
Postural Instability and Risk of Falls in Patients with Parkinson’s Disease Treated with Deep Brain Stimulation: A Stabilometric Platform Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessment
2.3. Stabilometric Platform
2.4. PI and RF Assessment
2.5. Experimental Conditions
2.6. Statistical Analysis
3. Results
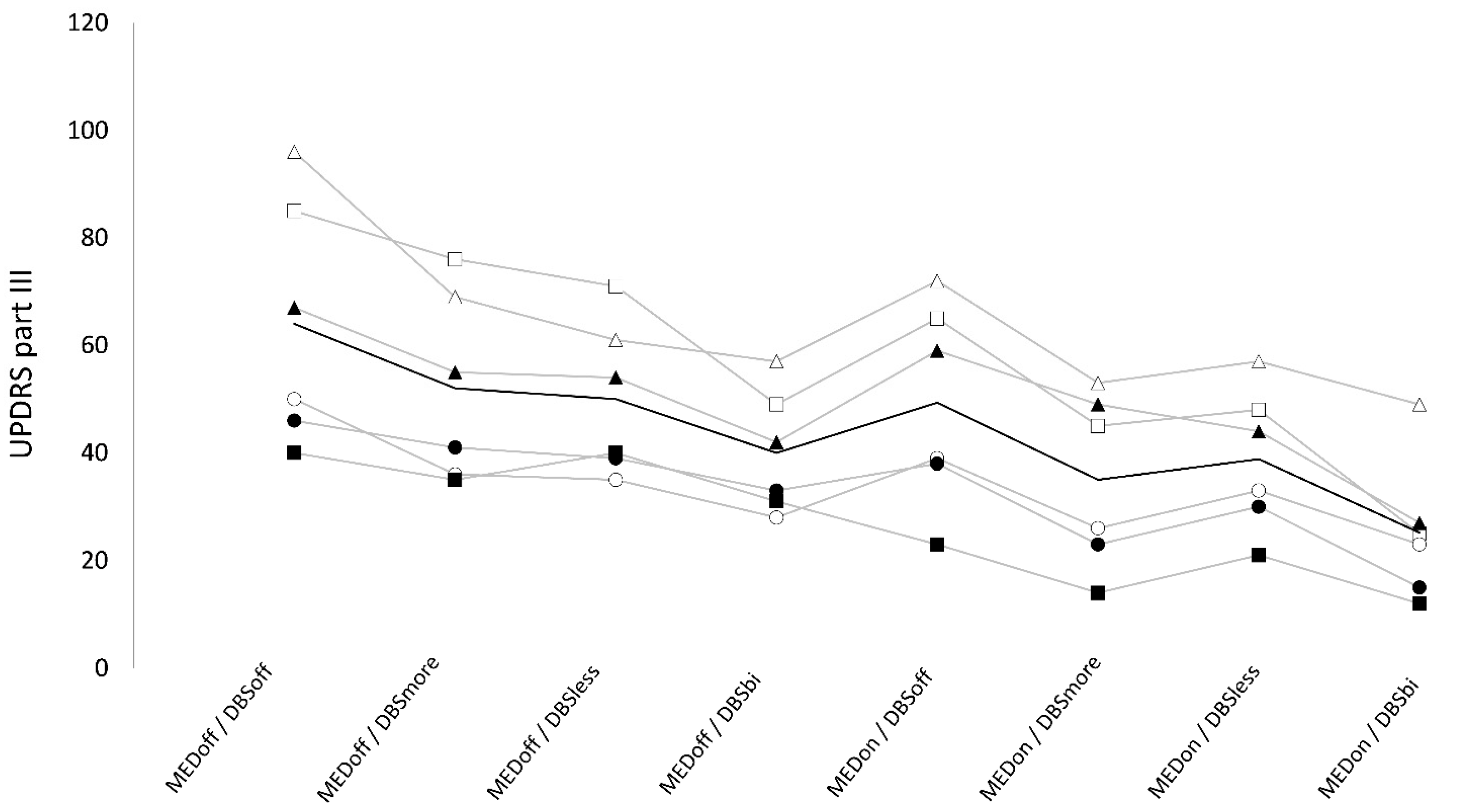
3.1. UPDRS Part III
3.1.1. Bilateral DBS
3.1.2. Unilateral DBS
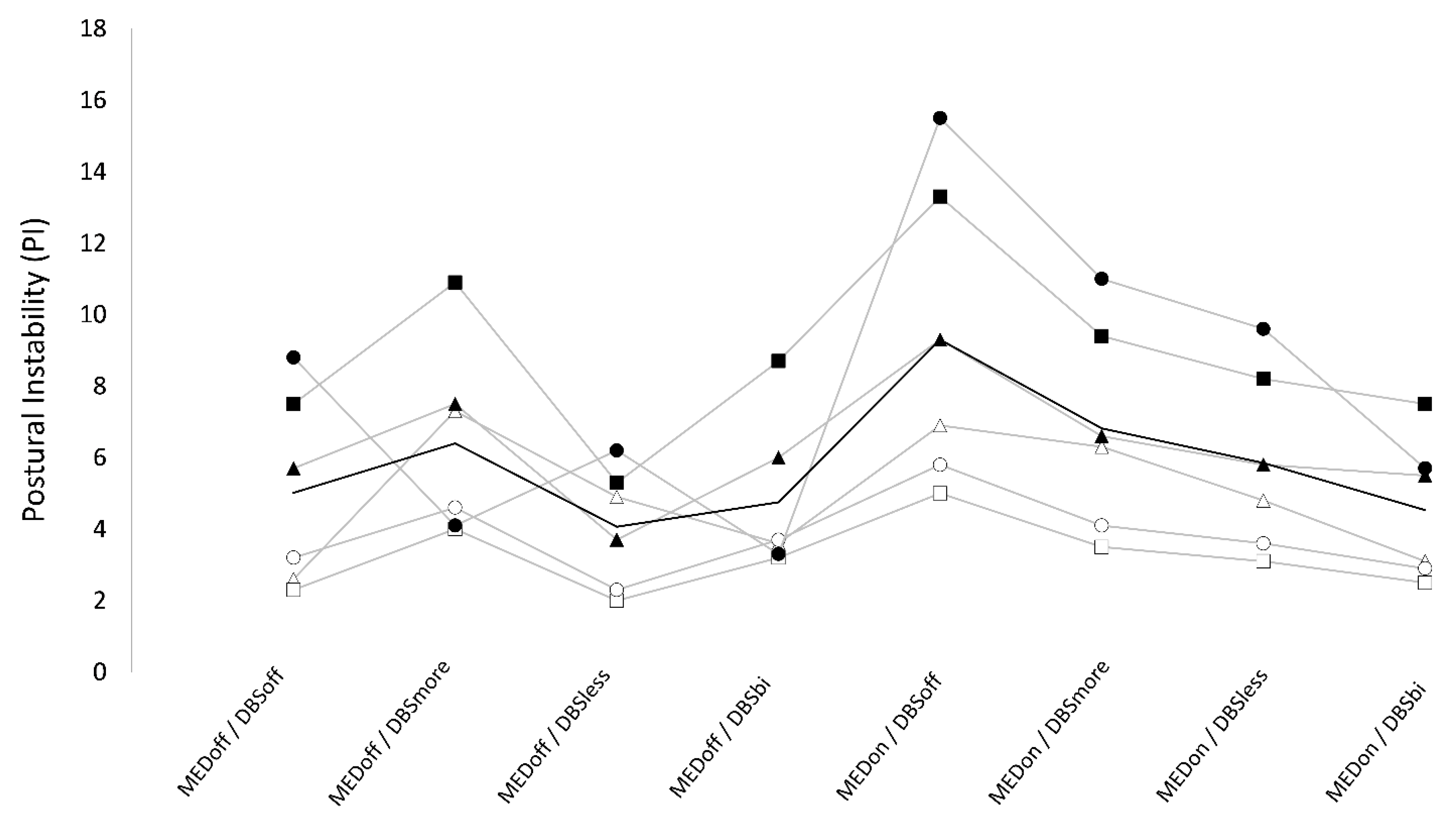
3.2. Postural Instability
3.2.1. Bilateral DBS
3.2.2. Unilateral DBS
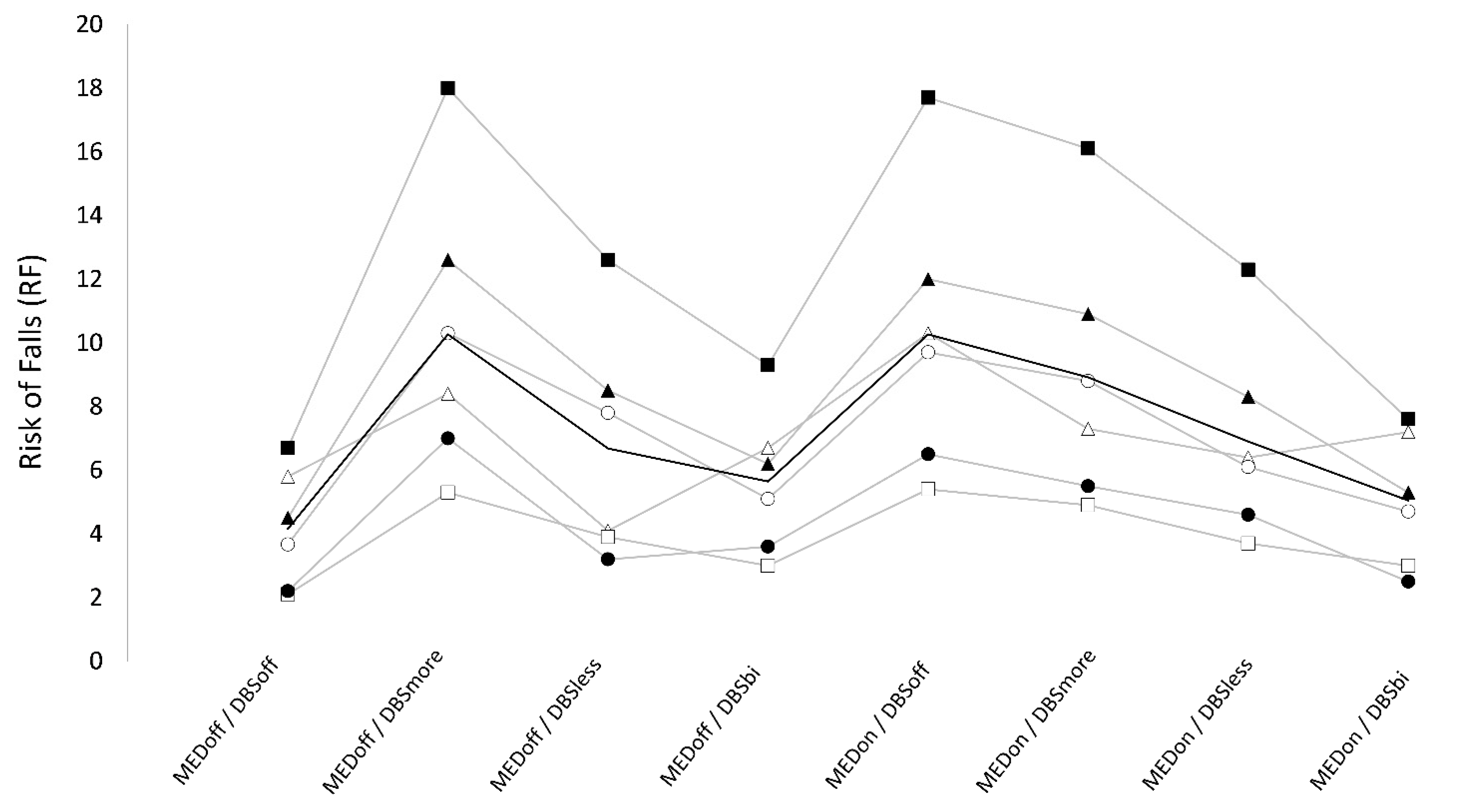
3.3. Risk of Falls
3.3.1. Bilateral DBS
3.3.2. Unilateral DBS
3.4. Summary of Results
3.4.1. Bilateral DBS
3.4.2. Unilateral DBS
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ivanenko, Y.; Gurfinkel, V.S. Human Postural Control. Front. Neurosci. 2018, 12, 171. [Google Scholar] [CrossRef] [PubMed]
- Nonnekes, J.; Goselink, R.J.M.; Růžička, E.; Fasano, A.; Nutt, J.G.; Bloem, B.R. Neurological disorders of gait, balance and posture: A sign-based approach. Nat. Rev. Neurol. 2018, 14, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Plotnik, M.; Bove, F.; Berardelli, A. The neurobiology of falls. Neurol. Sci. 2012, 33, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Schoneburg, B.; Mancini, M.; Horak, F.; Nutt, J.G. Framework for understanding balance dysfunction in Parkinson’s disease. Mov. Disord. 2013, 28, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Dimitrova, D.; Nutt, J.G. Direction-specific postural instability in subjects with Parkinson’s disease. Exp. Neurol. 2005, 193, 504–521. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Aquino, C.C.; Krauss, J.K.; Honey, C.R.; Bloem, B.R. Axial disability and deep brain stimulation in patients with Parkinson disease. Nat. Rev. Neurol. 2015, 11, 98–110. [Google Scholar] [CrossRef]
- Umemura, A.; Oka, Y.; Ohkita, K.; Yamawaki, T.; Yamada, K. Effect of subthalamic deep brain stimulation on postural abnormality in Parkinson disease. J. Neurosurg. 2010, 112, 1283–1288. [Google Scholar] [CrossRef]
- Artusi, C.A.; Zibetti, M.; Romagnolo, A.; Rizzone, M.G.; Merola, A.; Lopiano, L. Subthalamic deep brain stimulation and trunk posture in Parkinson’s disease. Acta Neurol. Scand. 2018, 137, 481–487. [Google Scholar] [CrossRef]
- St George, R.J.; Carlson-Kuhta, P.; Burchiel, K.J.; Hogarth, P.; Frank, N.; Horak, F.B. The effects of subthalamic and pallidal deep brain stimulation on postural responses in patients with Parkinson disease. J. Neurosurg. 2012, 116, 1347–1356. [Google Scholar] [CrossRef]
- Liu, W.; McIntire, K.; Kim, S.H.; Zhang, J.; Dascalos, S.; Lyons, K.E.; Pahwa, R. Bilateral subthalamic stimulation improves gait initiation in patients with Parkinson’s disease. Gait Posture 2006, 23, 492–498. [Google Scholar] [CrossRef]
- Brandmeir, N.J.; Brandmeir, C.L.; Carr, D.; Kuzma, K.; McInerney, J. Deep Brain Stimulation for Parkinson Disease Does not Worsen or Improve Postural Instability: A Prospective Cohort Trial. Neurosurgery 2018, 83, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Collomb-Clerc, A.; Welter, M.L. Effects of deep brain stimulation on balance and gait in patients with Parkinson’s disease: A systematic neurophysiological review. Neurophysiol. Clin. 2015, 45, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Crouse, J.J.; Phillips, J.R.; Jahanshahi, M.; Moustafa, A.A. Postural instability and falls in Parkinson’s disease. Rev. Neurosci. 2016, 27, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Nilsson, M.H.; Rehncrona, S.; Tjernström, F.; Magnusson, M.; Johansson, R.; Fransson, P.A. Effects of Deep Brain Stimulation on Postural Control in Parkinson’s Disease. Comput. Biol. Med. 2020, 122, 103828. [Google Scholar] [CrossRef] [PubMed]
- Fransson, P.A.; Nilsson, M.H.; Rehncrona, S.; Tjernström, F.; Magnusson, M.; Johansson, R.; Patel, M. Deep brain stimulation in the subthalamic nuclei alters postural alignment and adaptation in Parkinson’s disease. PLoS ONE 2021, 16, e0259862. [Google Scholar] [CrossRef] [PubMed]
- Schlenstedt, C.; Gavriliuc, O.; Boße, K.; Wolke, R.; Granert, O.; Deuschl, G.; Margraf, N.G. The Effect of Medication and Deep Brain Stimulation on Posture in Parkinson’s Disease. Front. Neurol. 2019, 10, 1254. [Google Scholar] [CrossRef]
- May, D.S.; van Dillen, L.R.; Earhart, G.M.; Rawson, K.S.; Perlmutter, J.S.; Duncan, R.P. Effects of Subthalamic Nucleus Deep Brain Stimulation and Levodopa on Balance in People with Parkinson’s Disease: A Cross Sectional Study. Brain Sci. 2020, 10, 693. [Google Scholar] [CrossRef]
- Lin, Z.; Zhang, C.; Li, D.; Sun, B. Lateralized effects of deep brain stimulation in Parkinson’s disease: Evidence and controversies. NPJ Parkinsons Dis. 2021, 7, 64. [Google Scholar] [CrossRef]
- Lizarraga, K.J.; Luca, C.C.; De Salles, A.; Gorgulho, A.; Lang, A.E.; Fasano, A. Asymmetric neuromodulation of motor circuits in Parkinson’s disease: The role of subthalamic deep brain stimulation. Surg. Neurol. Int. 2017, 8, 261. [Google Scholar] [CrossRef]
- Berardelli, A.; Wenning, G.K.; Antonini, A.; Berg, D.; Bloem, B.R.; Bonifati, V.; Brooks, D.; Burn, D.J.; Colosimo, C.; Fanciulli, A.; et al. EFNS/MDS-ES/ENS [corrected] recommendations for the diagnosis of Parkinson’s disease. Eur. J. Neurol. 2013, 20, 16–34. [Google Scholar] [CrossRef]
- Arnold, B.L.; Schmitz, R.J. Examination of balance measures produced by the biodex stability system. J. Athl. Train. 1998, 33, 323–327. [Google Scholar] [PubMed]
- Melzer, I.; Benjuya, N.; Kaplanski, J. Postural stability in the elderly: A comparison between fallers and non-fallers. Age Ageing 2004, 33, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Burleigh, A.; Horak, F.; Nutt, J.; Frank, J. Levodopa reduces muscle tone and lower extremity tremor in Parkinson’s disease. Can. J. Neurol. Sci. 1995, 22, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Crenna, P.; Carpinella, I.; Rabuffetti, M.; Rizzone, M.; Lopiano, L.; Lanotte, M.; Ferrarin, M. Impact of subthalamic nucleus stimulation on the initiation of gait in Parkinson’s disease. Exp. Brain Res. 2006, 172, 519–532. [Google Scholar] [CrossRef]
- Bloem, B.R.; Beckley, D.J.; van Dijk, J.G.; Zwinderman, A.H.; Remler, M.P.; Roos, R.A. Influence of dopaminergic medication on automatic postural responses and balance impairment in Parkinson’s disease. Mov. Disord. 1996, 11, 509–521. [Google Scholar] [CrossRef]
- Rocchi, L.; Chiari, L.; Cappello, A.; Gross, A.; Horak, F.B. Comparison between subthalamic nucleus and globus pallidus internus stimulation for postural performance in Parkinson’s disease. Gait Posture 2004, 19, 172–183. [Google Scholar] [CrossRef]
- Rocchi, L.; Palmerini, L.; Weiss, A.; Herman, T.; Hausdorff, J.M. Balance testing with inertial sensors in patients with Parkinson’s disease: Assessment of motor subtypes. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 1064–1071. [Google Scholar] [CrossRef]
- Grimbergen, Y.A.; Langston, J.W.; Roos, R.A.; Bloem, B.R. Postural instability in Parkinson’s disease: The adrenergic hypothesis and the locus coeruleus. Expert Rev. Neurother. 2009, 9, 279–290. [Google Scholar] [CrossRef]
- Bohnen, N.I.; Frey, K.A.; Studenski, S.; Kotagal, V.; Koeppe, R.A.; Scott, P.J.; Albin, R.L.; Müller, M.L. Gait speed in Parkinson disease correlates with cholinergic degeneration. Neurology 2013, 81, 1611–1616. [Google Scholar] [CrossRef]
- Pötter-Nerger, M.; Volkmann, J. Deep brain stimulation for gait and postural symptoms in Parkinson’s disease. Mov. Disord. 2013, 28, 1609–1615. [Google Scholar] [CrossRef]
- Nantel, J.; McDonald, J.C.; Bronte-Stewart, H. Effect of medication and STN-DBS on postural control in subjects with Parkinson’s disease. Park. Relat. Disord. 2012, 18, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Weil, R.S.; Schrag, A.E.; Warren, J.D.; Crutch, S.J.; Lees, A.J.; Morris, H.R. Visual dysfunction in Parkinson’s disease. Brain 2016, 139, 2827–2843. [Google Scholar] [CrossRef] [PubMed]
- Bronte-Stewart, H.M.; Minn, A.Y.; Rodrigues, K.; Buckley, E.L.; Nashner, L.M. Postural instability in idiopathic Parkinson’s disease: The role of medication and unilateral pallidotomy. Brain 2002, 125, 2100–2114. [Google Scholar] [CrossRef] [PubMed]
- Welter, M.L.; Demain, A.; Ewenczyk, C.; Czernecki, V.; Lau, B.; El Helou, A.; Belaid, H.; Yelnik, J.; François, C.; Bardinet, E.; et al. PPNa-DBS for gait and balance disorders in Parkinson’s disease: A double-blind, randomised study. J. Neurol. 2015, 262, 1515–1525. [Google Scholar] [CrossRef]
- Brandmeir, N.J.; Brandmeir, C.L.; Kuzma, K.; McInerney, J. A Prospective Evaluation of an Outpatient Assessment of Postural Instability to Predict Risk of Falls in Patients with Parkinson’s Disease Presenting for Deep Brain Stimulation. Mov. Disord. Clin. Pract. 2016, 3, 151–155. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Subjects | Age (ys) | Gender | Diseases Duration (ys) | UPDRS III OFF | UPDRS III ON | More Affected Side | LEDDS |
|---|---|---|---|---|---|---|---|
| 01 | 72 | F | 20 | 96 | 72 | R | 240 |
| 02 | 65 | F | 14 | 85 | 65 | L | 250 |
| 03 | 69 | M | 19 | 50 | 39 | R | 436 |
| 04 | 58 | F | 18 | 40 | 23 | R | 620 |
| 05 | 62 | M | 12 | 46 | 38 | L | 540 |
| 06 | 72 | M | 20 | 67 | 59 | R | 500 |
| Avg | 66 ± 6 | F/M 3/3 | 17 ± 3 | 64 ± 23 | 49 ± 19 | R/L 4/2 | 416 ± 147 |
| 2-Way ANOVA | ||||||
|---|---|---|---|---|---|---|
| Factor | DV | df | F | p | ||
| Postural Instability (PI) | ||||||
| Stim | PI | 3;15 | 5.51 | 0.009 | ||
| Med | PI | 1;5 | 5.4 | 0.068 | ||
| Stim * Med | PI | 3;15 | 12.48 | <0.001 | ||
| Risk of falls (RF) | ||||||
| Stim | RF | 3;15 | 12.92 | 0.01 | ||
| Med | RF | 1;5 | 18.61 | 0.008 | ||
| Stim × Med | RF | 3;15 | 22.7 | 0.003 | ||
| Pairwise comparisons | ||||||
| PI | RF | |||||
| t | p | adj. p | t | p | adj. p | |
| MEDoff/DBSoff vs. MEDoff/DBSmore | 1.04 | 0.345 | 0.467 | 4.62 | 0.006 | 0.014 |
| MEDoff/DBSoff vs. MEDoff/DBSless | 1.34 | 0.239 | 0.353 | 2.41 | 0.061 | 0.074 |
| MEDoff/DBSoff vs. MEDoff/DBSbil. | 0.25 | 0.810 | 0.810 | 5.08 | 0.004 | 0.014 |
| MEDoff/DBSoff vs. MEDon/DBSoff | 5.99 | 0.002 | 0.035 | 4.98 | 0.004 | 0.014 |
| MEDoff/DBSoff vs. MEDon/DBSmore | 4.04 | 0.010 | 0.035 | 3.98 | 0.011 | 0.018 |
| MEDoff/DBSoff vs. MEDon/DBSless | 2.94 | 0.032 | 0.075 | 3.68 | 0.014 | 0.023 |
| MEDoff/DBSoff vs. MEDon/DBSbil. | 0.90 | 0.411 | 0.523 | 4.16 | 0.009 | 0.018 |
| MEDoff/DBSmore vs. MEDoff/DBSless | 2.24 | 0.075 | 0.132 | 6.84 | 0.001 | 0.014 |
| MEDoff/DBSmore vs. MEDoff/DBSbil. | 3.54 | 0.017 | 0.052 | 4.46 | 0.007 | 0.014 |
| MEDoff/DBSmore vs. MEDon/DBSoff | 1.66 | 0.157 | 0.244 | 0.33 | 0.758 | 0.758 |
| MEDoff/DBSmore vs. MEDon/DBSmore | 0.32 | 0.763 | 0.791 | 9.59 | 0.000 | 0.006 |
| MEDoff/DBSmore vs. MEDon/DBSless | 0.44 | 0.678 | 0.756 | 5.77 | 0.002 | 0.014 |
| MEDoff/DBSmore vs. MEDon/DBSbil. | 2.29 | 0.071 | 0.132 | 4.07 | 0.010 | 0.018 |
| MEDoff/DBSless vs. MEDoff/DBSbil. | 0.71 | 0.508 | 0.592 | 1.35 | 0.235 | 0.253 |
| MEDoff/DBSless vs. MEDon/DBSoff | 4.38 | 0.007 | 0.035 | 4.46 | 0.007 | 0.014 |
| MEDoff/DBSless vs. MEDon/DBSmore | 4.69 | 0.005 | 0.035 | 5.11 | 0.004 | 0.014 |
| MEDoff/DBSless vs. MEDon/DBSless | 3.41 | 0.019 | 0.053 | 0.48 | 0.654 | 0.678 |
| MEDoff/DBSless vs. MEDon/DBSbil. | 0.78 | 0.473 | 0.576 | 1.54 | 0.184 | 0.207 |
| MEDoff/DBSbil. vs. MEDon/DBSoff | 2.87 | 0.035 | 0.075 | 4.93 | 0.004 | 0.014 |
| MEDoff/DBSbil. vs. MEDon/DBSmore | 1.75 | 0.141 | 0.233 | 3.61 | 0.015 | 0.024 |
| MEDoff/DBSbil. vs. MEDon/DBSless | 1.03 | 0.350 | 0.467 | 2.77 | 0.039 | 0.053 |
| MEDoff/DBSbil. vs. MEDon/DBSbil. | 0.41 | 0.702 | 0.756 | 1.91 | 0.115 | 0.134 |
| MEDon/DBSoff vs. MEDon/DBSmore | 4.06 | 0.010 | 0.035 | 3.29 | 0.022 | 0.030 |
| MEDon/DBSoff vs. MEDon/DBSless | 4.96 | 0.004 | 0.035 | 5.68 | 0.002 | 0.014 |
| MEDon/DBSoff vs. MEDon/DBSbil. | 4.30 | 0.008 | 0.035 | 4.56 | 0.006 | 0.014 |
| MEDon/DBSmore vs. MEDon/DBSless | 5.06 | 0.004 | 0.035 | 4.45 | 0.007 | 0.014 |
| MEDon/DBSmore vs. MEDon/DBSbil. | 3.31 | 0.021 | 0.054 | 3.33 | 0.021 | 0.030 |
| MEDon/DBSless vs. MEDon/DBSbil. | 2.39 | 0.063 | 0.125 | 2.56 | 0.051 | 0.065 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leodori, G.; Santilli, M.; Modugno, N.; D’Avino, M.; De Bartolo, M.I.; Fabbrini, A.; Rocchi, L.; Conte, A.; Fabbrini, G.; Belvisi, D. Postural Instability and Risk of Falls in Patients with Parkinson’s Disease Treated with Deep Brain Stimulation: A Stabilometric Platform Study. Brain Sci. 2023, 13, 1243. https://doi.org/10.3390/brainsci13091243
Leodori G, Santilli M, Modugno N, D’Avino M, De Bartolo MI, Fabbrini A, Rocchi L, Conte A, Fabbrini G, Belvisi D. Postural Instability and Risk of Falls in Patients with Parkinson’s Disease Treated with Deep Brain Stimulation: A Stabilometric Platform Study. Brain Sciences. 2023; 13(9):1243. https://doi.org/10.3390/brainsci13091243
Chicago/Turabian StyleLeodori, Giorgio, Marco Santilli, Nicola Modugno, Michele D’Avino, Maria Ilenia De Bartolo, Andrea Fabbrini, Lorenzo Rocchi, Antonella Conte, Giovanni Fabbrini, and Daniele Belvisi. 2023. "Postural Instability and Risk of Falls in Patients with Parkinson’s Disease Treated with Deep Brain Stimulation: A Stabilometric Platform Study" Brain Sciences 13, no. 9: 1243. https://doi.org/10.3390/brainsci13091243