
Depleted Myocardial Coenzyme Q10 in Cavalier King Charles Spaniels with Congestive Heart Failure Due to Myxomatous Mitral Valve Disease

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dogs
2.2. Clinical Examination and Sample Collection
2.3. Clinical Classification
2.4. Q10 Analyses
2.5. Citrate Synthase
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bentinger, M.; Brismar, K.; Dallner, G. The antioxidant role of coenzyme Q. Mitochondrion 2007, 7, S41–S50. [Google Scholar] [CrossRef]
- Pravst, I.; Zmitek, K.; Zmitek, J. Coenzyme Q10 contents in foods and fortification strategies. Crit. Rev. Food Sci. Nutr. 2010, 50, 269–280. [Google Scholar] [CrossRef]
- Bhagavan, H.N.; Chopra, R.K. Plasma coenzyme Q10 response to oral ingestion of coenzyme Q10 formulations. Mitochondrion 2007, 7, S78–S88. [Google Scholar] [CrossRef]
- Barth, E.; Stämmler, G.; Speiser, B.; Schaper, J. Ultrastructural quantitation of mitochondria and myofilaments in cardiac muscle from 10 different animal species including man. J. Mol. Cell. Cardiol. 1992, 24, 669–681. [Google Scholar] [CrossRef]
- Park, S.-Y.; Gifford, J.R.; Andtbacka, R.H.I.; Trinity, J.D.; Hyngstrom, J.R.; Garten, R.S.; Diakos, N.A.; Ives, S.J.; Dela, F.; Larsen, S.; et al. Cardiac, skeletal, and smooth muscle mitochondrial respiration: Are all mitochondria created equal? AJP Hear. Circ. Physiol. 2014, 307, H346–H352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, S.; Nielsen, J.; Hansen, C.N.; Nielsen, L.B.; Wibrand, F.; Stride, N.; Schroder, H.D.; Boushel, R.; Helge, J.W.; Dela, F.; et al. Biomarkers of mitochondrial content in skeletal muscle of healthy young human subjects. J. Physiol. 2012, 590, 3349–3360. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, H.; Hoppel, C.L. Mitochondria in the human heart. J. Bioenerg. Biomembr. 2009, 41, 99–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stride, N.; Larsen, S.; Hey-Mogensen, M.; Sander, K.; Lund, J.T.; Gustafsson, F.; Køber, L.; Dela, F. Decreased mitochondrial oxidative phosphorylation capacity in the human heart with left ventricular systolic dysfunction. Eur. J. Heart Fail. 2013, 15, 150–157. [Google Scholar] [CrossRef]
- Folkers, K.; Vadhanavikit, S.; Mortensen, S.A. Biochemical rationale and myocardial tissue data on the effective therapy of cardiomyopathy with coenzyme Q10. Proc. Natl. Acad. Sci. USA 1985, 82, 901–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, J.; Sylvén, C.; Jansson, E.; Böök, K.; Muratsu, K.; Folkers, K. Coenzyme Q10 and key enzyme activities in papillary muscle related to left ventricle function in mitral valve disease. Mol. Cell. Biochem. 1988, 84, 59–64. [Google Scholar] [CrossRef]
- Madmani, M.E.; Yusuf Solaiman, A.; Tamr Agha, K.; Madmani, Y.; Shahrour, Y.; Essali, A.; Kadro, W. Coenzyme Q10 for heart failure. Cochrane Database Syst. Rev. 2014, 2014, CD008684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, L.; Liu, Y. Efficacy of coenzyme Q10 in patients with cardiac failure: A meta-analysis of clinical trials. BMC Cardiovasc. Disord. 2017, 17, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortensen, S.A.; Rosenfeldt, F.; Kumar, A.; Dolliner, P.; Filipiak, K.J.; Pella, D.; Alehagen, U.; Steurer, G.; Littarru, G.P. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: Results from Q-SYMBIO: A randomized double-blind trial. JACC Hear. Fail. 2014, 2, 641–649. [Google Scholar] [CrossRef]
- Buchanan, J.W. Chronic valvular disease (endocardiosis) in dogs. Adv. Vet. Sci. Comp. Med. 1977, 21, 75–106. [Google Scholar] [PubMed]
- Detweiler, D.K.; Patterson, D.F. The prevalence and types of cardiovascular disease in dogs. Ann. N. Y. Acad. Sci. 1965, 127, 481–516. [Google Scholar] [CrossRef] [PubMed]
- Egenvall, A.; Bonnett, B.N.; Häggström, J. Heart disease as a cause of death in insured Swedish dogs younger than 10 years of age. J. Vet. Intern. Med. 2006, 20, 894–903. [Google Scholar] [CrossRef]
- Häggström, J.; Hansson, K.; Kvart, C.; Swenson, L. Chronic valvular disease in the cavalier King Charles spaniel in Sweden. Vet. Rec. 1992, 131, 549–553. [Google Scholar]
- Zois, N.E.; Olsen, N.T.; Moesgaard, S.G.; Rasmussen, C.E.; Falk, T.; Haggstrom, J.; Pedersen, H.D.; Moller, J.E.; Olsen, L.H. Left ventricular twist and circumferential strain in dogs with myxomatous mitral valve disease. J. Vet. Intern. Med. 2013, 27, 875–883. [Google Scholar] [CrossRef]
- Rasmussen, C.E.; Falk, T.; Zois, N.E.; Moesgaard, S.G.; Häggström, J.; Pedersen, H.D.; Ablad, B.; Nilsen, H.Y.; Olsen, L.H. Heart rate, heart rate variability, and arrhythmias in dogs with myxomatous mitral valve disease. J. Vet. Intern. Med. 2012, 26, 76–84. [Google Scholar] [CrossRef]
- Rasmussen, C.E.; Falk, T.; Domanjko Petrič, A.; Schaldemose, M.; Zois, N.E.; Moesgaard, S.G.; Åblad, B.; Nilsen, H.Y.; Ljungvall, I.; Höglund, K.; et al. Holter monitoring of small breed dogs with advanced myxomatous mitral valve disease with and without a history of syncope. J. Vet. Intern. Med. 2014, 28, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Zois, N.E.; Moesgaard, S.G.; Kjelgaard-Hansen, M.; Rasmussen, C.E.; Falk, T.; Fossing, C.; Häggström, J.; Pedersen, H.D.; Olsen, L.H. Circulating cytokine concentrations in dogs with different degrees of myxomatous mitral valve disease. Vet. J. 2012, 192, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Cremer, S.E.; Singletary, G.E.; Olsen, L.H.; Wallace, K.; Häggström, J.; Ljungvall, I.; Höglund, K.; Reynolds, C.A.; Pizzinat, N.; Oyama, M.A. Serotonin concentrations in platelets, plasma, mitral valve leaflet, and left ventricular myocardial tissue in dogs with myxomatous mitral valve disease. J. Vet. Intern. Med. 2014, 28, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Cremer, S.E.; Kristensen, A.T.; Reimann, M.J.; Eriksen, N.B.; Petersen, S.F.; Marschner, C.B.; Tarnow, I.; Oyama, M.A.; Olsen, L.H. Plasma and serum serotonin concentrations and surface-bound platelet serotonin expression in cavalier king charles spaniels with myxomatous mitral valve disease. Am. J. Vet. Res. 2015, 76, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Zois, N.E.; Tidholm, A.; Nägga, K.M.; Moesgaard, S.G.; Rasmussen, C.E.; Falk, T.; Häggström, J.; Pedersen, H.D.; Åblad, B.; Nilsen, H.Y.; et al. Radial and longitudinal strain and strain rate assessed by speckle-tracking echocardiography in dogs with myxomatous mitral valve disease. J. Vet. Intern. Med. 2012, 26, 1309–1319. [Google Scholar] [CrossRef]
- Thomas, W.P.; Gaber, C.E.; Jacobs, G.J.; Kaplan, P.M.; Lombard, C.W.; Vet, M.; Moise, N.S.; Moses, B.L. Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat. J. Vet. Intern. Med. 1993, 7, 247–252. [Google Scholar] [CrossRef]
- Reimann, M.J.; Møller, J.E.; Häggström, J.; Markussen, B.; Holen, A.E.W.; Falk, T.; Olsen, L.H. R-R interval variations influence the degree of mitral regurgitation in dogs with myxomatous mitral valve disease. Vet. J. 2014, 199, 348–354. [Google Scholar] [CrossRef]
- Boswood, A.; Häggström, J.; Gordon, S.G.; Wess, G.; Stepien, R.L.; Oyama, M.A.; Keene, B.W.; Bonagura, J.; MacDonald, K.A.; Patteson, M.; et al. Effect of pimobendan in dogs with preclinical myxomatous mitral valve disease and cardiomegaly: The EPIC study—A randomized clinical trial. J. Vet. Intern. Med. 2016, 30, 1765–1779. [Google Scholar] [CrossRef]
- Keene, B.W.; Atkins, C.E.; Bonagura, J.D.; Fox, P.R.; Häggström, J.; Fuentes, V.L.; Oyama, M.A.; Rush, J.E.; Stepien, R.; Uechi, M. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J. Vet. Intern. Med. 2019, 33, 1127–1140. [Google Scholar] [CrossRef]
- Gompf, R.E. The Clinical Approach to Heart Disease: History and Physical Examination; Fox, P.R., Ed.; Churchill Livingstone Inc.: New York, NY, USA, 1988. [Google Scholar]
- Häggström, J.; Hansson, K.; Karlberg, B.E.; Kvart, C.; Olsson, K. Plasma concentration of atrial natriuretic peptide in relation to severity of mitral regurgitation in Cavalier King Charles Spaniels. Am. J. Vet. Res. 1994, 55, 698–703. [Google Scholar]
- Cornell, C.C.; Kittleson, M.D.; Della Torre, P.; Häggström, J.; Lombard, C.W.; Pedersen, H.D.; Vollmar, A.; Wey, A. Allometric scaling of M-mode cardiac measurements in normal adult dogs. J. Vet. Intern. Med. 2004, 18, 311–321. [Google Scholar] [CrossRef]
- Lombard, C.W. Normal values of the canine M-mode echocardiogram. Am. J. Vet. Res. 1984, 45, 2015–2018. [Google Scholar] [PubMed]
- Wess, G.; Mäurer, J.; Simak, J.; Hartmann, K. Use of Simpson’s method of disc to detect early echocardiographic changes in Doberman Pinschers with dilated cardiomyopathy. J. Vet. Intern. Med. 2010, 24, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, H.D.; Häggström, J.; Falk, T.; Mow, T.; Olsen, L.H.; Iversen, L.; Jensen, A.L. Auscultation in mild mitral regurgitation in dogs: Observer variation, effects of physical maneuvers, and agreement with color Doppler echocardiography and phonocardiography. J. Vet. Intern. Med. 1999, 13, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Schou-Pedersen, A.M.V.; Schemeth, D.; Lykkesfeldt, J. Determination of reduced and oxidized coenzyme Q10 in canine plasma and heart tissue by HPLC-ECD: Comparison with LC-MS/MS quantification. Antioxidants 2019, 8, 253. [Google Scholar] [CrossRef] [Green Version]
- Srere, P.A. [1] Citrate synthase: [EC 4.1.3.7. Citrate oxaloacetate-lyase (CoA-acetylating)]. Methods Enzymol. 1969, 13, 3–11. [Google Scholar]
- Hidaka, T.; Fujii, K.; Funahashi, I.; Fukutomi, N.; Hosoe, K. Safety assessment of coenzyme Q10 (CoQ10). BioFactors 2008, 32, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Ikematsu, H.; Nakamura, K.; Harashima, S.-I.; Fujii, K.; Fukutomi, N. Safety assessment of coenzyme Q10 (Kaneka Q10) in healthy subjects: A double-blind, randomized, placebo-controlled trial. Regul. Toxicol. Pharmacol. 2006, 44, 212–218. [Google Scholar] [CrossRef]
- Yerramilli-Rao, P.; Beal, M.F.; Watanabe, D.; Kieburtz, K.; De Blieck, E.A.; Kitano, M.; Hosoe, K.; Funahashi, I.; Cudkowicz, M.E. Oral repeated-dose toxicity studies of coenzyme Q10 in beagle dogs. Int. J. Toxicol. 2012, 31, 58–69. [Google Scholar] [CrossRef] [Green Version]
- Langsjoen, P.H.; Langsjoen, A.M. Coenzyme Q10 in cardiovascular disease with emphasis on heart failure and myocardial ischaemia. Asia Pac. Hear J. 1998, 7, 160–168. [Google Scholar] [CrossRef]
- Soja, A.M.; Mortensen, S.A. Treatment of congestive heart failure with coenzyme Q10 illuminated by meta-analyses of clinical trials. Mol. Asp. Med. 1997, 18, 159–168. [Google Scholar] [CrossRef]
- Fotino, A.D.; Thompson-Paul, A.M.; Bazzano, L.A. Effect of coenzyme Q10 supplementation on heart failure: A meta-analysis. Am. J. Clin. Nutr. 2013, 97, 268–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheeran, F.L.; Pepe, S. Posttranslational modifications and dysfunction of mitochondrial enzymes in human heart failure. Am. J. Physiol. Endocrinol. Metab. 2016, 311, E449–E460. [Google Scholar] [CrossRef] [PubMed]
- Scheubel, R.J.; Tostlebe, M.; Simm, A.; Rohrbach, S.; Prondzinsky, R.; Gellerich, F.N.; Silber, R.E.; Holtz, J. Dysfunction of mitochondrial respiratory chain complex I in human failing myocardium is not due to disturbed mitochondrial gene expression. J. Am. Coll. Cardiol. 2002, 40, 2174–2181. [Google Scholar] [CrossRef] [Green Version]
- Kalsi, K.K.; Smolenski, R.T.; Pritchard, R.D.; Khaghani, A.; Seymour, A.M.L.; Yacoub, M.H. Energetics and function of the failing human heart with dilated or hypertrophic cardiomyopathy. Eur. J. Clin. Investig. 1999, 29, 469–477. [Google Scholar] [CrossRef]
- Quigley, A.F.; Kapsa, R.M.I.; Esmore, D.; Hale, G.; Byrne, E. Mitochondrial respiratory chain activity in idiopathic dilated cardiomyopathy. J. Card. Fail. 2000, 6, 47–55. [Google Scholar] [CrossRef]
- Garnier, A.; Zoll, J.; Fortin, D.; N’Guessan, B.; Lefebvre, F.; Geny, B.; Mettauer, B.; Veksler, V.; Clapier, R.V. Control by circulating factors of mitochondrial function and transcription cascade in heart failure. Circ. Hear Fail. 2009, 2, 342–350. [Google Scholar] [CrossRef] [Green Version]
- Sylvén, C.; Jansson, E.; Böök, K. Key enzymes of myocardial energy metabolism in patients with valvular heart disease: Relation to left ventricular function. Acta Physiol. Scand. 1988, 132, 267–270. [Google Scholar] [CrossRef]
- Boengler, K.; Kosiol, M.; Mayr, M.; Schulz, R.; Rohrbach, S. Mitochondria and ageing: Role in heart, skeletal muscle and adipose tissue. J. Cachexia. Sarcopenia Muscle 2017, 8, 349–369. [Google Scholar] [CrossRef] [Green Version]
- Hepple, R.T. Impact of aging on mitochondrial function in cardiac and skeletal muscle. Free Radic. Biol. Med. 2016, 98, 177–186. [Google Scholar] [CrossRef]
- Sorrentino, A.; Signore, S.; Qanud, K.; Borghetti, G.; Meo, M.; Cannata, A.; Zhou, Y.; Wybieralska, E.; Luciani, M.; Kannappan, R.; et al. Myocyte repolarization modulates myocardial function in aging dogs. Am. J. Physiol. Hear Circ. Physiol. 2016, 310, H873–H890. [Google Scholar] [CrossRef]
- Picard, M.; Wright, K.J.; Ritchie, D.; Thomas, M.M.; Hepple, R.T. Mitochondrial function in permeabilized cardiomyocytes is largely preserved in the senescent rat myocardium. PLoS ONE 2012, 7, e43003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picca, A.; Sirago, G.; Pesce, V.; Lezza, A.M.S.; Calvani, R.; Bossola, M.; Villani, E.R.; Landi, F.; Leeuwenburgh, C.; Bernabei, R.; et al. Administration of enalapril started late in life attenuates hypertrophy and oxidative stress burden, increases mitochondrial mass, and modulates mitochondrial quality control signaling in the rat heart. Biomolecules 2018, 8, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, M.V.; Horn, P.S.; Tang, P.H.; Morrison, J.A.; Miles, L.; Degrauw, T.; Pesce, A.J. Age-related changes in plasma coenzyme Q10 concentrations and redox state in apparently healthy children and adults. Clin. Chim. Acta 2004, 347, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Lagendijk, J.; Ubbink, J.B.; Vermaak, W.J. Measurement of the ratio between the reduced and oxidized forms of coenzyme Qlo in human plasma as a possible marker of oxidative stress. J. Lipid Res. 1996, 37, 67–75. [Google Scholar] [CrossRef]
- Åberg, F.; Appelkvist, E.L.; Dallner, G.; Ernster, L. Distribution and redox state of ubiquinones in rat and human tissues. Arch. Biochem. Biophys. 1992, 295, 230–234. [Google Scholar] [CrossRef]
- Tsutsui, H.; Kinugawa, S.; Matsushima, S. Oxidative stress and heart failure. Am. J. Physiol. Hear Circ. Physiol. 2011, 301, 2181–2190. [Google Scholar] [CrossRef] [Green Version]
- Reimann, M.J.; Haggstrom, J.; Mortensen, A.; Lykkesfeldt, J.; Moller, J.E.; Falk, T.; Olsen, L.H. Biopterin status in dogs with myxomatous mitral valve disease is associated with disease severity and cardiovascular risk factors. J. Vet. Intern. Med. 2014, 28, 1520–1526. [Google Scholar] [CrossRef] [Green Version]
- Qu, H.; Meng, Y.Y.; Chai, H.; Liang, F.; Zhang, J.Y.; Gao, Z.Y.; Shi, D.Z. The effect of statin treatment on circulating coenzyme Q10 concentrations: An updated meta-analysis of randomized controlled trials. Eur. J. Med. Res. 2018, 23, 57. [Google Scholar] [CrossRef]
- Folkers, K.; Langsjoen, P.; Willis, R.; Richardson, P.; Xia, L.I.J.; Ye, C.Q.U.; Tamagawa, H. Lovastatin decreases coenzyme Q levels in humans. Proc. Natl. Acad. Sci. USA 1990, 87, 8931–8934. [Google Scholar] [CrossRef] [Green Version]
- Paiva, H.; Thelen, K.; Coster, R.; Smet, J.; Paepe, B.; Mattila, K.; Laakso, J.; Lehtimakt, T.; Vonbergmann, K.; Lutjohann, D.; et al. High-dose statins and skeletal muscle metabolism in humans: A randomized, controlled trial. Clin. Pharmacol. Ther. 2005, 78, 60–68. [Google Scholar] [CrossRef]
- Willis, R.A.; Folkers, K.; Lan Tucker, J.; Ye, C.Q.U.; Xia, L.I.J.; Tamagawa, H. Lovastatin decreases coenzyme Q levels in rats. Proc. Natl. Acad. Sci. USA 1990, 87, 8928–8930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birkegård, A.C.; Reimann, M.J.; Martinussen, T.; Häggström, J.; Pedersen, H.D.; Olsen, L.H. Breeding restrictions decrease the prevalence of myxomatous mitral valve disease in cavalier king charles spaniels over an 8- to 10-year period. J. Vet. Intern. Med. 2016, 30, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, L.B.; Morsing, M.K.; Reimann, M.J.; Martinussen, T.; Birlie, Z.; Schou-Pedersen, A.M.V.; Lykkesfeldt, J.; Olsen, L.H. Pharmacokinetics of repeated oral dosing with coenzyme Q10 in cavalier king charles spaniels with myxomatous mitral valve disease. Antioxidants 2020, 9, 827. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CON | B1 | B2 | C | Overall p-Value | |
|---|---|---|---|---|---|
| N | 10 | 11 | 5 | 14 | |
| Breed CKCS/other | 0/10 | 11/0 | 5/0 | 14/0 | <0.0001 * |
| Sex Male/Female | 4/6 | 7/4 | 2/3 | 8/6 | 0.72 |
| Body weight (kg) | 27.5 (17.1–40.2) | 9.0 (8.1–10.1) a | 9.1 (9.0–9.9) a | 8.7 (7.9–11.4) a | <0.0001 * |
| BCS (1–9) | 5 (5–6) | 4 (4–5) | 5 (5–5) | 5 (4–5) | 0.14 |
| MR (no or mild/moderate/severe | 8/1/0 | 0/1/10 a | 0/0/5 a | 0/0/14 a | <0.0001 * |
| Murmur (1–6) | 0 (0–0) | 3 (2–3) a | 4 (4–5) a,b | 5 (4–5) a,b | <0.0001 * |
| Age (years) | 10.3 (4.0–11.8) | 10.8 (8.6–11.3) | 12.6 (12.6–12.7) | 10.01 (9.3–11.3) | 0.15 |
| LA/Ao | 1.3 (1.3–1.4) | 1.35 (1.3–1.4) | 2.0 (1.6–2.1) a,b | 2.75 (2.4–3.00) a,b,c | <0.0001 * |
| LVEDDN | 1.4 (1.30–1.60) | 1.6 (1.5–1.7) | 1.9 (1.9–2.1) a,b | 2.3 (1.9–2.6) a,b | <0.0001 * |
| FS (%) | 33.6 (33.0–38.8) | 35.5 (29.4–49.9) | 40.3 (39.8–43.2) | 45.4 (42.3–47.5) | 0.091 |
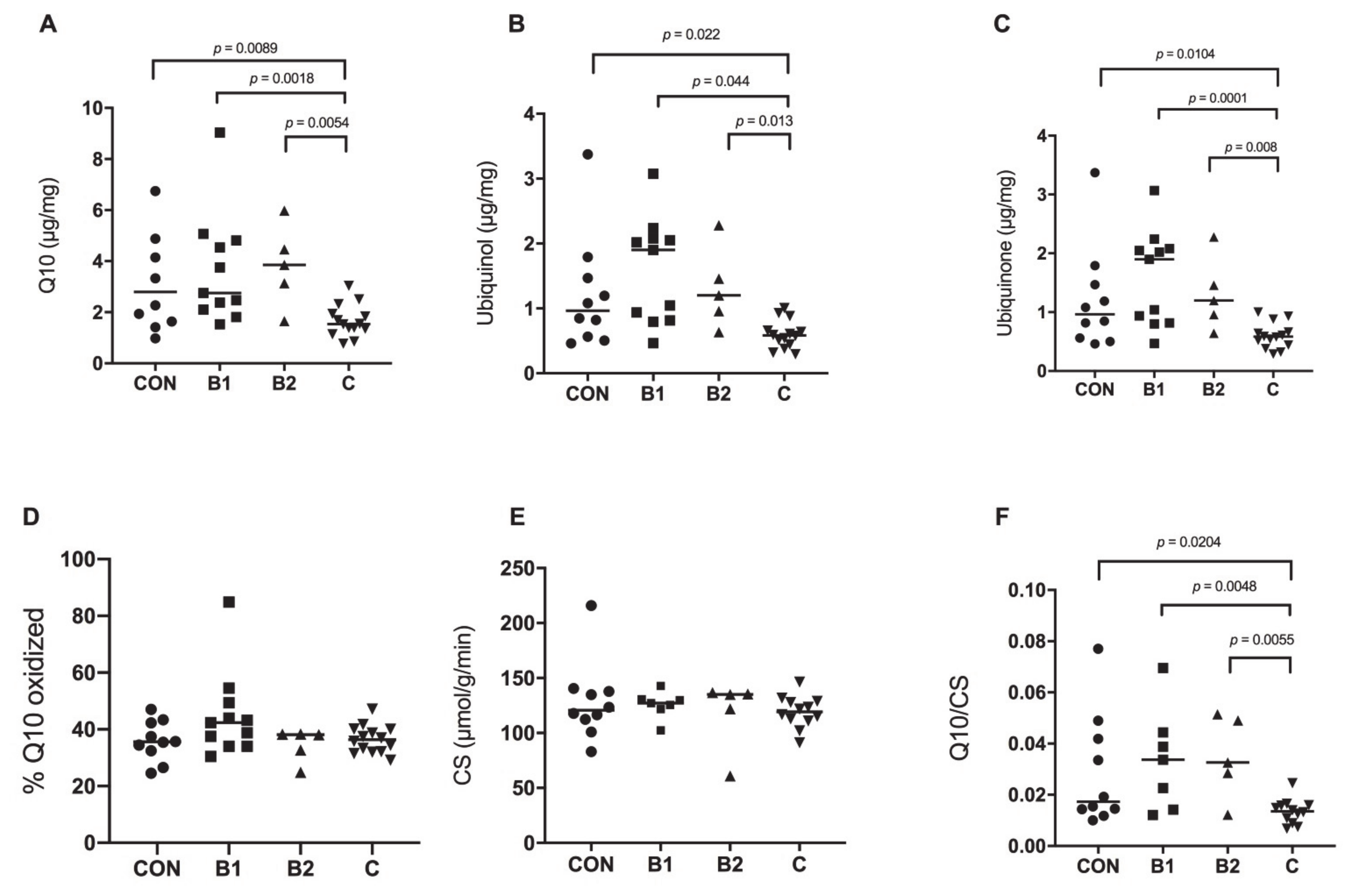
| Total Q10, myocardium, (µg/mg) | 2.8 (1.64–4.88) | 2.76 (2.10–4.81) | 3.85 (3.13–4.46) | 1.54 (1.36–1.94) a,b,c | 0.0035 * |
| Ubiquinone, myocardium, (µg/mg) | 0.97 (0.56–1.47) | 1.9 (0.82–2.08) | 1.2 (0.96–1.46) | 0.59 (0.44–0.66) a,b,c | 0.0008 * |
| Ubiquinol, myocardium, (µg/mg) | 1.84 (1.07–3.68) | 1.7 (1.06–2.73) | 2.89 (1.93–3.00) | 0.96 (0.76–1.33) a,b,c | 0.029 * |
| Oxidation rate (%) | 35.5 (32.4–42.3) | 42.2 (34.1–49.4) | 38.2 (32.7–38.3) | 36.6 (32.0–39.9) | 0.076 |
| CS μmol/g/min (n = 34) | 120.7 (109.6–138.5) n = 10 | 127.1 (121.8–130.7) n = 7 | 135.1 (121.9–135.5) n = 5 | 119.3 (111.95–128.3) n = 12 | 0.79 |
| Q10/CS | 0.017 (0.014–0.042) | 0.034 (0.014–0.044) | 0.033 (0.029–0.049) | 0.014 (0.0099–0.016) a,b,c | 0.0077 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christiansen, L.B.; Reimann, M.J.; Schou-Pedersen, A.M.V.; Larsen, S.; Lykkesfeldt, J.; Olsen, L.H. Depleted Myocardial Coenzyme Q10 in Cavalier King Charles Spaniels with Congestive Heart Failure Due to Myxomatous Mitral Valve Disease. Antioxidants 2021, 10, 161. https://doi.org/10.3390/antiox10020161
Christiansen LB, Reimann MJ, Schou-Pedersen AMV, Larsen S, Lykkesfeldt J, Olsen LH. Depleted Myocardial Coenzyme Q10 in Cavalier King Charles Spaniels with Congestive Heart Failure Due to Myxomatous Mitral Valve Disease. Antioxidants. 2021; 10(2):161. https://doi.org/10.3390/antiox10020161
Chicago/Turabian StyleChristiansen, Liselotte B., Maria J. Reimann, Anne Marie V. Schou-Pedersen, Steen Larsen, Jens Lykkesfeldt, and Lisbeth H. Olsen. 2021. "Depleted Myocardial Coenzyme Q10 in Cavalier King Charles Spaniels with Congestive Heart Failure Due to Myxomatous Mitral Valve Disease" Antioxidants 10, no. 2: 161. https://doi.org/10.3390/antiox10020161