
A Naturalistic Intervention to Promote Executive Functions in Primary School Children: A Pilot Study
 and
and
Abstract
:1. Introduction
1.1. Naturalistic Intervention and Executive Functions
1.2. Goal Management Training
1.3. Empirical Evidence
2. Materials and Methods
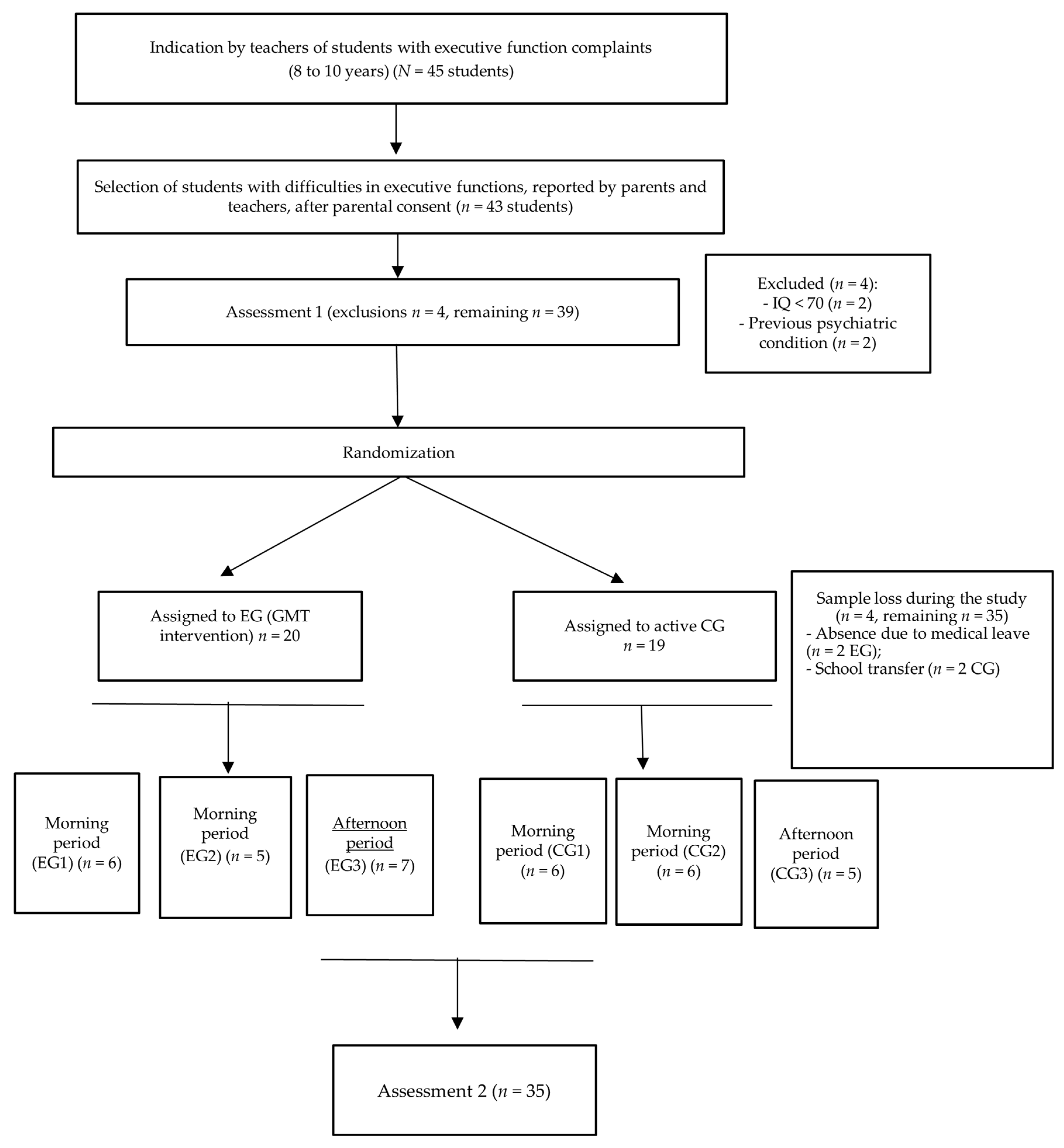
2.1. Participants
2.2. Assessment Instruments
2.3. Intervention Tools
2.3.1. Experimental Group: Intervention in Executive Functions
2.3.2. Control Group
2.4. Procedure
2.5. Analysis of the Results
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tiede, G.; Walton, K.M. Meta-analysis of naturalistic developmental behavioral interventions for young children with autism spectrum disorder. Autism 2019, 23, 2080–2095. [Google Scholar] [CrossRef]
- Barnett, D.W.; Carey, K.T.; Hall, J.D. Naturalistic intervention design for young children: Foundations, rationales, and strategies. Top. Early Child. Spec. Educ. 1993, 13, 430–444. [Google Scholar] [CrossRef]
- Dubin, A.H.; Lieberman-Betz, R.G. Naturalistic interventions to improve prelinguistic communication for children with autism spectrum disorder: A systematic review. Rev. J. Autism. Dev. Disord. 2020, 7, 151–167. [Google Scholar] [CrossRef]
- Lei, J.; Ventola, P. Pivotal response treatment for autism spectrum disorder: Current perspectives. Neuropsychiatr. Dis. Treat. 2017, 13, 1613–1626. [Google Scholar] [CrossRef]
- d’Apice, K.; Latham, R.M.; von Stumm, S. A naturalistic home observational approach to children’s language, cognition, and behavior. Dev. Psychol. 2019, 55, 1414. [Google Scholar] [CrossRef]
- Ashbaugh, K.; Koegel, R.L. Naturalistic interventions. In Encyclopedia of Autism Spectrum Disorders; Springer International Publishing: Heiligkreuz, Switzerland, 2021. [Google Scholar]
- Zelazo, P.D.; Blair, C.B.; Willoughby, M.T. Executive Function: Implications for Education (NCER 2017–2000); National Center for Education Research: Washington, DC, USA, 2016. Available online: https://ies.ed.gov/ncer/pubs/20172000/pdf/20172000.pdf (accessed on 10 November 2023).
- Zelazo, P.D.; Carlson, S.M. Hot and cool executive function in childhood and adolescence: Development and plasticity. Child Dev. Perspect. 2012, 6, 354–360. [Google Scholar] [CrossRef]
- Cardoso, C.D.O.; Seabra, A.G.; Gomes, C.M.A.; Fonseca, R.P. Program for the neuropsychological stimulation of cognition in students: Impact, effectiveness, and transfer effects on student cognitive performance. Front. Psychol. 2019, 10, 1784–1798. [Google Scholar] [CrossRef]
- Cardoso, C.D.O.; Dias, N.; Senger, J.; Colling, A.P.C.; Seabra, A.G.; Fonseca, R.P. Neuropsychological stimulation of executive functions in children with typical development: A systematic review. Appl. Neuropsychol. Child 2018, 7, 61–81. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive functions. In Handbook of Clinical Neurology; Neurocognitive Development: Normative Development; North-Holland Publishing Company: Amsterdam, The Netherlands, 2020; pp. 225–240. [Google Scholar] [CrossRef]
- Koşkulu-Sancar, S.; van de Weijer-Bergsma, E.; Mulder, H.; Blom, E. Examining the role of parents and teachers in executive function development in early and middle childhood: A systematic review. Dev. Rev. 2023, 67, 101063. [Google Scholar] [CrossRef]
- Otero, T.M.; Barker, L.A.; Naglieri, J.A. Executive function treatment and intervention in schools. Appl. Neuropsychol. Child 2014, 3, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A.; Barnett, W.S.; Thomas, J.; Munro, S. Preschool program improves cognitive control. Science 2007, 318, 1387–1388. [Google Scholar] [CrossRef]
- Panayiotou, M.; Humphrey, N.; Wigelsworth, M. An empirical basis for linking social and emotional learning to academic performance. Contemp. Educ. Psychol. 2019, 56, 193–204. [Google Scholar] [CrossRef]
- Dias, N.M.; Seabra, A.G. Intervention for executive functions development in early elementary school children: Effects on learning and behaviour, and follow-up maintenance. J. Educ. Psychol. 2017, 37, 468–486. [Google Scholar] [CrossRef]
- Watts, T.W.; Gandhi, J.; Ibrahim, D.A.; Masucci, M.D.; Raver, C.C. The Chicago School Readiness Project: Examining the long-term impacts of an early childhood intervention. PLoS ONE 2018, 13, e0200144. [Google Scholar] [CrossRef]
- Diamond, A.; Lee, K. Interventions shown to aid executive function development in children 4 to 12 years old. Science 2011, 333, 959–964. [Google Scholar] [CrossRef]
- Levine, B.; Schweizer, T.A.; O’Connor, C.; Turner, G.; Gillingham, S.; Stuss, D.T.; Robertson, I.H. Rehabilitation of executive functioning in patients with frontal lobe brain damage with goal management training. Front. Hum. Neurosci. 2011, 5, 9. [Google Scholar] [CrossRef]
- Robertson, I.H. Goal Management Training: A Clinical Manual; PsyConsult: Cambridge, UK, 1996. [Google Scholar]
- Duncan, J.; Humphreys, G.W. Visual search and stimulus similarity. Psychol. Rev. 1989, 96, 433. [Google Scholar] [CrossRef]
- Lodha, S.; Gupta, R. Mindfulness, attentional networks, and executive functioning: A review of interventions and long-term meditation practice. J. Cogn. Enhanc. 2022, 6, 531–548. [Google Scholar] [CrossRef]
- Marulis, L.M.; Baker, S.T.; Whitebread, D. Integrating metacognition and executive function to enhance young children’s perception of and agency in their learning. Early Child. Res. Q. 2020, 50, 46–54. [Google Scholar] [CrossRef]
- Tornås, S.; Løvstad, M.; Solbakk, A.K.; Schanke, A.K.; Stubberud, J. Goal management training combined with external cuing as a means to improve emotional regulation, psychological functioning, and quality of life in patients with acquired brain injury: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2016, 97, 1841–1852. [Google Scholar] [CrossRef] [PubMed]
- Stamenova, V.; Levine, B. Effectiveness of goal management training® in improving executive functions: A meta-analysis. Neuropsychol. Rehabil. 2018, 29, 1569–1599. [Google Scholar] [CrossRef]
- Nunes, L.G.; Seabra, A.G. Development of a Program based on Goal Management Training for Adolescents with Executive Dysfunctions Complaints. Span. J. Psychol. 2021, 24, e20. [Google Scholar] [CrossRef]
- Trevisan, B.T.; Berberian, A.A.; Dias, N.M.; Roama-Alves, R.J.; Seabra, A.G. Development and psychometric properties of the Difficulties in Executive Functions, Regulation and Delay Aversion Inventory-Version for children and adolescents. Aval. Psicol. 2022, 21, 261–272. [Google Scholar]
- Dias, N.M.; Trevisan, B.T.; León, C.B.R.; Prust, A.P.; Seabra, A.G. Can executive functions predict behavior in preschool children? Psychol. Neurosci. 2017, 10, 383–393. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Woerner, W.; Fleitlich-Bilyk, B.; Martinussen, R.; Fletcher, J.; Cucchiaro, G.; Dalgalarrondo, P.; Tannock, R. The Strengths and Difficulties Questionnaire overseas: Evaluations and applications of the SDQ beyond Europe. Eur. Child Adolesc. Psychiatry 2004, 13, ii47–ii54. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Abbreviated Scale of Intelligence; Psychological Corporation: San Antonio, TX, USA, 1999. [Google Scholar]
- Trentini, C.M.; Yates, D.B.; Heck, V.S. Escala de Inteligência Wechsler Abreviada (WASI): Manual Profissional; Casa do Psicólogo: São Paulo, Brazil, 2014. [Google Scholar]
- Wechsler, D. Escala Wechesler de Inteligência Para Crianças-WISC IV: Manual Técnico; Adaptação e Padronização de Uma Amostra Brasileira: Maria de Lourdes; Casa do Psicólogo: São Paulo, Brazil, 2014. [Google Scholar]
- Trevisan, B.T. Atenção e Controle Inibitório em Pré-Escolares e Correlação Com Indicadores de Desatenção e Hiperatividade. Master’s Thesis, Universidade Presbiteriana Mackenzie, São Paulo, Brazil, 2010. [Google Scholar]
- Sedó, M.A.; De Paula, J.J.; Malloy-Diniz, L.F. FDT: O Teste dos Cinco Dígitos; Hogreffe CETTEP: São Paulo, Brazil, 2015. [Google Scholar]
- Miotto, E.C. Avaliação Neuropsicológica e funções cognitivas. In Neuropsicologia Clinica; Miotto, E.C., Lucia, M.C.S., Scaff, M., Eds.; Roca: São Paulo, Brazill, 2012; pp. 8–9. [Google Scholar]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. nparLD: An R Software Package for the nonparametric analysis of Longitudinal Data in Factorial experiments. J. Stat. Softw. 2012, 50, 23. [Google Scholar] [CrossRef]
- Brunner, E.; Konietschke, F.; Pauly, M.; Puri, M.L. Rank-based procedures in factorial designs: Hypotheses about non-parametric treatment effects. J. R. Stat. Soc. Ser. B Stat. Methodol. 2017, 79, 1463–1485. [Google Scholar] [CrossRef]
- Vargha, A.; Delaney, H.D. A critique and improvement of the CL common language effect size statistics of McGraw and Wong. J. Educ. Behav. Stat. 2000, 25, 101–132. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.; Robertson, I.H.; Clare, L.; Carter, G.; Hong, J.; Wilson, B.A.; Stuss, D.T. Rehabilitation of executive functioning: An experimental–clinical validation of Goal Management Training. J. Int. Neuropsychol. Soc. 2000, 6, 299–312. [Google Scholar] [CrossRef]
- Diamond, A.; Ling, D.S. Conclusions about interventions, programs, and approaches for improving executive functions that appear justified and those that, despite much hype, do not. Dev. Cogn. Neurosci. 2016, 18, 34–48. [Google Scholar] [CrossRef]
- Pandey, A.; Hale, D.; Das, S.; Goddings, A.L.; Blakemore, S.J.; Viner, R.M. Effectiveness of Universal Self-Regulation-Based Interventions in Children and Adolescents: A Systematic Review and Meta-analysis. JAMA Pediatr. 2018, 172, 566–575. [Google Scholar] [CrossRef]
- Benzing, V.; Schmidt, M.; Jäger, K.; Egger, F.; Conzelmann, A.; Roebers, C.M.A. Classroom intervention to improve executive functions in late primary school children: Too ‘old’ for improvements? Br. J. Educ. Psychol. 2019, 89, 225–238. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Module | Structure | Description |
|---|---|---|
| (1) Attentional skill | Number of sessions | 4 |
| Number of activities | 12 | |
| Tool | Observation lens | |
| Objective of the tool | Promoting self-monitoring | |
| Description of psychoeducation activities | Transmission of the overall concept of executive functions to children; promoting awareness of errors due to lack of attention and the consequences of these errors | |
| Description of cognitive training activities | Formulation of goals and intervention strategies in attentional skills; self-monitoring training; mindfulness practice to stimulate sustained and selective attention | |
| Description of homework tasks | Self-monitoring practice according to the list of goals formulated in the first session; mindfulness | |
| Bridges between sessions and review of homework tasks. | Reviewing the concepts learned in the previous session by asking questions to relate to the current session; checking whether the child completed the homework, and discussing successes and difficulties | |
| (2) Inhibitory control skill | Number of sessions | 3 |
| Number of activities | 8 | |
| Tool | “Stop!” card | |
| Objective of the tool | Promoting inhibitory control | |
| Description of psychoeducation activities | Introduction to the concept of being on “autopilot”; developing the ability to control impulses in automated situations; application of metacognitive strategies to develop self-control | |
| Description of cognitive training activities | Practice of “Stop the autopilot!” aimed at stimulating attention, self-monitoring, and inhibitory control; a “stop” game for inhibitory control training, applying self-monitoring; reading colored numbers to stimulate inhibitory control; mindfulness practice | |
| Description of homework tasks | Practice stopping the “autopilot” in predetermined situations in the intervention planning; mindfulness | |
| Bridges between sessions and review of homework tasks. | Reviewing the concepts learned in the previous session by asking questions to relate to the current session; checking whether the child completed the homework, and discussing successes and difficulties | |
| (3) Working memory skill | Number of sessions | 2 |
| Number of activities | 5 | |
| Tool | Mind agenda | |
| Objective of the tool | Promoting working memory | |
| Description of psychoeducation activities | Introducing the concept of working memory; applying mnemonic strategies | |
| Description of cognitive training activities | Stimulating visual and auditory working memory through games with standardized sounds; using the metacognitive strategy of stopping and consulting the mind’s agenda at timed intervals; mindfulness | |
| Description of homework tasks | Daily practice of the stop-and-consult strategies at timed intervals in the mind agenda; mindfulness | |
| Bridges between sessions and review of homework tasks. | Reviewing the concepts learned in the previous session; assessing the application of these concepts in the week before the session | |
| (4) Goal setting/prioritization skill | Number of sessions | 2 |
| Number of activities | 6 | |
| Tool | Objective card | |
| Objective of the tool | Promoting goal representation | |
| Description of psychoeducation activities | Introducing the concept of goal selection; presenting the metacognitive strategy (stop, breathe, and ask yourself “What is my goal?”) | |
| Description of cognitive training activities | Activities involving pencil and paper; categorizing cards by color using the metacognitive strategy; mindfulness | |
| Description of homework tasks | Practicing “goal setting” using the self-instruction strategy; mindfulness | |
| Bridges between sessions and review of homework tasks. | Reviewing the concepts learned in the previous session; checking whether the planned goals were achieved | |
| (5) Decision-making skill | Number of sessions | 2 |
| Number of activities | 4 | |
| Tool | Decision balance | |
| Objective of the tool | Promoting decision-making | |
| Description of psychoeducation activities | Introducing the concept of decision-making and its implications in automated mechanisms | |
| Description of cognitive training activities | Activity “decide the end of the story” to train decision-making; using the “decision balance” technique to deal with advantages and disadvantages; mindfulness | |
| Description of homework tasks | Implementing the “decision balance” technique in the child’s daily activities to promote generalization; mindfulness | |
| Bridges between sessions and review of homework tasks. | Reviewing the concepts learned in the previous session about decision-making; checking the application of these concepts in the week before the session | |
| (6) Planning/organization skill | Number of sessions | 3 |
| Number of activities | 4 | |
| Tool | Steps to the goal | |
| Objective of the tool | Promoting the construction of sub-goals | |
| Description of psychoeducation activities | Introducing the concept of breaking down a goal into sub-goals; presenting metacognitive strategies | |
| Description of cognitive training activities | Activity “organizing the backpack” to stimulate planning/organization; dividing complex tasks into smaller ones; self-assessment of performance; mindfulness | |
| Description of homework tasks | Implementing the learned strategies in everyday activities | |
| Bridges between sessions and review of homework tasks. | Reviewing the main concepts learned and linking them with the homework; assessing the difficulties or successes |
| Education | N | Sex | Age | Race | |
|---|---|---|---|---|---|
| Experimental Group | 3th grade | 11 | 6 M; 5 F | 08 | 09 White; 02 Black |
| 4th grade | 02 | 1 M; 1 F | 09 | 02 White | |
| 5th grade | 05 | 3 M; 2 F | 10 | 01 Black; 04 White | |
| Control Group | 3th grade | 10 | 6 M; 4 F | 08 | 10 White |
| 4th grade | 03 | 2 M; 1 F | 10 | 01 Black; 02 White | |
| 5th grade | 04 | 2 M; 2 F | 10 | 02 Black; 02 White |
| Variable | Group | Mean (SD) Pre-Test | Mean (SD) Post-Test | Time p-Value | Time*Group p-Value | Relative Treatment Effect (RTE) |
|---|---|---|---|---|---|---|
| IQ total | E | 89.94 (10.95) | 98.06 (14.19) | <0.001 | 0.736 | 0.60 |
| C | 89.71 (10.59) | 97.47 (14.63) | ||||
| Digits | E | 7.17 (2.50) | 8.94 (2.13) | 0.053 | 0.044 | 0.61 |
| C | 7.94 (2.13) | 7.65 (2.50) | ||||
| FDT Inhibition | E | 45.28 (27.84) | 63.61 (35.39) | 0.021 | 0.209 | 0.58 |
| C | 55.29 (29.45) | 61.18 (33.38) | ||||
| FDT Flexibility | E | 43.89 (32.43) | 70.28 (29.28) | 0.008 | 0.073 | 0.64 |
| C | 51.06 (27.74) | 56.47 (29.36) | ||||
| Go/No-go Go items score | E | 0.91 (0.03) | 0.92 (0.05) | 0.718 | 0.363 | 0.58 |
| C | 0.85 (0.17) | 0.82 (0.15) | ||||
| Go/No-go No-go items score | E | 0.87 (0.08) | 0.93 (0.04) | 0.051 | 0.002 | 0.61 |
| C | 0.91 (0.06) | 0.89 (0.11) | ||||
| Go/No-go Go items reaction time | E | 0.59 (0.06) | 0.58 (0.06) | 0.432 | 0.447 | 0.47 |
| C | 0.62 (0.09) | 0.61 (0.09) | ||||
| Go/No-go No-Go items reaction time | E | 0.47 (0.07) | 0.44 (0.09) | 0.978 | 0.348 | 0.44 |
| C | 0.47 (0.10) | 0.59 (0.37) |
| Variable | Group | Mean (SD) Pre-Test | Mean (SD) Post-Test | Time p-Value | Time*Group p-Value | Relative Treatment Effect (RTE) |
|---|---|---|---|---|---|---|
| IFERA Parents | ||||||
| Inhibitory control | E | 3.22 (0.83) | 2.83 (0.79) | 0.233 | 0.05 | 0.39 |
| C | 3.12 (0.60) | 3.24 (0.81) | ||||
| Working memory | E | 3.12 (0.95) | 2.81 (0.94) | 0.165 | 0.252 | 0.43 |
| C | 3.04 (0.97) | 3.05 (1.10) | ||||
| Cognitive flexibility | E | 3.00 (0.87) | 2.71 (0.67) | 0.107 | 0.297 | 0.42 |
| C | 2.92 (0.71) | 2.90 (0.90) | ||||
| Delay aversion | E | 3.27 (0.96) | 2.98 (0.87) | 0.555 | 0.611 | 0.45 |
| C | 3.17 (0.73) | 3.16 (0.91) | ||||
| State regulation | E | 3.53 (0.89) | 3.23 (0.87) | 0.064 | 0.434 | 0.41 |
| C | 3.58 (0.58) | 3.42 (0.90) | ||||
| Total | E | 3.24 (0.71) | 2.93 (0.75) | 0.084 | 0.211 | 0.41 |
| C | 3.19 (0.45) | 3.17 (0.67) | ||||
| IFERA Teachers | ||||||
| Inhibitory control | E | 3.54 (0.72) | 2.71 (0.60) | <0.001 | 0.083 | 0.28 |
| C | 3.74 (0.78) | 3.63 (1.50) | ||||
| Working memory | E | 3.73 (0.85) | 2.77 (0.80) | <0.001 | 0.822 | 0.31 |
| C | 3.93 (0.84) | 3.13 (0.74) | ||||
| Cognitive flexibility | E | 3.65 (0.50) | 2.88 (0.70) | <0.001 | 0.082 | 0.31 |
| C | 3.65 (0.55) | 3.37 (0.80) | ||||
| Delay aversion | E | 3.24 (0.87) | 2.18 (0.91) | <0.001 | 0.041 | 0.30 |
| C | 3.25 (0.60) | 2.97 (1.11) | ||||
| State regulation | E | 3.76 (0.72) | 2.88 (0.98) | <0.001 | 0.05 | 0.34 |
| C | 3.57 (0.65) | 3.41 (0.82) | ||||
| Total | E | 3.57 (0.51) | 2.69 (0.62) | <0.001 | 0.029 | 0.25 |
| C | 3.63 (0.48) | 3.31 (0.71) | ||||
| Variable | Group | Mean (SD) Pre-Test | Mean (SD) Post-Test | Time p-Value | Time*Group p-Value | Relative Treatment Effect (RTE) |
|---|---|---|---|---|---|---|
| SDQ Parents | ||||||
| Total | E | 25.59 (3.87) | 23.76 (5.08) | 0.397 | 0.609 | 0.44 |
| C | 24.87 (9.49) | 25.87 (11.11) | ||||
| Emotional symptoms | E | 3.94 (1.56) | 3.35 (1.69) | 0.341 | 0.294 | 0.42 |
| C | 4.45 (2.35) | 4.55 (3.06) | ||||
| Conduct problems | E | 3.47 (1.01) | 3.41 (1.42) | 0.781 | 0.429 | 0.48 |
| C | 3.53 (1.77) | 4.12 (2.62) | ||||
| Hyperactivity | E | 5.06 (1.81) | 3.94 (1.48) | 0.676 | 0.013 | 0.39 |
| C | 4.60 (2.23) | 5.63 (2.43) | ||||
| Relationship problems | E | 4.71 (0.92) | 5.23 (1.71) | 0.514 | 0.058 | 0.51 |
| C | 5.82 (2.25) | 4.93 (2.28) | ||||
| Prosocial behavior | E | 8.41 (2.00) | 7.82 (1.78) | 0.458 | 0.264 | 0.48 |
| C | 7.51 (2.28) | 7.66 (2.24) | ||||
| SDQ Teachers | ||||||
| Total | E | 20.61 (4.54) | 19.89 (3.48) | 0.971 | 0.631 | 0.51 |
| C | 18.73 (4.71) | 20.07 (4.38) | ||||
| Emotional symptoms | E | 3.61 (2.59) | 3.00 (1.68) | 0.809 | 0.710 | 0.49 |
| C | 3.33 (2.87) | 3.46 (2.75) | ||||
| Conduct problems | E | 3.72 (2.05) | 3.17 (1.80) | 0.911 | 0.075 | 0.44 |
| C | 3.53 (1.73) | 4.07 (2.12) | ||||
| Hyperactivity | E | 5.22 (1.93) | 4.94 (1.80) | 0.808 | 0.292 | 0.48 |
| C | 4.73 (1.87) | 5.13 (1.30) | ||||
| Relationship problems | E | 3.89 (2.17) | 4.39 (1.38) | 0.139 | 0.368 | 0.58 |
| C | 3.76 (1.64) | 3.88 (2.18) | ||||
| Prosocial behavior | E | 7.06 (1.95) | 7.89 (2.45) | 0.132 | 0.174 | 0.61 |
| C | 6.13 (3.54) | 6.60 (2.64) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souza, J.B.; Trevisan, B.T.; Nunes, L.G.; Machado, W.L.; Seabra, A.G. A Naturalistic Intervention to Promote Executive Functions in Primary School Children: A Pilot Study. Brain Sci. 2024, 14, 70. https://doi.org/10.3390/brainsci14010070
Souza JB, Trevisan BT, Nunes LG, Machado WL, Seabra AG. A Naturalistic Intervention to Promote Executive Functions in Primary School Children: A Pilot Study. Brain Sciences. 2024; 14(1):70. https://doi.org/10.3390/brainsci14010070
Chicago/Turabian StyleSouza, Jonatas B., Bruna T. Trevisan, Liana G. Nunes, Wagner L. Machado, and Alessandra G. Seabra. 2024. "A Naturalistic Intervention to Promote Executive Functions in Primary School Children: A Pilot Study" Brain Sciences 14, no. 1: 70. https://doi.org/10.3390/brainsci14010070