; Gani, R.A.; Simadibrata, M. Mortality-related Factors in Patients with Malignant Obstructive Jaundice. Acta Med. Indones. 2016, 48, 282–288. [Google Scholar]
- Rees, J.; Mytton, J.; Evison, F.; Mangat, K.S.; Patel, P.; Trudgill, N. The outcomes of biliary drainage by percutaneous transhepatic cholangiography for the palliation of malignant biliary obstruction in England between 2001 and 2014: A retrospective cohort study. BMJ Open 2020, 10, e033576. [Google Scholar] [CrossRef]
- Cai, J.-S.; Qiang, S.; Bao-Bing, Y. Advances of recurrent risk factors and management of choledocholithiasis. Scand. J. Gastroenterol. 2016, 52, 34–43. [Google Scholar] [CrossRef]
- Silina, E.V.; Stupin, V.A.; Abramov, I.S.; Bolevich, S.B.; Deshpande, G.; Achar, R.R.; Sinelnikova, T.G. Oxidative Stress and Free Radical Processes in Tumor and Non-Tumor Obstructive Jaundice: Influence of Disease Duration, Severity and Surgical Treatment on Outcomes. Pathophysiology 2022, 29, 32–51. [Google Scholar] [CrossRef] [PubMed]
- Khokonov, M.A.; Silina, E.; Stupin, V.; Gakhramanov, T.V.; Bolevich, S.; Men’Shova, N.I.; Sinel’Nikova, T.G.; Balkizov, Z.Z. Free radical processes in patients with the acute calculous cholecystitis. Khirurgiia 2011, 2, 58–64. [Google Scholar]
- Prazdnikov, E.N.; Baranov, G.A.; Zinatulin, D.R.; Umyarov, R.K.; Shevchenko, V.P.; Nikolayev, N.M. Antegrade approach for cholangiolithiasis complicated by mechanical jaundice. Khirurgiia 2018, 1, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Savdan, M.; Cakir, M.; Vatansev, H.; Kucukkartallar, T.; Tekin, A.; Tavli, S. Preventing oxygen free radical damage by proanthocyanidin in obstructive jaundice. Turk. J. Surg. 2017, 33, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Badger, S.A.; Jones, C.; McCaigue, M.; Clements, B.W.; Parks, R.W.; Diamond, T.; McCallion, K.; Taylor, M.A. Cytokine response to portal endotoxaemia and neutrophil stimulation in obstructive jaundice. Eur. J. Gastroenterol. Hepatol. 2012, 24, 25–32. [Google Scholar] [CrossRef]
- Yang, R.; Zhu, S.; Pischke, S.E.; Haugaa, H.; Zou, X.; Tonnessen, T.I. Bile and circulating HMGB1 contributes to systemic inflammation in obstructive jaundice. J. Surg. Res. 2018, 228, 14–19. [Google Scholar] [CrossRef]
- Huh, C.W.; Jang, S.I.; Lim, B.J.; Kim, H.W.; Kim, J.K.; Park, J.S.; Kim, J.K.; Lee, S.J.; Lee, D.K. Clinicopathological features of choledocholithiasis patients with high aminotransferase levels without cholangitis: Prospective comparative study. Medicine 2016, 95, e5176. [Google Scholar] [CrossRef]
- Pavlidis, E.T.; Pavlidis, T.E. Pathophysiological consequences of obstructive jaundice and perioperative management. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 17–21. [Google Scholar] [CrossRef]
- Fukui, H. Increased Intestinal Permeability and Decreased Barrier Function: Does It Really Influence the Risk of Inflammation? Inflamm. Intest. Dis. 2016, 1, 135–145. [Google Scholar] [CrossRef]
- Yamada, S.; Noguchi, H.; Tanimoto, A. Critical and diverse in vivo roles of apoptosis signal-regulating kinase 1 in animal models of atherosclerosis and cholestatic liver injury. Histol. Histopathol. 2017, 32, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Labib, P.L.; Goodchild, G.; Pereira, S.P. Molecular Pathogenesis of Cholangiocarcinoma. BMC Cancer 2019, 19, 185. [Google Scholar] [CrossRef] [PubMed]
- Moura, F.A.; de Andrade, K.Q.; dos Santos, J.C.F.; Araújo, O.R.P.; Goulart, M.O.F. Antioxidant therapy for treatment of inflammatory bowel disease: Does it work? Redox Biol. 2015, 6, 617–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Andrade, K.Q.; Moura, F.A.; Dos Santos, J.M.; De Araújo, O.R.P.; De Farias Santos, J.C.; Goulart, M.O.F. Oxidative Stress and Inflammation in Hepatic Diseases: Therapeutic Possibilities of N-Acetylcysteine. Int. J. Mol. Sci. 2015, 16, 30269–30308. [Google Scholar] [CrossRef] [PubMed]
- Cichoz-Lach, H.; Michalak, A. Oxidative stress as a crucial factor in liver diseases. World J. Gastroenterol. 2014, 20, 8082–8091. [Google Scholar] [CrossRef]
- Silina, E.V.; Sobirovz, M.A.; Bolevich, S.; Stupin, V.A. Regularities of the Oxidative Stress Processes in Case of Bleedings from Acute and Chronic Ulcers of the Stomach and Duodenum. Online J. Biol. Sci. 2018, 18, 208–220. [Google Scholar] [CrossRef]
- Salehi-Abargouei, A.; Ghiasvand, R.; Hariri, M. Prebiotics, Prosynbiotics and Synbiotics: Can They Reduce Plasma Oxidative Stress Parameters? A Systematic Review. Probiotics Antimicrob. Proteins 2017, 9, 1–11. [Google Scholar] [CrossRef]
- Omidian, M.; Abdolahi, M.; Daneshzad, E.; Sedighiyan, M.; Aghasi, M.; Abdollahi, H.; Omidian, P.; Dabiri, S.; Mahmoudi, M.; Hadavi, S.; et al. The Effects of Resveratrol on Oxidative Stress Markers: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Endocrine, Metab. Immune Disord.-Drug Targets 2020, 20, 718–727. [Google Scholar] [CrossRef]
- Higgins, P.; Dawson, J.; Lees, K.R.; McArthur, K.; Quinn, T.J.; Walters, M.R. Xanthine Oxidase Inhibition For The Treatment Of Cardiovascular Disease: A Systematic Review and Meta-Analysis. Cardiovasc. Ther. 2011, 30, 217–226. [Google Scholar] [CrossRef]
- Romano, R.; Cristescu, S.M.; Risby, T.H.; Marczin, N. Lipid peroxidation in cardiac surgery: Towards consensus on biomonitoring, diagnostic tools and therapeutic implementation. J. Breath Res. 2017, 12, 027109. [Google Scholar] [CrossRef]
- Zabel, M.; Nackenoff, A.; Kirsch, W.M.; Harrison, F.E.; Perry, G.; Schrag, M. Markers of oxidative damage to lipids, nucleic acids and proteins and antioxidant enzymes activities in Alzheimer’s disease brain: A meta-analysis in human pathological specimens. Free Radic. Biol. Med. 2017, 115, 351–360. [Google Scholar] [CrossRef]
- Wang, L.; Yu, W.-F. Obstructive jaundice and perioperative management. Acta Anaesthesiol. Taiwanica 2014, 52, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Cecilia, D.; Reyes-Díaz, M.; Ruiz-Rabelo, J.; Gomez-Alvarez, M.; Villanueva, C.M.; Álamo, J.; Muntané, J.; Padillo, F.J. Oxidative stress influence on renal dysfunction in patients with obstructive jaundice: A case and control prospective study. Redox Biol. 2016, 8, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assimakopoulos, S.F.; Scopa, C.D.; Vagianos, C.E. Pathophysiology of increased intestinal permeability in obstructive jaundice. World J. Gastroenterol. 2007, 13, 6458–6464. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wu, F.; Long, Y.; Yu, W. Glutathione Supplementation Attenuates Oxidative Stress and Improves Vascular Hyporesponsiveness in Experimental Obstructive Jaundice. Oxidative Med. Cell. Longev. 2015, 2015, 486148. [Google Scholar] [CrossRef] [Green Version]
- Long, Y.; Dong, X.; Yuan, Y.; Huang, J.; Song, J.; Sun, Y.; Lu, Z.; Yang, L.; Yu, W. Metabolomics changes in a rat model of obstructive jaundice: Mapping to metabolism of amino acids, carbohydrates and lipids as well as oxidative stress. J. Clin. Biochem. Nutr. 2015, 57, 50–59. [Google Scholar] [CrossRef] [Green Version]
- Atalay, E.; Ozdemir, M.T.; Tur, B.K.; Erdogdu, H.I.; Sisman, P. The effect of alpha-lipoic acid on oxidative parameters and liver injury in rats with obstructive jaundice. Bratisl. Med. J. 2019, 120, 843–848. [Google Scholar] [CrossRef] [Green Version]
- Bolevich, S.; Stupin, V.; Gakhramanov, T.V.; Khokonov, M.A.; Silina, E.; Men’Shova, N.I.; Bogdanova, L.S. Free radical processes at patients with pathologies of biliary ducts and methods of their correction. Khirurgiia 2010, 7, 65–70. [Google Scholar]
- Moole, H.; Bechtold, M.; Puli, S.R. Efficacy of preoperative biliary drainage in malignant obstructive jaundice: A meta-analysis and systematic review. World J. Surg. Oncol. 2016, 14, 182. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.-Z.; Wang, X.-B. Effects of biliary drainage on the intestinal barrier function in obstructive jaundice. Hepatogastroenterology 2013, 60, 1284–1288. [Google Scholar] [CrossRef]
- Chen, D.; Liang, L.-J.; Peng, B.-G.; Zhou, Q.; Li, S.-Q.; Tang, D.; Huang, L.; Huang, J.-F. Effect of preoperative biliary drainage on liver function changes in patients with malignant obstructive jaundice in the low bile duct before and after pancreaticoduodenectomy. Ai Zheng 2008, 27, 78–82. [Google Scholar]
- Fang, Y.; Gurusamy, K.S.; Wang, Q.; Davidson, B.R.; Lin, H.; Xie, X.; Wang, C. Pre-operative biliary drainage for obstructive jaundice. Cochrane Database Syst. Rev. 2012, 9, CD005444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gridasov, I.M.; Goroshinskaya, I.A.; Ushakova, N.D.; Leonova, A.V.; Maksimov, A.Y. Dynamics of oxidative stress and the state of antioxidant potential in patients with mechanical jaundice of tumor genesis during correction of bile outflow. Modern Probl. Sci. Educ. 2013, 5, 297. [Google Scholar]
- Mailloux, R.J. Teaching the fundamentals of electron transfer reactions in mitochondria and the production and detection of reactive oxygen species. Redox Biol. 2015, 4, 381–398. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Qu, J.; Chen, H.; Ge, P.; Jiang, Y.; Xu, C.; Chen, H.; Shang, D.; Zhang, G. The pathogenesis of renal injury in obstructive jaundice: A review of underlying mechanisms, inducible agents and therapeutic strategies. Pharmacol. Res. 2020, 163, 105311. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| I Comparison Group (n = 61) | II Group AOT (n = 52) | p-Value | Total (n = 113) | |
|---|---|---|---|---|
| Distribution of patients by sex | ||||
| Men | 23 (37.7%) | 24 (46.2%) | 0.364 | 47 (41.6%) |
| Women | 38 (62.3%) | 28 (53.8%) | 66 (58.4%) | |
| Distribution by age, years | ||||
| ≤50 | 10 (16.4%) | 3 (5.8%) | 0.158 | 13 (11.5%) |
| 50–64 | 11 (18.0%) | 11 (21.1%) | 22 (19.5%) | |
| 65–79 | 21 (34.4%) | 26 (50.0%) | 47 (41.6%) | |
| ≥ 80 | 19 (31.3%) | 12 (23.1%) | 31 (27.4%) | |
| Average age | 67.2 ± 16.5 71 [57:81] | 69.4 ± 14.6 75 [61:79] | 0.556 | 68.2 ± 15.6 72 [58:80] |
| Distribution of patients by the severity of the condition (on the SOFA scale) at hospitalization | ||||
| <4 points (n;%) | 33 (54.1%) | 30 (57.7%) | 0.709 | 63 (55.8%) |
| ≥4 points (n;%) | 28 (45.9%) | 22 (42.3%) | 50 (44.2%) | |
| Distribution of patients according to the severity of jaundice upon admission (according to the level of total bilirubin, μmol/L) | ||||
| <100 μmol/L | 22 (36.1%) | 15 (28.8%) | 0.284 | 37 (32.7%) |
| 100–150 μmol/L | 13 (21.3%) | 18 (34.6%) | 31 (27.4%) | |
| >150 μmol/L | 26 (42.6%) | 19 (36.5%) | 45 (39.8%) | |
| Distribution of patients by the etiology of obstructive jaundice | ||||
| Neoplastic jaundice | 18 (29.5%) | 15 (28.8%) | 0.939 | 33 (29.2%) |
| Non-neoplastic jaundice | 43 (70.5%) | 37 (71.2%) | 80 (70.8%) | |
| Including: | 0.597 | |||
| Cholelithiasis | 17 (27.9%) | 17 (32.7%) | 34 (30.1%) | |
| Cholangitis | 6 (9.8%) | 8 (15.4%) | 14 (12.4%) | |
| Acute pancreatitis | 5 (8.2%) | 5 (9.6%) | 10 (8.8%) | |
| Distal choledoch stenosis | 15 (24.6%) | 7 (13.5%) | 22 (19.5%) | |
| Duration of clinical manifestations of jaundice at the time of hospitalization (self-reported and/or referred by a caregiver) | ||||
| 0–2 days | 15 (24.6%) | 13 (25.0%) | 0.673 | 28 (24.8%) |
| 3–7 days | 28 (45.9%) | 20 (38.5%) | 48 (42.5%) | |
| >7 days | 18 (29.5%) | 19 (36.5%) | 37 (32.7%) | |
| Stay in intensive care units | ||||
| No | 35 (57.4%) | 32 (61.5%) | 0.654 | 67 (59.3%) |
| Were | 26 (42.6%) | 20 (38.5%) | 46 (40.7%) | |
| Surgical treatments for obstructive jaundice | ||||
| Endoscopic papillo-sphincterotomy | 27 (44.3%) | 30 (57.7%) | 0.560 | 57 (50.4%) |
| Nasobiliary drainage + stenting | 12 (19.7%) | 10 (19.2%) | 22 (19.5%) | |
| Cholecystostomy and cholecystectomy with drainage, | 22 (36.1%) | 12 (23.1%) | 34 (30.1%) | |
| Including: | ||||
| Microcholecystostomy/Gallbladder puncture | 13 (21.3%) | 4 (7.7%) | 17 (15.0%) | |
| Cholecystectomy + drainage | 9 (14.8%) | 8 (15.4%) | 17 (15.0%) | |
| Outcome | n, % | <4 Points on SOFA | ≥4 Points on SOFA | Total |
|---|---|---|---|---|
| Survivors | n | 61 | 39 | 100 |
| % Outcome | 61.0% | 39.0% | 100% | |
| % SOFA | 96.8% | 78.0% | 88.5% | |
| Dead | n | 2 | 11 | 13 |
| % Outcome | 15.4% | 84.6% | 100% | |
| % SOFA | 3.2% | 22.0% | 11.5% |
| Indicator | Day | Comparison Group (n = 61) | Antioxidant Therapy (n = 52) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Total bilirubin, μmol/L | 0 | 129.7 73.8/193.1 | 129.0 94.5/189.0 | 0.641 | |||
| 3 | 47.4 23.0/152.9 | 41.5 21.9/101.2 | 0.257 | ||||
| 8 | 46.0 21.1/78.0 | 25.8 13.7/63.9 | 0.031 | ||||
| Non-tumor | Tumor | Non-tumor | Tumor | Non-tumor | Tumor | ||
| 1 | 118 69/192 | 162 84.2/296 | 114 82/141 | 189 156.7/406 | 0.806 | 0.193 | |
| 3 | 29.2 21.2/58 | 112.6 73/224.3 | 30.4 21.1/55.7 | 136.1 80.4/165.1 | 0.519 | 0.354 | |
| 8 | 24.4 19.6/60.1 | 138.4 62.4/235 | 20.8 13.0/34.9 | 73.1 52.4/114.5 | 0.047 | 0.135 | |
| Direct bilirubin, μmol/L | 0 | 90.3 50.5/147.0 | 81.5 49.7/149.5 | 0.915 | |||
| 3 | 44.1 14.7/75.7 | 19.7 9.9/35.7 | 0.008 | ||||
| 8 | 25.8 12.5/71.0 | 10.5 7.0/23.1 | 0.0001 | ||||
| Non-tumor | Tumor | Non-tumor | Tumor | Non-tumor | Tumor | ||
| 1 | 87.9 49.8/109 | 134 51.5/228.2 | 76.1 47.0/107.0 | 163 87.7/351 | 0.493 | 0.181 | |
| 3 | 20.1 12.6/52.0 | 64.4 54.5/131.7 | 12.0 8.7/21.7 | 59.1 30.2/96.4 | 0.005 | 0.384 | |
| 8 | 18.3 8.3/30.6 | 68.4 46.4/147.3 | 8.3 6.6/12.8 | 23.9 18.8/43.4 | 0.004 | 0.004 | |
| Indirect bilirubin, μmol/L | 0 | 32.6 19.0/83.3 | 34.1 21.5/60.6 | 0.807 | |||
| 3 | 25.4 11.3/73.4 | 28.6 13.6/43.6 | 0.980 | ||||
| 8 | 22.0 13.7/35.3 | 18.6 12.0/39.3 | 0.520 | ||||
| Non-tumor | Tumor | Non-tumor | Tumor | Non-tumor | Tumor | ||
| 1 | 29.0 21.1/69.5 | 75.4 16/96.8 | 29.1 19.0/47.0 | 63.1 40.5/89 | 0.508 | 0.828 | |
| 3 | 15.8 7.4/29.5 | 82.6 29.1/149 | 17.4 9.7/31.2 | 57 38.4/80.8 | 0.647 | 0.384 | |
| 8 | 15.1 11.2/22.9 | 61.2 22.3/148.8 | 14.3 10.1/23.9 | 49.2 31.4/70.8 | 0.836 | 0.401 | |
| Alanine aminotransferase, U/L | 1 | 189.2 103.3/293.8 | 193.4 118.9/261.2 | 0.951 | |||
| 3 | 68.3 51.0/130 | 71.2 52.5/140.3 | 0.914 | ||||
| 8 | 68.3 41.9/94.5 | 48.6 31.1/75.9 | 0.045 | ||||
| Non-tumor | Tumor | Non-tumor | Tumor | Non-tumor | Tumor | ||
| 1 | 211.7 87.0/332.0 | 178.1 119.5/269.4 | 225.6 123.9/286.2 | 176.0 82.7/213 | 0.698 | 0.587 | |
| 3 | 80.1 55.4/139 | 62.3 45.4/122.5 | 64.8 54.4/144.6 | 77.6 45.3/131.3 | 0.961 | 0.955 | |
| 8 | 69.2 39.4/91.3 | 68.3 50.4/137.1 | 53.1 31.9/81.4 | 46.7 30.7/71.4 | 0.109 | 0.156 | |
| Aspartate aminotransferase, U/L | 1 | 127 96.7/195.5 | 113 80.5/209.4 | 0.386 | |||
| 3 | 67 43.2/92 | 58 42.1/93.7 | 0.002 | ||||
| 8 | 63.3 36/97 | 38.9 27.4/58.3 | 0.013 | ||||
| Non-tumor | Tumor | Non-tumor | Tumor | Non-tumor | Tumor | ||
| 1 | 121.8 94/195.4 | 132.9 102/170 | 119.0 85/219 | 88.9 59.7/146.5 | 0.954 | 0.097 | |
| 3 | 64.5 40/69 | 67.6 55/77.3 | 58 42/90.4 | 60.4 45.9/118.4 | 0.771 | 0.865 | |
| 8 | 65.6 34.6/85.2 | 63.3 44.8/116.2 | 36.9 29.9/53.7 | 43.3 26.4/60.7 | 0.025 | 0.047 | |
| Day | Comparison Group (n = 61) | Antioxidant Therapy (n = 52) | p-Value | |||
|---|---|---|---|---|---|---|
| 1 | 7.3 5.7/10.9 | 7.5 5.8/10.3 | 0.972 | |||
| 3 | 7.6 5.8/11.2 | 6.7 5.0/8.4 | 0.049 | |||
| 8 | 8.1 5.7/12.2 | 6.3 5.0/9.0 | 0.022 | |||
| Non-tumor | Tumor | Non-tumor | Tumor | Non-tumor | Tumor | |
| 1 | 7.3 5.9/11.6 | 7.3 5.7/7.7 | 7.5 6.0/10.6 | 7.1 5.1/9.6 | 0.912 | 0.814 |
| 3 | 7.6 5.8/11.4 | 7.7 6.0/8.6 | 6.5 5.1/7.6 | 7.4 5.2/9.7 | 0.116 | 0.760 |
| 8 | 8.1 5.7/12.8 | 7.8 5.9/10.7 | 6.0 5.3/8.5 | 8.0 4.6/9.9 | 0.030 | 0.476 |
| Indicator | Day | Comparison Group (n = 61) | Antioxidant Therapy (n = 52) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Lactate dehydrogenase (N: 130–230 U/L) | 1 | 497 357/573 | 472 361/579 | 0.994 | |||
| 3 | 423 342/521 | 454 374/559 | 0.362 | ||||
| 8 | 544 345/603 | 410 353/459 | 0.046 | ||||
| Non-tumor | Tumor | Non-tumor | Tumor | Non-tumor | Tumor | ||
| 1 | 438 352/615 | 528 451/542 | 468 377/577 | 474 349/586 | 0.803 | 0.872 | |
| 3 | 404 342/485 | 544 354/606 | 440 361/508 | 553 454/664 | 0.501 | 0.479 | |
| 8 | 435 340/589 | 574 367/615 | 411 363/452 | 405 333/428 | 0.457 | 0.048 | |
| Glucose (N: 2.3–6.0 mmol/L on an empty stomach) | 1 | 5.4 4.5/6.3 | 5.9 5.0/7.2 | 0.160 | |||
| 3 | 5.9 5.3/7.0 | 6.0 5.2/7.1 | 0.756 | ||||
| 8 | 6.2 4.7/8.6 | 5.85 5.4/6.5 | 0.639 | ||||
| Non-tumor | Tumor | Non-tumor | Tumor | Non-tumor | Tumor | ||
| 1 | 5.6 4.6/6.3 | 4.8 4.4/6.4 | 5.8 5.3/6.8 | 6.2 4.6/7.3 | 0.506 | 0.401 | |
| 3 | 5.7 4.8/6.3 | 6.6 5.6/11.3 | 5.7 5.0/6.7 | 7.3 6.3/7.7 | 0.770 | 0.654 | |
| 8 | 5.3 4.6/6.4 | 7.2 6.5/13.9 | 5.6 5.0/6.1 | 6.4 5.7/7.1 | 0.352 | 0.037 | |
| Outcome | I Comparison Group (n =61) | II AOT Group (n = 52) | p-Value | Total (n = 113) |
|---|---|---|---|---|
| Discharged | 50 (82.0%) | 50 (96.2%) | 0.018 | 100 (88.5%) |
| Dead | 11 (18.0%) | 2 (3.8%) | 13 (11.5%) | |
| Non-tumor OJ | ||||
| Discharged Dead | 37 (86.0%) 6 (14.0%) | 35 (94.6%) 2 (5.4%) | 0.204 | 72 (90.0%) 8 (10.0%) |
| Tumor OJ | ||||
| Discharged Dead | 13 (72.2%) 5 (27.8%) | 15 (100.0%) 0 | 0.027 | 28 (84.8%) 5 (15.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stupin, V.; Abramov, I.; Gahramanov, T.; Kovalenko, A.; Manturova, N.; Litvitskiy, P.; Balkizov, Z.; Silina, E. Comparative Study of the Results of Operations in Patients with Tumor and Non-Tumor Obstructive Jaundice Who Received and Did Not Receive Antioxidant Therapy for the Correction of Endotoxemia, Glycolysis, and Oxidative Stress. Antioxidants 2022, 11, 1203. https://doi.org/10.3390/antiox11061203
Stupin V, Abramov I, Gahramanov T, Kovalenko A, Manturova N, Litvitskiy P, Balkizov Z, Silina E. Comparative Study of the Results of Operations in Patients with Tumor and Non-Tumor Obstructive Jaundice Who Received and Did Not Receive Antioxidant Therapy for the Correction of Endotoxemia, Glycolysis, and Oxidative Stress. Antioxidants. 2022; 11(6):1203. https://doi.org/10.3390/antiox11061203
Chicago/Turabian StyleStupin, Victor, Igor Abramov, Teymur Gahramanov, Alexey Kovalenko, Natalia Manturova, Petr Litvitskiy, Zalim Balkizov, and Ekaterina Silina. 2022. "Comparative Study of the Results of Operations in Patients with Tumor and Non-Tumor Obstructive Jaundice Who Received and Did Not Receive Antioxidant Therapy for the Correction of Endotoxemia, Glycolysis, and Oxidative Stress" Antioxidants 11, no. 6: 1203. https://doi.org/10.3390/antiox11061203