
Non-Invasive Measurement of Exercise-Induced Oxidative Stress in Response to Physical Activity. A Systematic Review and Meta-Analysis

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
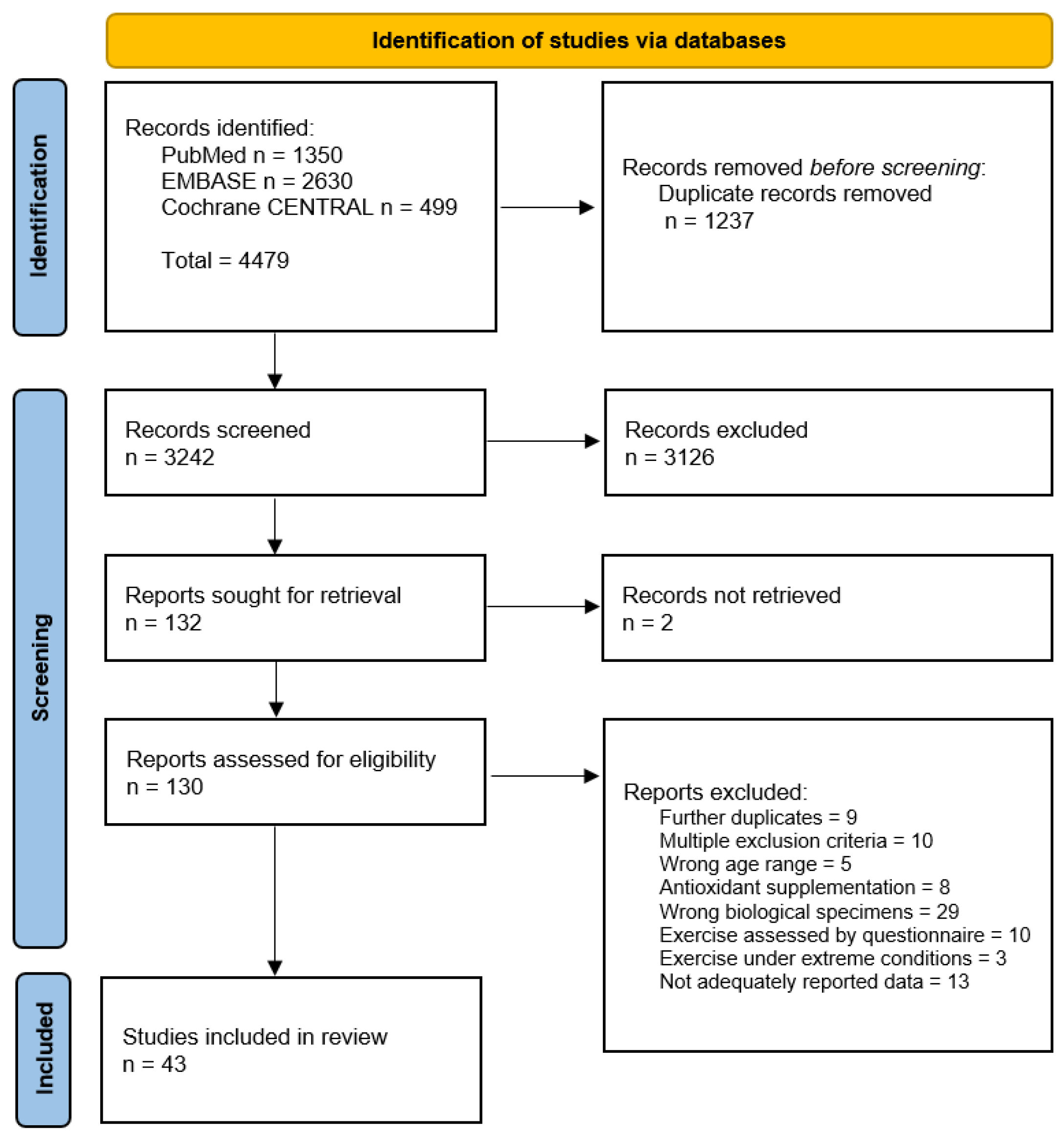
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Methods
3. Results
3.1. Qualitative Synthesis
3.1.1. Study and Participant Characteristics
3.1.2. Oxidative Stress Biomarkers
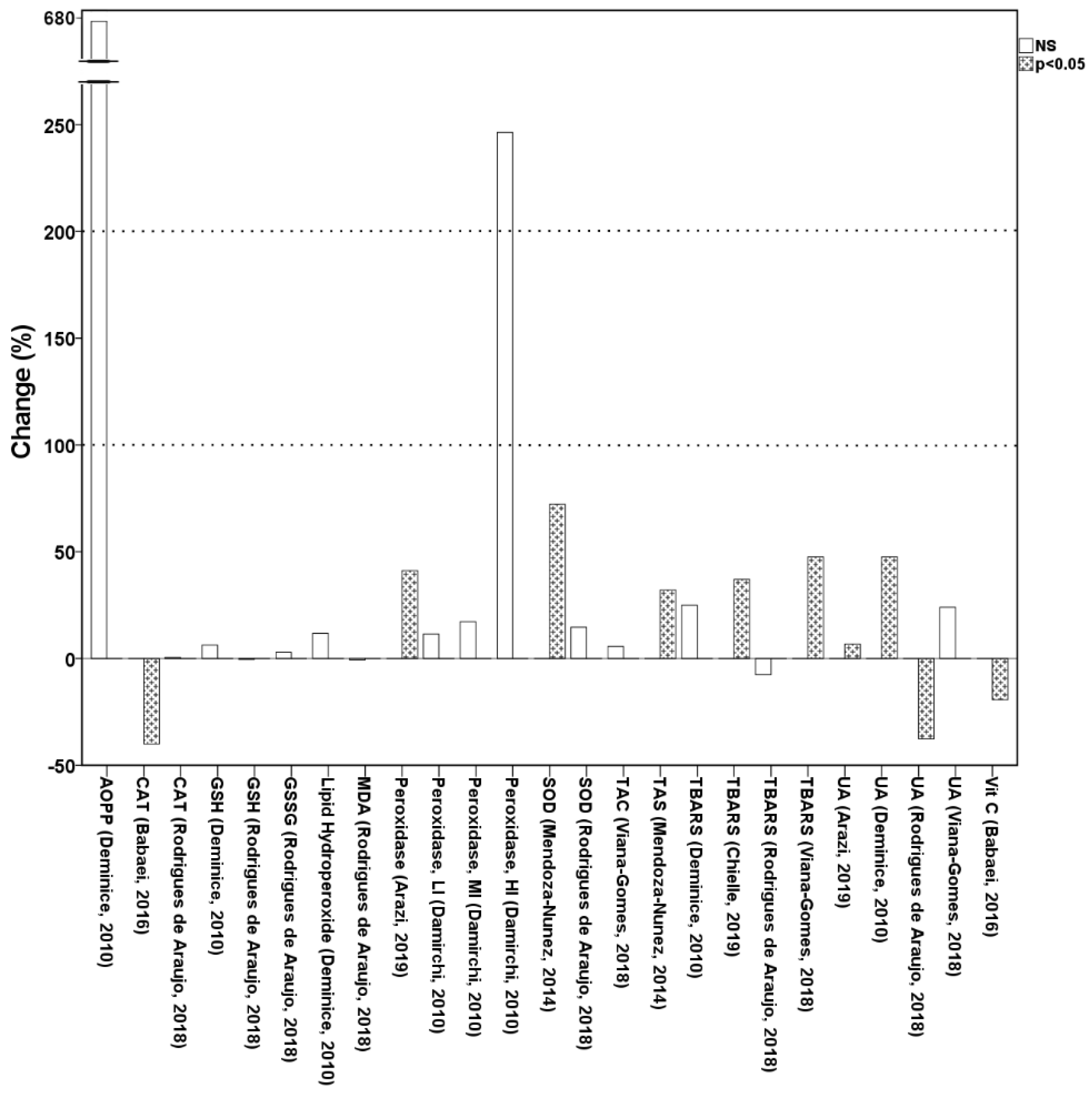
3.1.3. The Effect of Physical Activity on Oxidative Stress Biomarkers in Saliva
3.1.4. The Effect of Physical Activity on Oxidative Stress Biomarkers in Urine
3.2. Quality of the Studies
3.3. Meta-Analyses of Exercise-Induced Oxidative Stress Biomarkers
3.4. Meta-Regressions and Subgroup Analysis
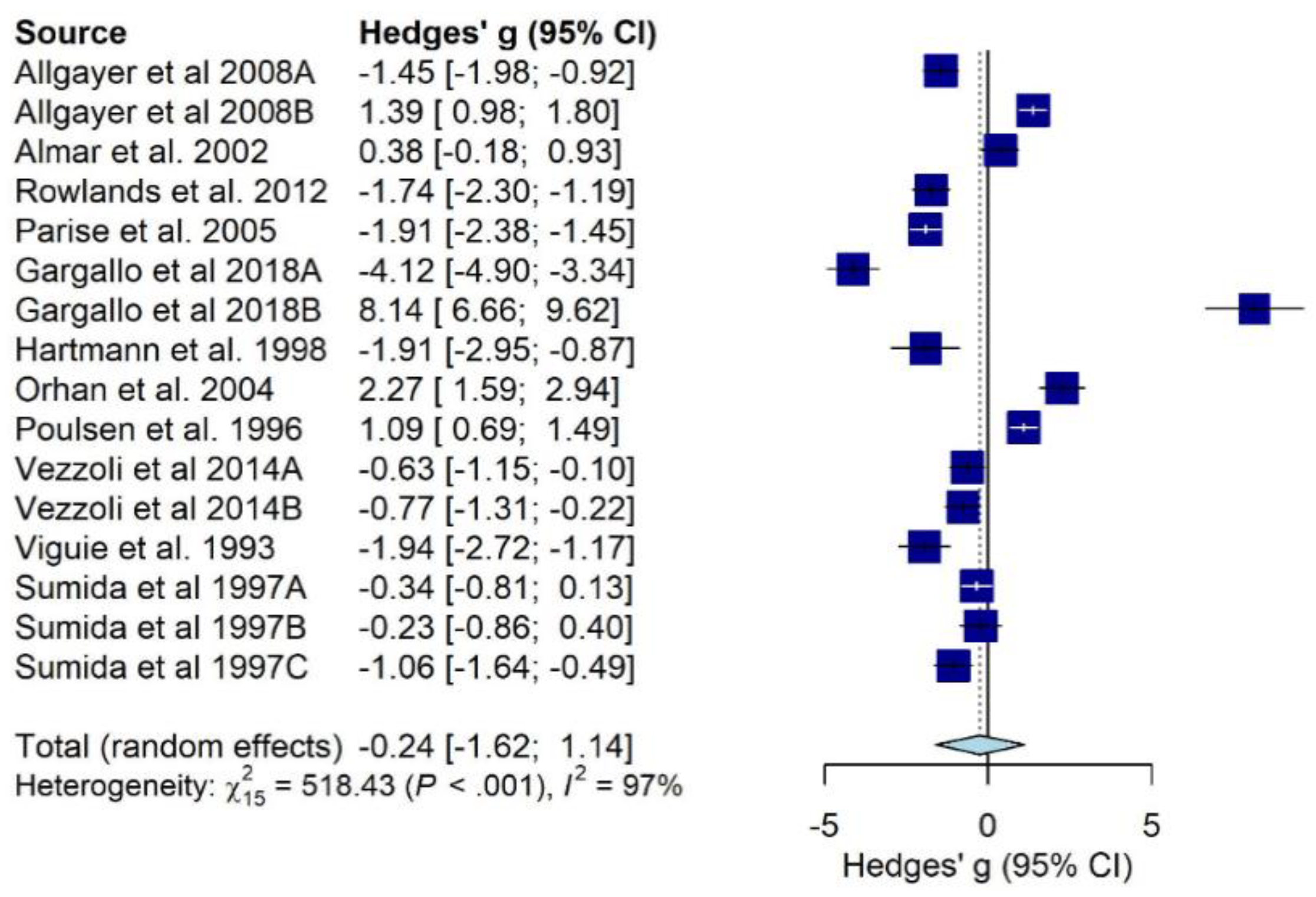
3.4.1. Meta-Regression Analyses on DNA Oxidation Biomarkers (8-oxo-dG or 8-OH-dG)
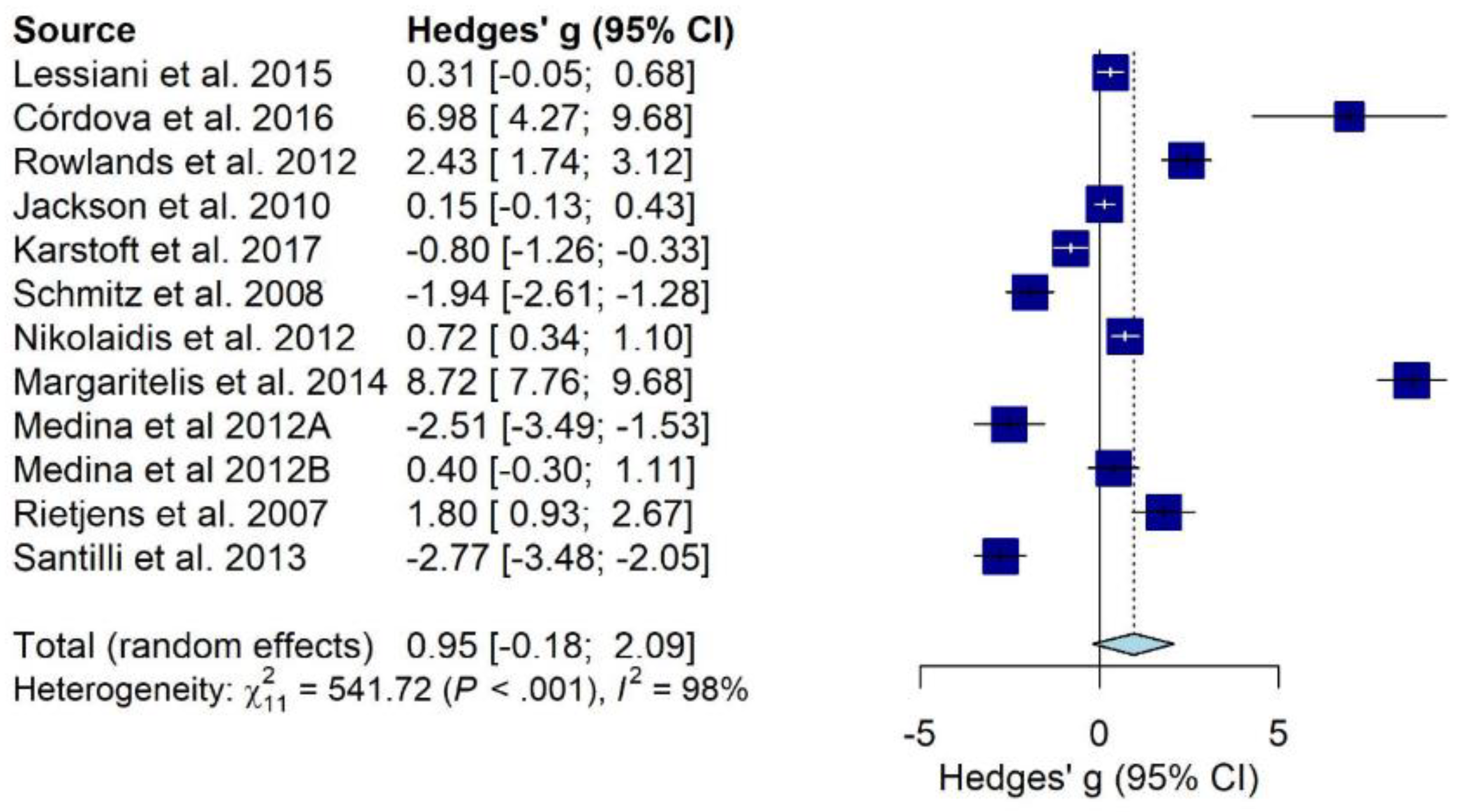
3.4.2. Meta-Regressions and Subgroup Analyses on Lipid Peroxidation Biomarkers (Isoprostanes)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Kruk, J. Physical activity in the prevention of the most frequent chronic diseases: An analysis of the recent evidence. Asian Pac. J. Cancer Prev. 2007, 8, 325–338. [Google Scholar]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.; Galano, J.; Durand, T.; Le Guennec, J.; Lee, J.C. Physiological role of reactive oxygen species as promoters of natural defenses. FASEB J. 2017, 31, 3729–3745. [Google Scholar] [CrossRef] [Green Version]
- Kruk, J.; Aboul-Enein, H.Y.; Kładna, A.; Bowser, J.E. Oxidative stress in biological systems and its relation with pathophysiological functions: The effect of physical activity on cellular redox homeostasis. Free Radic. Res. 2019, 53, 497–521. [Google Scholar] [CrossRef]
- Dillard, C.J.; Litov, R.E.; Savin, W.M.; Dumelin, E.E.; Tappel, A.L. Effects of exercise, vitamin E, and ozone on pulmonary function and lipid peroxidation. J. Appl. Physiol. 1978, 45, 927–932. [Google Scholar] [CrossRef]
- Davies, K.J.A.; Quintanilha, A.T.; Brooks, G.A.; Packer, L. Free radicals and tissue damage produced by exercise. Biochem. Biophys. Res. Commun. 1982, 107, 1198–1205. [Google Scholar] [CrossRef]
- Reid, M.B.; Khawli, F.A.; Moody, M.R. Reactive oxygen in skeletal muscle. III. Contractility of unfatigued muscle. J. Appl. Physiol. 1993, 75, 1081–1087. [Google Scholar] [CrossRef]
- Hammeren, J.; Powers, S.; Lawler, J.; Criswell, D.; Martin, D.; Lowenthal, D.; Pollock, M. Exercise Training-Induced Alterations in Skeletal Muscle Oxidative and Antioxidant Enzyme Activity in Senescent Rats. Int. J. Sports Med. 1992, 13, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Palmer, R.M.J.; Ferrige, A.G.; Moncada, S. Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nat. Cell Biol. 1987, 327, 524–526. [Google Scholar] [CrossRef] [PubMed]
- Balon, T.W.; Nadler, J.L. Nitric oxide release is present from incubated skeletal muscle preparations. J. Appl. Physiol. 1994, 77, 2519–2521. [Google Scholar] [CrossRef]
- Radak, Z.; Chung, H.Y.; Goto, S. Exercise and hormesis: Oxidative stress-related adaptation for successful aging. Biogerontology 2005, 6, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Mattson, M.P. Hormesis defined. Ageing Res. Rev. 2008, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Fisher-Wellman, K.; Bloomer, R.J. Acute exercise and oxidative stress: A 30 year history. Dyn. Med. 2009, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; He, H. Hormesis, allostatic buffering capacity and physiological mechanism of physical activity: A new theoretic framework. Med. Hypotheses 2009, 72, 527–532. [Google Scholar] [CrossRef]
- Powers, S.K.; Radak, Z.; Ji, L.L. Exercise-induced oxidative stress: Past, present and future. J. Physiol. 2016, 594, 5081–5092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, R.; Hughes, M.G.; Thomas, A.W.; Morris, K. The Ability of Exercise-Associated Oxidative Stress to Trigger Redox-Sensitive Signalling Responses. Antioxidants 2017, 6, 63. [Google Scholar] [CrossRef] [Green Version]
- Goto, C.; Higashi, Y.; Kimura, M.; Noma, K.; Hara, K.; Nakagawa, K.; Kawamura, M.; Chayama, K.; Yoshizumi, M.; Nara, I. Effect of Different Intensities of Exercise on Endothelium-Dependent Vasodilation in Humans: Role of Endothelium-Dependent Nitric Oxide and Oxidative Stress. Circulation 2003, 108, 530–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Il’Yasova, D.; Scarbrough, P.; Spasojevic, I. Urinary biomarkers of oxidative status. Clin. Chim. Acta 2012, 413, 1446–1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thirupathi, A.; Pinho, R.A.; Ugbolue, U.C.; He, Y.; Meng, Y.; Gu, Y. Effect of Running Exercise on Oxidative Stress Biomarkers: A Systematic Review. Front. Physiol. 2021, 11, 1789. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- National Institutes of Health, Quality Assessment Tool. 2014. Available online: https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort (accessed on 1 July 2020).
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J. Systematic Reviews of Effectiveness; Aromataris, E., Munn, Z., Eds.; Man. Evid. Synth.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Rosenthal, R. Applied social research methods series. In Survey Research; Sage Publications: Newbury Pa, CA, USA, 1991. [Google Scholar]
- Olkin, I.; Dahabreh, I.J.; Trikalinos, T.A. GOSH—A graphical display of study heterogeneity. Res. Synth. Methods 2012, 3, 214–223. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Allgayer, H.; Owen, R.W.; Nair, J.; Spiegelhalder, B.; Streit, J.; Reichel, C.; Bartsch, H. Short-term moderate exercise programs reduce oxidative DNA damage as determined by high-performance liquid chromatography-electrospray ionization-mass spectrometry in patients with colorectal carcinoma following primary treatment. Scand. J. Gastroenterol. 2008, 43, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Almar, M.; Villa, J.G.; Cuevas, M.J.; Rodríguez-Marroyo, J.A.; Avila, C.; Gonzalez-Gallego, J. Urinary levels of 8-hydroxydeoxyguanosine as a marker of oxidative damage in road cycling. Free Radic. Res. 2002, 36, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Arazi, H.; Taati, B.; Sajedi, F.R.; Suzuki, K. Salivary Antioxidants Status Following Progressive Aerobic Exercise: What Are the Differences between Waterpipe Smokers and Non-Smokers? Antioxidants 2019, 8, 418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babaei, P.; Damirchi, A.; Tehrani, B.S.; Nazari, Y.; Sariri, R.; Hoseini, R. Effect of exercise training on saliva brain derived neurotrophic factor, catalase and vitamin c. Med. J. Islam. Repub. Iran 2016, 30, 452. [Google Scholar]
- Chielle, E.O.; Granella, L.W.; Maziero, J.S.; Vidigal, T.M.A.; Mallmann, B.L.K.; Karal, J. Evolution of potential biomarkers of acute muscle injury after physical exercise. Braz. J. Pharm. Sci. 2019, 55, 17594. [Google Scholar] [CrossRef]
- Córdova, A.; Sureda, A.; Albina, M.L.; Linares, V.; Bellés, M.; Sánchez, D.J. Oxidative Stress Markers After a Race in Professional Cyclists. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Damirchi, A.; Kiani, M.; Jafarian, V.; Sariri, R. Response of salivary peroxidase to exercise intensity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 108, 1233–1237. [Google Scholar] [CrossRef]
- Deminice, R.; Sicchieri, T.; Payão, P.O.; Jordão, A.A. Blood and Salivary Oxidative Stress Biomarkers Following an Acute Session of Resistance Exercise in Humans. Int. J. Sports Med. 2010, 31, 599–603. [Google Scholar] [CrossRef]
- Devries, M.C.; Hamadeh, M.; Glover, A.W.; Raha, S.; Samjoo, I.A.; Tarnopolsky, M.A. Endurance training without weight loss lowers systemic, but not muscle, oxidative stress with no effect on inflammation in lean and obese women. Free Radic. Biol. Med. 2008, 45, 503–511. [Google Scholar] [CrossRef]
- Gargallo, P.; Colado, J.C.; Juesas, A.; Hernando-Espinilla, A.; Capell, N.E.; Monzó-Beltran, L.; García-Pérez, P.; Cauli, O.; Sáez, G. The Effect of Moderate- Versus High-Intensity Resistance Training on Systemic Redox State and DNA Damage in Healthy Older Women. Biol. Res. Nurs. 2018, 20, 205–217. [Google Scholar] [CrossRef]
- Hartmann, A.; Pfuhler, S.; Dennog, C.; Germadnik, D.; Pilger, A.; Speit, G. Exercise-Induced DNA Effects in Human Leukocytes Are Not Accompanied by Increased Formation of 8-Hydroxy-2′-Deoxyguanosine or Induction of Micronuclei. Free Radic. Biol. Med. 1998, 24, 245–251. [Google Scholar] [CrossRef]
- Hofer, T.; Fontana, L.; Anton, S.D.; Weiss, E.P.; Villareal, D.; Malayappan, B.; Leeuwenburgh, C. Long-Term Effects of Caloric Restriction or Exercise on DNA and RNA Oxidation Levels in White Blood Cells and Urine in Humans. Rejuvenation Res. 2008, 11, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.; Ramos, C.; Gupta, C.; Gomez-Marin, O. Exercise decreases plasma antioxidant capacity and increases urinary isoprostanes of IPF patients. Respir. Med. 2010, 104, 1919–1928. [Google Scholar] [CrossRef] [Green Version]
- Karstoft, K.; Clark, M.A.; Jakobsen, I.; Müller, I.A.; Pedersen, B.K.; Solomon, T.; Ried-Larsen, M. The effects of 2 weeks of interval vs continuous walking training on glycaemic control and whole-body oxidative stress in individuals with type 2 diabetes: A controlled, randomised, crossover trial. Diabetologia 2017, 60, 508–517. [Google Scholar] [CrossRef]
- Lessiani, G.; Santilli, F.; Boccatonda, A.; Iodice, P.; Liani, R.; Tripaldi, R.; Saggini, R.; Davì, G. Arterial stiffness and sedentary lifestyle: Role of oxidative stress. Vasc. Pharmacol. 2016, 79, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Margaritelis, N.; Kyparos, A.; Paschalis, V.; Theodorou, A.; Panayiotou, G.; Zafeiridis, A.; Dipla, K.; Nikolaidis, M.; Vrabas, I. Reductive stress after exercise: The issue of redox individuality. Redox Biol. 2014, 2, 520–528. [Google Scholar] [CrossRef] [Green Version]
- Margonis, K.; Fatouros, I.G.; Jamurtas, T.; Nikolaidis, M.G.; Douroudos, I.; Chatzinikolaou, A.; Mitrakou, A.; Mastorakos, G.; Papassotiriou, I.; Taxildaris, K.; et al. Oxidative stress biomarkers responses to physical overtraining: Implications for diagnosis. Free Radic. Biol. Med. 2007, 43, 901–910. [Google Scholar] [CrossRef]
- Medina, S.; Domínguez-Perles, R.; Cejuela-Anta, R.; Villaño, D.; Martínez-Sanz, J.M.; Gil, P.; García-Viguera, C.; Ferreres, F.; Gil, J.I.; Gil-Izquierdo, A. Assessment of oxidative stress markers and prostaglandins after chronic training of triathletes. Prostaglandins Other Lipid Mediat. 2012, 99, 79–86. [Google Scholar] [CrossRef]
- Mendoza-Núñez, V.M.; Hernández-Monjaraz, B.; Santiago-Osorio, E.; Betancourt-Rule, J.M.; Ruiz-Ramos, M. Tai Chi Exercise Increases SOD Activity and Total Antioxidant Status in Saliva and Is Linked to an Improvement of Periodontal Disease in the Elderly. Oxidative Med. Cell. Longev. 2014, 2014, 603853. [Google Scholar] [CrossRef]
- Mercken, E.M.; Hageman, G.J.; Schols, A.M.W.J.; Akkermans, M.A.; Bast, A.; Wouters, E.F.M. Rehabilitation Decreases Exercise-induced Oxidative Stress in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2005, 172, 994–1001. [Google Scholar] [CrossRef]
- Mikami, T.; Kita, K.; Tomita, S.; Qu, G.-J.; Tasaki, Y.; Ito, A. Is allantoin in serum and urine a useful indicator of exercise-induced oxidative stress in humans? Free Radic. Res. 2000, 32, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, K.; Oh-Ishi, S.; Itoh, M.; Saito, T.; Ichiwata, T. Urinary 8-Hydroxydeoxyguanosine Is a Potential Indicator for Estimating Pulmonary Rehabilitation-Induced Oxidative Stress in COPD Patients. Tohoku J. Exp. Med. 2014, 233, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolaidis, M.G.; Kyparos, A.; Dipla, K.; Zafeiridis, A.; Sambanis, M.; Grivas, G.; Paschalis, V.; Theodorou, A.A.; Papadopoulos, S.; Spanou, C.; et al. Exercise as a model to study redox homeostasis in blood: The effect of protocol and sampling point. Biomarkers 2012, 17, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, M.G.; Kyparos, A.; Spanou, C.; Paschalis, V.; Theodorou, A.A.; Panayiotou, G.; Grivas, G.; Zafeiridis, A.; Dipla, K.; Vrabas, I.S. Aging is not a barrier to muscle and redox adaptations: Applying the repeated eccentric exercise model. Exp. Gerontol. 2013, 48, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Nojima, H.; Watanabe, H.; Yamane, K.; Kitahara, Y.; Sekikawa, K.; Yamamoto, H.; Yokoyama, A.; Inamizu, T.; Asahara, T.; Kohno, N. Effect of aerobic exercise training on oxidative stress in patients with type 2 diabetes mellitus. Metabolism 2008, 57, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Orhan, H.; van Holland, B.; Krab, B.; Moeken, J.; Vermeulen, N.P.; Hollander, P.; Meerman, J.H. Evaluation of a Multi-parameter Biomarker Set for Oxidative Damage in Man: Increased Urinary Excretion of Lipid, Protein and DNA Oxidation Products after One Hour of Exercise. Free Radic. Res. 2004, 38, 1269–1279. [Google Scholar] [CrossRef]
- Parise, G.; Brose, A.N.; Tarnopolsky, M.A. Resistance exercise training decreases oxidative damage to DNA and increases cytochrome oxidase activity in older adults. Exp. Gerontol. 2005, 40, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, S.L.H.E. Extreme exercise and oxidative DNA modification. J. Sports Sci. 1996, 14, 343–346. [Google Scholar] [CrossRef]
- Radák, Z.; Pucsuk, J.; Boros, S.; Josfai, L.; Taylor, A. Changes in urine 8-hydroxydeoxyguanosine levels of super-marathon runners during a four-day race period. Life Sci. 2000, 66, 1763–1767. [Google Scholar] [CrossRef]
- Rall, L.C.; Roubenoff, R.; Meydani, S.N.; Han, S.N.; Meydani, M. Urinary 8-hydroxy-2′-deoxyguanosine (8-OHdG) as a marker of oxidative stress in rheumatoid arthritis and aging: Effect of progressive resistance training. J. Nutr. Biochem. 2000, 11, 581–584. [Google Scholar] [CrossRef]
- Rietjens, S.J.; Beelen, M.; Koopman, R.; VAN Loon, L.J.C.; Bast, A.; Haenen, G.R.M.M. A Single Session of Resistance Exercise Induces Oxidative Damage in Untrained Men. Med. Sci. Sports Exerc. 2007, 39, 2145–2151. [Google Scholar] [CrossRef] [PubMed]
- De Araujo, V.R.; Lisboa, P.; Boaventura, G.; Caramez, F.; Pires, L.; Oliveira, E.; Moura, E.; Casimiro-Lopes, G. Acute high-intensity exercise test in soccer athletes affects salivary biochemical markers. Free Radic. Res. 2018, 52, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, D.S.; Pearce, E.; Aboud, A.; Gillen, J.B.; Gibala, M.J.; Donato, S.; Waddington, J.M.; Green, J.G.; Tarnopolsky, M.A. Oxidative stress, inflammation, and muscle soreness in an 894-km relay trail run. Graefe’s Arch. Clin. Exp. Ophthalmol. 2012, 112, 1839–1848. [Google Scholar] [CrossRef]
- Samia, B.A.A.; Youssef, G.A. Changes in Urinary 8-Hydroxydeoxyguanosine Levels During Heptathlon Race in Professional Female Athletes. J. Hum. Kinet. 2014, 41, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Samjoo, I.A.; Safdar, A.; Hamadeh, M.J.; Raha, S.; Tarnopolsky, M.A. The effect of endurance exercise on both skeletal muscle and systemic oxidative stress in previously sedentary obese men. Nutr. Diabetes 2013, 3, e88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santilli, F.; Vazzana, N.; Iodice, P.; Lattanzio, S.; Liani, R.; Bellomo, R.G.; Lessiani, G.; Perego, F.; Saggini, R.; Davì, G. Effects of high-amount–high-intensity exercise on in vivo platelet activation: Modulation by lipid peroxidation and AGE/RAGE axis. Thromb. Haemost. 2013, 110, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.H.; Warren, M.; Rundle, A.G.; Williams, N.I.; Gross, M.D.; Kurzer, M.S. Exercise Effect on Oxidative Stress Is Independent of Change in Estrogen Metabolism. Cancer Epidemiol. Biomark. Prev. 2008, 17, 220–223. [Google Scholar] [CrossRef] [Green Version]
- Sumida, S.; Okamura, K.; Doi, T.; Sakurai, M.; Yoshioka, Y.; Sugawa-Katayama, Y. No influence of a single bout of exercise on urinary excretion of 8-hydroxy-deoxyguanosine in humans. IUBMB Life 1997, 42, 601–609. [Google Scholar] [CrossRef]
- Vempati, R.; Bijlani, R.L.; Deepak, K.K. The efficacy of a comprehensive lifestyle modification programme based on yoga in the management of bronchial asthma: A randomized controlled trial. BMC Pulm. Med. 2009, 9, 37. [Google Scholar] [CrossRef] [Green Version]
- Vezzoli, A.; Pugliese, L.; Marzorati, M.; Serpiello, F.R.; La Torre, A.; Porcelli, S. Time-Course Changes of Oxidative Stress Response to High-Intensity Discontinuous Training versus Moderate-Intensity Continuous Training in Masters Runners. PLoS ONE 2014, 9, e87506. [Google Scholar] [CrossRef] [Green Version]
- Vezzoli, A.; Dellanoce, C.; Mrakic-Sposta, S.; Montorsi, M.; Moretti, S.; Tonini, A.; Pratali, L.; Accinni, R. Oxidative Stress Assessment in Response to Ultraendurance Exercise: Thiols Redox Status and ROS Production according to Duration of a Competitive Race. Oxidative Med. Cell. Longev. 2016, 2016, 6439037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viana-Gomes, D.; Rosa, F.; Mello, R.; Paz, G.; Miranda, H.; Salerno, V. Oxidative stress, muscle and liver cell damage in professional soccer players during a 2-game week schedule. Sci. Sports 2018, 33, e221–e228. [Google Scholar] [CrossRef]
- Viguie, C.A.; Frei, B.; Shigenaga, M.K.; Ames, B.N.; Packer, L.; Brooks, G.A. Antioxidant status and indexes of oxidative stress during consecutive days of exercise. J. Appl. Physiol. 1993, 75, 566–572. [Google Scholar] [CrossRef]
- Wragg, C.B.; Maxwell, N.S.; Doust, J.H. Evaluation of the reliability and validity of a soccer-specific field test of repeated sprint ability. Graefe’s Arch. Clin. Exp. Ophthalmol. 2000, 83, 77–83. [Google Scholar] [CrossRef]
- Thirupathi, A.; Wang, M.; Lin, J.K.; Fekete, G.; István, B.; Baker, J.S.; Gu, Y. Effect of Different Exercise Modalities on Oxidative Stress: A Systematic Review. BioMed. Res. Int. 2021, 2021, 1947928. [Google Scholar] [CrossRef]
- Marquez, D.X.; Aguiñaga, S.; Vásquez, P.M.; Conroy, D.E.; Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Sheppard, B.B.; Petruzzello, S.J.; et al. A systematic review of physical activity and quality of life and well-being. Transl. Behav. Med. 2020, 10, 1098–1109. [Google Scholar] [CrossRef] [PubMed]
- Viitala, P.; Newhouse, I.J. Vitamin E supplementation, exercise and lipid peroxidation in human participants. Graefe’s Arch. Clin. Exp. Ophthalmol. 2004, 93, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Vollaard, N.B.J.; Shearman, J.; Cooper, C. Exercise-Induced Oxidative Stress. Sports Med. 2005, 35, 1045–1062. [Google Scholar] [CrossRef]
- Kawamura, T.; Muraoka, I. Exercise-Induced Oxidative Stress and the Effects of Antioxidant Intake from a Physiological Viewpoint. Antioxidants 2018, 7, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, D.; Arend, E.; Rocha, S.M.; Rudnitskaya, A.; Delgado, L.; Moreira, A.; Carvalho, M.J. The impact of exercise training on the lipid peroxidation metabolomic profile and respiratory infection risk in older adults. Eur. J. Sport Sci. 2019, 19, 384–393. [Google Scholar] [CrossRef]
- Nikolaidis, M.G.; Kyparos, A.; Vrabas, I.S. F2-isoprostane formation, measurement and interpretation: The role of exercise. Prog. Lipid Res. 2011, 50, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Urso, M.L.; Clarkson, P.M. Oxidative stress, exercise, and antioxidant supplementation. Toxicology 2003, 189, 41–54. [Google Scholar] [CrossRef]
- Sacheck, J.M.; Blumberg, J.B. Role of vitamin E and oxidative stress in exercise. Nutrition 2001, 17, 809–814. [Google Scholar] [CrossRef]
- Powers, S.K.; Deminice, R.; Ozdemir, M.; Yoshihara, T.; Bomkamp, M.P.; Hyatt, H. Exercise-induced oxidative stress: Friend or foe? J. Sport Health Sci. 2020, 9, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Wang, X.; Yamanaka, T.; Ogita, F.; Nakatani, K.; Takeuchi, T. Effects of anaerobic exercise and aerobic exercise on biomarkers of oxidative stress. Environ. Health Prev. Med. 2007, 12, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Bloomer, R.J.; Goldfarb, A.H. Anaerobic Exercise and Oxidative Stress: A Review. Can. J. Appl. Physiol. 2004, 29, 245–263. [Google Scholar] [CrossRef]
- Radak, Z.; Taylor, A.W.; Ohno, H.; Goto, S. Adaptation to exercise-induced oxidative stress: From muscle to brain. Exerc. Immunol. Rev. 2001, 7, 90–107. [Google Scholar]
- Elejalde, E.; Villarán, M.C.; Alonso, R.M. Grape polyphenols supplementation for exercise-induced oxidative stress. J. Int. Soc. Sports Nutr. 2021, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- Simioni, C.; Zauli, G.; Martelli, A.M.; Vitale, M.; Sacchetti, G.; Gonelli, A.; Neri, L.M. Oxidative stress: Role of physical exercise and antioxidant nutraceuticals in adulthood and aging. Oncotarget 2018, 9, 17181–17198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, S.K.; Jackson, M.J. Exercise-Induced Oxidative Stress: Cellular Mechanisms and Impact on Muscle Force Production. Physiol. Rev. 2008, 88, 1243–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michailidis, Y.; Jamurtas, A.Z.; Nikolaidis, M.G.; Fatouros, I.G.; Koutedakis, Y.; Papassotiriou, I.; Kouretas, D. Sampling Time is Crucial for Measurement of Aerobic Exercise-Induced Oxidative Stress. Med. Sci. Sports Exerc. 2007, 39, 1107–1113. [Google Scholar] [CrossRef]
- Martinez-Moral, M.-P.; Kannan, K. How stable is oxidative stress level? An observational study of intra- and inter-individual variability in urinary oxidative stress biomarkers of DNA, proteins, and lipids in healthy individuals. Environ. Int. 2019, 123, 382–389. [Google Scholar] [CrossRef]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and Clinical Significance of Biomarkers of Oxidative Stress in Humans. Oxidative Med. Cell. Longev. 2017, 2017, 6501046. [Google Scholar] [CrossRef] [PubMed]
- Graille, M.; Wild, P.; Sauvain, J.-J.; Hemmendinger, M.; Canu, I.G.; Hopf, N. Urinary 8-isoprostane as a biomarker for oxidative stress. A systematic review and meta-analysis. Toxicol. Lett. 2020, 328, 19–27. [Google Scholar] [CrossRef]
- Wang, J.; Schipper, H.M.; Velly, A.M.; Mohit, S.; Gornitsky, M. Salivary biomarkers of oxidative stress: A critical review. Free Radic. Biol. Med. 2015, 85, 95–104. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Design | Sample Population (n; Sex; Age; Training; Health) | Physical Activity (Type; Duration; Intensity) | Main Findings | Quality Assessment | Ref. |
|---|---|---|---|---|---|---|---|
| Allgayer 2008 | Germany | RCT | ♂ 17 moderately active, age (SD) = 58 (2) ♀ 27 active, age (SD) = 59 (1) non-athlete, cancer patients | aerobic 35 min duration 30–60% Vo2max | ↑ Urinary 8-OH-dG. After 2 weeks of individualised aerobic exercise (30–40 min/Day) | High | [27] |
| Almar 2002 | Spain | Longitudinal | ♂ 8 Age (SD) = 25.5 (1.7) athlete, healthy | mixed NA duration 75% Vo2max | N.S. changes in urinary 8-OH-dG normalised to creatinine. ↑ not normalised 8-OH-dG. After a 3-day cycling race | Medium | [28] |
| Arazi 2019 | Iran Japan | Controlled before-after | ♀ 23 11 smokers, age (SD) =23.6 (2.9) 12 non-smokers, age (SD) = 22.7 (2.9) sedentary, healthy | aerobic NA duration Until exhaustion | ↑ Salivary peroxidase ↑ Salivary UA (non-smokers). After a treadmill bout until exhaustion | High | [29] |
| Babaei 2016 | Iran | RCT | ♂ 25 Age (SD) = 21 (3) sedentary, healthy | aerobic NA duration Until exhaustion | ↓ Salivary CAT, Vitamin C. After treadmill run | Medium | [30] |
| Chielle 2019 | Brazil | Before after | ♂ 27 Age (SD) = 22.5 (4.2) athlete, healthy | mixed 60 min duration NA intensity | ↑ Salivary TBARS ↑ TBARS After supervised training | High | [31] |
| Córdova 2015 | Spain | Longitudinal | ♂ 8 Age (SD) = 25.7 (3.3) athlete, healthy | aerobic 230 min duration 85% Vo2max | ↑ Urinary isoprostane. After a cycling race | Medium | [32] |
| Damirchi 2010 | Iran | Controlled before-after | ♂ 10 Age (SD) = 23.2 (2.3) non-athlete, healthy | aerobic 18 min duration 50–75% VO2max | ↑ Salivary peroxidase. After a treadmill run until exhaustion | Medium | [33] |
| Deminice 2010 | Brazil | Before after | ♂ 11 Age (SD) = 25.9 (2.8) non-athlete, healthy | anaerobic NA duration 75% 1RM | ↑ Salivary UA. N.S. changes in TBARS, AOPP, GSH and lipid hydroperoxides After resistance exercise | High | [34] |
| Devries 2008 | Canada | Controlled before-after | ♀ 24 12 lean, age (SD) = 41 (2) 12 obese, age (SD) = 40 (3) sedentary, healthy and obese | aerobic 38 min duration 50–65% Vo2max | ↓ Urinary 8-OH-dG ↓ Isoprostane After a 12-week program of endurance training | High | [35] |
| Gargallo 2018 | Spain | RCT | ♀ 36 High intensity, age (SD) = 71.1 (5.3) Moderate intensity, age (SD) = 68.7 (6.1) sedentary, healthy | anaerobic 58 min duration 70–85% Vo2max | ↑ Urinary 8-OH-dG and ↓ Urinary 8-OH-dG, after high and moderate exercise intensity, respectively | Medium | [36] |
| Hartmann 1998 | Austria Germany | Before after | ♂ 3 ♀ 3 Age (SD) = 27 (6) athlete, healthy | aerobic 150 min duration High intensity (Triathlon) | ↑ Urinary 8-OH-dG. After a 24 h short-distance triathlon | High | [37] |
| Hofer 2008 | Italy USA | RCT | ♂ 5 ♀12 Age (SD) = 58.6 (2.7) sedentary, healthy | aerobic NA duration NA intensity | Urinary nucleic acid oxidation products were not significantly different from baseline following 12-month intervention program | Medium | [38] |
| Jackson 2010 | USA | RCT | ♂ 23 ♀ 6 Age (SD) = 70 (9) sedentary, idiopathic pulmonary fibrosis | aerobic 4 min duration low intensity (50-W bicycle) | ↑ Urinary isoprostane, N.S. changes in urinary H2O2 found after 50-W bicycle | High | [39] |
| Karstoft 2017 | Denmark UK | Randomised crossover trial | ♂ 11 ♀ 3 Age (SD) = 65 (2) non-athlete, diabetic | aerobic 60 min duration 75% Vo2max | N.S. changes in urinary isoprostane after 60 min of supervised waling on a treadmill | High | [40] |
| Lessiani 2016 | Italy | Before after | ♂ 12 ♀ 6 Age (IQR) = 54 (48–66) sedentary, healthy | aerobic 55 min duration 75% Vo2max | ↓ Urinary isoprostane. After an eight-week aerobic training program | High | [41] |
| Margaritelis 2014 | Cyprus Greece | Before after | ♂ 98 age (SD) = 23.5 (4) non-athlete | anaerobic NA duration high intensity (maximal voluntary contractions) | ↑ Urinary isoprostane 48 h after an acute isokinetic eccentric exercise bout | High | [42] |
| Margonis 2007 | Greece | Before after | ♂ 12 age (SD) = 22.4 (2.1) non-athlete, healthy | anaerobic NA duration 85% Vo2max | ↑ Urinary isoprostane 96 h after a 12-week resistance training protocol | Medium | [43] |
| Medina 2012 | Spain | Longitudinal | ♂ 10 Age (SD) = 19.0 (1.7) ♀ 5 Age (SD) = 21.8 (3.0) athlete, healthy | aerobic NA duration NA intensity | ↓ Urinary total isoprostanes and 8-iso-15-keto PGF2α in males after 3 weeks of triathlon training. N.S. changes in isoprostane, 8-iso-15(R) PGF2α, 2,3-dinor-8-iso PGF2α, 2,3-dinor-11β PGF2α | Medium | [44] |
| Mendoza-Núñez 2014 | Mexico | Before after | ♀ 24 Age (SD) = 67 (7) sedentary, periodontal disease | aerobic 60 min duration 55% Vo2max | ↑ Salivary SOD and TAS ↓ IL-1β. After 6 months of Tai Chi 5 days/week | High | [45] |
| Mercken 2005 | Netherlands | Controlled before-after | ♂ 11 ♀ 11 11 healthy, age (SD) = 59.7 (1.5) 11 COPD patients, age (SD) = 56.7 (2.0) sedentary, non-athlete, healthy and COPD | aerobic 23 min duration 60% Vo2max | ↑ Urinary MDA in COPD patients shortly after submaximal exercise and maximal exercise before pulmonary rehabilitation | High | [46] |
| Mikami 2000 | Japan | Controlled before-after | ♂ 7 Age range = 20–30 non-athlete, healthy | aerobic 40 min duration 40–100% VO2max | ↑ Urinary allantoin shortly after moderate intensity cycling exercise. N.S. changes of urate nor TBARS | High | [47] |
| Nemoto 2014 | Japan | Before after | ♂ 18 12 COPD II and III stage, age (SD) = 71, (1.3) 6 COPD IV stage, age (SD) = 65.7(1.52) COPD | aerobic 20 min duration 70% Vo2max | ↑ Urinary 8-OH-dG in COPD (Stage IV) following 8-week pulmonary rehabilitation and aerobic training | High | [48] |
| Nikolaidis 2012 | Cyprus Greece | Before after | ♂ 20 10 muscle damaging, age (SD) = 27 (6) 10 no muscle damaging, age (SD) = 25 (5) non-athlete, healthy | aerobic 45 min duration 70–75% Vo2max | ↑ Urinary isoprostane shortly after a running protocol on a treadmill | High | [49] |
| Nikolaidis 2013 | Cyprus Greece | Before after | ♂ 20 10 young, age(SD) = 20.6 (0.5) 10 elderly, age (SD) = 64.6 (1.1) non-athlete, healthy | anaerobic NA duration 30–50% Vo2max | ↑ Urinary isoprostane in elderly shortly after a single bout of isokinetic eccentric exercise | High | [50] |
| Nojima 2008 | Japan | RCT | ♂ 59 ♀ 28 Exercise in a fitness centre, age (SD) = 55.4 (1.1) Self-paced exercise, age (SD) = 55.9 (1.1) non-athlete, diabetic | aerobic 30 min duration 50% Vo2max | ↓ Urinary 8-OH-dG after 12-month program of aerobic exercise either self-paced either in a fitness centre | High | [51] |
| Orhan 2004 | Netherlands | Case series self-controlled | ♂ 18 Age (SD) = 24.6 (0.7) non-athlete, healthy | aerobic 60 min duration 70% Vo2max | ↑ Urinary 8-OH-dG 1 day after 1 h cycling bout (p = 0.07) N.S. changes of urinary MDA | Medium | [52] |
| Parise 2005 | Canada | Before after | ♂ 15 ♀ 15 Age (SD) = 68.5 (5.1) non-athlete, healthy | anaerobic NA duration 65% 1RM | ↓ Urinary 8-OH-dG. After a 14-week program of resistance training | High | [53] |
| Poulsen 1996 | Denmark | Before after | ♂ 23 Age (SD) = 22 (2) athlete, healthy | aerobic 570 min duration high intensity (30-day program of vigorous exercise) | ↑ Urinary 8-OH-dG after a 30-day program of vigorous exercise (6 days per week, 8–11 h per day) | Medium | [54] |
| Radák 2000 | Canada Hungary | Longitudinal | ♂ 5 Age (SD) = 35.5 (9.5) athlete, healthy | aerobic NA duration high intensity (marathon) | ↑ Urinary 8-OH-dG after the first day (120 km) of a 4-day race (marathon) | Medium | [55] |
| Rall 2000 | USA | Controlled before-after | ♂ 6 ♀ 10 8 healthy, age (SD) = 70.3 (5.0) 8 arthritis rheumatoid, age (SD) = 41.8 (12.6) sedentary, healthy and rheumatoid arthritis | anaerobic NA duration 80% 1 RM | N.S. changes in urinary 8-OH-dG following a 12-week progressive resistance training | Medium | [56] |
| Rietjens 2007 | Netherlands | Before after | ♂ 8 Age (SD) = 22.4 (2) athlete, healthy | anaerobic 41 min duration 75% Vo2max | ↑ Urinary isoprostane following a single session of resistance exercise | Medium | [57] |
| Rodrigues de Araujo 2018 | Brazil | Before after | ♂ 32 Age (SD) = 21.2 (4.2) healthy | anaerobic 3 min duration high intensity | ↓ Salivary UA and N.S. changes in salivary TBARS, MDA, GSH, GSSG, SOD and CAT after acute high intensity exercise | High | [58] |
| Rowlands 2012 | Canada | Longitudinal | ♂ 16 ♀ 3 Age (SD) = 37.0 (6.7) athlete, healthy | aerobic 5700 min duration high intensity (894-Km run) | ↑ Urinary isoprostane N.S. changes in 8-0H-dG. After an 894-km run | Medium | [59] |
| Samia 2014 | Egypt | Longitudinal | ♀ 8 Age (SD) = 22.9 (4.2) athlete | mixed 150 min duration high intensity (National 1st Class Republic Competition) | ↑ Urinary 8-OH-dG after the first day of the National First, Class Republic Competition consisting of 100 m run, high jump, shot put and 200 m run. | Medium | [60] |
| Samjoo 2013 | Canada USA | Before after | ♂ 18 9 lean, age (SD) = 38 (3) 9 obese, age (SD) = 39 (3) sedentary, healthy and obese | aerobic 45 min duration 50–70% Vo2max | ↓ Urinary isoprostane and ↑ Urinary 8-OH-dG (p = 0.07) in obese after 3-month endurance cycling training | High | [61] |
| Santilli 2013 | Italy | Before after | ♂ 15 ♀ 7 Age (SD) = 57 (9) sedentary, healthy | aerobic 50 min duration 65% Vo2max | ↓ Urinary isoprostane after 8-week aerobic training program | High | [62] |
| Schmitz 2008 | USA | Before after | ♀ 15 Age (SD) = 20.9 (2.4) sedentary, healthy | aerobic 30 min duration 70–85% Vo2max | ↓ Urinary isoprostane after 15 weeks of aerobic exercise | High | [63] |
| Sumida 1997 | Japan | Controlled before-after | ♂ 28 11 runners’ group I, age (SD) = 20.7 (0.5) 6 untrained, age (SD) = 9.8 (0.3) 11 runners’ group II, age (SD) = 19.1 (0.2) athletes, sedentary, healthy | aerobic NA duration high intensity | N.S. changes in urinary 8-OH-dG after a single bout of intensive exercise | High | [64] |
| Vempati 2009 | India | RCT | ♂ 13 ♀ 16 Age (SD) = 33.5 (11.4) sedentary, asthmatic patients | aerobic 240 min duration low intensity (yoga) | N.S. changes in urinary 11β-PGF2α after 8-week yoga intervention | Medium | [65] |
| Vezzoli 2014 | Italy | Before after | ♂ 20 moderate-intensity training, age (SD) = 50.6 (6.3) high-intensity training, age (SD) = 45.1 (8.5) healthy | aerobic NA duration 80–140% VO2peak | ↑ Urinary 8-OH-dG after either high-intensity discontinuous training and moderate-intensity continuous training | High | [66] |
| Vezzoli 2016 | Italy | Longitudinal | ♂ 10 ♀ 14 50 km race group, age (SD) = 41.8 (5.9) 100 km race group, age (SD) = 41.4 (3.6) athlete, healthy | aerobic 426 min duration high intensity (ultra-endurance exercise) | ↑ Urinary isoprostane and 8-OH-dG after ultra-endurance exercise | Medium | [67] |
| Viana-Gomes 2018 | Brazil | Before after | ♂ 8 Age (SD) = 27.2 (5.5) athlete, healthy | mixed 64 min duration high intensity (Football game) | N.S. changes in salivary TAC, UA. ↑ Salivary TBARS. After one football game | High | [68] |
| Viguie 1993 | USA | Before after | ♂ 11 Age (SD) = 24.3 (1.1) healthy | aerobic 90 min duration 65% Vo2max | N.S. changes of urinary 8-OH-dG following single exercise bout on a cycle ergometer | Medium | [69] |
| Study | Sample | Urinary Biomarker | Analytical Method | Urinary Baseline Measure | After Physical Activity | Salivary Biomarker | Analytical Method | Salivary Baseline Measure | After Physical Activity | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| Allgayer 2008 | 12 h | 8-oxo-dG [ng/mg crea] | HPLC | moderate intensity 8.5 (2.0) § high intensity 5.0 (1.3) § | 5.8 (1.5) § 7.1 (1.6) § | -- | -- | -- | -- | [27] |
| Almar 2002 | 12 h | 8-OH-dG [nmol/mmol crea] | HPLC | 117.4 (38.1) * | 136.5 (54.8) * | -- | -- | -- | -- | [28] |
| Arazi 2019 | spot | -- | -- | -- | -- | UA [mg/100 mL] | Spectrophotometric (enzymatic reaction) | non-smokers 5.9 (0.8) * smokers 5.8 (0.6) * | 6.3 (0.8) * 5.9 (0.7) * | [29] |
| Arazi 2019 | spot | -- | -- | -- | -- | Peroxidase [mm/u] | Colorimetric | non-smokers 0.17 (0.07) * smokers 0.13 (0.08) * | 0.24 (0.08) * 0.19 (0.08) * | |
| Babaei 2016 | spot | -- | -- | -- | -- | CAT [u/mL] | Spectrophotometric | 0.005 (0.001) § | 0.003 (0.001) § | [30] |
| Babaei 2016 | spot | -- | -- | -- | -- | Vitamin C [mg%] | Colorimetric | 0.274 (0.29) § | 0.221 (0.45) § | |
| Chielle 2019 | spot | TBARS [mmol/L] | ELISA | 13.6 (7.3) § | 80.1 (14.3) § | TBARS [mmol/L] | ELISA | 19.4 (11.7) § | 26.6 (18) § | [31] |
| Córdova 2015 | spot | isoprostane [pg/mg crea] | ELISA | 359 (71) § | 686 (139) § | -- | -- | -- | -- | [32] |
| Damirchi 2010 | spot | -- | -- | -- | -- | Peroxidase [U/L] | Spectrophotometric | 50% VO2max 3.22 (0.24) § 75% VO2max 3.47 (0.37) § Exhaustion 3.17 (0.40) § | 3.59 (0.25) § 4.07 (0.38) § 10.98 (0.27) § | [33] |
| Deminice 2010 | spot | -- | -- | -- | -- | TBARS [umol/L] | Colorimetric (Ellman’s reaction) | 2.0 (1.2) § | 2.5 (1.2) § | [34] |
| Deminice 2010 | spot | -- | -- | -- | -- | Lipid hydroperoxide [umol H2O2 equivalents/L] | Colorimetric | 10.2 (2.6) § | 11.4 (4.5)v | |
| Deminice 2010 | spot | -- | -- | -- | -- | AOPP [umol chloromina T equivalents/L] | Spectrophotometric | 30.8 (14.8) § | 37.4 (17.7) § | |
| Deminice 2010 | spot | -- | -- | -- | -- | UA [mg/dL] | Enzymatic | 2.1 (1.1) § | 3.1 (1.1) § | |
| Deminice 2010 | spot | -- | -- | -- | -- | GSH [umol/L] | Colorimetric (Ellman’s reaction) | 0.16 (0.08) § | 0.17 (0.08) § | |
| Devries 2008 | 24 h | isoprostane [pg/mL] | ELISA | lean 54.41 (17.12) * obese 72.20 (17.97) * | 37.97 (8.3) * 53.22 (12.03) * | -- | -- | -- | -- | [35] |
| Devries 2008 | 8-OH-2-dG [ng/mL] | ELISA | lean 5.71 (1.31) * obese 15.02 (3.73) * | 3.15 (0.76) * 4.69 (1.54) * | -- | -- | -- | -- | ||
| Gargallo 2018 | spot | 8-OH-dG [nmol/mmol crea] | HPLC | high intensity 2.12 (1.34) § moderate intensity 3.91 (1.40) § | 3.64 (1.37) § 2.90 (1.54) § | -- | -- | -- | -- | [36] |
| Gargallo 2018 | GSH [nmol/mg protein] | Colorimetric (enzymatic recycling) | high intensity 22.71 (3.83) § moderate intensity 20.84 (3.15) § | 20.23 (3.35) § 20.69 (4.22) § | -- | -- | -- | -- | ||
| Gargallo 2018 | GSSG [nmol/mg protein] | Colorimetric (enzymatic recycling) | high intensity 0.23 (0.08) § moderate intensity 0.25 (0.07) § | 0.25 (0.13) § 0.23 (0.09) § | -- | -- | -- | -- | ||
| Gargallo 2018 | GSSG/GSH [%] | Colorimetric (enzymatic recycling) | high intensity 1.05 (0.48) § moderate intensity 1.25 (0.40) § | 1.29 (0.79) § 1.19 (0.57) § | -- | -- | -- | -- | ||
| Hartmann 1998 | 24 h | 8-OH-dG [umol/mol crea] | HPLC | 2.42 (1.26) § | 1.30 (0.23) § | -- | -- | -- | -- | [37] |
| Hofer 2008 | 12 h | FapyGua [nmol/mmol crea] | MS-MS | 4.50 (2.4) * | 3.25 (1.0) * | -- | -- | -- | -- | [38] |
| Hofer 2008 | 8-oxoGua [nmol/mmol crea] | MS-MS | 127 (28) * | 144 (44) * | -- | -- | -- | -- | ||
| Hofer 2008 | 8-oxoGuo [nmol/mmol crea] | MS-MS | 6.28 (2.1) * | 5.34 (1.5) * | -- | -- | -- | -- | ||
| Hofer 2008 | 8-oxodGuo [nmol/mmol crea] | MS-MS | 2.30 (0.74) * | 2.78 (0.82) * | -- | -- | -- | -- | ||
| Jackson 2010 | spot | isoprostane [pg/g crea] | HPLC-MSMS | 275 (184) † | 335 (295) † | -- | -- | -- | -- | [39] |
| Jackson 2010 | H2O2 [umol/mg crea] | Colorimetric | 30.8 (15.4) † | 38.5 (53.8) † | -- | -- | -- | -- | ||
| Karstoft 2017 | 24 h | isoprostane [pg/mg crea] | ELISA | 1148 (127) * | 1051 (114) * | -- | -- | -- | -- | [40] |
| Lessiani 2016 | 12 h | isoprostane [pg/mg crea] | RIA | 320 (287–435) † | 209 (154–258) † | -- | -- | -- | -- | [41] |
| Margaritelis 2014 | spot | isoprostane [pg/ng crea] | ELISA | 690 (220) § | 950 (320) § | -- | -- | -- | -- | [42] |
| Margonis 2007 | spot | isoprostane [ng/mL] | ELISA | 1.65 (1.43;1.89) * | 3.90 (3.60;4.35) * | -- | -- | -- | -- | [43] |
| Medina 2012 | 24 h | Total isoprostanes [ng/24 h] | UPLC | males 12,920 (4790) § females 7700 (2900) § | 9380 (2910) § 8230 (1070) § | -- | -- | -- | -- | [44] |
| Medina 2012 | isoprostane [ng/24 h] | UPLC | males 1714.3 (723.7) § females 1476.2 (951.8) § | 1009.5 (485.5) § 809.5 (389.5) § | -- | -- | -- | -- | ||
| Medina 2012 | 8-iso-15(R)-PGF2α [ng/24 h] | UPLC | males 634.2 (451.2) § females 1341.5 (134.1) § | 1939 (841) § 902.4 (341.5) § | -- | -- | -- | -- | ||
| Medina 2012 | 2,3-dinor-8-iso PGF2α [ng/24 h] | UPLC | males 4000 (875) § females 2087 (725) § | 2887 (587.4) § 2824 (738) § | -- | -- | -- | -- | ||
| Medina 2012 | 2,3-dinor-11β-PGF2α [ng/24 h] | UPLC | males 3124.9 (1205) § females 2375 (772) § | 2295 (682) § 3454 (432) § | -- | -- | -- | -- | ||
| Mendoza-Núñez 2014 | spot | -- | -- | -- | -- | SOD [UI/L] | Colorimetric | 1.62 (0.83) * | 2.79 (1.6) * | [45] |
| Mendoza-Núñez 2014 | spot | -- | -- | -- | -- | TAS [mmol/L] | Colorimetric | 0.53 (0.33) * | 0.70 (0.35) * | |
| Mendoza-Núñez 2014 | spot | -- | -- | -- | -- | TNF-alpha [pg/mL] | Flow cytometry | 0.5119 (0.009) * | 4.2410 (0.435) * | |
| Mendoza-Núñez 2014 | spot | -- | -- | -- | -- | IL-1 beta [pg/mL] | Flow cytometry | 783.62 (174.9) * | 624.97 (196.7) * | |
| Mendoza-Núñez 2014 | spot | -- | -- | -- | -- | IL-6 [pg/mL] | Flow cytometry | 18.66 (7.25) * | 4.76 (1.93) * | |
| Mendoza-Núñez 2014 | spot | -- | -- | -- | -- | IL-8 [pg/mL] | Flow cytometry | 4971.2 (835.0) * | 2242.4 (330.0) * | |
| Mendoza-Núñez 2014 | spot | -- | -- | -- | -- | IL-10 [pg/mL] | Flow cytometry | 0.21 (2.5) * | 2.9 (1.5) * | |
| Mendoza-Núñez 2014 | spot | -- | -- | -- | -- | Lipid hydroperoxidase [umol/L] | 0.11 (0.07) § | 0.14 (0.09) § | ||
| Mercken 2005 | spot | MDA [μmol/mmol crea] | HPLC | healthy subjects 0.28 (0.04) * COPD patients 0.38 (0.02) * | 0.29 (0.03) * 0.52 (0.07) * | -- | -- | -- | -- | [46] |
| Mikami 2000 | spot | Allantoin [μmol/mg crea] | HPLC | 40% VOmax 0.08 (0.002) * 100% VO2max 0.08 (0.001) * | 0.09 (0.001) * 0.08 (0.001) * | -- | -- | -- | -- | [47] |
| Mikami 2000 | TBARS [μmol/mg crea] | HPLC | 40% VO2max 2.80 (0.8) * 100% VO2max 2.90 (0.4) * | 2.76 (0.6) * 2.57 (0.4) * | -- | -- | -- | -- | ||
| Mikami 2000 | Urate [μmol/mg crea] | UA B-test Wako | 40% VO2max 0.40 (0.06) * 100% VO2max 0.42 (0.06) * | 0.40 (0.06) * 0.37 (0.07) * | -- | -- | -- | -- | ||
| Nemoto 2014 | spot | 8-OH-dG [ng/mg crea] | ELISA | II–III COPD severity 16.6 (2.2) * IV COPD severity 14.6 (1.8) * | 17.8 (2.3) * 24.3 (2.6) * | -- | -- | -- | -- | [48] |
| Nikolaidis 2012 | spot | isoprostane [pg/ng crea] | ELISA | muscle damaging 588.8 (315.4) * non-muscle damaging 352.8 (196.3) * | 1126.17 (324.78) * 967.29 (233.64) * | -- | -- | -- | -- | [49] |
| Nikolaidis 2013 | spot | isoprostane [pg/mg crea] | ELISA | young 430.4 (30.4) * elederly 560.9 (39) * | 434.8 (39) * 587 (47) * | -- | -- | -- | -- | [50] |
| Nojima 2008 | spot | 8-OH-dG [ng/mg crea] | ELISA | Exercise in a fitness centre 10.3 (1.1) * Self-paced exercise 11.3 (1.4) * | 9.3 (1.0) * 8.1 (0.8) * | -- | -- | -- | -- | [51] |
| Orhan 2004 | 24 h | 8-OH-dG [nmol/12 h] | ELISA | 12.14 (5) * | 47.4 (15) * | -- | -- | -- | -- | [52] |
| Orhan 2004 | MDA [nmol/12 h] | HPLC | 1.45 (0.33) * | 1.74 (0.35) * | ||||||
| Parise 2005 | spot | 8-OH-dG [ng/g crea] | ELISA | 10783 (5856) § | 8897 (4030) § | -- | -- | -- | -- | [53] |
| Poulsen 1996 | spot | 8-OH-dG [nmol/mmol crea] | HPLC | 1.03 (0.59) § | 1.25 (0.59) § | -- | -- | -- | -- | [54] |
| Radák 2000 | spot | 8-OH-dG [ng/mL] | ELISA | 14.74 (2.50) § | 19.15 (2.50) § | -- | -- | -- | -- | [55] |
| Rall 2000 | 24 h | 8-OH-dG [nmol/day] | ELISA | healty elderly 24.82 (16.35) § rheumatoid arthritis 45.43 (16.67) § | 15.50 (10.74) § 30.11 (31.17) § | -- | -- | -- | -- | [56] |
| Rietjens 2007 | spot | isoprostane [nmol/mmol crea] | ELISA | 0.117 (0.021) * | 0.164 (0.030) * | -- | -- | -- | -- | [57] |
| Rodrigues de Araujo 2018 | spot | -- | -- | -- | -- | TBARS [nmol/mL] | Colorimetric | 9.20 (3.13) § | 8.50 (2.43) § | [58] |
| Rodrigues de Araujo 2018 | spot | -- | -- | -- | -- | MDA [uM] | Colorimetric | 5.40 (2.15) § | 5.37 (1.52) § | |
| Rodrigues de Araujo 2018 | spot | -- | -- | -- | -- | GSH [uM] | Colorimetric | 54.78 (3.57) § | 54.55 (9.57) § | |
| Rodrigues de Araujo 2018 | spot | -- | -- | -- | -- | GSSG [uM] | Colorimetric | 2.04 (1.18) § | 2.10 (1.13) § | |
| Rodrigues de Araujo 2018 | spot | -- | -- | -- | -- | UA [ug/dL] | Colorimetric | 2.66 (1.33) § | 1.66 (0.92) § | |
| Rodrigues de Araujo 2018 | spot | -- | -- | -- | -- | SOD [U/g dL−1] | Spectrophotometric | 32.6 (43.9) § | 37.4 (42.1) § | |
| Rodrigues de Araujo 2018 | spot | -- | -- | -- | -- | CAT [U/g dL−1] | Colorimetric | 1.65 (1.53) § | 1.66 (2.90) § | |
| Rowlands 2012 | spot | isoprostane [pg/umol crea] | ELISA | 84.9 (28.6) § | 112.6 (52.7) § | -- | -- | -- | -- | [59] |
| Rowlands 2012 | 8-OH-dG [pg/umol crea] | ELISA | 11166 (5613) § | 9045 (4813) § | -- | -- | -- | -- | ||
| Samia 2014 | spot | 8-OH-dG [nmol/L] | ELISA | 23.78 (1.95) § | 25.96 (1.33) § | -- | -- | -- | -- | [60] |
| Samjoo 2013 | 24 h | 8-OH-dG [ng/d] | ELISA | healthy 10399 (1600) * obese 14879 (2720) * | 10319 (2480) * 12639 (2240) * | -- | -- | -- | -- | [61] |
| Samjoo 2013 | isoprostane [ng/day] | ELISA | healthy 1087 (104) * obese 1479 (272) * | 935 (88) * 959 (136) * | -- | -- | -- | -- | ||
| Santilli 2013 | 24 h | isoprostane [pg/mg crea] | RIA | 325 (287–508) * | 218 159–335) * | -- | -- | -- | -- | [62] |
| Schmitz 2008 | 24 h | isoprostane [pmol/mg crea] | GC-MS | 78.79 (52.13) § | 52.19 (19.17) § | -- | -- | -- | -- | [63] |
| Sumida 1997 | 24 h | 8-OH-dG [nmol/mmol crea] | HPLC | treadmill exhaustion 1.67 (0.18) * bycycle exhaustion 1.93 (0.09) * running for 20 km 1.66 (0.16) * | 1.61 (0.17) * 1.89 (0.18) * 1.49 (0.16) * | -- | -- | -- | -- | [64] |
| Vempati 2009 | spot | isoprostane [pg/mg crea] | ELISA | 455.4 (991) † | 26.9 (210) † | -- | -- | -- | -- | [65] |
| Vezzoli 2014 | spot | 8-OH-dG [ng/mg crea] | ELISA | moderate intensity 5.50 (0.66) § high intensity 4.52 (0.50) § | 4.16 (0.40) § 3.18 (0.34) § | -- | -- | -- | -- | [66] |
| Vezzoli 2016 | spot | isoprostane [ng/mg crea] | ELISA | 50 km running 0.42 (0.13) § 100 km running 0.40 (0.13) § | 0.60 (0.14) § 0.94 (0.13) § | -- | -- | -- | -- | [67] |
| Vezzoli 2016 | 8-OH-dG [ng/mg crea] | ELISA | 50 km running 4.38 (1.16) § 100 km running 4.50 (0.94) § | 7.48 (1.16) § 11.61 (1.18) § | -- | -- | -- | -- | ||
| Viana-Gomes 2018 | spot | -- | -- | -- | -- | TBARS [umol/L] | Colorimetric | 2.1 (0.3) * | 3.1 (0.4) * | [68] |
| Viana-Gomes 2018 | -- | -- | -- | -- | TAC [umol/L] | Colorimetric | 41.8 (2.3) * | 44.2 (2.8) * | ||
| Viana-Gomes 2018 | -- | -- | -- | -- | UA [IU/dL] | Colorimetric | 2.5 (0.3) * | 3.1 (0.4) * | ||
| Viguie 1993 | 24 h | 8-OH-dG [pmol/kg/day] | HPLC | 405.3 (44.8) * | 306.9 (54) * | -- | -- | -- | -- | [69] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Squillacioti, G.; Guglieri, F.; Colombi, N.; Ghelli, F.; Berchialla, P.; Gardois, P.; Bono, R. Non-Invasive Measurement of Exercise-Induced Oxidative Stress in Response to Physical Activity. A Systematic Review and Meta-Analysis. Antioxidants 2021, 10, 2008. https://doi.org/10.3390/antiox10122008
Squillacioti G, Guglieri F, Colombi N, Ghelli F, Berchialla P, Gardois P, Bono R. Non-Invasive Measurement of Exercise-Induced Oxidative Stress in Response to Physical Activity. A Systematic Review and Meta-Analysis. Antioxidants. 2021; 10(12):2008. https://doi.org/10.3390/antiox10122008
Chicago/Turabian StyleSquillacioti, Giulia, Fulvia Guglieri, Nicoletta Colombi, Federica Ghelli, Paola Berchialla, Paolo Gardois, and Roberto Bono. 2021. "Non-Invasive Measurement of Exercise-Induced Oxidative Stress in Response to Physical Activity. A Systematic Review and Meta-Analysis" Antioxidants 10, no. 12: 2008. https://doi.org/10.3390/antiox10122008