
Exploring the Relationship between Mood Disorders and Coexisting Health Conditions: The Focus on Nutraceuticals


Abstract
:1. Introduction
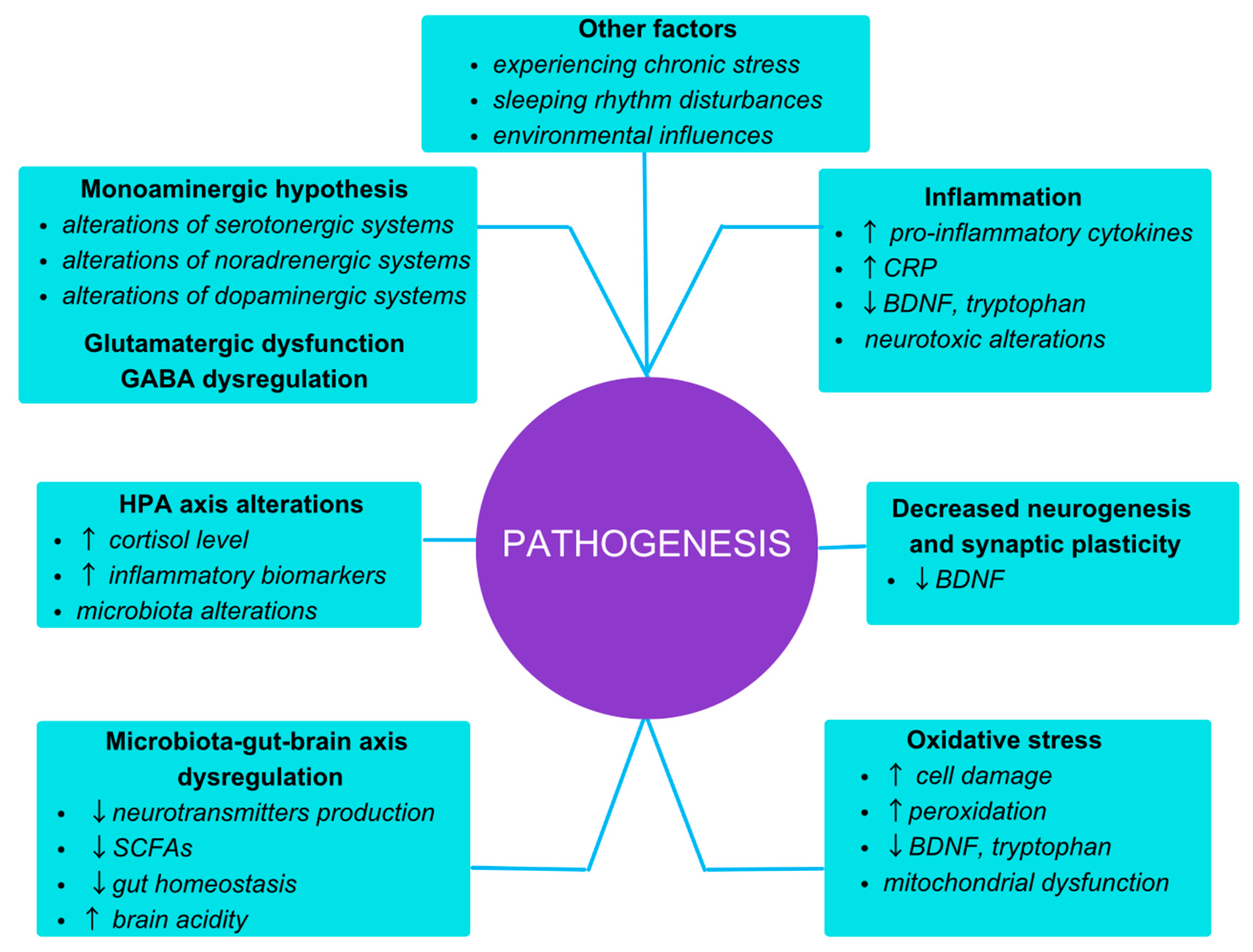
2. Pathogenesis

3. The Concept of Comorbidity and Its Implication for Disease Prognosis and Modifiable Factors
4. Body Weight and Compliance with Medication
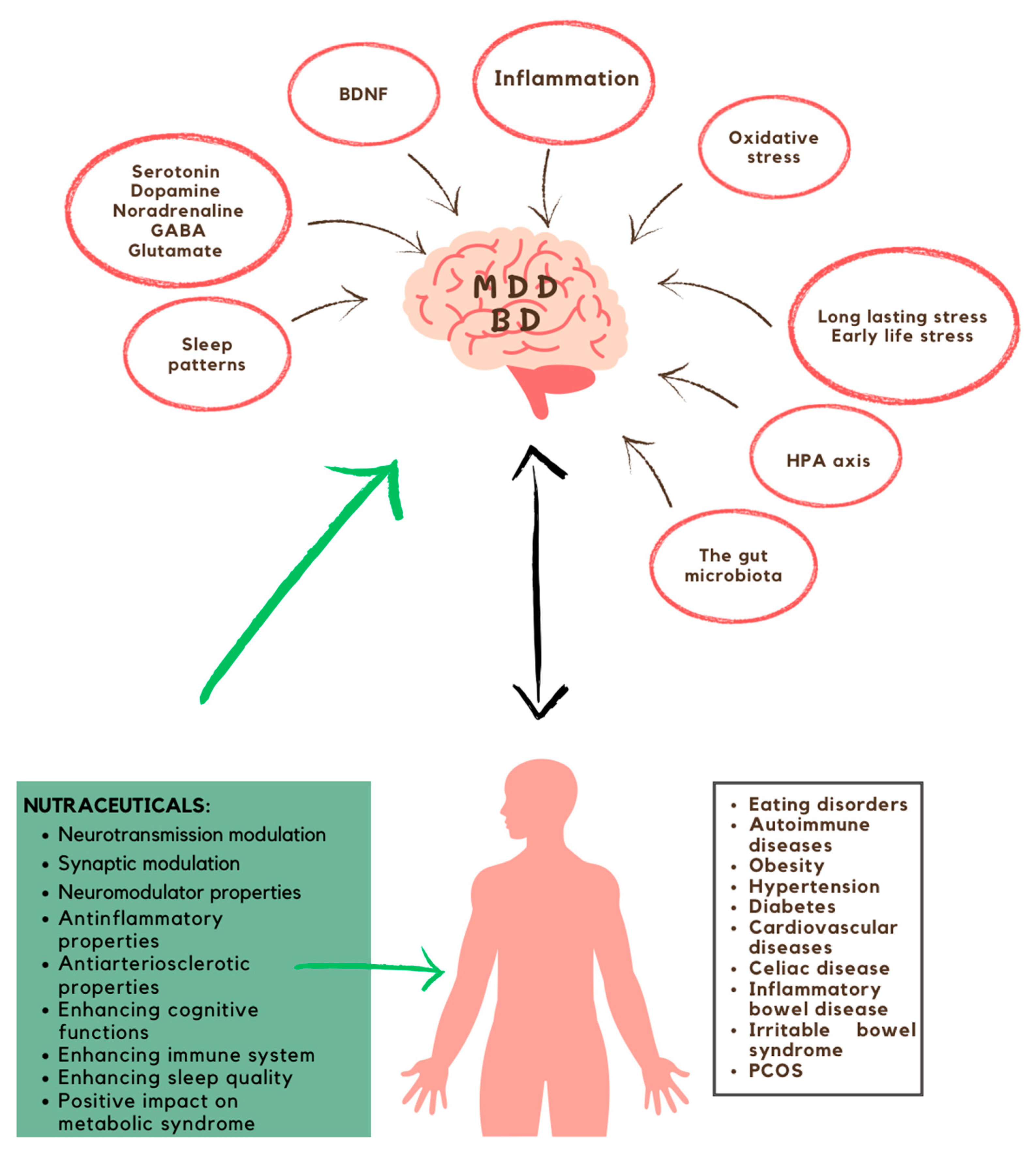
5. Nutraceuticals and Their Impact on Mood Disorders

{kind=link}
{kind=link}
| Major Depressive Disorder | Bipolar Disorder | |
| Vitamin D A sterol-derived nutritional compound, comprising a spectrum of 50 metabolites. Vitamin D is essential for calcium absorption in the gut and maintaining adequate calcium and phosphate concentrations in the blood.
| Participating in the neurotransmitters synthesis Enhancing the immune system Enhancing neurogenesis | |
| 1500–4000 IU daily 4 | Lack of data | |
| Expected to offer heightened benefits during the winter season [13]. | ||
| Omega-3 fatty acids Polyunsaturated fatty acids, including eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), are indispensable nutritional compounds that have numerous health benefits, including reducing inflammation and supporting brain health. They are mainly acquired through dietary intake.
| Neurotransmission modulation Enhancing neurogenesis Enhancing immune system Preserving the integrity of the neuronal cell membrane | |
| 1–2 g of eicosapentaenoic acid 1,8 | 1–2 g of eicosapentaenoic acid 3 | |
| There is a lack of evidence supporting a reduction in mania or hypomania; however, it may be still efficacious for individuals with elevated inflammation and/or obesity [13]. | ||
| Probiotics Live microorganisms which, while being administered in optimal doses, bestow a health benefit upon the host organism.
| The production and control of neurotransmitters Enhancing cognitive functions Enhancing immune system Improving BDNF levels HPA axis modulation Reduction of pro-inflammatory bacteria Mitigating the adverse effect of antibiotic administration | |
| 1–10 billion units daily 2,5 | Lack of data | |
| The optimal probiotic strains for treating depression have not been established [13]. | ||
| Zinc A trace mineral essential playing a pivotal role in numerous fundamental physiological functions; it is known as a cofactor in ≥300 enzymes.
| Neuroplasticity modulation Preserving the integrity of the neuronal cell membrane Enhancing memory and learning mechanisms Enhancing cognitive functions Increasing BDNF levels Participating in glutamatergic transmission Pro-inflammatory cytokine reduction | |
| ~25 mg hydroaspartate or sulphate 2 | Lack of data | |
| May be beneficial for comorbid conditions involving weakened immunity, increased inflammation, or elevated oxidative stress, particularly in cases of dietary deficiency. Proven to be safe, but potential for causing nausea when taken on an empty stomach [13]. | ||
| Magnesium An indispensable mineral known as a cofactor in over 600 enzymes, it is engaged in CNS proper functioning and DNA reactions [83].
| Reducing neuronal hyperexcitability Increasing the availability of GABA Counteracting the inflammation Anxiety modulation Microbiota–gut–brain axis modulation | |
| 100–400 mg daily 7 | Lack of data | |
| At elevated dosages, there exists a potential for interference with mineral absorption and their subsequent reduction; furthermore, such doses can also precipitate gastrointestinal disturbances [13]. | ||
| Vitamin C Vitamin C, also known as ascorbic acid, is an essential water-soluble micronutrient involved in tissue repair and the enzymatic production of certain neurotransmitters.
| Participating in neuromodulation Participating in neurotransmitters transformation Counteracting the inflammation | |
| ~1 g/day 7 | Lack of data | |
| May be beneficial for comorbid conditions involving weakened immunity or elevated oxidative stress. Proven to be safe, but potential for causing gastrointestinal upset [13]. | ||
| Folate-based compounds A vital compound important to the synthesis of methionine by conveying single-carbon units [lam]. It leads to a reduction in homocysteine levels and contributes to the production of monoamines [83].
| Participating in neurotransmitters metabolism Engaging in the development of the nervous system Protection against neurotoxicity | |
| 15 mg of methylfolate 2 | Lack of data | |
| Additional benefits can be obtained by addressing factors such as obesity, preconception care, pregnancy, and inflammation [13]. | ||
| S-Adenosyl Methionine It is a crucial compound for metabolic pathways, as it provides a methyl group that impacts gene expression regulation. When this regulation occurs improperly, it can lead to disturbances in the function of the nervous system.
| Participating in the neurotransmitters synthesis Participating in maintaining membrane fluidity Neuroprotective properties Counteracting the inflammation | |
| 800 mg daily 8 1600–3200 mg 3 | There is a risk of triggering manic episodes. | |
| N-Acetyl Cysteine A compound arises from L-cysteine subjected to acetylation, recognized for its role as a precursor to glutathione regarded as antioxidant. It is often used as a medication to treat acetaminophen overdose.
| Shielding against oxidative stress damage Pro-inflammatory cytokines reduction Neuroprotection Neurotransmitter modulation | |
| Lack of data | 1–3 g daily 6 | |
| Additional benefits can be attained under conditions of increased oxidative stress [13]. | ||
| Tryptophan An indispensable amino acid known as a serotonin precursor, which can be delivered from protein-rich food sources.
| Participating in serotonin synthesis Sleep rhythm regulation Enhancing cognitive functions Enhancing the immune system | |
| 50–200 mg of 5-HTP/1 g of tryptophan 7 | Lack of data | |
| A possibility of uncommon risk of serotonin syndrome [13]. | ||
| Creatine It is a guanidine compound synthesized by certain bodily organs involving the amino acids arginine and glycine in its production, and additionally requiring methionine as a donor of a methyl group.
| Enhancing nervous system operation Protection against brain atrophy | |
| 5 g daily 7 | Lack of data | |
| Renal disturbances should be carefully considered when contemplating administration [13]. | ||
| Inositol A polyol with myo-inositol as a predominant isomer, which can be obtained both from diet, especially fresh fruits and vegetables, and through endogenous synthesis. Inositol plays a role in various cellular processes, including cell growth and insulin signal transduction.
| Affecting sleep quality Participating in neurotransmission Marker of glial cells Improving insulin sensitivity | |
| 12 g daily 7 | Lack of data | |
| Risk of occurring gastrointestinal disturbances [13]. | ||
 —the names of individual nutraceuticals along with supplementary information;
—the names of individual nutraceuticals along with supplementary information;  —potential involvement in the mood disorders mangement;
—potential involvement in the mood disorders mangement;  —suggested formulations and dosages;
—suggested formulations and dosages;  —additional information.
—additional information.6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-disorders (accessed on 25 March 2023).
- Nestsiarovich, A.; Reps Jenna, M.; Matheny Michael, E.; DuVall, S.; Lynch, K.; Beaton, M.; Jiang, X.; Spotnitz, M.; Pfohl, S.R.; Shah, N.H.; et al. Predictors of diagnostic transition from major depressive disorder to bipolar disorder: A retrospective observational network study. Transl. Psychiatr. 2021, 11, 642. [Google Scholar] [CrossRef]
- Rakofsky, J.; Rapaport, M. Mood Disorders. Continuum. Behav. Neurol. Psychiatr. 2018, 24, 804–827. [Google Scholar] [CrossRef]
- Jones, B.D.M.; Daskalakis, Z.J.; Carvalho, A.F.; Strawbridge, R.; Young, A.H.; Mulsant, B.H.; Ishrat Husain, M. Inflammation as a treatment target in mood disorders: Review. BJPsych Open 2020, 6, e60. [Google Scholar] [CrossRef]
- Sarno, E.; Moeser, A.J.; Robison, A.J. Neuroimmunology of depression. Adv. Pharmacol. 2021, 91, 259–292. [Google Scholar] [PubMed]
- Wilkowska, A.; Cubała, W.J. The Downstaging Concept in Treatment-Resistant Depression: Spotlight on Ketamine. Int. J. Mol. Sci. 2022, 23, 14605. [Google Scholar] [CrossRef]
- Koning, E.; Vorstman, J.; McIntyre, R.S.; Brietzke, E. Characterizing eating behavioral phenotypes in mood disorders: A narrative review. Psychol. Med. 2022, 52, 2885–2898. [Google Scholar] [CrossRef] [PubMed]
- Ashton, M.M.; Kavanagh, B.E.; Marx, W.; Berk, M.; Sarris, J.; Ng, C.H.; Hopwood, M.; Williams, L.J.; Dean, O.M. A Systematic Review of Nutraceuticals for the Treatment of Bipolar Disorder. Can. J. Psychiatr. 2021, 66, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Alvarez-Mon, M.A.; Lahera, G.; Monserrat, J.; Llavero-Valero, M.; Gutiérrez-Rojas, L.; Molina, R.; Rodríguez-Jimenez, R.; et al. Biological Role of Nutrients, Food and Dietary Patterns in the Prevention and Clinical Management of Major Depressive Disorder. Nutrients 2022, 14, 3099. [Google Scholar] [CrossRef]
- Ceolin, G.; Breda, V.; Koning, E.; Meyyappan, A.C.; Gomes, F.A.; Moreira, J.D.; Gerchman, F.; Brietzke, E. A Possible Antidepressive Effect of Dietary Interventions: Emergent Findings and Research Challenges. Curr. Treat. Options Psychiatr. 2022, 9, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.; Behl, T.; Bungau, S.; Zengin, G.; Mehta, V.; Kumar, A.; Uddin, M.S.; Ashraf, G.M.; Abdel-Daim, M.M.; Arora, S.; et al. Nutraceuticals in neurological disorders. Int. J. Mol. Sci. 2020, 21, 4424. [Google Scholar] [CrossRef]
- AlAli, M.; Alqubaisy, M.; Aljaafari, M.N.; AlAli, A.O.; Baqais, L.; Molouki, A.; Abushelaibi, A.; Lai, K.; Lim, S.E. Nutraceuticals: Transformation of conventional foods into health promoters/disease preventers and safety considerations. Molecules 2021, 26, 2540. [Google Scholar] [CrossRef]
- Sarris, J.; Ravindran, A.; Yatham, L.N.; Marx, W.; Rucklidge, J.J.; McIntyre, R.S.; Akhondzadeh, S.; Benedetti, F.; Caneo, C.; Cramer, H.; et al. Clinician guidelines for the treatment of psychiatric disorders with nutraceuticals and phytoceuticals: The World Federation of Societies of Biological Psychiatry (WFSBP) and Canadian Network for Mood and Anxiety Treatments (CANMAT) Taskforce. World J. Biol. Psychiatr. 2022, 23, 424–455. [Google Scholar] [CrossRef] [PubMed]
- Perez-Caballero, L.; Torres-Sanchez, S.; Romero-López-Alberca, C.; González-Saiz, F.; Mico, J.A.; Berrocoso, E. Monoaminergic system and depression. Cell Tissue Res. 2019, 377, 107–113. [Google Scholar] [CrossRef]
- Oakes, P.; Loukas, M.; Oskouian, R.J.; Tubbs, R.S. The neuroanatomy of depression: A review. Clin. Anat. 2017, 30, 44–49. [Google Scholar] [CrossRef]
- Dean, J.; Keshavan, M. The neurobiology of depression: An integrated view. Asian, J. Psychiatr. 2017, 27, 101–111. [Google Scholar]
- Kennedy, S.H.; Lam, R.W.; McIntyre, R.S.; Tourjman, S.V.; Bhat, V.; Blier, P.; Hasnain, M.; Jollant, F.; Levitt, A.J.; MacQueen, G.M.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 ClinicalGuidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments. Can. J. Psychiatr. 2016, 61, 540–560. [Google Scholar] [CrossRef]
- Buzuk, G.A.; Owiecki, M. Molecular mechanisms of anti-depressive drugs activity. Adv. Cell Biol. 2014, 41, 147–160. [Google Scholar]
- Edinoff, A.N.; Haseeb, A.A.; Hanna, T.A.; Ochoa, C.O.; Patti, S.J.; Ghaffar, Y.A.; Kaye, A.D.; Viswanath, O.; Urits, I.; Boyer, A.G.; et al. Selective serotonin reuptake inhibitors and adverse effects: A narrative review. Neurol. Int. 2021, 13, 387–401. [Google Scholar] [CrossRef] [PubMed]
- Sigitova, E.; Fišar, Z.; Hroudová, J.; Cikánková, T.; Raboch, J. Biological hypotheses and biomarkers of bipolar disorder. Psychiatr. Clin. Neurosci. 2017, 71, 77–103. [Google Scholar] [CrossRef]
- Lin, C.; Huang, T. Brain-derived neurotrophic factor and mental disorders. Biomed. J. 2020, 43, 134–142. [Google Scholar] [CrossRef]
- Schmitt, K.; Holsboer-Trachsler, E.; Eckert, A. BDNF in sleep, insomnia, and sleep deprivation. Ann. Med. 2016, 48, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Polyakova, M.; Stuke, K.; Schuemberg, K.; Mueller, K.; Schoenknecht, P.; Schroeter, M.L. BDNF as a biomarker for successful treatment of mood disorders: A systematic & quantitative meta-analysis. J. Affect. Disord. 2015, 174, 432–440. [Google Scholar] [PubMed]
- Bauer, M.E.; Teixeira, A.L. Neuroinflammation in Mood Disorders: Role of Regulatory Immune Cells. Neuroimmunomodulation 2021, 28, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, N.A.L.; Del Ángel, D.S.; Brizuela, N.O.; Peraza, A.V.; Olguín, H.J.; Soto, M.P.; Guzmán, D.C. Inflammatory Process and Immune System in Major Depressive Disorder. Int. J. Neuropsychopharmacol. 2022, 25, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Gałecki, P.; Mossakowska-Wójcik, J.; Talarowska, M. The anti-inflammatory mechanism of antidepressants—SSRIs, SNRIs. Prog. Neuro-Psychopharmacol. Biol. Psychiatr. 2018, 80, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Osimo, E.F.; Baxter, L.J.; Lewis, G.; Jones, P.B.; Khandaker, G.M. Prevalence of low-grade inflammation in depression: A systematic review and meta-analysis of CRP levels. Psychol. Med. 2019, 49, 1958–1970. [Google Scholar] [CrossRef]
- Ting, E.Y.C.; Yang, A.C.; Tsai, S.J. Role of interleukin-6 in depressive disorder. Int. J. Mol. Sci. 2020, 21, 2194. [Google Scholar] [CrossRef]
- Cereda, G.; Enrico, P.; Ciappolino, V.; Delvecchio, G.; Brambilla, P. The role of vitamin D in bipolar disorder: Epidemiology and influence on disease activity. J. Affect. Disord. 2020, 278, 209–217. [Google Scholar] [CrossRef]
- Won, E.; Kim, Y. Stress, the Autonomic Nervous System, and the Immune-kynurenine Pathway in the Etiology of Depression. Curr. Neuropharmacol. 2016, 14, 665–673. [Google Scholar] [CrossRef]
- Hebbrecht, K.; Skorobogatov, K.; Giltay, E.J.; Coppens, V.; De Picker, L.; Morrens, M. Tryptophan Catabolites in Bipolar Disorder: A Meta-Analysis. Front. Immunol. 2021, 12, 667179. [Google Scholar] [CrossRef]
- Kadriu, B.; Farmer, C.A.; Yuan, P.; Park, L.T.; Deng, Z.-D.; Moaddel, R.; Henter, I.D.; Shovestul, B.; Ballard, E.D.; Kraus, C.; et al. The kynurenine pathway and bipolar disorder: Intersection of the monoaminergic and glutamatergic systems and immune response. Mol. Psychiatr. 2021, 26, 4085–4095. [Google Scholar] [CrossRef]
- Eriksen, J.K.D.; Coello, K.; Stanislaus, S.; Kjærstad, H.L.; Sletved, K.S.O.; McIntyre, R.S.; Faurholt-Jepsen, M.; Miskowiak, K.K.; Poulsen, H.E.; Kessing, L.V.; et al. Associations between childhood maltreatment and oxidative nucleoside damage in affective disorders. Eur. Psychiatr. 2022, 65, e46. [Google Scholar] [CrossRef]
- Madireddy, S.; Madireddy, S. Therapeutic Interventions to Mitigate Mitochondrial Dysfunction and Oxidative Stress–Induced Damage in Patients with Bipolar Disorder. Int. J. Mol. Sci. 2022, 23, 1844. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Zhang, Q.; Cai, D.; Yang, X.-H.; Qui, Y.; Ungvari, G.S.; Ng, C.H.; Berk, M.; Ning, Y.-P.; Xiang, Y.-T. N-acetylcysteine for major mental disorders: A systematic review and meta-analysis of randomized controlled trials. Acta Psychiatr. Scand. 2018, 137, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Toniolo, R.A.; de Brito Ferreira Fernandes, F.; Silva, M.; da Silva Dias, R.; Lafer, B. Cognitive effects of creatine monohydrate adjunctive therapy in patients with bipolar depression: Results from a randomized, double-blind, placebo-controlled trial. J. Affect. Disord. 2016, 224, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Belvederi Murri, M.; Prestia, D.; Mondelli, V.; Pariante, C.; Patti, S.; Olivieri, B.; Arzani, C.; Masotti, M.; Respino, M.; Antonioli, M.; et al. The HPA axis in bipolar disorder: Systematic review and meta-analysis. Psychoneuroendocrinology 2015, 63, 327–342. [Google Scholar] [CrossRef] [PubMed]
- Zajkowska, Z.; Gullett, N.; Walsh, A.; Zonca, V.; Pedersen, G.A.; Souza, L.; Kieling, C.; Fisher, H.L.; Kohort, B.A.; Mondelli, V. Cortisol and development of depression in adolescence and young adulthood—A systematic review and meta-analysis. Psychoneuroendocrinology 2021, 136, 105625. [Google Scholar] [CrossRef]
- Nikkheslat, N.; McLaughlin, A.; Hastings, C.; Zajkowska, Z.; Nettis, M.A.; Mariani, N.; Enache, D.; Lombardo, G.; Pointon, L.; Cowen, P.J.; et al. Childhood trauma, HPA axis activity and antidepressant response in patients with depression. Brain. Behav. Immun. 2019, 87, 229–237. [Google Scholar] [CrossRef]
- Mikulska, J.; Juszczyk, G.; Gawrońska-Grzywacz, M.; Herbet, M. Hpa axis in the pathomechanism of depression and schizophrenia: New therapeutic strategies based on its participation. Brain Sci. 2021, 11, 1298. [Google Scholar] [CrossRef]
- Murphy, F.; Nasa, A.; Cullinane, D.; Raajakesary, K.; Gazzaz, A.; Sooknarine, V.; Haines, M.; Roman, E.; Kelly, L.; O’Neill, A.; et al. Childhood Trauma, the HPA Axis and Psychiatric Illnesses: A Targeted Literature Synthesis. Front. Psychiatr. 2022, 13, 748372. [Google Scholar] [CrossRef]
- Ceruso, A.; Martínez-Cengotitabengoa, M.; Peters-Corbett, A.; Diaz-Gutierrez, M.J.; Martínez-Cengotitabengoa, M. Alterations of the HPA Axis Observed in Patients with Major Depressive Disorder and Their Relation to Early Life Stress: A Systematic Review. Neuropsychobiology 2020, 79, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Li, N.; Li, W.A.; Khan, H. Association between psychosocial stress and hypertension: A systematic review and meta-analysis. Neurol. Res. 2017, 39, 573–580. [Google Scholar] [CrossRef]
- Cai, J.; Wei, Z.; Chen, M.; He, L.; Wang, H.; Li, M.; Peng, Y. Socioeconomic status, individual behaviors and risk for mental disorders: A Mendelian randomization study. Eur. Psychiatr. 2022, 65, e28. [Google Scholar] [CrossRef]
- Baglioni, C.; Nanovska, S.; Regen, W.; Spiegelhalder, K.; Feige, B.; Nissen, C.; Reynolds, C.F.; Riemann, D. Sleep and mental disorders: A meta-analysis of polysomnographic research. Psychol. Bull. 2016, 142, 969–990. [Google Scholar] [CrossRef] [PubMed]
- Hepsomali, P.; Groeger, J.A. Diet, sleep, and mental health: Insights from the UK biobank study. Nutrients 2021, 13, 2573. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Tu, S.; Sheng, J.; Shao, A. Depression in sleep disturbance: A review on a bidirectional relationship, mechanisms and treatment. J. Cell. Mol. Med. 2019, 23, 2324–2332. [Google Scholar] [CrossRef]
- Mörkl, S.; Butler, M.I.; Holl, A.; Cryan, J.F.; Dinan, T.G. Probiotics and the Microbiota-Gut-Brain Axis: Focus on Psychiatry. Curr. Nutr. Rep. 2020, 9, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Wieërs, G.; Belkhir, L.; Enaud, R.; Leclercq, S.; Philippart de Foy, J.-M.; Dequenne, I.; de Timary, P.; Cani, P.D. How Probiotics Affect the Microbiota. Front. Cell. Infect. Microbiol. 2020, 9, 454. [Google Scholar] [CrossRef]
- Gondalia, S.; Parkinson, L.; Stough, C.; Scholey, A. Gut microbiota and bipolar disorder: A review of mechanisms and potential targets for adjunctive therapy. Psychopharmacology 2019, 236, 1433–1443. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, J.; Chen, Y. Regulation of neurotransmitters by the gut microbiota and effects on cognition in neurological disorders. Nutrients 2021, 13, 2099. [Google Scholar] [CrossRef]
- Generoso, J.S.; Giridharan, V.V.; Lee, J.; Macedo, D.; Barichello, T. The role of the microbiota-gut-brain axis in neuropsychiatric disorders. Braz. J. Psychiatr. 2021, 43, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, R.; Bouzari, B.; Hosseini-Fard, S.R.; Mazaheri, M.; Ahmadyousefi, Y.; Abdi, M.; Jalalifar, S.; Karimitabar, Z.; Teimoori, A.; Keyvani, H.; et al. Role of microbiota-derived short-chain fatty acids in nervous system disorders. Biomed. Pharmacother. 2021, 139, 111661. [Google Scholar] [CrossRef]
- McGuinness, A.J.; Davis, J.A.; Loughman, A.; Collier, F.; O’Hely, M.; Simpson, C.A.; Greem, J.; Marx, W.; Hair, C.; Jacka, F.N.; et al. A systematic review of gut microbiota composition in observational studies of major depressive disorder, bipolar disorder and schizophrenia. Mol. Psychiatr. 2022, 27, 1920–1935. [Google Scholar] [CrossRef]
- Perugi, G.; Quaranta, G.; Belletti, S.; Casalini, F.; Mosti, N.; Toni, C.; Dell’Osso, L. General medical conditions in 347 bipolar disorder patients: Clinical correlates of metabolic and autoimmune-allergic diseases. J. Affect. Disord. 2014, 170, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, M.; Sathiyaseelan, T.; Wani, R.J.; Fernandopulle, P. Obesity, food insecurity, and depression among females. Arch. Public. Heal. 2020, 78, 83. [Google Scholar] [CrossRef]
- Karakatsoulis, G.N.; Tsapakis, E.M.; Mitkani, C.; Fountoulakis, K.N. Subclinical thyroid dysfunction and major depressive disorder. Hormones 2021, 20, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Lauden, A.; Geishin, A.; Merzon, E.; Korobeinikov, A.; Green, I.; Golan-Cohen, A.; Vinker, S.; Manor, I.; Weizman, A.; Magen, E. Higher rates of allergies, autoimmune diseases and low-grade inflammation markers in treatment-resistant major depression. Brain Behav. Immun. Heal. 2021, 16, 100313. [Google Scholar] [CrossRef]
- Rochlani, Y.; Pothineni, N.V.; Kovelamusi, S.; Metha, J.L. Metabolic syndrome: Pathophysiology, management, and modulation by natural compounds. Ther. Adv. Vaccines 2018, 9, 259–261. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Mitchell, A.J.; De Hert, M.; Wampers, M.; Ward, P.B.; Rosenbaum, S.; Correll, C.U. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: A systematic review and meta-analysis. World Psychiatr. 2015, 14, 339–347. [Google Scholar] [CrossRef]
- Martins, L.B.; Tibães, J.R.B.; Berk, M.; Teixeira, A.L. Diabetes and mood disorders: Shared mechanisms and therapeutic opportunities. Int. J. Psychiatr. Clin. Pract. 2021, 26, 183–195. [Google Scholar] [CrossRef]
- Gardea-Resendez, M.; Winham, S.J.; Romo-Nava, F.; Cuellar-Barboza, A.; Clark, M.M.; Andreazza, A.C.; Cabello-Arreola, A.; Veldic, M.; Bondi, D.J.; Singh, B.; et al. Quantification of diet quality utilizing the rapid eating assessment for participants-shortened version in bipolar disorder: Implications for prospective depression and cardiometabolic studies. J. Affect. Disord. 2022, 310, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Joelson, A.M.; Geller, M.G.; Zylberberg, H.M.; Green, P.H.R.; Lebwohl, B. The effect of depressive symptoms on the association between gluten-free diet adherence and symptoms in celiac disease: Analysis of a patient powered research network. Nutrients 2018, 10, 538. [Google Scholar] [CrossRef] [PubMed]
- Joshua, J.; Golden, J.; Golden, S.H. Cortisol dysregulation: The bidirectional link between stress, depression, and type 2 diabetes mellitus. Ann. N. Y. Acad. Sci. 2017, 1391, 20–34. [Google Scholar]
- Cantelmi, T.; Lambiase, E.; Unfer, V.R.; Gambioli, R.; Unfer, V. Inositol treatment for psychological symptoms in Polycystic Ovary Syndrome women. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 2383–2389. [Google Scholar] [PubMed]
- Clappison, E.; Hadjivassiliou, M.; Zis, P. Psychiatric manifestations of coeliac disease, a systematic review and meta-analysis. Nutrients 2020, 12, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Navabi, S.; Gorrepati, V.S.; Yadav, S.; Chintanaboina, J.; Maher, S.; Demuth, P.; Stern, B.; Stuart, A.; Tinsley, A.; Clarke, K.; et al. Influences and impact of Anxiety and Depression in the setting of inflammatory bowel disease. Inflamm. Bowel Dis. 2018, 24, 2303–2308. [Google Scholar] [CrossRef]
- Sibelli, A.; Chalder, T.; Everitt, H.; Workman, P.; Windgassen, S.; Moss-Morris, R. A systematic review with meta-analysis of the role of anxiety and depression in irritable bowel syndrome onset. Psychol. Med. 2016, 46, 3065–3080. [Google Scholar] [CrossRef]
- Pinto-Sanchez, M.I.; Hall, G.B.; Ghajar, K.; Nardelli, A.; Bolino, C.; Lau, J.T.; Martin, F.-P.; Cominetti, O.; Welsh, C.; Rieder, A.; et al. Probiotic Bifidobacterium longum NCC3001 Reduces Depression Scores and Alters Brain Activity: A Pilot Study in Patients with Irritable Bowel Syndrome. Gastroenterology 2017, 153, 448–459. [Google Scholar] [CrossRef]
- Lin, J.A.; Jhe, G.; Vitagliano, J.A.; Milliren, C.E.; Spigel, R.; Woods, E.R.; Forman, S.F.; Richmond, T.K. The Association of Malnutrition, illness duration, and pre-morbid weight status with anxiety and depression symptoms in adolescents and young adults with restrictive eating disorders: A cross-sectional study. J. Eat. Disord. 2021, 9, 60. [Google Scholar] [CrossRef]
- McCuen-Wurst, C.; Ruggieri, M.; Allison, K.C. Disordered eating and obesity: Associations between binge eating-disorder, night-eating syndrome, and weight-related co- morbidities. Ann. N. Y. Acad. Sci. 2018, 1411, 96–105. [Google Scholar] [CrossRef]
- Semahegn, A.; Torpey, K.; Manu, A.; Assefa, N.; Tesfaye, G.; Ankomah, A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Gill, H.; Gill, B.; El-Halabi, S.; Chen-Li, D.; Lipsitz, O.; Rosenblat, J.D.; Van Rheenen, T.E.; Rodrigues, N.B.; Mansur, R.B.; Majeed, A.; et al. Antidepressant Medications and Weight Change: A Narrative Review. Obesity 2020, 28, 2064–2072. [Google Scholar] [CrossRef]
- Aronson, J.K. Defining ‘nutraceuticals’: Neither nutritious nor pharmaceutical. Br. J. Clin. Pharmacol. 2016, 83, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Ruchi, S.; Amanjot, K.; Sourav, T.; Keerti, B.; Sujit, B. Role of nutraceuticals in health care: A review. Int. J. Green. Pharm. 2017, 11, S385–S394. [Google Scholar]
- da Conceição Silva Chaves, R.; Aguiar, O.B.; Moreno, A.B.; Brunoni, A.R.; Molina, M.d.C.B.; Viana, M.C.; Bensoñor, I.; Griep, R.H.; da Fonseca, M.D.J.M. Consumption of Omega-3 and Maintenance and Incidence of Depressive Episodes: The ELSA-Brasil Study. Nutrients 2022, 14, 3227. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.B.; Brotchie, H.; Graham, R.K. Vitamin D and depression. J. Affect. Disord. 2017, 208, 56–61. [Google Scholar] [CrossRef]
- Steardo, L., Jr.; Luciano, M.; Sampogna, G.; Carbone, E.A.; Caivano, V.; Di Cerbo, A.; Giallonardo, V.; Palummo, C.; Vece, A.; Fiorillo, A.; et al. Clinical severity and calcium metabolism in patients with bipolar disorder. Brain Sci. 2020, 10, 417. [Google Scholar] [CrossRef] [PubMed]
- Thangaleela, S.; Sivamaruthi, B.S.; Kesika, P.; Chaiyasut, C. Role of Probiotics and Diet in the Management of Neurological Diseases and Mood States: A Review. Microorganisms 2022, 10, 2268. [Google Scholar] [CrossRef] [PubMed]
- Del Toro-Barbosa, M.; Hurtado-Romero, A.; Garcia-Amezquita, L.E.; García-Cayuela, T. Psychobiotics: Mechanisms of action, evaluation methods and effectiveness in applications with food products. Nutrients 2020, 12, 3896. [Google Scholar] [CrossRef]
- Styczeń, K.; Sowa-Kućma, M.; Siwek, M.; Dudek, D.; Reczyński, W.; Szewczyk, B.; Misztak, P.; Topór-Mądry, R.; Opoka, W.; Nowak, G. The serum zinc concentration as a potential biological marker in patients with major depressive disorder. Metab. Brain Dis. 2016, 32, 97–103. [Google Scholar] [CrossRef]
- Jafari, F.; Mohammadi, H.; Amani, R. The effect of zinc supplementation on brain derived neurotrophic factor: A meta-analysis. J. Trace Elem. Med. Biol. 2021, 66, 126753. [Google Scholar] [CrossRef] [PubMed]
- Hoepner, C.T.; Mcintyre, R.S.; Papakostas, G.I. Impact of Supplementation and Nutritional Interventions on Pathogenic Processes of Mood Disorders: A Review of the Evidence. Nutrients 2021, 13, 767. [Google Scholar] [CrossRef] [PubMed]
- Bansal, V.; Chatterjee, I. Association of Vitamins and Neurotransmitters: Understanding the Effect on Schizophrenia. Neurochem. J. 2022, 16, 39–45. [Google Scholar] [CrossRef]
- Jenkins, T.A.; Nguyen, J.C.D.; Polglaze, K.E.; Bertrand, P.P. Influence of tryptophan and serotonin on mood and cognition with a possible role of the gut-brain axis. Nutrients 2016, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.Z.; Li, H.; Liu, C.; Guan, J.-T.; Guo, X.-B.; Wen, C.-H.; Ou, S.-M.; Zhang, Y.-N.; Zhang, J.; Xu, C.-T.; et al. Main Effects of Diagnoses, Brain Regions, and their Interaction Effects for Cerebral Metabolites in Bipolar and Unipolar Depressive Disorders. Sci. Rep. 2016, 6, 37343. [Google Scholar] [CrossRef] [PubMed]
- Beal, M.F. Neuroprotective effects of creatine. Amino Acids 2011, 40, 1305–1313. [Google Scholar] [CrossRef]
- Mashayekh-Amiri, S.; Delavar, M.A.; Bakouei, F.; Faramarzi, M.; Esmaeilzadeh, S. The impact of myo-inositol supplementation on sleep quality in pregnant women: A randomized, double-blind, placebo-controlled study. J. Matern. Neonatal Med. 2022, 35, 3415–3423. [Google Scholar] [CrossRef] [PubMed]
- Botturi, A.; Ciappolino, V.; Delvecchio, G.; Boscutti, A.; Viscardi, B.; Brambilla, P. The role and the effect of magnesium in mental disorders: A systematic review. Nutrients 2020, 12, 1661. [Google Scholar] [CrossRef]
- Alonso, N.; Zelzer, S.; Eibinger, G.; Herrmann, M. Vitamin D Metabolites: Analytical Challenges and Clinical Relevance. Calcif. Tissue Int. 2023, 112, 158–177. [Google Scholar] [CrossRef]
- Lange, K.W. Omega-3 fatty acids and mental health. Glob. Health J. 2020, 4, 18–30. [Google Scholar] [CrossRef]
- Wong, S.; Chin, K.; Ima-Nirwana, S. Vitamin C: A Review on its Role in the Management of Metabolic Syndrome. Int. J. Med. Sci. 2020, 17, 1625–1638. [Google Scholar] [CrossRef] [PubMed]
- Guerini, M.; Condro, G.; Friuli, V.; Maggi, L.; Perugini, P. N-acetylcysteine (NAC) and Its Role in Clinical Practice Management of Cystic Fibrosis (CF): A Review. Pharmaceuticals 2022, 15, 217. [Google Scholar] [CrossRef] [PubMed]
- Croze, M.L.; Soulage, C.O. Potential role and therapeutic interests of myo-inositol in metabolic diseases. Biochimie 2013, 95, 1811–1827. [Google Scholar] [CrossRef]
- Weinberg, R.L.; Brook, R.D.; Rubenfire, M.; Eagle, K.A. Cardiovascular Impact of Nutritional Supplementation with Omega-3 Fatty Acids: JACC Focus Seminar. J. Am. Coll. Cardiol. 2021, 77, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Xing, C.; Zhang, J.; He, B. Comparative efficacy of oral insulin sensitizers metformin, thiazolidinediones, inositol, and berberine in improving endocrine and metabolic profiles in women with PCOS: A network meta-analysis. Reprod. Health 2021, 18, 171. [Google Scholar] [CrossRef]
- Kassaian, N.; Feizi, A.; Aminorroaya, A.; Amini, M. Probiotic and synbiotic supplementation could improve metabolic syndrome in prediabetic adults: A randomized controlled trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2991–2996. [Google Scholar] [CrossRef]
- Rodríguez-Morán, M.; Simental-Mendía, L.E.; Gamboa-Gómez, C.I.; Guerrero-Romero, F. Oral Magnesium Supplementation and Metabolic Syndrome: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Adv. Chronic Kidney Dis. 2018, 25, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Robin, B.G.; Kim, Y.; Kwon, J.; Kim, H.; Cho, J.H.; Kim, H.B.; Lee, J.-H. Role of probiotics in human gut microbiome-associated diseases. J. Microbiol. Biotechnol. 2019, 29, 1335–1340. [Google Scholar] [CrossRef]
- Wu, Y.; Huang, X.; Zhong, C.; Wu, T.; Sun, D.; Wang, R.; Zhan, Q.; Luo, H. Efficacy of Dietary Supplements on Sleep Quality and Daytime Function of Shift Workers: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 850417. [Google Scholar] [CrossRef]
- Matta, J.; Hoertel, N.; Airagnes, G.; Czernichow, S.; Kesse-Guyot, E.; Limosin, F.; Goldberg, M.; Zins, M.; Lemogne, C. Dietary restrictions and depressive symptoms: Longitudinal results from the constances cohort. Nutrients 2020, 2, 2700. [Google Scholar] [CrossRef]
- Ekinci, G.N.; Sanlier, N. The relationship between nutrition and depression in the life process: A mini-review. Exp. Gerontol. 2022, 172, 112072. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mechlińska, A.; Wiglusz, M.S.; Słupski, J.; Włodarczyk, A.; Cubała, W.J. Exploring the Relationship between Mood Disorders and Coexisting Health Conditions: The Focus on Nutraceuticals. Brain Sci. 2023, 13, 1262. https://doi.org/10.3390/brainsci13091262
Mechlińska A, Wiglusz MS, Słupski J, Włodarczyk A, Cubała WJ. Exploring the Relationship between Mood Disorders and Coexisting Health Conditions: The Focus on Nutraceuticals. Brain Sciences. 2023; 13(9):1262. https://doi.org/10.3390/brainsci13091262
Chicago/Turabian StyleMechlińska, Agnieszka, Mariusz S. Wiglusz, Jakub Słupski, Adam Włodarczyk, and Wiesław J. Cubała. 2023. "Exploring the Relationship between Mood Disorders and Coexisting Health Conditions: The Focus on Nutraceuticals" Brain Sciences 13, no. 9: 1262. https://doi.org/10.3390/brainsci13091262