
Oxidative Stress and Inflammatory Markers in Abdominal Aortic Aneurysm

 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Samples
2.2. ELISA Kits
2.3. Total mRNA and Protein Isolation from Tissue
2.4. Quantitative Real-Time PCR
2.5. Immunostaining and Histology
2.6. Reactive Oxygen Species (ROS) Quantification in Plasma
2.7. Western Blot
2.8. Finite Element Analysis
2.9. Statistical Analysis
3. Results
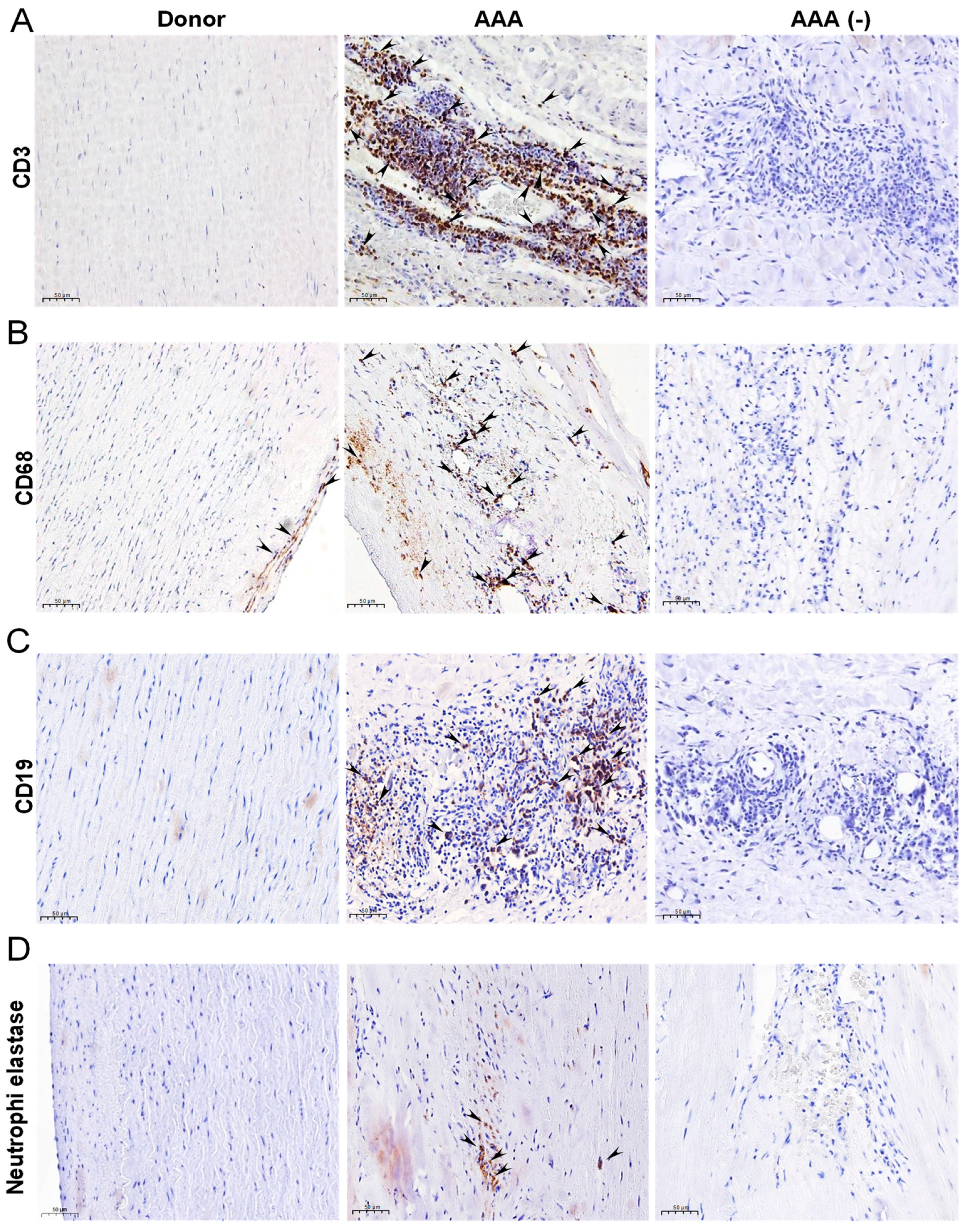
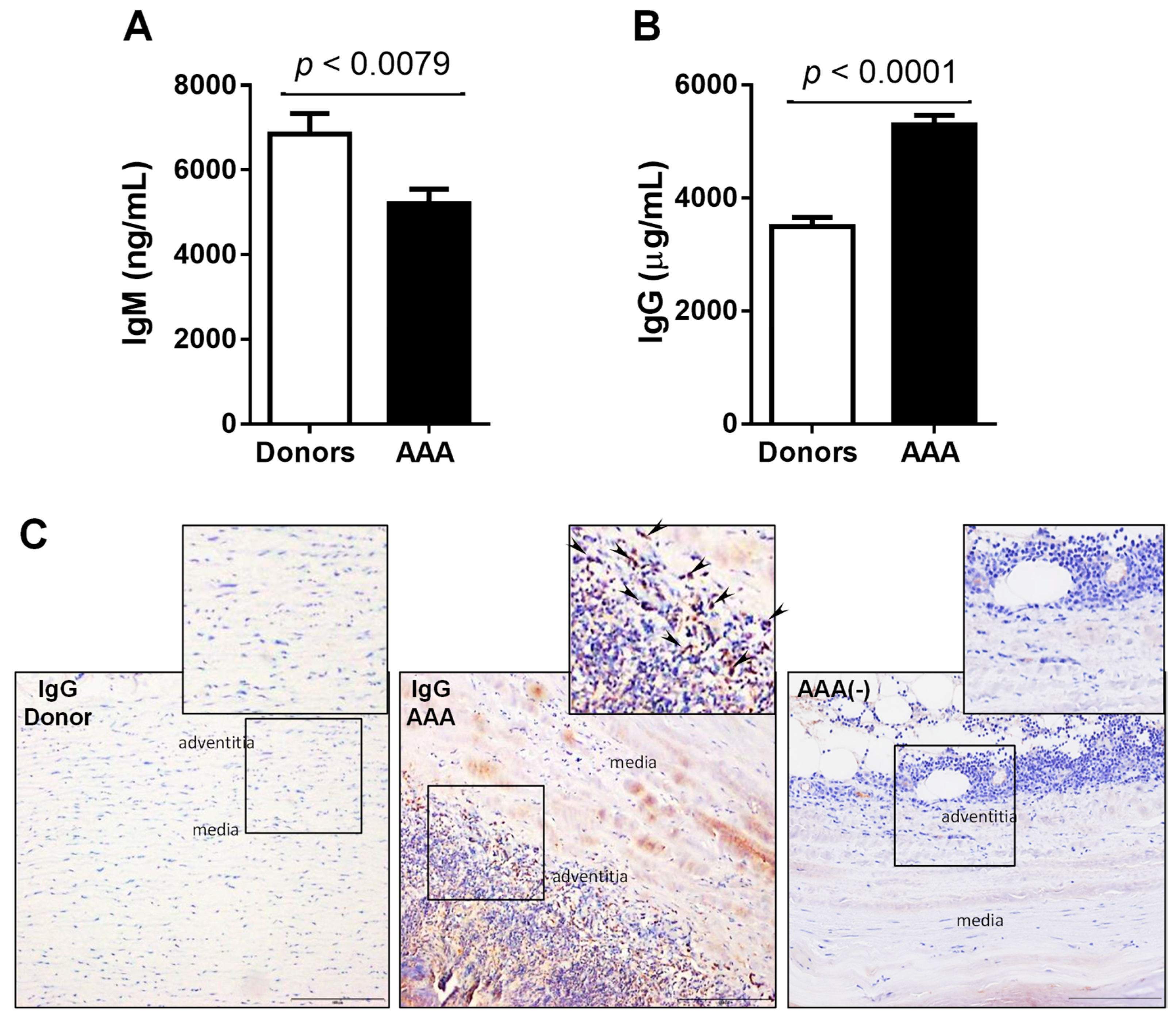
3.1. Immune Infiltrate and Immunoglobulins in Human AAA
3.2. Vascular and Circulating Levels of Oxidative Stress and Inflammation-Related Biomarkers in AAA Patients
3.3. Correlation of Biomarker Levels and Preoperative Aortic Diameter
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nordon, I.M.; Hinchliffe, R.J.; Loftus, I.M.; Thompson, M.M. Pathophysiology and epidemiology of abdominal aortic aneurysms. Nat. Rev. Cardiol. 2011, 8, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ge Zhao, G.; Zhang, J.; Duan, Z.; Xin, S. Prevalence and trends of the abdominal aortic aneurysms epidemic in general population--a meta-analysis. PLoS ONE 2013, 8, e81260. [Google Scholar] [CrossRef]
- Brady, A.R.; Thompson, S.G.; Fowkes, F.G.; Greenhalgh, R.M.; Powell, J.T. UK Small Aneurysm Trial Participants. Abdominal aortic aneurysm expansion: Risk factors and time intervals for surveillance. Circulation 2004, 110, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Golledge, J.; Norman, P.E. Pathophysiology of abdominal aortic aneurysm relevant to improvements in patients’ management. Curr. Opin. Cardiol. 2009, 24, 532–538. [Google Scholar] [CrossRef]
- Kent, K.C. Clinical practice. Abdominal aortic aneurysms. N. Engl. J. Med. 2014, 371, 2101–2108. [Google Scholar] [CrossRef]
- Weintraub, N.L. Understanding abdominal aortic aneurysm. N. Engl. J. Med. 2009, 361, 1114–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, K.; Mitchell, R.N.; Libby, P. Inflammation and celular immune responses in abdominal aortic aneurysms. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 987–994. [Google Scholar] [CrossRef]
- Papalambros, E.; Sigala, F.; Georgopoulos, S.; Paraskevas, K.I.; Andreadou, I.; Menenakos, X.; Sigalas, P.; Papalambros, A.L.; Vourliotakis, G.; Giannopoulos, A.; et al. Malondialdehyde as an indicator of oxidative stress during abdominal aortic aneurysm repair. Angiology 2007, 58, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.J., Jr.; Sharp, W.J.; Fang, X.; Oberley, L.W.; Oberley, T.D.; Weintraub, N.L. Oxidative stress in human abdominal aortic aneurysms: A potential mediator of aneurysmal remodeling. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 560–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormick, M.L.; Gavrila, D.; Weintraub, N.L. Role of oxidative stress in the pathogenesis of abdominal aortic aneurysms. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 461–469. [Google Scholar] [CrossRef] [Green Version]
- Ocana, E.; Bohorquez, J.C.; Perez-Requena, J.; Brieva, J.A.; Rodríguez, C. Characterisation of T and B lymphocytes infiltrating abdominal aortic aneurysms. Atherosclerosis 2003, 170, 39–48. [Google Scholar] [CrossRef]
- Potteaux, S.; Tedgui, A. Monocytes, Macrophages and Other Inflammatory Mediators of Abdominal Aortic Aneurysm. Curr. Pharm. Des. 2015, 21, 4007–4015. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, Y. B lymphocytes in abdominal aortic aneurysms. Atherosclerosis 2015, 242, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Morandi, F.; Airoldi, I.; Marimpietri, D.; Bracci, C.; Faini, A.C.; Gramignoli, R. CD38, a Receptor with Multifunctional Activities: From Modulatory Functions on Regulatory Cell Subsets and Extracellular Vesicles, to a Target for Therapeutic Strategies. Cells 2019, 8, 1527. [Google Scholar] [CrossRef] [Green Version]
- Shu, B.; Feng, Y.; Gui, Y.; Lu, Q.; Wei, W.; Xue, X.; Sun, X.; He, W.; Yang, J.; Dai, C. Blockade of CD38 diminishes lipopolysaccharide-induced macrophage classical activation and acute kidney injury involving NF-κB signaling suppression. Cellular Signal. 2018, 42, 249–258. [Google Scholar] [CrossRef] [PubMed]
- de Toledo, F.G.; Cheng, J.; Liang, M.; Chini, E.N.; Dousa, T.P. ADP-Ribosyl cyclase in rat vascular smooth muscle cells: Properties and regulation. Circ. Res. 2000, 86, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Bai, N.; Lee, H.C.; Laher, I. Emerging role of cyclic ADP-ribose (cADPR) in smooth muscle. Pharmacol. Ther. 2005, 105, 189–207. [Google Scholar] [CrossRef]
- Vaisitti, T.; Serra, S.; Pepper, C.; Rossi, D.; Laurenti, L.; Gaidano, G.; Malavasi, F.; Deaglio, S. CD38 signals upregulate expression and functions of matrix metalloproteinase-9 in chronic lymphocytic leukemia cells. Leukemia 2013, 27, 1177–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corre, J.; He’braud, B.; Bourin, P. Concise review: Growth differentiation factor 15 in pathology: A clinical role? Stem Cells Transl. Med. 2013, 2, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Arkoumani, M.; Papadopoulou-Marketou, N.; Nicolaides, N.C.; Kanaka-Gantenbein, C.; Tentolouris, N.; Papassotiriou, I. The clinical impact of growth differentiation factor-15 in heart disease: A 2019 update. Crit. Rev. Clin. Lab. Sci. 2020, 57, 114–125. [Google Scholar] [CrossRef]
- Jia, L.X.; Zhang, W.M.; Zhang, H.J.; Li, T.T.; Wang, Y.L.; Qin, Y.W.; Gu, H.; Du, J. Mechanical stretch-induced endoplasmic reticulum stress, apoptosis and inflammation contribute to thoracic aortic aneurysm and dissection. J. Pathol. 2015, 236, 373–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambartsumian, N.; Klingelhöfer, J.; Grigorian, M. The Multifaceted S100A4 Protein in Cancer and Inflammation. Methods Mol. Biol. 2019, 1929, 339–365. [Google Scholar] [PubMed]
- Febbraio, M.; Hajjar, D.P.; Silverstein, R.L. CD36: A class B scavenger receptor involved in angiogenesis, atherosclerosis, inflammation, and lipid metabolism. J. Clin. Invest. 2001, 108, 785–791. [Google Scholar] [CrossRef]
- Navas-Madroñal, M.; Rodriguez, C.; Kassan, M.; Fité, J.; Escudero, J.R.; Cañes, L.; Martínez-González, J.; Camacho, M.; Galán, M. Enhanced endoplasmic reticulum and mitochondrial stress in abdominal aortic aneurysm. Clin. Sci. 2019, 133, 1421–1438. [Google Scholar] [CrossRef] [PubMed]
- Laurindo, F.R.; Fernandes, D.C.; Santos, C.X. Assessment of superoxide production and NADPH oxidase activity by HPLC analysis of dihydroethidium oxidation products. Methods Enzymol. 2008, 441, 237–260. [Google Scholar]
- Michalski, R.; Michalowski, B.; Sikora, A.; Zielonka, J.; Kalyanaraman, B. On the use of fluorescence lifetime imaging and dihydroethidium to detect superoxide in intact animals and ex vivo tissues: A reassessment. Free Radic. Biol. Med. 2014, 67, 278–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soto, B.; Vila, L.; Dilmé, J.F.; Escudero, J.R.; Bellmunt, S.; Camacho, M. Increased Peak Wall Stress, but Not Maximum Diameter, Is Associated with Symptomatic Abdominal Aortic Aneurysm. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 706–711. [Google Scholar] [CrossRef] [Green Version]
- Raffort, J.; Lareyre, F.; Clément, M.; Hassen-Khodja, R.; Chinetti, G.; Mallat, Z. Monocytes and macrophages in abdominal aortic aneurysm. Nat. Rev. Cardiol. 2017, 14, 457–471. [Google Scholar] [CrossRef]
- Li, H.; Bai, S.; Ao, Q.; Wang, X.; Tian, X.; Li, X.; Tong, H.; Hou, W.; Fan, J. Modulation of Immune-Inflammatory Responses in Abdominal Aortic Aneurysm: Emerging Molecular Targets. J. Immunol. Res. 2018, 2018, 7213760. [Google Scholar] [CrossRef]
- Xu, M.; Li, X.X.; Wang, L.; Wang, M.; Zhang, Y.; Li, P.L. Contribution of Nrf2 to Atherogenic Phenotype Switching of Coronary Arterial Smooth Muscle Cells Lacking CD38 Gene. Cell. Physiol. Biochem. 2015, 37, 432–444. [Google Scholar] [CrossRef]
- Li, W.; Febbraio, M.; Reddy, S.P.; Yu, D.Y.; Yamamoto, M.; Silverstein, R.L. CD36 participates in a signaling pathway that regulates ROS formation in murine VSMCs. J. Clin. Invest. 2010, 120, 3996–4006. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Seok, Y.M.; Jung, K.J.; Park, K.M. Reactive oxygen species/oxidative stress contributes to progression of kidney fibrosis following transient ischemic injury in mice. Am. J. Physiol. Ren. Physiol. 2009, 297, F461–F470. [Google Scholar] [CrossRef] [Green Version]
- Indrakusuma, R.; Jalalzadeh, H.; Planken, R.N.; Marquering, H.A.; Legemate, D.A.; Koelemay, M.J.W.; Balm, R. Biomechanical imaging markers as predictors of abdominal aortic aneurysm growth or rupture: A systematic review. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 475–486. [Google Scholar] [CrossRef] [Green Version]
- Gasser, T.C.; Auer, M.; Labruto, F.; Swedenborg, J.; Roy, J. Biomechanical rupture risk assessment of abdominal aortic aneurysms: Model complexity versus predictability of finite element simulations. Eur. J. Vasc. Endovasc. Surg. 2010, 40, 176–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzik, B.; Sagan, A.; Ludew, D.; Mrowiecki, W.; Chwała, M.; Bujak-Gizycka, B.; Filip, G.; Grudzien, G.; Kapelak, B.; Zmudka, K.; et al. Mechanisms of oxidative stress in human aortic aneurysms-association with clinical risk factors for atherosclerosis and disease severity. Int. J. Cardiol. 2013, 168, 2389–2396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawada, H.; Hao, H.; Naito, Y.; Oboshi, M.; Hirotani, S.; Mitsuno, M.; Miyamoto, Y.; Hirota, S.; Masuyama, T. Aortic iron overload with oxidative stress and inflammation in human and murine abdominal aortic aneurysm. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 1507–1514. [Google Scholar] [CrossRef] [Green Version]
- Emeto, T.I.; Moxon, J.V.; Au, M.; Golledge, J. Oxidative stress and abdominal aortic aneurysm: Potential treatment targets. Clin. Sci. 2016, 130, 301–315. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Inuzuka, K.; Iida, Y.; Shimizu, H.; Unno, N.; Urano, T. Proprotein Convertase Subtilisin/Kexin Type 9 Is Associated with Degenerating Adipocytes in Abdominal Aortic Aneurysm. J. Oleo. Sci. 2018, 67, 1355–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnaoutoglou, E.; Kouvelos, G.; Papa, N.; Karamoutsios, A.; Bouris, V.; Vartholomatos, G.; Matsagkas, M. Platelet activation after endovascular repair of abdominal aortic aneurysm. Vascular 2016, 24, 287–294. [Google Scholar] [CrossRef]
- Cao, J.; Geng, L.; Wu, Q.; Wang, W.; Chen, Q.; Lu, L.; Shen, W.; Chen, Y. Spatio temporal expression of matrix metalloproteinases (MMPs) is regulated by the Ca2+-signal transducer S100A4 in the pathogenesis of thoracic aortic aneurysm. PLoS ONE 2013, 8, e70057. [Google Scholar]
- Kyaw, T.; Tipping, P.; Bobik, A.; Toh, B.H. Protective role of natural IgM-producing B1a cells in atherosclerosis. Trends Cardiovasc. Med. 2012, 22, 48–53. [Google Scholar] [CrossRef]
- Su, J.; Hua, X.; Vikström, M.; Leander, K.; Gigante, B.; Hellenius, M.L.; de Faire, U.; Frostegård, J. Low levels of IgM antibodies to oxidized cardiolipin increase and high levels decrease risk of cardiovascular disease among 60-year olds: A prospective study. BMC Cardiovasc. Disord. 2013, 13, 1. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, S.M.; Perry, H.M.; Gonen, A.; Prohaska, T.A.; Srikakulapu, P.; Grewal, S.; Das, D.; McSkimming, C.; Taylor, A.M.; Tsimikas, S.; et al. B-1b Cells Secrete Atheroprotective IgM and Attenuate Atherosclerosis. Circ. Res. 2015, 117, e28–e39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, F.E. Cytokine-producing B lymphocytes-key regulators of immunity. Curr. Opin. Immunol. 2008, 20, 332–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furusho, A.; Hiroki, A.H.; Ohno-Urabe, S.; Nishihara, M.; Furusho, A.; Hirakata, S.; Hayashi, M.; Ito, S.; Yamada, H.; Hirata, Y.; et al. Involvement of B Cells, Immunoglobulins, and Syk in the Pathogenesis of Abdominal Aortic Aneurysm. J. Am. Heart. Assoc. 2018, 7, e007750. [Google Scholar] [CrossRef] [Green Version]
- Dutertre, C.A.; Clement, M.; Morvan, M.; Schäkel, K.; Castier, Y.; Alsac, J.M.; Michel, J.B.; Nicoletti, A. Deciphering the stromal and hematopoietic cell network of the adventitia from non-aneurysmal and aneurysmal human aorta. PLoS ONE 2014, 9, e89983. [Google Scholar]
- Sharma, N.; Dev, R.; Belenchia, A.M.; Aroor, A.R.; Whaley-Connell, A.; Pulakat, L.; Hans, C.P. Deficiency of IL12p40 (Interleukin 12 p40) Promotes Ang II (Angiotensin II)-Induced Abdominal Aortic Aneurysm. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 212–223. [Google Scholar] [CrossRef]
- Vats, D.; Mukundan, L.; Odegaard, J.I.; Zhang, L.; Smith, K.L.; Morel, C.R.; Wagner, R.A.; Greaves, D.R.; Murray, P.J.; Chawla, A. Oxidative metabolism and PGC-1beta attenuate macrophage mediated inflammation. Cell. Metab. 2006, 4, 13–24. [Google Scholar] [CrossRef] [Green Version]
- Odegaard, J.I.; Ricardo-Gonzalez, R.R.; Red Eagle, A.; Vats, D.; Morel, C.R.; Goforth, M.H.; Subramanian, V.; Mukundan, L.; Ferrante, A.W.; Chawla, A. Alternative M2 activation of Kupffer cells by PPARdelta ameliorates obesity-induced insulin resistance. Cell. Metab. 2008, 7, 496–507. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Dev, R.; Ruiz-Rosado, J.D.; Partida-Sanchez, S.; Guerau-de-Arellano, M.; Dhakal, P.; Kuivaniemi, H.; Hans, C.P. Pharmacological inhibition of Notch signaling regresses pre-established abdominal aortic aneurysm. Sci. Rep. 2019, 9, 13458. [Google Scholar] [CrossRef] [Green Version]
- Hogan, K.A.; Chini, C.C.S.; Chini, E.N. The Multi-faceted Ecto-enzyme CD38: Roles in Immunomodulation, Cancer, Aging, and Metabolic Diseases. Front. Immunol. 2019, 10, 1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanatani, S.; Izumiya, Y.; Takashio, S.; Kojima, S.; Yamamuro, M.; Araki, S.; Rokutanda, T.; Tsujita, K.; Yamamoto, E.; Tanaka, T.; et al. Growth differentiation factor 15 can distinguish between hypertrophic cardiomyopathy and hypertensive hearts. Heart Vessel. 2014, 29, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.A.; Wu, S.; Juang, J.J.; Chiang, F.T.; Teng, M.S.; Teng, M.S.; Lin, J.F.; Huang, H.L.; Ko, Y.L. Growth Differentiation Factor 15 May Predict Mortality of Peripheral and Coronary Artery Diseases and Correlate with Their Risk Factors. Mediat. Inflamm. 2017, 2017, 9398401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bettencourt, P.; Ferreira-Coimbra, J.; Rodrigues, P.; Marques, P.; Moreira, H.; Pinto, M.J.; Guimarães, J.T.; Lourenço, P. Towards a Multi-Marker Prognostic Strategy in Acute Heart Failure: A Role for GDF-15. ESC. Heart Fail. 2018, 5, 1017–1022. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhu, L.; Wu, Y.; Sun, K.; Yu, L.; Chen, J.; Li, W.; Yang, J.; Yuan, Z.; Hui, R. Plasma growth differentiation factor 15 predicts first-ever stroke in hypertensive patients. Medicine 2016, 95, e4342. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| mRNA | Plasma | |||
|---|---|---|---|---|
| AAA | Normal Aorta | AAA | Blood Donors | |
| N | 80 | 15 | 94 | 46 |
| Age (years) | 70 ± 6.2 | 63 ± 11.5 | 71.4 ± 6.5 | 59.9 ± 5.3 * |
| Women (%, N) | 5 (4) | 20 (3) | 4.3 (4) | 10.9 (5) |
| Aortic diameter (mm) | 63.5 ± 1.4 | - | 63.9 ± 1.4 | - |
| Dyslipidemia (%, N) | 56.3 (45) | 26.7 (4) | 63.8 (60) | - |
| HTN (%, N) | 81.25 (66) | 40 (6) | 77.6 (73) | 19.6 (9) |
| Diabetes (%, N) | 21.25 (17) | 33.3 (5) | 19.1 (18) | 23.91 (11) |
| Smokers/ex-smokers (%, N) | 81.25 (66) | 40 (6) | 80.1 (76) | 45.7 (21) |
| PWS (kPa) TC (mM) | 222 ± 74.8 - | - - | 222 ± 74.8 3.9 ± 1.2 | - 5.6 ± 0.8 |
| HDL-C (mM) | - | - | 1 ± 0.3 | 1.5 ± 0.3 |
| LDL-C (mM) | - | - | 2.3 ± 0.9 | 3.5 ± 0.7 |
| VLDL-C (mM) | - | - | 0.6 ± 0.3 | 0.6 ± 0.3 |
| Triglycerides (mM) | - | - | 1.3 ± 0.7 | 1.4 ± 0.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Infantes, D.; Nus, M.; Navas-Madroñal, M.; Fité, J.; Pérez, B.; Barros-Membrilla, A.J.; Soto, B.; Martínez-González, J.; Camacho, M.; Rodriguez, C.; et al. Oxidative Stress and Inflammatory Markers in Abdominal Aortic Aneurysm. Antioxidants 2021, 10, 602. https://doi.org/10.3390/antiox10040602
Sánchez-Infantes D, Nus M, Navas-Madroñal M, Fité J, Pérez B, Barros-Membrilla AJ, Soto B, Martínez-González J, Camacho M, Rodriguez C, et al. Oxidative Stress and Inflammatory Markers in Abdominal Aortic Aneurysm. Antioxidants. 2021; 10(4):602. https://doi.org/10.3390/antiox10040602
Chicago/Turabian StyleSánchez-Infantes, David, Meritxell Nus, Miquel Navas-Madroñal, Joan Fité, Belén Pérez, Antonio J. Barros-Membrilla, Begoña Soto, José Martínez-González, Mercedes Camacho, Cristina Rodriguez, and et al. 2021. "Oxidative Stress and Inflammatory Markers in Abdominal Aortic Aneurysm" Antioxidants 10, no. 4: 602. https://doi.org/10.3390/antiox10040602