

Breathing Practices for Stress and Anxiety Reduction: Conceptual Framework of Implementation Guidelines Based on a Systematic Review of the Published Literature

Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Search Strategy
2.3. Selection Criteria
2.3.1. Publication and Study Type
2.3.2. Intervention
2.3.3. Outcomes
2.3.4. Populations
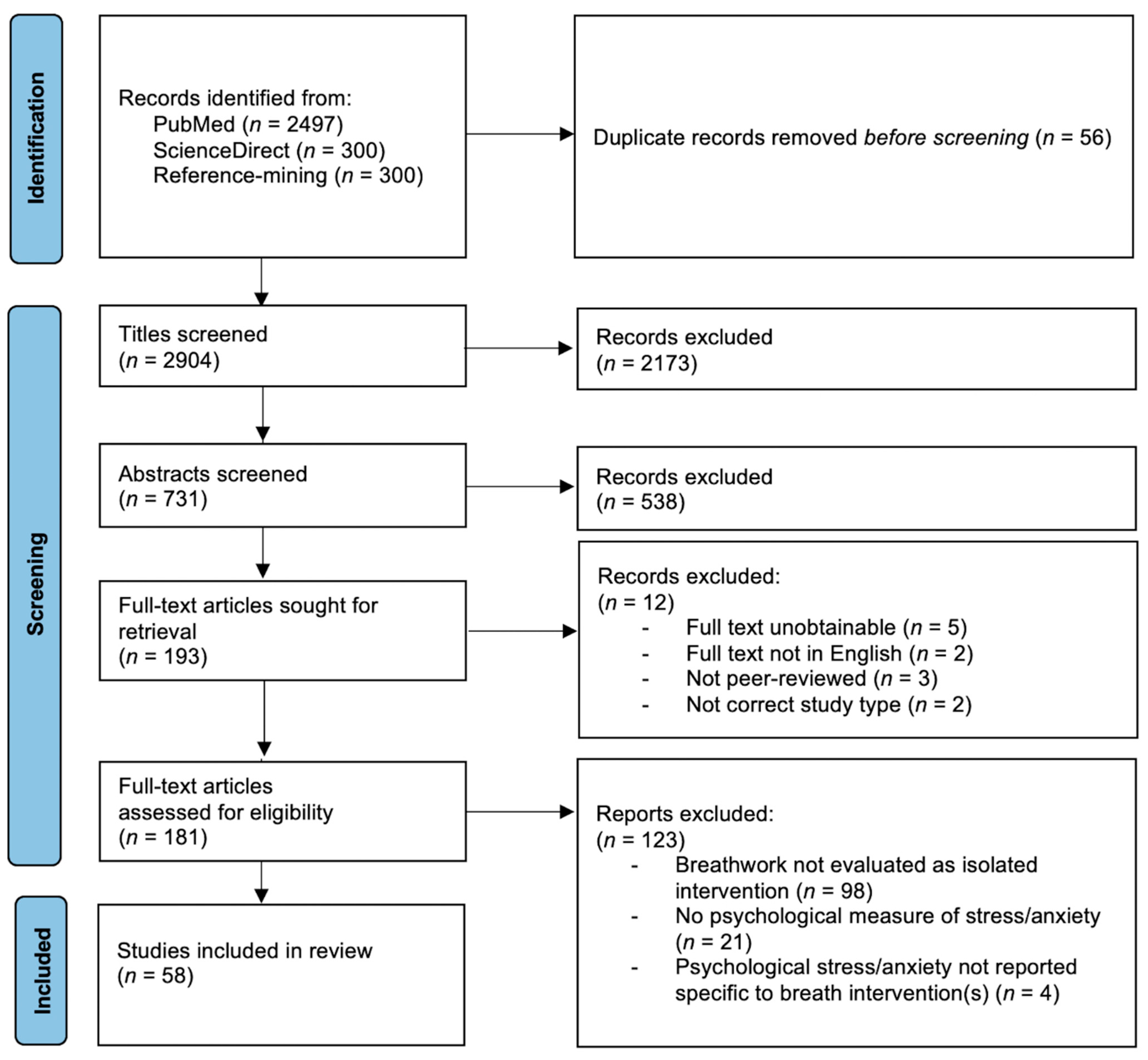
2.4. Article Screening and Data Extraction
- Title-screening;
- Abstract-screening of accepted titles;
- Full-text screening of accepted abstracts;
- Data extraction from accepted articles.
2.5. Assessment of Study Quality
2.6. Synthesis
3. Results
3.1. Study Selection and Characteristics
3.2. Study Characteristics and Outcomes by Population
3.2.1. Youth
3.2.2. Healthy Adults
3.2.3. High-Anxiety Populations
3.2.4. Clinical Populations, Acute
3.2.5. Clinical Populations, Chronic
3.2.6. Simulated Stress Settings
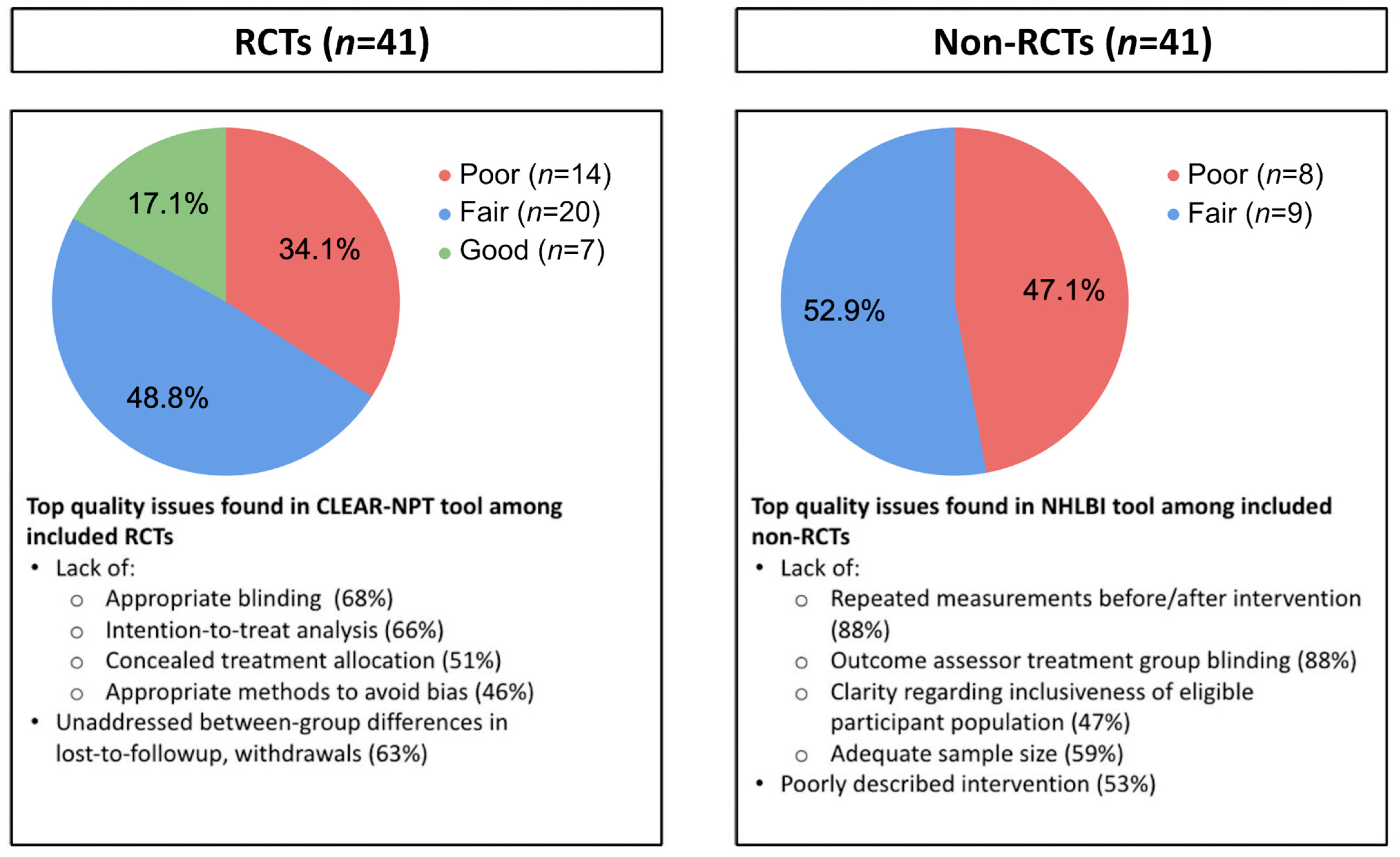
3.3. Study and Reporting Quality
3.4. Synthesis Results
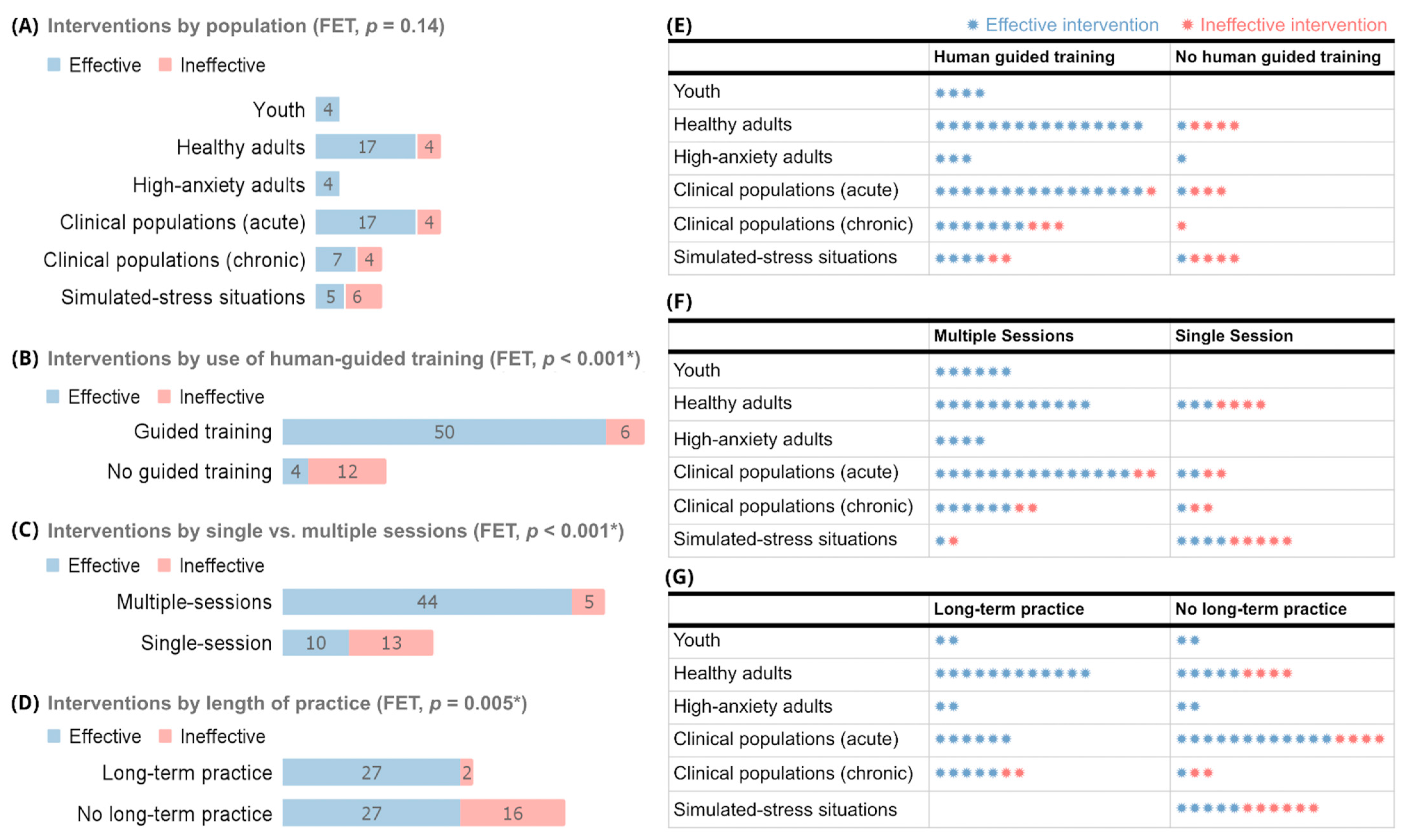
3.4.1. Study Design Parameters
3.4.2. Breathing Practice and Implementation Parameters
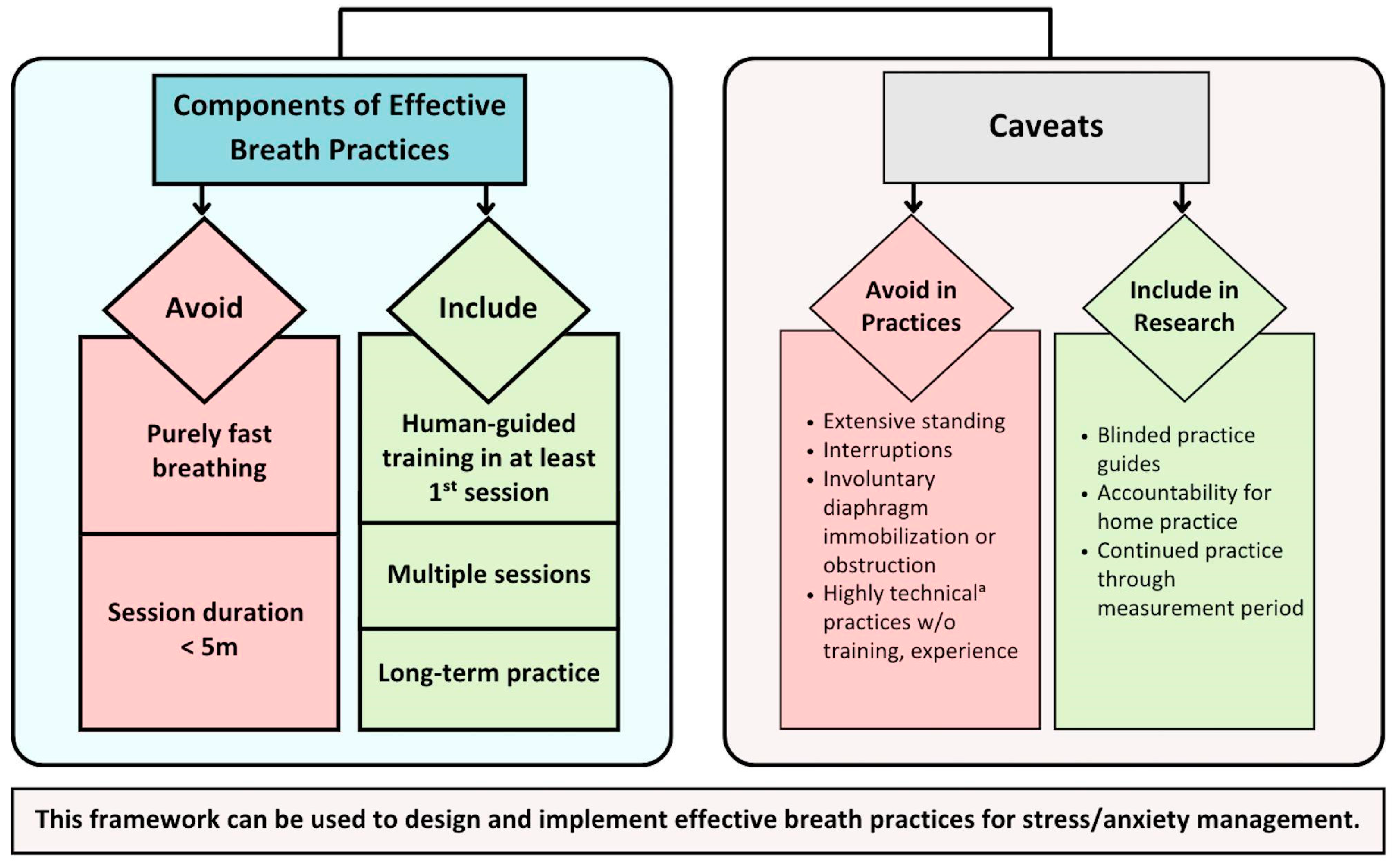
3.4.3. Framework Development
4. Discussion
4.1. Overview
4.2. Exclusionary Components
4.2.1. Breath Pace
4.2.2. Session Duration
4.3. Core Components
4.3.1. Human-Guided Training
4.3.2. Multiple Sessions
4.3.3. Long-Term Practice
4.4. Components Not Associated with Effectiveness
4.5. Framework Caveats
4.6. Limitations and Future Directions
4.7. Implications
4.8. Actionable Takeaways
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. PubMed and ScienceDirect Search Details
- PubMed MeSH terms [“OR” between all]
- Anxiety/analysis
- Anxiety/etiology
- Anxiety/pathology
- Anxiety/physiology
- Anxiety/physiopathology
- Anxiety/rehabilitation
- Anxiety/therapy
- Stress, Psychological/analysis
- Stress, Psychological/physiology
- Stress, Psychological/physiopathology
- Stress, Psychological/prevention, and control
- Stress, Psychological/psychology
- Stress, Psychological/rehabilitation
- Stress, Psychological/therapy
- panic
- panic/physiology
- panic/prevention and control
- panic/therapy
- panic disorder/etiology
- panic disorder/physiology
- panic disorder/physiopathology
- panic disorder/prevention and control
- panic disorder/therapy
- breathing exercises*
- respiration*
- Diaphragm/therapy
- PubMed Search String:
- PubMed filters:
- English Language
- PubMed study types:
- clinical trial
- clinical study
- controlled clinical trial
- pragmatic clinical trial
- randomized controlled trial
- ScienceDirect study types:
- Research studies
- ScienceDirect title keywords:
Appendix A.2. Data Points Abstracted from Articles Accepted for Review
- Study (i.e., Timestamp, RefID, Author, Title)
- Is the psychological (e.g., survey-based) stress/anxiety measure the primary outcome?
- Journal
- Year
- Study design (e.g., RCT, non-randomized prospective trial, etc.)
- Inclusion criteria
- Exclusion criteria
- Other population descriptions
- Setting
- Geographic location
- Sample size: Intervention (Intervention)—randomized
- Sample size: Intervention (Intervention)—at baseline
- Sample size: Intervention—# completed
- Sample size: control—randomized
- Sample size: control—at baseline
- Sample size: control—# completed
- Sample size: notes
- % Female: overall
- % Female: Intervention
- % Female: control
- Subgroups considered
- Age: Mean—Overall
- Age: Mean—Intervention
- Age: Mean—control
- Race/ethnicity (% each)
- Intervention type
- Intervention other: parameters, components. etc. (What situations is breath protocol being used?)
- Control description
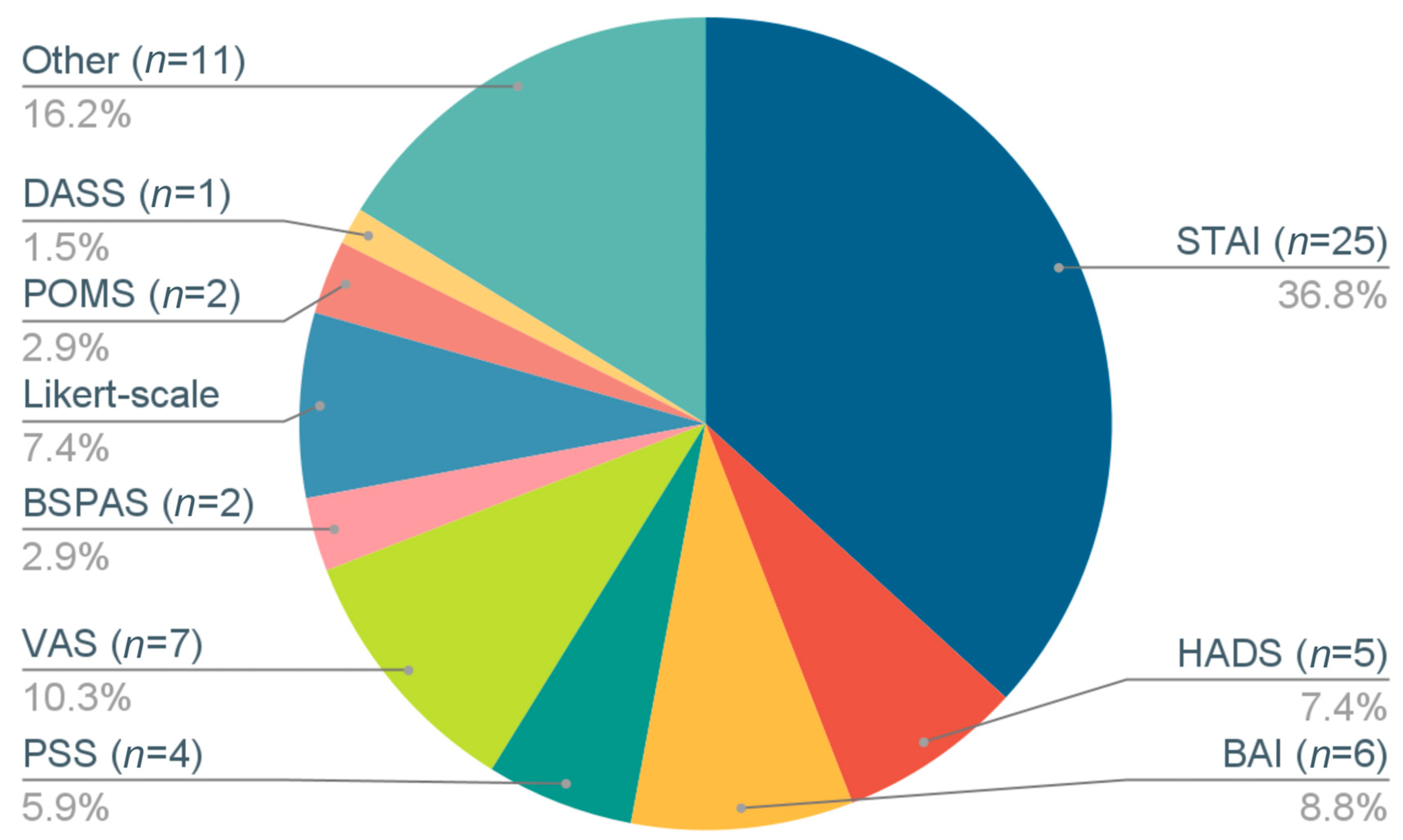
- Measurement tools: stress/anxiety-related
- Measurement tools: other
- Results: stress/anxiety-related
- Results: other metrics
- Subgroup results
- Limitations
- Implications
- Notes
- CLEAR Score of study quality
- Study population category
- Significant Benefit for Stress Outcome (yes/no)
- Intervention: breathing type (i.e., slow, fast, combined fast-slow, other)
- Slow breathing type(s) used
- Describe fast breathing practice (if used)
- Intervention breath pattern
- Breaths per minute (bpm) in breath practice
- Note regarding bpm
- Human-guided training (yes/no)
- Type of human-guided training
- Number of human-guided training sessions
- Number of minutes per human-guided training session
- Device-guided breath training/pacing (yes/no)
- Device type
- Number of device-guided training sessions
- Number of minutes per device-guided training session
- Intervention: group or individual
- Number of group sessions
- Number of minutes per group session
- Intervention homework (yes/no)
- Intervention homework description
- Total number of homework breath sessions
- Length of homework breath sessions (minutes)
- Intervention duration (days)
- Multiple (≥1) sessions (yes/no)
- Number of breath practice sessions, total known
- Length of general sessions (minutes)
- Length of group sessions, if done (minutes)
- Long-term practice (yes/no)
- Sessions continued through outcome measurement (yes/no)
- Control includes (e.g., no control/usual care/no intervention)
- At least one framework criterion met (yes/no)
- Framework: effectiveness of breathing practice
- Which criteria were included
- How many criteria were included
- Randomized controlled trial (yes/no)
- Primary outcome: stress/anxiety (yes/no)
- How many times were stress/anxiety outcomes measured
- Participants: # total randomized
Appendix A.3. Modified CLEAR-NPT Quality Assessment Tool [51,62]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criterion | Yes | No | Unclear | |
|---|---|---|---|---|
| 1 | Was the generation of allocation sequences (group assignment procedure) adequate? | |||
| 2 | Was the treatment allocation concealed? | |||
| 3 | Were details of the intervention administered to each group stated or made available? | |||
| 4 | Were care providers’ experience or skills in each arm (group) appropriate? | |||
| 5 | Was participant adherence or compliance assessed quantitatively? | |||
| 6 | Were participants adequately blinded?
| |||
| 6.1.1 | Were other treatments and care (i.e., co-interventions) the same in each randomized group? | |||
| 6.1.2 | Were withdrawals and lost-to-follow-up the same in each randomized group? | |||
| 7 | Were care providers for the participants adequately blinded?
| |||
| 7.1.1 | Were all other treatments and care (co-interventions) the same in each randomized group? | |||
| 7.1.2 | Were withdrawals and lost-to-follow-up the same in each randomized group? | |||
| 8 | Were outcome assessors adequately blinded to assess the primary outcomes? | |||
| 8.1 | If outcome assessors were not adequately blinded, were specific methods used to avoid ascertainment bias (systematic differences in outcome assessment)? | |||
| 9 | Was the follow-up schedule the same in each group? (parallel design) | |||
| 10 | Were the treatment and control group comparable at entry? (Any significant differences at baseline?) | |||
| 11 | Were the main outcomes analyzed according to the intention-to-treat principle? | |||
| Total | Total Scores (number of Yes) |
Appendix A.4. National Heart Lung Blood Institute-NHLBI/National Institutes of Health-NIH Quality Assessment Tool [63] for Pre-Post Studies with No Control Group
- Was the study question or objective clearly stated?
- Were eligibility/selection criteria for the study population prespecified and clearly described?
- Were the participants in the study representative of those who would be eligible for the test/service/intervention in the general or clinical population of interest?
- Were all eligible participants that met the prespecified entry criteria enrolled?
- Was the sample size sufficiently large to provide confidence in the findings?
- Was the test/service/intervention clearly described and delivered consistently across the study population?
- Were the outcome measures prespecified, clearly defined, valid, reliable, and assessed consistently across all study participants?
- Were the people assessing the outcomes blinded to the participants’ exposures/interventions?
- Was the loss to follow-up after baseline 20% or less? Were those lost to follow-up accounted for in the analysis?
- Did the statistical methods examine changes in outcome measures from before to after the intervention? Were statistical tests carried out that provided p-values for the pre-to-post changes?
- Were outcome measures of interest taken multiple times before the intervention and multiple times after the intervention (i.e., did they use an interrupted time-series design)?
- If the intervention was conducted at a group level (e.g., a whole hospital, a community, etc.), did the statistical analysis take into account the use of individual-level data to determine effects at the group level?
| Author, Year, Setting | Stress/Anxiety Metric | Outcomes ** | Quality Score, Tool † [62,63] |
|---|---|---|---|
| A. Youth | |||
| Youth: Stress/anxiety as primary outcome | |||
| * Sellakumar, 2015 [20] India, secondary school (grades 6–12) | STAI-state, trait | After Ix:
| 0.44 (CLEAR) Poor |
| * Khng, 2017 [66] Singapore, 4 elementary schools | STAI-C-state | When doing test after and w/Ix:
| 0.57 (CLEAR) Poor |
| * Bargale, 2021 [67] India, hospital pediatric dentistry dept. | Animated emoji scale |
| 0.86 (CLEAR) Good |
| Youth: Stress/anxiety as secondary outcome | |||
| * Hakked, 2017 [68] India, swim academy | SAS-2 | From before to after Ix:
| 0.69 (CLEAR) Fair |
| B. Healthy Adults | |||
| Healthy Adults: Stress/anxiety as primary outcome | |||
| * Gupta, 2010 [69] India, yoga training camp | Sinha Anxiety Scale |
| 0.25 (NHLBI) Poor |
| * Bhimani, 2011 [31] India, medical college | Authors’ 20-item stress questionnaire | From before to after Ix:
| 0.27 (NHLBI) Poor |
| * Sharma, 2013 [70] India, yoga research center and school | PSS | From baseline to 12 wks:
| 0.66 (CLEAR) Fair |
| * Sundram 2014 [71] Malaysia, automotive assembly plant | DASS-21 stress subscale | 9-mo DASS-21 was significant:
| 0.62 (NHLBI) Fair |
| * Schmalzl, 2018 [72] US, university town | PSS |
PSS decrease in Ix and C (p < 0.01)
| 0.75 (CLEAR) Fair |
| * Okado, 2020 [73] US, university setting | PSS, GAD-7 | From baseline to 2 wks:
| 0.31 (CLEAR) Poor |
| * Magnon, 2021 [74] France, setting unclear | SAI | SAI significantly lower post-Ix among entire group (p < 0.001), young adults (p = 0.003), and older adults (p = 0.019)
| 0.67 (NHLBI) Fair |
| * Balban, 2023 [75] US, remote setting | STAI |
| 0.53 (CLEAR) Poor |
| Healthy Adults: Stress/anxiety as secondary outcome | |||
| * Busch, 2012 [76] Germany, university setting | POMS tension- anxiety | Following Ix:
| 0.73 (NHBLI) Fair |
| Lin, 2014 [45] Taiwan, university setting | VAS-anxiety | During Ix:
Using retrospective ratings taken after all Ix’s:
| 0.58 (NHLBI) Poor |
| * Hunt, 2018 [21] US, large private university | 10-point Likert scale of subjective stress vs. relaxation |
| 0.56 (CLEAR) Poor |
| * Naik, 2018 [77] India, medical school | PSS | After 12 wks, Ix but not C had significant:
| 0.62 (CLEAR) Fair |
| * Conlon, 2022 [78] UK, University of Bath | IAMS, 7-point Likert scale of perceived stress |
| 100 (CLEAR) Good |
| * Schlatter, 2022 [79] France, university medical school | VAS-stress |
| 0.90 (CLEAR) Good |
| C. High-Anxiety Populations | |||
| High-Anxiety Populations: Stress/anxiety primary outcome | |||
| * Clark, 1990 [80] US, inpatient alcohol rehabilitation facility | STAI-state |
| 0.50 (CLEAR) Poor |
| * Chen, 2017 [81] Taiwan, medical center | BAI |
| 0.69 (CLEAR) Fair |
| * Serafim, 2018 [82] Brazil, hospital | HAM-A, BAI | After the Ix and at 10-wk follow-up:
| 0.50 (NHBLI) Poor |
| High-Anxiety Populations: Stress/anxiety as secondary outcome | |||
| * Clark, 1985 [83] UK, setting unclear | 100-pt Likert scale, MMFQ | Compared w/before Ix:
| 0.73 (NHBLI) Fair |
| D. Clinical Populations (Acute) | |||
| Clinical Populations (Acute): Stress/anxiety as primary outcome | |||
| Biggs 2003 [40] US, private dental practice | DAR-S |
| 0.38 (CLEAR) Poor |
| * Hayama, 2012 [84] Japan, hospital inpatient | Short-form POMS (Japanese version) |
| 0.69 (CLEAR) Fair |
| * Valenza, 2014 [85] Spain, hospital | HADS-anxiety |
| 0.63 (CLEAR) Fair |
| * Bidgoli, 2016 [86] Iran, hospital | SAI | Compared w/before Ix:
| 0.53 (CLEAR) Poor |
| Boaviagem, 2017 [41] Brazil, maternity hospital | STAI (unclear whether state or trait) |
| 0.75 (CLEAR) Fair |
| * Cicek, 2017 [87] Turkey, hospital delivery room | STAI-state |
| 0.69 (CLEAR) Fair |
| * Chandrababu, 2019 [88] India, hospital | STAI-state | From before surgery to 5th post-op day:
| 0.73 (NHLBI) Fair |
| Ratcliff, 2019 [47] US, university medical center | VAS-anxiety, STAI-state | Reduction in VAS anxiety during biopsy was:
| 0.64 (CLEAR) Fair |
| * Grinberg, 2020 [89] US, medical center | STAI-state | Compared to C, Ix group had significant:
| 0.50 (NHLBI) Poor |
| * Abo El Ata AB, 2021 [90] Egypt, hospital | Burn-specific pain anxiety scale | Significantly reduced burn-specific pain anxiety:
| 0.64 (NHLBI) Fair |
| * Hosseinzadeh-Karimkoshteh, 2021 [91] Iran, medical center | Burn patient anxiety inventory |
| 0.78 (CLEAR) Fair |
| * Zahn, 2021 [92] Switzerland, university hospital | STAI, APAIS, VAS-stress | Compared w/C, Ix intraoperative anxiety was:
| 0.64 (CLEAR) Fair |
| * Moghadam, 2022 [93] Iran, psychiatric hospital | BAI | Mean anxiety was significantly lower post-Ix:
| 0.56 (CLEAR) Poor |
| * Aktas, 2023 [39] Turkey, Ankara Hospital, | STAI | From pre-op to post-Ix:
| 0.37 (CLEAR) Poor |
| Clinical Populations (Acute): Stress/anxiety as secondary outcome | |||
| * Dhruva, 2012 [94] US, university medical center | HADS-anxiety |
| 0.63 (CLEAR) Fair |
| * Park, 2013 [95] South Korea, medical center | VAS-anxiety | Compared w/C and over the 3 days, Ix had significant:
| 0.67 (NHLBI) Fair |
| * Eldin, 2015 [96] Libya, hospital | STAI-state | Post-Ix, Ix but not C had significant:
| 0.55 (NHLBI) Poor |
| * Iyer, 2020 [97] India, medical center | VAS-anxiety, PASS | Compared w/pre-Ix, significant decreases found after 1 and 7 days in (p = 0.00 all):
| 0.73 (NHLBI) Fair |
| * Ursavas, 2020 [98] Turkey, hospital | HADS-anxiety | At 1,2,4,8,12, and 24 h post-op:
| 0.68 (CLEAR) Fair |
| * Lu, 2022 [99] China, hospital | HADS | Compared w/C, Ix had significant differences in:
| 0.73 (CLEAR) Fair |
| E. Clinical Populations (Chronic) | |||
| Clinical Populations (Chronic): Stress/anxiety as primary outcome | |||
| * Marshall, 2014 [100] US, setting unclear | BAI |
| 0.55 (NHLBI) Fair |
| Clinical Populations (Chronic): Stress/anxiety as secondary outcome | |||
| * Han, 1996 [22] Belgium, setting unclear | STAI-state and trait |
| 0.73 (NHLBI) Fair |
| * Thomas, 2009 [101] UK, primary care general practices | HADS-anxiety | At 6 mo following Ix, Ix had significantly greater improvements than C in AQLQ (p = 0.01), HADS anxiety (p = 0.02), and depression (p = 0.03), and hyperventilation symptoms (p = 0.005)
| 0.73 (CLEAR) Fair |
| Jefferson, 2010 [43] US, setting unclear | PSS, STAI |
| 0.25 (CLEAR) Poor |
| * Sureka, 2014 [102] India, prison hospital | PGWBS-anxiety | After 6 wks, Ix vs. C had significantly greater improvements in:
| 0.80 (CLEAR) Fair |
| * Sureka, 2015 [103] India, prison hospital | PGWBS-anxiety | After 6 wks, Ix vs. C significantly improved in:
| 0.73 (CLEAR) Fair |
| Thomas, 2017 [50] UK, general practices | HADS-anxiety | 12 mo after Ix:
| 0.80 (CLEAR) Fair |
| * Fiskin, 2018 [104] Turkey, medical center | DASS | After 30 days, Ix had:
| 0.50 (CLEAR) Poor |
| * Watson, 2022 [105] New Zealand hospital | 5-point Likert Scale | Compared w/Ix-2, Ix-1 significant initial increase in:
| 0.75 (CLEAR) Fair |
| F. Simulated Stress | |||
| Simulated Stress Populations: Stress/anxiety as primary outcome | |||
| Kamath, 2017 [44] India, medical school | VAMS-anxiety |
| 0.88 (CLEAR) Good |
| Simulated Stress Populations: Stress/anxiety as secondary outcome | |||
| Holmes, 1978 [42] US, university setting | Author-designed 18-item anxiety checklist | After threat or stimulation:
| 0.33 (NHLBI) Poor |
| * McCaul, 1979 [106] US, university setting | Author-designed 18-item anxiety checklist | Following threat/stimulation:
| 0.50 (CLEAR) Poor |
| Sakakibara, 1996 [48] Japan, university setting | STAI-state | Following threat anticipation:
| 0.50 (CLEAR) Poor |
| * Telles, 2019 [49] India, residential yoga center | STAI-state | From pre- to post- each Ix:
| 0.85 (CLEAR) Good |
| Meier, 2020 [46] Canada, setting unclear | VAS-stress | In response to Ix, no significant differences between groups for cortisol (p = 0.847), alpha amylase (p = 0.735), or stress (p = 0.986) In response to stressor:
| 0.81 (CLEAR) Good |
| * Sharma, 2022 [107] India, university setting | STAI-state | From pre- to post-Ix:
| 100 (CLEAR) Good |
References
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global Prevalence and Burden of Depressive and Anxiety Disorders in 204 Countries and Territories in 2020 Due to the COVID-19 Pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- DuPont, R.L.; Rice, D.P.; Miller, L.S.; Shiraki, S.S.; Rowland, C.R.; Harwood, H.J. Economic Costs of Anxiety Disorders. Anxiety 1996, 2, 167–172. [Google Scholar] [CrossRef]
- Kalia, M. Assessing the Economic Impact of Stress—The Modern Day Hidden Epidemic. Metabolism 2002, 51, 49–53. [Google Scholar] [CrossRef]
- Niles, A.N.; O’Donovan, A. Comparing Anxiety and Depression to Obesity and Smoking as Predictors of Major Medical Illnesses and Somatic Symptoms. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2019, 38, 172–181. [Google Scholar] [CrossRef]
- Kang, H.-J.; Bae, K.-Y.; Kim, S.-W.; Shin, H.-Y.; Shin, I.-S.; Yoon, J.-S.; Kim, J.-M. Impact of Anxiety and Depression on Physical Health Condition and Disability in an Elderly Korean Population. Psychiatry Investig. 2017, 14, 240–248. [Google Scholar] [CrossRef]
- Jonas, B.S.; Franks, P.; Ingram, D.D. Are Symptoms of Anxiety and Depression Risk Factors for Hypertension? Longitudinal Evidence from the National Health and Nutrition Examination Survey I Epidemiologic Follow-up Study. Arch. Fam. Med. 1997, 6, 43–49. [Google Scholar] [CrossRef]
- Eaker, E.D.; Sullivan, L.M.; Kelly-Hayes, M.; D’Agostino, R.B.; Benjamin, E.J. Tension and Anxiety and the Prediction of the 10-Year Incidence of Coronary Heart Disease, Atrial Fibrillation, and Total Mortality: The Framingham Offspring Study. Psychosom. Med. 2005, 67, 692–696. [Google Scholar] [CrossRef]
- Reiche, E.M.V.; Nunes, S.O.V.; Morimoto, H.K. Stress, Depression, the Immune System, and Cancer. Lancet Oncol. 2004, 5, 617–625. [Google Scholar] [CrossRef]
- Rozanski, A.; Blumenthal, J.A.; Kaplan, J. Impact of Psychological Factors on the Pathogenesis of Cardiovascular Disease and Implications for Therapy. Circulation 1999, 99, 2192–2217. [Google Scholar] [CrossRef]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. STRESS AND HEALTH: Psychological, Behavioral, and Biological Determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Panahi, Y.; Sahraei, H.; Johnston, T.P.; Sahebkar, A. The Impact of Stress on Body Function: A Review. EXCLI J. 2017, 16, 1057–1072. [Google Scholar] [CrossRef]
- Machado, A.; Herrera, A.J.; de Pablos, R.M.; Espinosa-Oliva, A.M.; Sarmiento, M.; Ayala, A.; Venero, J.L.; Santiago, M.; Villarán, R.F.; Delgado-Cortés, M.J.; et al. Chronic Stress as a Risk Factor for Alzheimer’s Disease. Rev. Neurosci. 2014, 25, 785–804. [Google Scholar] [CrossRef]
- Vyas, S.; Rodrigues, A.J.; Silva, J.M.; Tronche, F.; Almeida, O.F.X.; Sousa, N.; Sotiropoulos, I. Chronic Stress and Glucocorticoids: From Neuronal Plasticity to Neurodegeneration. Neural Plast. 2016, 2016, 6391686. [Google Scholar] [CrossRef]
- McEwen, B.S. Central Effects of Stress Hormones in Health and Disease: Understanding the Protective and Damaging Effects of Stress and Stress Mediators. Eur. J. Pharmacol. 2008, 583, 174–185. [Google Scholar] [CrossRef]
- Carpenter, J.K.; Andrews, L.A.; Witcraft, S.M.; Powers, M.B.; Smits, J.A.J.; Hofmann, S.G. Cognitive Behavioral Therapy for Anxiety and Related Disorders: A Meta-Analysis of Randomized Placebo-Controlled Trials. Depress. Anxiety 2018, 35, 502–514. [Google Scholar] [CrossRef]
- Bandelow, B.; Michaelis, S.; Wedekind, D. Treatment of Anxiety Disorders. Dialogues Clin. Neurosci. 2017, 19, 93–107. [Google Scholar] [CrossRef]
- Sengupta, P. Health Impacts of Yoga and Pranayama: A State-of-the-Art Review. Int. J. Prev. Med. 2012, 3, 444–458. [Google Scholar]
- Cramer, H.; Lauche, R.; Anheyer, D.; Pilkington, K.; de Manincor, M.; Dobos, G.; Ward, L. Yoga for Anxiety: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Depress. Anxiety 2018, 35, 830–843. [Google Scholar] [CrossRef]
- Sellakumar, G. Effect of Slow-Deep Breathing Exercise to Reduce Anxiety among Adolescent School Students in a Selected Higher Secondary School in Coimbatore, India. J. Psychol. Educ. Res. (JPER) 2015, 23, 54–72. [Google Scholar]
- Hunt, M.G.; Rushton, J.; Shenberger, E.; Murayama, S. Positive Effects of Diaphragmatic Breathing on Physiological Stress Reactivity in Varsity Athletes. J. Clin. Sport Psychol. 2018, 12, 27–38. [Google Scholar] [CrossRef]
- Han, J.N.; Stegen, K.; De Valck, C.; Clément, J.; Van de Woestijne, K.P. Influence of Breathing Therapy on Complaints, Anxiety and Breathing Pattern in Patients with Hyperventilation Syndrome and Anxiety Disorders. J. Psychosom. Res. 1996, 41, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Banushi, B.; Brendle, M.; Ragnhildstveit, A.; Murphy, T.; Moore, C.; Egberts, J.; Robison, R. Breathwork Interventions for Adults with Clinically Diagnosed Anxiety Disorders: A Scoping Review. Brain Sci. 2023, 13, 256. [Google Scholar] [CrossRef]
- Leyro, T.M.; Versella, M.V.; Yang, M.-J.; Brinkman, H.R.; Hoyt, D.L.; Lehrer, P. Respiratory Therapy for the Treatment of Anxiety: Meta-Analytic Review and Regression. Clin. Psychol. Rev. 2021, 84, 101980. [Google Scholar] [CrossRef] [PubMed]
- Malviya, S.; Meredith, P.; Zupan, B.; Kerley, L. Identifying Alternative Mental Health Interventions: A Systematic Review of Randomized Controlled Trials of Chanting and Breathwork. J. Spiritual. Ment. Health 2022, 24, 191–233. [Google Scholar] [CrossRef]
- Ashhad, S.; Kam, K.; Del Negro, C.A.; Feldman, J.L. Breathing Rhythm and Pattern and Their Influence on Emotion. Annu. Rev. Neurosci. 2022, 45, 223–247. [Google Scholar] [CrossRef]
- Tort, A.B.L.; Brankačk, J.; Draguhn, A. Respiration-Entrained Brain Rhythms Are Global but Often Overlooked. Trends Neurosci. 2018, 41, 186–197. [Google Scholar] [CrossRef]
- Masaoka, Y.; Homma, I. Anxiety and Respiratory Patterns: Their Relationship during Mental Stress and Physical Load. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 1997, 27, 153–159. [Google Scholar] [CrossRef]
- Wilhelm, F.H.; Gevirtz, R.; Roth, W.T. Respiratory Dysregulation in Anxiety, Functional Cardiac, and Pain Disorders. Assessment, Phenomenology, and Treatment. Behav. Modif. 2001, 25, 513–545. [Google Scholar] [CrossRef]
- Martinez, J.M.; Kent, J.M.; Coplan, J.D.; Browne, S.T.; Papp, L.A.; Sullivan, G.M.; Kleber, M.; Perepletchikova, F.; Fyer, A.J.; Klein, D.F.; et al. Respiratory Variability in Panic Disorder. Depress. Anxiety 2001, 14, 232–237. [Google Scholar] [CrossRef]
- Nardi, A.E.; Freire, R.C.; Zin, W.A. Panic Disorder and Control of Breathing. Respir. Physiol. Neurobiol. 2009, 167, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Bechbache, R.R.; Chow, H.H.; Duffin, J.; Orsini, E.C. The Effects of Hypercapnia, Hypoxia, Exercise and Anxiety on the Pattern of Breathing in Man. J. Physiol. 1979, 293, 285–300. [Google Scholar] [CrossRef] [PubMed]
- Grossman, P. Respiration, Stress, and Cardiovascular Function. Psychophysiology 1983, 20, 284–300. [Google Scholar] [CrossRef]
- Bhimani, N.T.; Kulkarni, N.B.; Kowale, A.; Salvi, S. Effect of Pranayama on Stress and Cardiovascular Autonomic Function. Indian J. Physiol. Pharmacol. 2011, 55, 370–377. [Google Scholar] [PubMed]
- Fincham, G.W.; Strauss, C.; Montero-Marin, J.; Cavanagh, K. Effect of Breathwork on Stress and Mental Health: A Meta-Analysis of Randomised-Controlled Trials. Sci. Rep. 2023, 13, 432. [Google Scholar] [CrossRef]
- Hopper, S.I.; Murray, S.L.; Ferrara, L.R.; Singleton, J.K. Effectiveness of Diaphragmatic Breathing for Reducing Physiological and Psychological Stress in Adults: A Quantitative Systematic Review. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 1855–1876. [Google Scholar] [CrossRef]
- Miri, S.; Hosseini, S.J.; Takasi, P.; Mollaei, A.; Firooz, M.; Falakdami, A.; Osuji, J.; Ghorbani Vajargah, P.; Karkhah, S. Effects of Breathing Exercise Techniques on the Pain and Anxiety of Burn Patients: A Systematic Review and Meta-Analysis. Int. Wound J. 2023, 20, 2360–2375. [Google Scholar] [CrossRef]
- Rung, O.; Stauber, L.; Loescher, L.J.; Pace, T.W. Alternate Nostril Breathing to Reduce Stress: An Option for Pregnant Women Survivors of Intimate Partner Violence? J. Holist. Nurs. Off. J. Am. Holist. Nurses Assoc. 2021, 39, 393–415. [Google Scholar] [CrossRef]
- Aktaş, G.K.; İlgin, V.E. The Effect of Deep Breathing Exercise and 4-7-8 Breathing Techniques Applied to Patients After Bariatric Surgery on Anxiety and Quality of Life. Obes. Surg. 2023, 33, 920–929. [Google Scholar] [CrossRef]
- Biggs, Q.M.; Kelly, K.S.; Toney, J.D. The Effects of Deep Diaphragmatic Breathing and Focused Attention on Dental Anxiety in a Private Practice Setting. J. Dent. Hyg. JDH 2003, 77, 105–113. [Google Scholar]
- Boaviagem, A.; Melo Junior, E.; Lubambo, L.; Sousa, P.; Aragão, C.; Albuquerque, S.; Lemos, A. The Effectiveness of Breathing Patterns to Control Maternal Anxiety during the First Period of Labor: A Randomized Controlled Clinical Trial. Complement. Ther. Clin. Pract. 2017, 26, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.S.; McCaul, K.D.; Solomon, S. Control of Respiration as a Means of Controlling Responses to Threat. J. Pers. Soc. Psychol. 1978, 36, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, L.L. Exploring Effects of Therapeutic Massage and Patient Teaching in the Practice of Diaphragmatic Breathing on Blood Pressure, Stress, and Anxiety in Hypertensive African-American Women: An Intervention Study. J. Natl. Black Nurses Assoc. JNBNA 2010, 21, 17–24. [Google Scholar]
- Kamath, A.; Urval, R.P.; Shenoy, A.K. Effect of Alternate Nostril Breathing Exercise on Experimentally Induced Anxiety in Healthy Volunteers Using the Simulated Public Speaking Model: A Randomized Controlled Pilot Study. BioMed Res. Int. 2017, 2017, 2450670. [Google Scholar] [CrossRef] [PubMed]
- Lin, I.M.; Tai, L.Y.; Fan, S.Y. Breathing at a Rate of 5.5 Breaths per Minute with Equal Inhalation-to-Exhalation Ratio Increases Heart Rate Variability. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2014, 91, 206–211. [Google Scholar] [CrossRef]
- Meier, M.; Wirz, L.; Dickinson, P.; Pruessner, J.C. Laughter Yoga Reduces the Cortisol Response to Acute Stress in Healthy Individuals. Stress 2021, 24, 44–52. [Google Scholar] [CrossRef]
- Ratcliff, C.G.; Prinsloo, S.; Chaoul, A.; Zepeda, S.G.; Cannon, R.; Spelman, A.; Yang, W.T.; Cohen, L. A Randomized Controlled Trial of Brief Mindfulness Meditation for Women Undergoing Stereotactic Breast Biopsy. J. Am. Coll. Radiol. JACR 2019, 16, 691–699. [Google Scholar] [CrossRef]
- Sakakibara, M.; Hayano, J. Effect of Slowed Respiration on Cardiac Parasympathetic Response to Threat. Psychosom. Med. 1996, 58, 32–37. [Google Scholar] [CrossRef]
- Telles, S.; Vishwakarma, B.; Gupta, R.K.; Balkrishna, A. Changes in Shape and Size Discrimination and State Anxiety After Alternate-Nostril Yoga Breathing and Breath Awareness in One Session Each. Med. Sci. Monit. Basic Res. 2019, 25, 121–127. [Google Scholar] [CrossRef]
- Thomas, M.; Bruton, A.; Little, P.; Holgate, S.; Lee, A.; Yardley, L.; George, S.; Raftery, J.; Versnel, J.; Price, D.; et al. A Randomised Controlled Study of the Effectiveness of Breathing Retraining Exercises Taught by a Physiotherapist Either by Instructional DVD or in Face-to-Face Sessions in the Management of Asthma in Adults. Health Technol. Assess. Winch. Engl. 2017, 21, 1–162. [Google Scholar] [CrossRef]
- Chen, K.W.; Berger, C.C.; Manheimer, E.; Forde, D.; Magidson, J.; Dachman, L.; Lejuez, C.W. Meditative Therapies for Reducing Anxiety: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Depress. Anxiety 2012, 29, 545–562. [Google Scholar] [CrossRef] [PubMed]
- Zaccaro, A.; Piarulli, A.; Laurino, M.; Garbella, E.; Menicucci, D.; Neri, B.; Gemignani, A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front. Hum. Neurosci. 2018, 12, 353. [Google Scholar] [CrossRef]
- Paulus, M.P. The Breathing Conundrum–Interoceptive Sensitivity and Anxiety. Depress. Anxiety 2013, 30, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Ruth, D.A. The Health Benefits of Nose Breathing. Nurs. Gen. Pract. 2015, 40–42. [Google Scholar]
- Jerath, R.; Beveridge, C.; Barnes, V.A. Self-Regulation of Breathing as an Adjunctive Treatment of Insomnia. Front. Psychiatry 2019, 9, 780. [Google Scholar] [CrossRef]
- Jerath, R.; Crawford, M.W.; Barnes, V.A.; Harden, K. Self-Regulation of Breathing as a Primary Treatment for Anxiety. Appl. Psychophysiol Biofeedback 2015, 40, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Yue, Z.-Q.; Gong, Z.-Q.; Zhang, H.; Duan, N.-Y.; Shi, Y.-T.; Wei, G.-X.; Li, Y.-F. The Effect of Diaphragmatic Breathing on Attention, Negative Affect and Stress in Healthy Adults. Front. Psychol. 2017, 8, 874. [Google Scholar] [CrossRef]
- Pal, G.K.; Velkumary, S. Effect of Short-Term Practice of Breathing Exercises on Autonomic Functions in Normal Human Volunteers. Indian J. Med. Res. 2004, 120, 115–121. [Google Scholar]
- Saoji, A.A.; Raghavendra, B.R.; Manjunath, N.K. Effects of Yogic Breath Regulation: A Narrative Review of Scientific Evidence. J. Ayurveda Integr. Med. 2019, 10, 50–58. [Google Scholar] [CrossRef]
- Sovik, R. The Science of Breathing—The Yogic View. Prog. Brain Res. 2000, 122, 491–505. [Google Scholar] [CrossRef]
- Victoria, H.K.; Caldwell, C. Breathwork in body psychotherapy: Clinical applications. Body Mov. Dance Psychother. 2013, 8, 216–228. [Google Scholar] [CrossRef]
- Boutron, I.; Moher, D.; Tugwell, P.; Giraudeau, B.; Poiraudeau, S.; Nizard, R.; Ravaud, P. A Checklist to Evaluate a Report of a Nonpharmacological Trial (CLEAR NPT) Was Developed Using Consensus. J. Clin. Epidemiol. 2005, 58, 1233–1240. [Google Scholar] [CrossRef]
- Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 17 August 2023).
- Mehta, C.R.; Patel, N.R. A Network Algorithm for Performing Fisher’s Exact Test in r × c Contingency Tables. J. Am. Stat. Assoc. 1983, 78, 427–434. [Google Scholar] [CrossRef]
- Fisher, R.A. Statistical Methods for Research Workers. In Breakthroughs in Statistics: Methodology and Distribution; Kotz, S., Johnson, N.L., Eds.; Springer Series in Statistics; Springer: New York, NY, USA, 1992; pp. 66–70. ISBN 978-1-4612-4380-9. [Google Scholar]
- Khng, K.H. A Better State-of-Mind: Deep Breathing Reduces State Anxiety and Enhances Test Performance through Regulating Test Cognitions in Children. Cogn. Emot. 2017, 31, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Bargale, S.; Khandelwal, J.R.; Dave, B.H.; Deshpande, A.N.; Shah, S.S.; Chari, D.N. Comparative Evaluation of Effect of Two Relaxation Breathing Exercises on Anxiety during Buccal Infiltration Anesthesia in Children Aged 6–12 Years: A Randomized Clinical Study. J. Indian Soc. Pedod. Prev. Dent. 2021, 39, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Hakked, C.S.; Balakrishnan, R.; Krishnamurthy, M.N. Yogic Breathing Practices Improve Lung Functions of Competitive Young Swimmers. J. Ayurveda Integr. Med. 2017, 8, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.K.; Kumar, M.; Kumari, R.; Deo, J.M. Anuloma-Viloma Pranayama and Anxiety and Depression among the Aged. J. Indian Acad. Appl. Psychol. 2010, 1, 159–164. [Google Scholar]
- Sharma, V.K.; Trakroo, M.; Subramaniam, V.; Rajajeyakumar, M.; Bhavanani, A.B.; Sahai, A. Effect of Fast and Slow Pranayama on Perceived Stress and Cardiovascular Parameters in Young Health-Care Students. Int. J. Yoga 2013, 6, 104–110. [Google Scholar] [CrossRef]
- Sundram, B.M.; Dahlui, M.; Chinna, K. “Taking My Breath Away by Keeping Stress at Bay”–An Employee Assistance Program in the Automotive Assembly Plant. Iran. J. Public Health 2014, 43, 263–272. [Google Scholar] [PubMed]
- Schmalzl, L.; Powers, C.; Zanesco, A.P.; Yetz, N.; Groessl, E.J.; Saron, C.D. The Effect of Movement-Focused and Breath-Focused Yoga Practice on Stress Parameters and Sustained Attention: A Randomized Controlled Pilot Study. Conscious. Cogn. 2018, 65, 109–125. [Google Scholar] [CrossRef]
- Okado, Y.; De Pace, D.; Ewing, E.; Rowley, C. Brief Relaxation Training for the Prevention of Stress-Related Difficulties: A Pilot Study. Int. Q. Community Health Educ. 2020, 40, 193–200. [Google Scholar] [CrossRef]
- Magnon, V.; Dutheil, F.; Vallet, G.T. Benefits from One Session of Deep and Slow Breathing on Vagal Tone and Anxiety in Young and Older Adults. Sci. Rep. 2021, 11, 19267. [Google Scholar] [CrossRef]
- Balban, M.Y.; Neri, E.; Kogon, M.M.; Weed, L.; Nouriani, B.; Jo, B.; Holl, G.; Zeitzer, J.M.; Spiegel, D.; Huberman, A.D. Brief Structured Respiration Practices Enhance Mood and Reduce Physiological Arousal. Cell Rep. Med. 2023, 4, 100895. [Google Scholar] [CrossRef] [PubMed]
- Busch, V.; Magerl, W.; Kern, U.; Haas, J.; Hajak, G.; Eichhammer, P. The Effect of Deep and Slow Breathing on Pain Perception, Autonomic Activity, and Mood Processing—An Experimental Study. Pain Med. Malden Mass. 2012, 13, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Naik, G.S.; Gaur, G.S.; Pal, G.K. Effect of Modified Slow Breathing Exercise on Perceived Stress and Basal Cardiovascular Parameters. Int. J. Yoga 2018, 11, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Conlon, A.; Arnold, R.; Preatoni, E.; Moore, L.J. Pulling the Trigger: The Effect of a 5-Minute Slow Diaphragmatic Breathing Intervention on Psychophysiological Stress Responses and Pressurized Pistol Shooting Performance. J. Sport Exerc. Psychol. 2022, 44, 206–219. [Google Scholar] [CrossRef] [PubMed]
- Schlatter, S.T.; Thérond, C.C.; Guillot, A.; Louisy, S.P.; Duclos, A.; Lehot, J.-J.; Rimmelé, T.; Debarnot, U.S.; Lilot, M.E. Effects of Relaxing Breathing Paired with Cardiac Biofeedback on Performance and Relaxation during Critical Simulated Situations: A Prospective Randomized Controlled Trial. BMC Med. Educ. 2022, 22, 422. [Google Scholar] [CrossRef]
- Clark, M.E.; Hirschman, R. Effects of Paced Respiration on Anxiety Reduction in a Clinical Population. Biofeedback Self-Regul. 1990, 15, 273–284. [Google Scholar] [CrossRef]
- Chen, Y.-F.; Huang, X.-Y.; Chien, C.-H.; Cheng, J.-F. The Effectiveness of Diaphragmatic Breathing Relaxation Training for Reducing Anxiety. Perspect. Psychiatr. Care 2017, 53, 329–336. [Google Scholar] [CrossRef]
- Serafim, S.D.; da Ponte, F.D.R.; Lima, F.M.; Martins, D.S.; Rosa, A.R.; Kunz, M. Effects of Deep Breathing in Patients with Bipolar Disorder. Perspect. Psychiatr. Care 2019, 55, 119–125. [Google Scholar] [CrossRef]
- Clark, D.M.; Salkovskis, P.M.; Chalkley, A.J. Respiratory Control as a Treatment for Panic Attacks. J. Behav. Ther. Exp. Psychiatry 1985, 16, 23–30. [Google Scholar] [CrossRef]
- Hayama, Y.; Inoue, T. The Effects of Deep Breathing on “tension-Anxiety” and Fatigue in Cancer Patients Undergoing Adjuvant Chemotherapy. Complement. Ther. Clin. Pract. 2012, 18, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Valenza, M.C.; Valenza-Peña, G.; Torres-Sánchez, I.; González-Jiménez, E.; Conde-Valero, A.; Valenza-Demet, G. Effectiveness of Controlled Breathing Techniques on Anxiety and Depression in Hospitalized Patients with COPD: A Randomized Clinical Trial. Respir. Care 2014, 59, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Mobini Bidgoli, M.; Taghadosi, M.; Gilasi, H.; Farokhian, A. The Effect of Sukha Pranayama on Anxiety in Patients Undergoing Coronary Angiography: A Single -Blind Randomized Controlled Trial. J. Cardiovasc. Thorac. Res. 2016, 8, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Cicek, S.; Basar, F. The Effects of Breathing Techniques Training on the Duration of Labor and Anxiety Levels of Pregnant Women. Complement. Ther. Clin. Pract. 2017, 29, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Chandrababu, R.; Kurup, S.B.; Ravishankar, N.; Ramesh, J. Effect of Pranayama on Anxiety and Pain among Patients Undergoing Cardiac Surgery: A Non-Randomized Controlled Trial. Clin. Epidemiol. Glob. Health 2019, 7, 606–610. [Google Scholar] [CrossRef]
- Grinberg, A.S.; Sellinger, J.J.; Sprenkle, P.C.; Bandin, A.J.; Nawaf, C.B.; Syed, J.S.; Leapman, M.S. Effect of Diaphragmatic Breathing on Procedural Anxiety During Transrectal Prostate Biopsy. Urology 2020, 137, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Abo El Ata, A.B.; Shaheen, E.S.; Abdelgilil Khalil, A.; Yousef Saleh, A.M.N. Effect of breathing exercise on reducing pain associated with dressing among hospitalized burned patients. Port Said Sci. J. Nurs. 2021, 8, 76–102. [Google Scholar] [CrossRef]
- Hosseinzadeh-Karimkoshteh, M.; Firouzkouhi, M.; Masinaeinezhad, N.; Abdollahimohammad, A. The Effect of Modified Relaxation Breathing Technique on Pain Anxiety in Patients with Second-Degree Burns: A Clinical Trial Study. J. Nurs. Explor. 2021, 1, 11–14. [Google Scholar] [CrossRef]
- Zahn, C.A.; Kuonen, F. Deep Breathing Reduces Intraoperative Anxiety and Pain Perception in Patients Undergoing Dermatologic Surgery. Dermatol. Surg. Off. Publ. Am. Soc. Dermatol. Surg. Al 2021, 47, 1137–1139. [Google Scholar] [CrossRef]
- Moghadam, Z.E.; Delmoradi, F.; Aemmi, S.Z.; Vaghee, S.; Vashani, H.B. Effectiveness of Aromatherapy with Inhaled Lavender Essential Oil and Breathing Exercises on ECT-Related Anxiety in Depressed Patients. Explore 2022, 18, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Dhruva, A.; Miaskowski, C.; Abrams, D.; Acree, M.; Cooper, B.; Goodman, S.; Hecht, F.M. Yoga Breathing for Cancer Chemotherapy-Associated Symptoms and Quality of Life: Results of a Pilot Randomized Controlled Trial. J. Altern. Complement. Med. 2012, 18, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Oh, H.; Kim, T. The Effects of Relaxation Breathing on Procedural Pain and Anxiety during Burn Care. Burns J. Int. Soc. Burn Inj. 2013, 39, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Eldin, S.M.A.; Mohamed, H.G.; Ragab, I.I. Effect of Relaxation Breathing Technique among Patients with Moderate Burn on Their Pain and Anxiety at Wound Care. World J. Nurs. Sci. 2015, 1, 110–123. [Google Scholar]
- Iyer, A.R.; Mitra, S.; Dabadghav, R. The Effect of Rhythmic Deep Breathing on Pain and Anxiety in Patients with Burns. Indian J. Burn. 2020, 28, 74. [Google Scholar] [CrossRef]
- Ursavas, F.; Catakli, M. The Effect of Diaphragmatic Breathing Exercise on Pain, Anxiety, and Depression in Patients Undergoing Total Knee Replacement: A Randomized Controlled Trial. Ann. Med. Res. 2020, 27, 2408. [Google Scholar] [CrossRef]
- Lu, H.-B.; Liu, X.; Wang, Y.-Q.; Cao, H.-P.; Ma, R.-C.; Yin, Y.-Y.; Song, C.-Y.; Yang, T.-T.; Xie, J. Active Cycle of Breathing Technique: A Respiratory Modality to Improve Perioperative Outcomes in Patients With Lung Cancer. Clin. J. Oncol. Nurs. 2022, 26, 176–182. [Google Scholar] [CrossRef]
- Marshall, R.S.; Basilakos, A.; Williams, T.; Love-Myers, K. Exploring the Benefits of Unilateral Nostril Breathing Practice Post-Stroke: Attention, Language, Spatial Abilities, Depression, and Anxiety. J. Altern. Complement. Med. 2014, 20, 185–194. [Google Scholar] [CrossRef]
- Thomas, M.; McKinley, R.K.; Mellor, S.; Watkin, G.; Holloway, E.; Scullion, J.; Shaw, D.E.; Wardlaw, A.; Price, D.; Pavord, I. Breathing Exercises for Asthma: A Randomised Controlled Trial. Thorax 2009, 64, 55–61. [Google Scholar] [CrossRef]
- Sureka, P.; Govil, S.; Dash, D.; Dash, C.; Kumar, M.; Singhal, V. Effect of Sudarshan Kriya on Male Prisoners with Non Psychotic Psychiatric Disorders: A Randomized Control Trial. Asian J. Psychiatry 2014, 12, 43–49. [Google Scholar] [CrossRef]
- Sureka, P.; Govil, S.; Dash, D.; Dash, C.; Kumar, C.; Singhal, V. Sudarshan Kriya for Male Patients with Psycho Active Substance Dependence: A Randomized Control Trial. Asian J. Psychiatry 2015, 16, 28–37. [Google Scholar]
- Fiskin, G.; Sahin, N.H. Effect of Diaphragmatic Breathing Exercise on Psychological Parameters in Gestational Diabetes: A Randomised Controlled Trial. Eur. J. Integr. Med. 2018, 23, 50–56. [Google Scholar] [CrossRef]
- Watson, G.M.; Sutherland, J.; Lacey, C.; Bridgman, P.G. A Randomised Cross-over Trial of QT Response to Hyperventilation-Induced Anxiety and Diaphragmatic Breathing in Patients with Stress Cardiomyopathy and in Control Patients. PLoS ONE 2022, 17, e0265607. [Google Scholar] [CrossRef] [PubMed]
- McCaul, K.D.; Solomon, S.; Holmes, D.S. Effects of Paced Respiration and Expectations on Physiological and Psychological Responses to Threat. J. Pers. Soc. Psychol. 1979, 37, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Kala, N.; Telles, S. Volitional Yoga Breathing Influences Attention and Anxiety: An Exploratory Randomized Crossover Study. Complement. Med. Res. 2022, 29, 120–126. [Google Scholar] [CrossRef] [PubMed]
- PORGES, S.W. The Polyvagal Theory: New Insights into Adaptive Reactions of the Autonomic Nervous System. Cleve. Clin. J. Med. 2009, 76, S86–S90. [Google Scholar] [CrossRef]
- Thayer, J.F.; Lane, R.D. A Model of Neurovisceral Integration in Emotion Regulation and Dysregulation. J. Affect. Disord. 2000, 61, 201–216. [Google Scholar] [CrossRef]
- Battaglia, M.; Ogliari, A.; D’Amato, F.; Kinkead, R. Early-Life Risk Factors for Panic and Separation Anxiety Disorder: Insights and Outstanding Questions Arising from Human and Animal Studies of CO2 Sensitivity. Neurosci. Biobehav. Rev. 2014, 46, 455–464. [Google Scholar] [CrossRef]
- Brown, R.P.; Gerbarg, P.L. Sudarshan Kriya Yogic Breathing in the Treatment of Stress, Anxiety, and Depression: Part I-Neurophysiologic Model. J. Altern. Complement. Med. 2005, 11, 189–201. [Google Scholar] [CrossRef]
- Strohmaier, S. The Relationship Between Doses of Mindfulness-Based Programs and Depression, Anxiety, Stress, and Mindfulness: A Dose-Response Meta-Regression of Randomized Controlled Trials. Mindfulness 2020, 11, 1315–1335. [Google Scholar] [CrossRef]
- Driscoll, D.; Dicicco, G. The Effects of Metronome Breathing on the Variability of Autonomic Activity Measurements. J. Manip. Physiol. Ther. 2000, 23, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Chang, Q.; Zhang, J.; Chai, W. Effects of Slow Breathing Rate on Heart Rate Variability and Arterial Baroreflex Sensitivity in Essential Hypertension. Medicine 2018, 97, e0639. [Google Scholar] [CrossRef] [PubMed]
- Kromenacker, B.W.; Sanova, A.A.; Marcus, F.I.; Allen, J.J.B.; Lane, R.D. Vagal Mediation of Low-Frequency Heart Rate Variability During Slow Yogic Breathing. Psychosom. Med. 2018, 80, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, P.; Sasaki, Y.; Saito, Y. Zazen and Cardiac Variability. Psychosom. Med. 1999, 61, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Fiorentini, A.; Ora, J.; Tubani, L. Autonomic System Modification in Zen Practitioners. Indian J. Med. Sci. 2013, 67, 161. [Google Scholar] [CrossRef]
- Abelson, J.L.; Khan, S.; Giardino, N. HPA Axis, Respiration and the Airways in Stress—A Review in Search of Intersections. Biol. Psychol. 2010, 84, 57–65. [Google Scholar] [CrossRef]
- Griffin, A. Adolescent Neurological Development and Implications for Health and Well-Being. Healthcare 2017, 5, 62. [Google Scholar] [CrossRef]
- Kim, H.-G.; Cheon, E.-J.; Bai, D.-S.; Lee, Y.H.; Koo, B.-H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef]
- Laborde, S.; Allen, M.S.; Borges, U.; Dosseville, F.; Hosang, T.J.; Iskra, M.; Mosley, E.; Salvotti, C.; Spolverato, L.; Zammit, N.; et al. Effects of Voluntary Slow Breathing on Heart Rate and Heart Rate Variability: A Systematic Review and a Meta-Analysis. Neurosci. Biobehav. Rev. 2022, 138, 104711. [Google Scholar] [CrossRef]






| Author, Year, Setting | Study Design, Population | Mean Age (SD), % Female, N | Intervention and Control, Time Frame |
|---|---|---|---|
| A. Youth | |||
| Youth: Stress/anxiety as primary outcome | |||
| * Sellakumar, 2015 [20] India, secondary school (grades 6–12) | RCT Adolescent school students | 14 y, 48% Ix: 50 C: 50 | Ix: 1-time guided group training followed by 45 days of 30 min individual: rhythmic breathing, pranayama, SK, slow breathing, deep breathing, prolonged exhales, brief breath-holds C: No intervention |
| * Khng, 2017 [66] Singapore, 4 elementary schools | RCT 5th-grade students | Ix: 10.7 y, 48%, 61 C: 10.7 y, 48%, 61 | For 10 min prior to and during six 1 min breaks in 2nd administration of math test: Ix: Deep abdominal breathing; C: Resting quietly |
| * Bargale, 2021 [67] India, hospital pediatric dentistry dept. | RCT Children needing dental treatment under anesthesia | 51% Ix: 8.5 y (1.9), 30 C: 8.4 y (1.9), 30 | Two sessions, before and after anesthetic procedure, of guided: Ix: Slow inhale, 2 s hold, exhale into pinwheel C: Relaxation breathing, feeling chest and belly move |
| Youth: Stress/anxiety as secondary outcome | |||
| * Hakked, 2017 [68] India, swim academy | RCT Competitive youth swimmers | 52% Ix: 15.2 y, 14 C: 15.1 y, 13 | For 4 wks, regular swim training alongside: Ix: 10 m, 5×/wk in group w/audio-guided yogic breathing practices: * Sectional (abdominal, thoracic, upper lobar) breathing * Yogic bellows breathing (forceful nasal breathing w/o strain and w/abdominal expansion/contraction) * ANB w/breath retention after inhaling C: No intervention |
| B. Healthy Adults | |||
| Healthy Adults: Stress/anxiety as primary outcome | |||
| * Gupta, 2010 [69] India, yoga training camp | Pre-post trial Married men | 60–70 y (range), 0%, 30 | 7-day group training + 3 mo individual practice of ANB |
| * Bhimani, 2011 [31] India, medical college | Pre-post trial Newly admitted medical students | 17–22 y (range), 54%, 59 | 8 wks of 1 h/day, 5 days/wk instructor-led group pranayama: Kapalabhati, External Kumbhaka (Bahya), Easy Comfortable Pranayama (Sukha Purvaka), Surya Bhedan, Ujjayi, Sitkari, Sitali |
| * Sharma, 2013 [70] India, yoga research center and school | RCT Healthy healthcare students | Ix-1: 18.4 y, 77%, 30 Ix-2: 19.2 y, 87%, 30 C: 18.9 y, 83%, 30 | For 12 wks, 30 m/day, 3×/week, of guided group: Ix-1: Fast pranayama—repeated cycles of 1 min each kapalabhati, Bhastrika, kukkriya, then 1 min rest Ix-2: Slow pranayama—repeated cycles of 2 min each of ANB, 6-3-6-3 breath, extended exhales w/sounds, then 1 min rest * Ix-1 and Ix-2 both end w/10 min shavasana C: No intervention |
| * Sundram, 2014 [71] Malaysia, automotive assembly plant | Pre/post-test nonequivalent-groups design Male automotive assembly line workers | 20+ y (range) Ix: 20+ y, 0%, 468 C: 20+ y, 0%, 293 | Ix: Five 10 min group sessions of guided deep breathing over 9 mo, +2×/day at-home practice encouraged C: Pamphlet on stress and its ill-effects, w/no stress reduction technique info |
| * Schmalzl, 2018 [72] US, university town | RCT Yoga-naive healthy adults | Ix: 25 y, 54%, 22 C: 24 y, 61%, 18 | 8-wk, 2×/wk instructor-led group classes + remaining days 15–20 min video-guided group practice: Ix: Yoga + breathing, equal-paced inhales/exhales, movements paced to breathing, 5 breaths in each pose C: Seated breath practice, visualizing breath moving up and down spine, directing breath to specific body parts, short breath holds after inhale/exhale, and ANB |
| * Okado, 2020 [73] US, university setting | RCT Undergraduate students | 19.81 y (2.42) Ix-1: 20.16 y (3.80), 45.5%, 20 Ix-2: 19.40 y (1.75), 72.1%, 31 Ix-3: 19.68 y (1.74), 68.2%, 30 C: 19.99 y (2.37), 79%, 64 | 1 in-person session followed by 2 wks of individual practice: Ix-1: Guided diaphragmatic breathing Ix-2: Relaxation techniques, asked to identify relaxation strategies in session Ix-3: Identical to Ix-2, +activity handout w/behavioral strategies to promote relaxation C: No intervention |
| * Magnon, 2021 [74] France, setting unclear | Single-arm study Healthy older and young adults | 41.2 y (23.6), 80.9%, 47 Older: 65.9 y (5.1) Young: 19.6 y (1.6) | Single 5 min session of slow breathing following on-screen moving drop of water; starting w/4 s inhale/exhale, gradually extending exhale to 6 s |
| * Balban, 2023 [75] US, remote setting | RCT Adults w/o severe psychiatric or medical conditions | 27.97 y, 68.5% Ix: 84 C: 24 | 28 days of daily 5 min home practice: Ix-1: Cyclic sighing: inhale slowly, inhale once more, slowly exhale all breath Ix-2: Box breathing: individualized pace w/equal length inhale, exhale, and breath holds Ix-3: Cyclic hyperventilation w/retention: 3 rounds of 30 deep inhales w/passive exhale, ending w/15 s hold C: Mindfulness meditation: sit/lie down, close eyes, breathe, focus on forehead between eyes |
| Healthy Adults: Stress/anxiety as secondary outcome | |||
| * Busch, 2012 [76] Germany, university setting | Pre-post trial of 2 Ix’s separated by 6 mo Healthy undergraduate students | 25 y, 87%, 15 | 6 weekly sessions of 20 min instructor-guided DSB, 7 bpm: Ix-1: DSB alone; Ix-2: DSB w/attentive concentration respiratory feedback task |
| Lin, 2014 [45] Taiwan, university setting | Within-subjects, 4-arm trial Healthy college students | 20.98 y (1.03), 78.7%, 47 | 5 min sitting then paced breathing using on-screen pacer for 2 min per pattern w/1 min rest between Ix-1: 6 bpm, 5-0-5-0; Ix-2: 6 bpm, 4-0-6-0; Ix-3: 5.5 bpm, 4.4-0-6.6-0; Ix-4: 5.5 bpm, 5.5-0-5.5-0 |
| * Hunt, 2018 [21] US, large private university | RCT Collegiate varsity soccer, swimming, track athletes | 20 y, 59%, 76 | 10 min metronome-guided paced breathing at 6 bpm followed by either: Ix: 5 min guided + 5 min unguided DB, aiming for 4 bpm C: 10 min guided PMR Afterwards, all did 5 min paced breathing (6 bpm) followed by cognitive stressor challenge |
| * Naik, 2018 [77] India, medical school | RCT Healthy adult male volunteers | Ix: 24.45 y, 0%, 49 C: 24.12 y, 0%, 50 | For 12 wks: Ix: 5×/wk of 30 min guided modified ANB (6-6-6-0) + instructions to practice at home other 2 days/wk C: No Ix |
| * Conlon, 2022 [78] UK, University of Bath | RCT Collegiate and National Team level athletes w/no formal shooting experience | 20.17 y (2.77) Ix-1: 60.9%, 23 Ix-2: 60.9%, 23 C: 57.1%, 21 | Between 2 shooting task exercises, 5 min guided training + 5 min pacer-guided practice w/nasal inhales, pursed-lip exhales of: Ix-1: 4 s inhale, 6 s exhale (6 bpm) diaphragmatic breathing Ix-2: 2.5 s inhale, 2.5 s exhale (12 bpm) paced breathing C: Watched 10 min respiratory anatomy educational video |
| * Schlatter, 2022 [79] France, university medical school | RCT 5th-yr anesthesiology and critical care residents participating in simulations for medical training | 29 y (1) Ix-1: 50%, 12 Ix-2: 27%, 11 C: 46%, 11 | For 5 min before engaging in 15 min simulated medical scenario w/performance evaluation: Ix-1: Relaxing breathing w/4 s inhale, 6 s exhale, following moving cursor on computer Ix-2: Same as Ix-1, but w/HRV biofeedback and instructions to increase HRV C: Read lab test results |
| C. High-Anxiety Populations | |||
| High-Anxiety Populations: Stress/anxiety primary outcome | |||
| * Clark, 1990 [80] US, inpatient alcohol rehabilitation facility | RCT Male, alcohol-dependent inpatients scoring high trait anxiety (STAI > 46.62) | 39.3 y Ix: 0%, 18 C: 0%, 18 | Two 10 min sessions, 2 days apart, w/audio pacing tones in 1st session and no sound in 2nd: Ix: Guided slow breathing (10 bpm) at audio tone pace session 1; at same yet self-guided pace session 2 C: Count audio tones session 1, relax session 2 |
| * Chen, 2017 [81] Taiwan, medical center | RCT High-anxiety adults from outpatient psych unit | Ix: 24 y (6), 60%, 15 C: 25 y (7), 73%, 15 | 12 individual training sessions over 8 wks + 2×/day home practice of: Ix: Guided diaphragmatic breathing C: “Routine respiration” |
| * Serafim, 2018 [82] Brazil, hospital | Pre-post open-label uncontrolled clinical trial Outpatients w/stable BD and complaints of anxiety | 42.8 y, 70%, 14 | Ix: 4 weekly 1:1 guided deep breathing trainings of 7, 10, 15, and 20 m, respectively, followed by at-home practice for 1 wk |
| High-Anxiety Populations: Stress/anxiety as secondary outcome | |||
| * Clark, 1985 [83] UK, setting unclear | AB case series Outpatient adults with frequent panic attacks and associated anxiety | 36 y, 72%, 18 | Ix: 2 sessions, w/1 wk between, of 2 min voluntary hyperventilation+ discussion of over-breathing and panic attacks, followed by guided slow breathing Before and after Ix, 11 were exposed to individually determined anxiety-provoking situation |
| D. Clinical Populations (Acute) | |||
| Clinical Populations (Acute): Stress/anxiety as primary outcome | |||
| Biggs, 2003 [40] US, private dental practice | RCT Patients seeking dental treatment | 38 y, 58%, 272 | Written instruction in waiting room: Ix-1: Unguided deep diaphragmatic breathing Ix-2: Focused attention on non-teeth body part C: No intervention |
| * Hayama, 2012 [84] Japan, hospital inpatient | RCT Women w/recent Dx of gynecological cancer undergoing 1st chemo Tx | Ix: 53.6 y (9.4), 100%, 11 C: 61.7 y (9.8), 100%, 12 | Ix: Before 1st chemo session and on days 2, 4, 6 post-chemo, 10 min of 4-step individual guided diaphragmatic breathing of 10 deep inhales and slow exhales per step, done lying down: breaths 0–10 and 30–40 w/arms raised; 11–20 abdominal and 21–30 thoracic breathing C: Usual chemo + nursing care |
| * Valenza, 2014 [85] Spain, hospital | RCT COPD exacerbation patients | Ix: 76 y, 0%, 23 C: 74.4 y, 0%, 23 | Ix: 10-day, 2×/day 30 m, guided breathing of inspiratory muscle relaxation, pursed lip breathing, prolonged and active expiration C: Standard care |
| * Bidgoli, 2016 [86] Iran, hospital | RCT Patients undergoing first coronary angiography and experiencing anxiety | Ix: 55.5 y, 55%, 40 C: 62.7 y, 45%, 40 | Ix: Single session before surgery of 5 min guided sukha pranayama—slow, rhythmic breathing w/equal length inhales-exhales C: Routine care |
| Boaviagem, 2017 [41] Brazil, maternity hospital | RCT Nulliparous women in active labor, 37–41 wks gestation | Ix: 21.2 y, 100%, 60 C: 20.6 y, 100%, 61 | Ix: Instruction to use slow deep breathing (5 s inhales, 5 s pursed lip exhales) during dilation, active, late labor phases, including post-exhale pause (1–2 s) for active and late active labor only C: Standard care |
| * Cicek, 2017 [87] Turkey, hospital delivery room | RCT Nulliparous women 38–42 wks pregnant w/o complications in early labor | Ix: 23.3 y, 100%, 35 C: 22.4 y, 100%, 35 | Ix: 30 min guided Lamaze breath stages for progressive labor w/real-time guidance during labor of normal nasal, slow deep chest, rapid shallow, rapid abdominal C: Routine hospital checks only |
| * Chandrababu, 2019 [88] India, hospital | Non-randomized 2-arm trial Patients undergoing 1st-time cardiac surgery | 58.7 y Ix: 25%, 24 C: 29%, 24 | Ix: 15 min guided ANB, taught 2 days prior to surgery and performed on days 3–5 post-surgery C: Usual pre- and post-operative care |
| Ratcliff, 2019 [47] US, university medical center | RCT Women scheduled for stereotactic breast biopsy | 55.4 y (11.27) Ix-1: 55.1 y, 100%, 30 Ix-2: 55.1 y, 100%, 30 C: 55.9 y, 100%, 16 | 10 min prior to and throughout biopsy, guided: Ix-1: Mindfulness meditation; Ix-2: Diaphragmatic breathing C: Listened to neutral-content audio |
| * Grinberg, 2020 [89] US, medical center | Non-randomized pre-post study Male veterans scheduled for prostate biopsy | 66.9 y (6.46) Ix: 66.7 y, 0%, 20 C: 65.05 y, 0%, 20 | Ix: 15 min guided diaphragmatic breathing immediately prior to biopsy C: Standard care |
| * Abo El Ata AB, 2021 [90] Egypt, hospital | Pre-post study Burn patients during dressing changes | 28.8 y (8.9), 37%, 7 | 2 wk daily guided relaxation breathing exercises before and during daily dressing change |
| * Hosseinzadeh-Karimkoshteh, 2021 [91] Iran, medical center | RCT Burn patients | Ix: 25.5 y, 33.3%, 15 C: 28.1 y, 40%, 15 | 4 days of: Ix: 30 min guided relaxation breathing before dressing change, 4-4-4-0 pursed-lip exhales C: Routine care |
| * Zahn, 2021 [92] Switzerland, university hospital | RCT Adults having dermatological surgery w/local anesthesia | Ix: 60.7 y (20.6), 40.8%, 86 C: 60.2 y (18.9), 48.8%, 84 | Before undergoing surgery: Ix: Deep breathing instruction, were told to perform before and during procedure C: No Instruction |
| * Moghadam, 2022 [93] Iran, psychiatric hospital | RCT Adults receiving ECT for depression | Ix-1: 35 y (14), 50%, 30 Ix-2: 38 y (9), 53.3%, 30 C: 36 y (10), 50%, 32 | Before ECT procedure: Ix-1: 10 min guided slow breathing, (5 s deep nasal inhale, 5 s mouth exhale) Ix-2: 3–5 min breathing lavender aromatherapy oil C: Routine care |
| * Aktas, 2023 [39] Turkey, Ankara Hospital | RCT Postoperative bariatric surgery patients | 34.7 y Ix-1: 76.7%, 23 Ix-2: 66.7%, 20 C: 53.3%, 16 | Each h during post-op h’s 1-6: Ix-1: 4-7-8 breathing technique, 10 breaths; Ix-2: Deep Breathing, 4 breaths C: Treatment as usual |
| Clinical Populations (Acute): Stress/anxiety as secondary outcome | |||
| * Dhruva, 2012 [94] US, university medical center | RCT w/single-arm crossover Cancer patients undergoing intravenous chemo | Ix: 52 y, 75%, 8 C: 56 y, 100%, 8 | During 2 consecutive chemo cycles: Ix: Usual care + 60 min class 1×/wk + 2×/day of 10–15 min individual home pranayama: * breath observation * ujjayi breathing: slow, deep abdominal rhythmic inhales/exhales, w/extended exhales and partially closed glottis * kapalabhati breathing: gentle inhales, brief pause, forceful exhale * ANB C: Usual care for 1st chemo cycle; usual care + Ix for 2nd cycle |
| * Park, 2013 [95] South Korea, medical center | Pre-post study comparison group Burn patients | 44.9 y Ix: 44.5 y, 43.3%, 30 C: 45.3 y, 60%, 30 | Over 3 days: Ix: Guided relaxation breathing 4-0-4-0 before and 4-0-2-0 during dressing changes C: Usual dressing change procedure |
| * Eldin, 2015 [96] Libya, hospital | RCT Burn patients | Ix: 18–50 y, 45%, 20 C: 18–50 y, 30%, 20 | Over 3 days: Ix: 15+ min guided relaxation breathing (in-nose, out-mouth) C: Standard care |
| * Iyer, 2020 [97] India, medical center | Pre-post Burn patients | 31.8 y (17.8), 35%, 20 | Over 7 days: Ix: 15 m/day guided deep breathing |
| * Ursavas, 2020 [98] Turkey, hospital | RCT Total knee replacement patients | Ix: 65 y, 79%, 19 C: 69 y, 79%, 19 | Ix: Guided diaphragmatic breathing + instruction to use at 1, 2, 4, 8, 12, and 24h post-op + when experiencing pain/anxiety C: Standard care |
| * Lu, 2022 [99] China, hospital | RCT Lung cancer patients undergoing thoracic surgery | 59.3 y (10.2) Ix: 55%, 34 C: 61%, 34 | Over 14 days: Ix: 2×/day of 15–20 min guided Active Cycle of Breathing Technique, each part repeated 3–5×: slow inhale, 3 s hold, 6 s pursed-lip exhale; deep active inhale, 3 s hold, passive exhale (all nasal; slow deep nasal inhale, 2–3 forceful “huff” mouth exhales) C: Usual care |
| E. Clinical Populations (Chronic) | |||
| Clinical Populations (Chronic): Stress/anxiety as primary outcome | |||
| * Marshall, 2014 [100] US, setting unclear | Pre-post repeated-measures trial Post-stroke individuals w/brain damage, w and w/o aphasia | 55.6 y, 18%, 11 | 4 wks of 1 h guided practice 1×/wk, followed by 6 wks of 5–40 min independent practice of right UNB: occlude left nostril while inhaling and exhaling through the other, work toward exhaling twice as long as inhale |
| Clinical Populations (Chronic): Stress/anxiety as secondary outcome | |||
| * Han, 1996 [22] Belgium, setting unclear | Pre-post single-arm trial Adults w/HVS | 37 y, 65%, 92 | 17 sessions over 2.5 mo of physiotherapist-guided breathing therapy and retraining: * 1st session: 3 min voluntary hyperventilation at 60 bpm followed by therapy to reattribute cause of daily life complaints to hyperventilation and explain breath retraining purpose * Remaining sessions: 45 min breath retraining w/abdominal breathing and slowed exhales |
| * Thomas, 2009 [101] UK, primary care general practices | RCT Adults w/asthma and impaired health status | Ix: 46 y (median), 58%, 66 C: 46 y (median), 64%, 63 | Ix: 3 physiotherapist-guided sessions w/2–4 wks between each: * One 1 h small group breathing education session * Two 30–45 min individual DB and nasal breathing training sessions * Participants instructed to practice breathing exercises ≥10 m/day C: Asthma nurse-delivered education |
| Jefferson, 2010 [43] US, setting unclear | RCT African-American females w/hypertension | Ix: 54 y, 100% C: 56 y, 100% | Ix: 20 min therapeutic chair massage C: Education on DB |
| * Sureka, 2014 [102] India, prison hospital | RCT Adult male prisoners w/psychiatric disorder | Ix: 36 y, 0%, 116 C: 36 y, 0%, 115 | For 6 wks, 30 m/day: Ix: Guided SKY breathing: 8 min Ujjayi, 5 min bellows (Bhastrika) followed by Om Chant, 10 min SK, and 5 min ANB C: Seated w/eyes closed and gentle attention on breath |
| * Sureka, 2015 [103] India, prison hospital | RCT Male inmates w/substance dependence | Ix: 39.3 y, 0%, 55 C: 38.8 y, 0%, 56 | For 6 wks, 23 m/day: Ix: Guided SKY breathing: 8 min Ujjayi, 5 min bellows (Bhastrika), and 10 min SK C: Sitting, eyes closed, attention to breath |
| Thomas, 2017 [50] UK, general practices | RCT Adults w/impaired asthma control | Ix-1: 56 y, 63%, 261 Ix-2: 55 y, 69%, 132 C: 57 y, 63%, 262 | Ix: Guided breath training delivered either via DVD (Ix-1) or 3 biweekly 30–40 min sessions w/physiotherapist (Ix-2), comprising: nose breathing, abdominal breathing, slow breathing, controlled breath holding, relaxation C: Usual care |
| * Fiskin, 2018 [104] Turkey, medical center | RCT Pregnant women w/GDM | Ix: 30.6 y, 100%, 30 C:31.3 y, 100%, 30 | 30 days of: Ix: Unguided diaphragmatic breathing, 5 min in the morning before leaving bed C: Standard care, invited to talk about their pregnancies 2×/mo |
| * Watson, 2022 [105] New Zealand hospital | RCT (cross-over) Postmenopausal women w/stress cardiomyopathy | 66.8 y (2.7) Ix: 100%, 12 C: 100%, 12 | One 3 min session each, separated by 5 days, of guided: Ix-1: Hyperventilation; Ix-2: Slow breathing w/3 s hold |
| F. Simulated Stress | |||
| Simulated Stress Populations: Stress/anxiety as primary outcome | |||
| Kamath, 2017 [44] India, medical school | RCT Healthy, yoga-naive undergrad medical students | Range 19–24 y Ix: 60%, 15 C: 80%, 15 | After brief instruction and practice for 15 min prior to simulated public speaking task: Ix: Guided ANB C: Sitting in quiet room |
| Simulated Stress Populations: Stress/anxiety as secondary outcome | |||
| Holmes, 1978 [42] US, university setting | 3-arm clinical trial (randomization/Tx allocation unclear) Undergraduate students | Age not reported, 54%, 111 | 90 s threat of electric shock (never administered) or visual stimulation, after 5 min of: Ix-1: Respiration tracing, breathing at pace where real-time respiration polygraph pen matched previously recorded resting respiration polygraph Ix-2: Attention tracing, using hand-held knob to follow previously recorded resting respiration polygraph recording C: Sitting quietly and relaxing |
| * McCaul, 1979 [106] US, university setting | RCT, 3 × 2 + 1 factorial-designed Male undergraduate students | Ix-1: 0%, 29 Ix-2: 0%, 28 Ix-3: 0%, 28 C: 0%, 14 (Ages not Reported) | 3 groups threatened w/impending electric shock, w/possibly 2 min (duration unclear) of unguided: Ix-1: Slow-pace regulated breathing (8 bpm); Ix-2: Normal-pace regulated breathing (16 bpm); Ix-3: Non-regulated breathing C: No breath pacing, no expectations, no threat, anticipation of visual stimulation Ix-1 and Ix-2 had 2 min practice before threat |
| Sakakibara, 1996 [48] Japan, university setting | RCT Healthy college students | 23 y Ix-1: 40%, 10 Ix-2: 30%, 10 C: 50%, 10 | Prior to 2 min threat (electric shock) anticipation w/15 bpm paced breathing, 5 min of unguided: Ix-1: Slow breathing (8 bpm) Ix-2: Fast breathing (30 bpm) C: Spontaneous breathing |
| * Telles, 2019 [49] India, residential yoga center | Randomized cross-over study Adult males w/yoga breathing experience | 28.4 y (8.2), 0%, 50 | In 3 separate, 18 min sessions across 3 days, w/timed shape and size discrimination task before/after each: Ix-1: ANB Ix-2: Breath awareness C: Quiet sitting |
| Meier, 2020 [46] Canada, setting unclear | RCT Young healthy men and women | 23.8 y (4.5), 51%, 35 Ix-1: 12 Ix-2: 11 C: 12 | 30 m, prior to simulated stress test (modified TSST-G): Ix-1: Guided relaxation breathing while standing Ix-2: Laughter yoga C: Reading magazines or books |
| * Sharma, 2022 [107] India, university setting | Randomized cross-over study University males w/yoga breathing experience | 24 y (4), 0%, 38 | 6 breath sessions in random order, w/timed SLCT before/after each, for 18 min w/1 min rest every 5 m, guided: Ix-1: ANB; Ix-2: Bellows breathing; Ix-3: Bumblebee breathing; Ix-4: High-frequency breathing at 50–65 bpm; Ix-5: Breath awareness; Ix-6: Quiet seated rest |
| Parameter | N | p-Value |
|---|---|---|
| Study design | ||
| Study design (RCT vs. other) | 72 | 0.77 |
| Control group (yes/no) | 72 | 0.19 |
| Primary vs. Secondary stress/anxiety outcome metric | 72 | 0.78 |
| # stress/anxiety outcome measurements (1, 2, 3+) | 72 | 0.43 |
| Breath practice and implementation | ||
| Population | 72 | 0.14 |
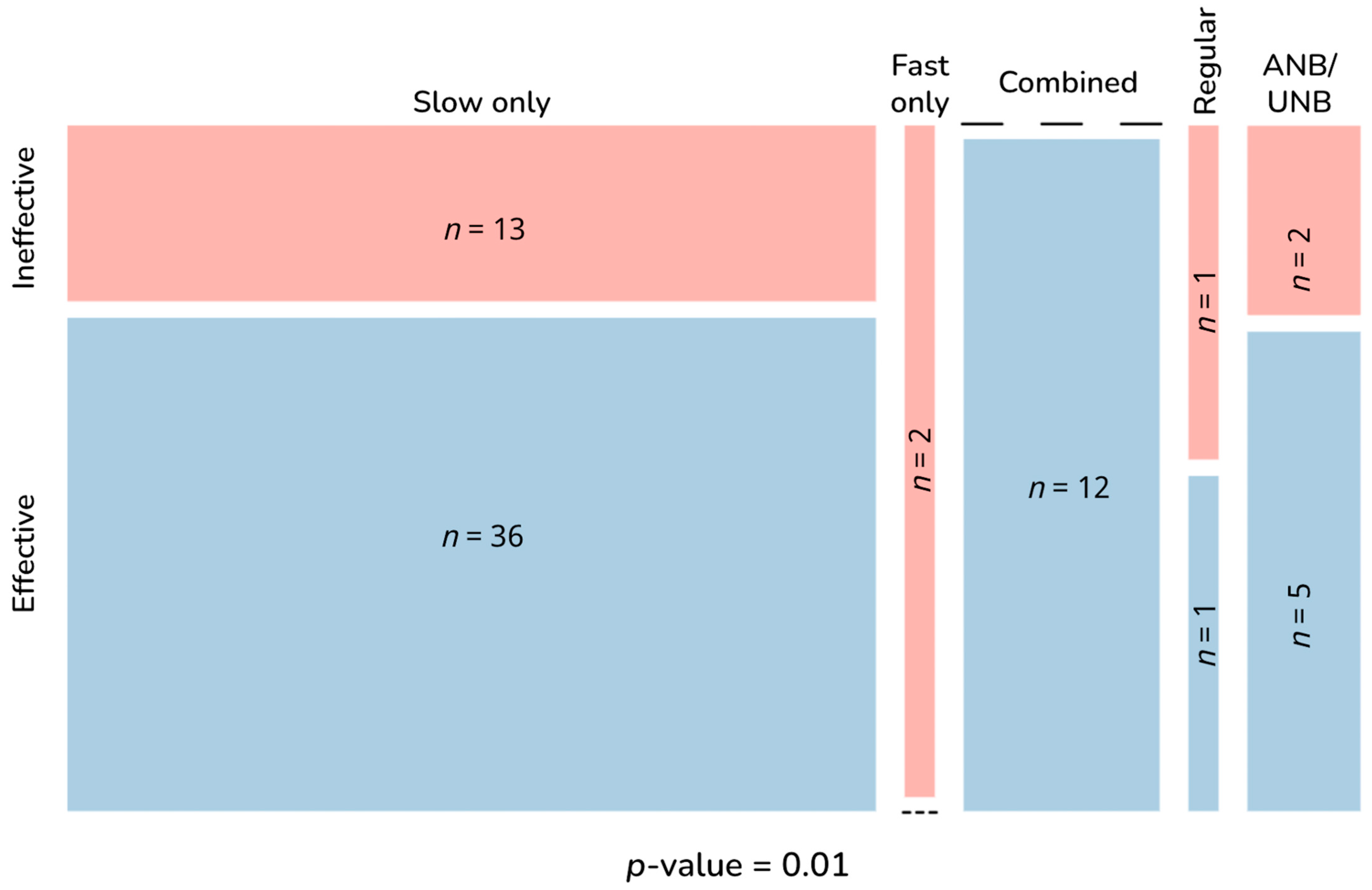
| Breath practice pace | 72 | 0.01 * |
| Breath pace other than fast-only | 70 | 0.10 |
| Human-guided training (yes/no) | 72 | <0.001 * |
| # human-guided sessions (0, 1, 2−3, 4+) | 71 | <0.001 * |
| Human-guided training included within device-guided interventions (yes/no) | 15 | 0.03 * |
| Single vs. Multiple sessions | 72 | <0.001 * |
| Long-term vs. No long-term practice | 72 | 0.005 * |
| Intervention duration (1, 2−5, 6−30, or 31+ days) | 71 | <0.001 * |
| Session duration: | ||
| <5, 5–10, 11–20, or >20 m | 61 | 0.03 * |
| <5 or ≥5 m | 61 | 0.005 * |
| Among sessions ≥5 m: 5–10, 11–20, or >20 m | 52 | 0.81 |
| Group vs. individual practice vs. both | 67 | 0.79 |
| At-home practice (yes/no) | 72 | 0.24 |
| Intervention | Potential Caveats | ||
|---|---|---|---|
| Author, Year (Population) | Description | Practice | Research |
| Effective practices incorporating zero core components | |||
| Schlatter, 2022 [79] (healthy adults) | 5 min of 6 bpm relaxing breathing prior to simulated medical scenario and test |
| |
| Ineffective practices that incorporated the following components: | |||
| Human-guided training | |||
| Meier, 2020 [46] (simulated stress) | 30 min guided standing relaxation breathing prior to simulated stress test |
| |
| Human-guided training, multiple sessions | |||
| Kamath, 2017 [44] (simulated stress) | 15 min guided ANB prior to simulated public speaking task |
| |
| Ratcliff, 2019 [47] (clinical, acute) | Guided diaphragmatic breathing for 10 min prior to and during breast biopsy |
|
|
| Human-guided training, multiple sessions, long-term practice | |||
| Thomas, 2017 [50] (clinical, chronic) | Guided diaphragmatic breathing with breath holds, guided via DVD |
| |
| Same as above, delivered by physiotherapist | |||
| For Practitioners, Program Developers, and Leaders Designing and Implementing Breath Practices | For Researchers Designing and Implementing Breath Practice Studies |
|---|---|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bentley, T.G.K.; D’Andrea-Penna, G.; Rakic, M.; Arce, N.; LaFaille, M.; Berman, R.; Cooley, K.; Sprimont, P. Breathing Practices for Stress and Anxiety Reduction: Conceptual Framework of Implementation Guidelines Based on a Systematic Review of the Published Literature. Brain Sci. 2023, 13, 1612. https://doi.org/10.3390/brainsci13121612
Bentley TGK, D’Andrea-Penna G, Rakic M, Arce N, LaFaille M, Berman R, Cooley K, Sprimont P. Breathing Practices for Stress and Anxiety Reduction: Conceptual Framework of Implementation Guidelines Based on a Systematic Review of the Published Literature. Brain Sciences. 2023; 13(12):1612. https://doi.org/10.3390/brainsci13121612
Chicago/Turabian StyleBentley, Tanya G. K., Gina D’Andrea-Penna, Marina Rakic, Nick Arce, Michelle LaFaille, Rachel Berman, Katie Cooley, and Preston Sprimont. 2023. "Breathing Practices for Stress and Anxiety Reduction: Conceptual Framework of Implementation Guidelines Based on a Systematic Review of the Published Literature" Brain Sciences 13, no. 12: 1612. https://doi.org/10.3390/brainsci13121612