1. Introduction
In modern neurosurgery, minimally invasive skull base techniques are the cornerstone for treating lesions at the base of the skull [
1].
The pterional approach is the gold standard technique for treating several pathologies of the skull base [
2,
3,
4,
5,
6,
7,
8,
9]. This approach offers the opportunity to treat lesions of the anterior and middle fossa and of the union of the medium and upper third of the clivus. A combination with other surgical techniques, such as the orbitozigomatic approach, allows for the treatment of neoplastic lesions that occupy large and complex skull base compartments [
2,
10,
11,
12,
13].
Traditionally, minimally invasive techniques consider a careful dissection of the temporal fossa’s soft tissues to avoid the inherent risk of injury from handling brain tissue and cranial nerves. However, even in the most experienced hands, these valuable techniques require a relatively longer surgical time. In addition, they will be associated with non-negligible blood loss, pain, postoperative complications, and a longer recovery, in addition to the esthetic and functional sequelae that can occur—a loss of hair on the suture line on the skin, a higher frequency of defects in the skin surface of the temporal region secondary to the atrophy of the temporalis muscle, and temporomandibular joint dysfunction.
The sphenoid ridge approach (SRA) is a minimally invasive technique commonly used to treat pathologies near the Sylvian fissure [
14]. It has been demonstrated to be safe and effective in treating aneurysms of the bifurcation of the internal carotid and middle cerebral arteries. Some isolated reports have suggested that an extended variation in this approach, involving the removal of the orbital roof, pterion, sphenoid wing, and anterior clinoid process, along with an extradural anterior clinoidectomy, can further expand the surgical field and provide access to the most profound areas of the skull base [
15,
16,
17,
18,
19,
20,
21,
22,
23,
24].
Pediatric patients lack formal descriptions of minimally invasive techniques for treating neoplastic lesions in their supraorbital, sellar, suprasellar, and parasellar regions. Hence, this report aims to describe the benefits of the E-SRA for managing skull base tumors in pediatric patients.
Therefore, in this study, we propose a comprehensive extended approach to the sphenoid ridge (E-SRA), which includes a centered craniotomy at the pterion, in addition to the removal of the orbital walls (roof and lateral wall), greater sphenoid wing, and anterior clinoid process. This extended technique aims to reach the most profound areas of the skull base.
2. Patients and Methods
From 1 March 2015 to 30 June 2020, a total of 115 patients with presumptive diagnoses of neoplastic lesions located in their supraorbital, sellar, suprasellar, and parasellar regions were identified from the Department of Neurosurgery at the National Institute of Pediatrics of Mexico. Among these patients, 36 were selected to undergo a biopsy or gross total resection by E-SRA. The biopsy cases were considered a priori when a suspicion of a visual pathway glioma and germ cell tumors did not show conclusive tumor markers in the preoperative evaluation. The E-SRA procedure was followed based on a collegiate decision made by the Neurosurgery Department. In addition, informed consent from the patients’ parents for the surgical procedure was obtained. The Ethics and Research Committee of the National Institute of Pediatrics evaluated and approved this study.
The criteria for selecting patients for the E-SRA procedure were as follows: (1) no history of prior surgery involving the pterion region; (2) radiological evidence of neoplastic lesions with a solid component volume of less than 50 cm3; and (3) patients with neoplastic lesions suggestive of an optic pathway glioma. Patients who did not meet the criteria for the E-SRA were treated using conventional craniotomy and skull base surgery techniques.
E-SRA Technique: The SRA approach was performed as previously described [
1]. A skin incision was made approximately 4 to 5 cm below the hairline and behind the external border of the eye, centered at the estimated location of the pterion. After the dissection of the skin and subcutaneous tissue, the superficial fascia and temporal muscle fibers were dissected along the skin incision. Next, a subperiosteal dissection was performed to expose the pterional region. A single burr hole was then made behind the pterion, followed by a small craniotomy (3 × 3 cm) around the visible landmarks of the sphenoid ridge. The hemostasis of the middle meningeal artery and dural vessels was achieved using a bipolar electrode after removing the bone flap. Once the pterion was removed, a triangular bone structure, defined by specific orbital points, became visible. The anterosuperior point, located at the upper and anterior angles, represented the union of the frontal bone and the internal table of the orbital roof. The posteromedial point, positioned at the medial and inferior angles, corresponded to the junction of the greater wing of the sphenoid bone and the base of the anterior clinoid process, projecting into the deep outer boundary of the superior orbital fissure. Finally, the posteroinferior point, found at the posterior and inferior angles, denoted the union of the internal table of the temporal bone and the wing of the sphenoid bone. The outer edge of the superior orbital fissure was delineated, and the meningo-orbital fold and meningo-orbital artery were dissected and coagulated to access the body and apex of the clinoid. The anterior clinoid process was drilled out and the optic strut was released at the lateral wall of the optic canal. At this stage, a dissection of the pretemporal dura allowed for an expanded surgical field of view, avoiding the use of brain retractors. Following the contour of the craniotomy edge, a dural opening was made, leaving a 5 mm free margin. After the tumor resection, the dura was sutured using a water seal technique with a 4–0 nylon suture. Sometimes, the use of a dural sealant reduces the risk of cerebrospinal fluid leakage. Next, the bone flap was repositioned and secured with non-absorbable sutures or mini plates. Finally, the temporal fascia and muscle were repaired using a 2–0 absorbable suture and the skin was closed with a 4–0 nylon suture. Subgaleal drainages were not utilized in our case (
Figure 1 and
Video S1).
The surgical objective was determined a priori based on the surgical plan established during the Department of Neurosurgery’s session. The patients were categorized into two groups: those undergoing a biopsy and those undergoing an extensive resection surgery. Extensive resection surgery was considered when a neoplastic remanent accounted for less than 5% of the volume.
The evaluation of the surgical procedure included the length of the skin incision and the extension of the craniotomy, the time required to perform the E-SRA, and the associated bleeding. The complications were analyzed by reviewing all the clinical records until the patient was discharged from the institution and over a 24-month follow-up period. The statistical analysis presented the results as mean (±) standard deviation and ranges (lower and higher) for the quantitative variables and frequencies (%) for the qualitative variables.
3. Results
Patients and the Extended Sphenoid Ridge Approach Technique. We included 36 patients with a mean age of 7.8 ± 3 years; 17 male and 19 female patients were enrolled. The mean length of the skin incision was 4.2 ± 0.8 cm (3.4–5 cm) and that for the craniotomy area measured was 3.1 ± 0.5 cm
2 (2.6–3.6 cm
2). The average time taken to perform the E-SRA was 36 ± 6 min (30–42 min) and the quantified bleeding during the procedure was 20 ± 5 mL (15–25 mL). Brain retractors were not utilized in any of the cases and a dynamic retraction using cotton patties, bipolar forceps, and suction devices was preferred (
Table 1).
Surgical objective. In all the patients, the objective of the surgery was accomplished: either a biopsy (22%) or a surgical excision (78%). A biopsy was performed in eight cases, when the intraoperative histopathological diagnoses were an optic pathway glioma (n = 4) or germinoma (n = 4). In 28 patients, an extensive surgical resection was performed (78%). It was considered total in 28 cases (86%) and subtotal (>90% volume) in 4 cases (14%) due to the invasion of diencephalic structures.
Histopathological diagnosis. The most common histopathological diagnosis was adamantinomatous craniopharyngioma (n = 22), followed, in order of frequency, by germinal tumors (n = 6), visual pathway gliomas (n = 4), pituitary adenoma (n = 3), and, in one case, orbital Ewing’s sarcoma (n = 1).
Complications. Vascular injury. No vascular injuries related to the approach were observed—specifically, injuries to the internal carotid artery during the anterior clinoidectomy. In one case, there was a vascular injury at the origin of the contralateral posterior communicating artery during the dissection of the tumor capsule. It was controlled by applying an aneurysm clip (
Video S2). One patient with Ewing’s sarcoma presented a cerebrospinal fluid leak related to the infiltration of the dura mater above the orbital roof; two patients (5.5%) developed subgaleal hematomas in their temporal regions. No patient required further surgery to treat complications. Other than removing the orbital roof and lateral wall, we did not observe pulsatile exophthalmos. Despite the superior orbital fissure dissection, we did not observe clinical manifestations regarding cranial nerve paresis.
4. Discussion
The pterional approach, which was first described in the late 1970s, has become widely used for treating supratentorial neurosurgical diseases. It is considered to be the primary surgical corridor for accessing the skull base. In this study, we found that the extended sphenoid ridge approach (E-SRA) provided a safe and effective method for accessing neoplastic lesions in the skull bases of pediatric patients.
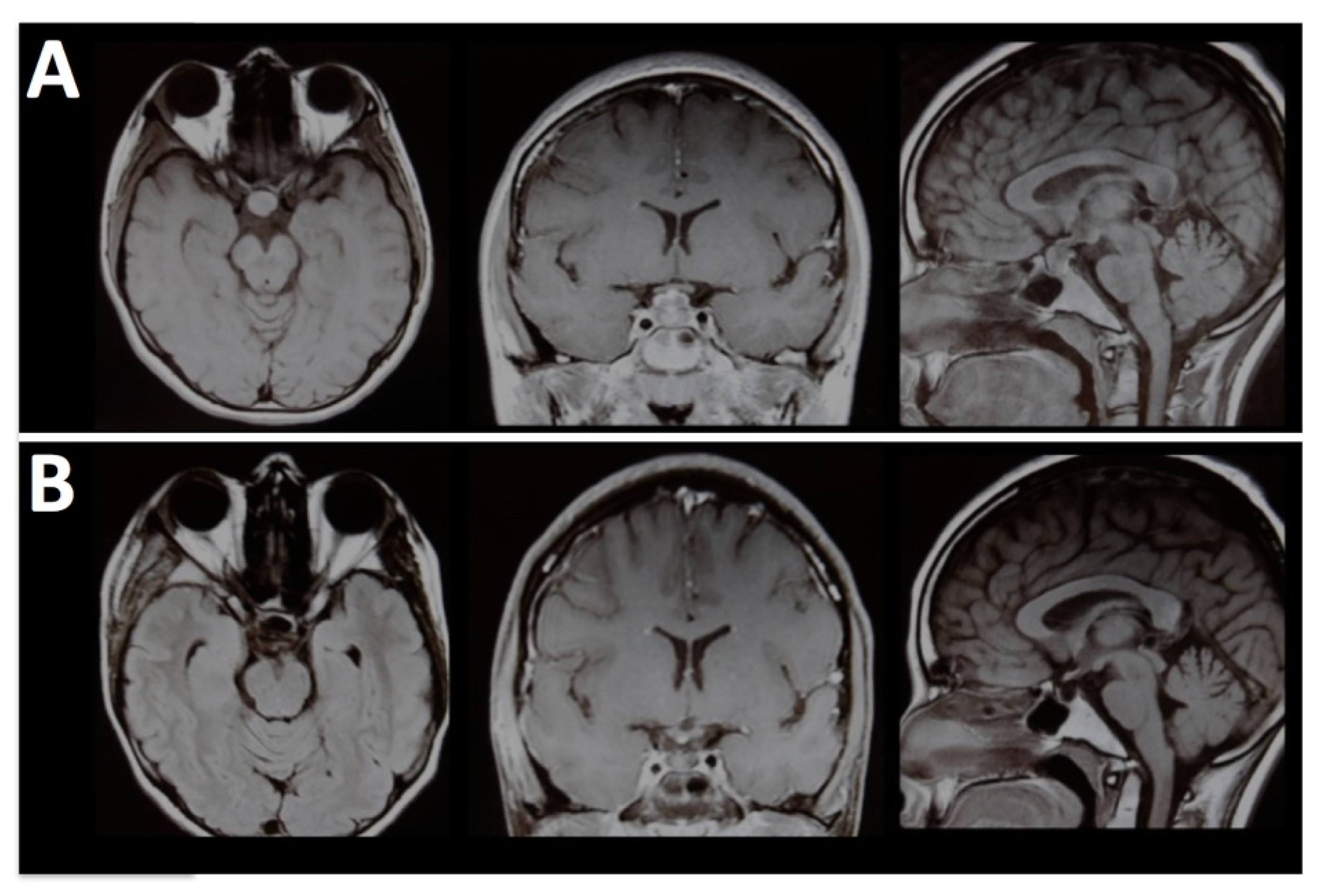
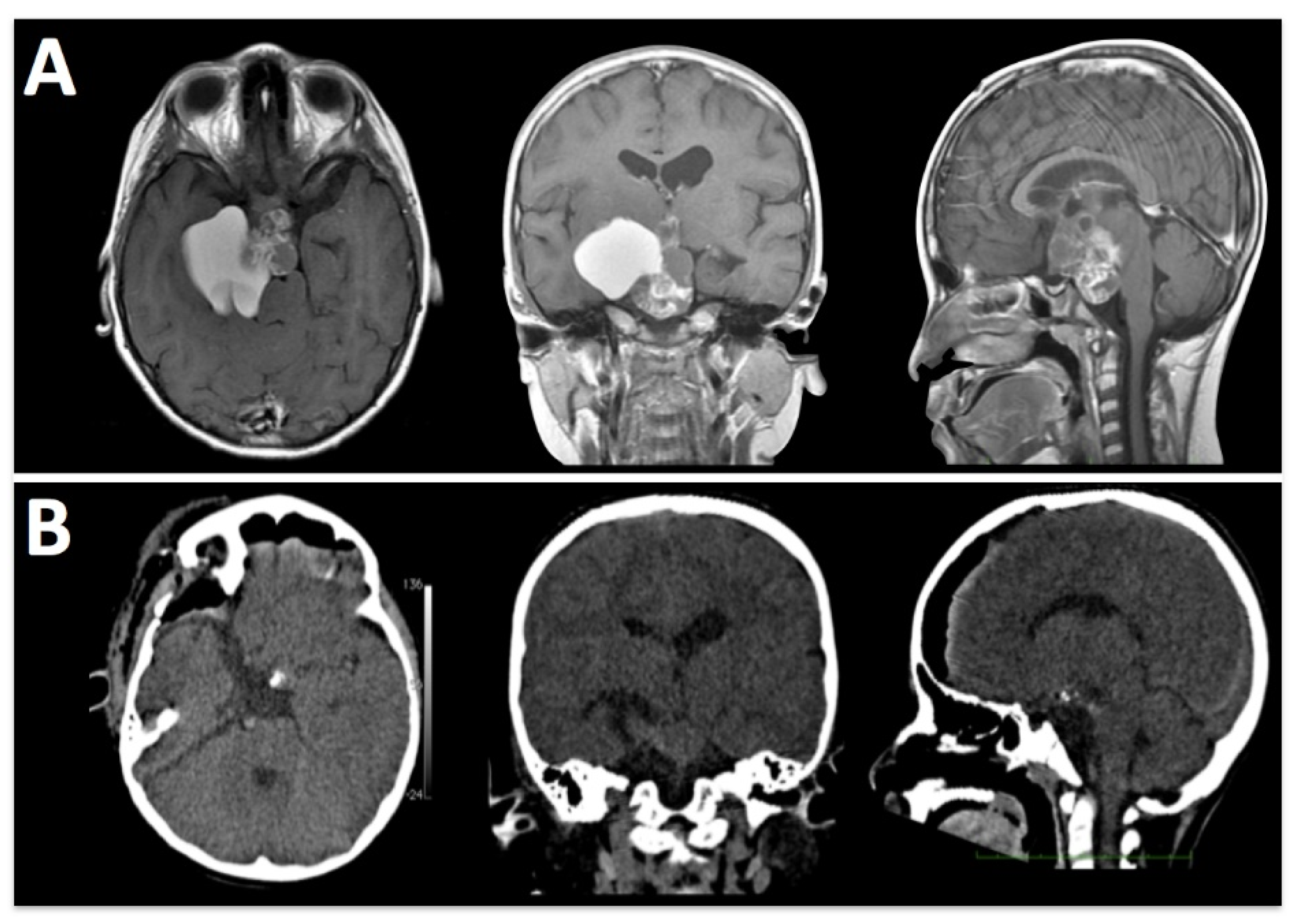
By removing the orbital roof and lateral wall, the E-SRA technique allows for transcranial access to extraconal lesions, including those with an ethmoidal extension. This expanded access enables surgeons to reach tumors in challenging locations (
Figure 2).
The E-SRA approach offers several advantages, including a shorter operative time, minimal bleeding, and a lower rate of complications. These benefits contribute to its improved surgical outcomes and patient recovery. However, it is essential to note that complications related to dural closure were the most frequently observed in our study.
Traditionally, various approaches, such as the supraorbital, subfrontal, pterional, and orbitozygomatic approaches, reach lesions in the sellar, suprasellar, and parasellar regions. However, these techniques pose specific risks to pediatric patients, including a longer surgical time, an increased bleeding volume, extensive soft tissue dissection, potential facial nerve injury, and a risk of temporomandibular dysfunction (
Figure 3).
In this study, the extended sphenoid ridge approach (E-SRA) provided comparable exposure with other skull base approaches, while minimizing the need for extensive soft tissue dissection (
Figure 4).
The E-SRA technique allows for access to various structures in the skull base. The subfrontal corridor provides access to the olfactory nerves, optic nerves, inter-optic space, chiasm, lamina terminalis, A1 segment of the anterior cerebral artery, and anterior communicating artery. Dissecting Liliquist’s membrane allows for access to the interpeduncular cistern, posterior cerebral arteries, superior cerebellar arteries, basilar tip, and trunk.
Figure 5 and
Figure 6 and
Video S2.
Understanding the complex dural arrangement in the pterional region is crucial. Our observations indicate that the meningo-orbital dural fold plays a critical role as a crossroad between the superior orbital fissure, pretemporal dura, and lateral wall of the cavernous sinus. A blunt dissection initiated at the meningo-orbital fold allows for a confident dissection of the dural sheath of the superior orbital fissure and the base and lateral aspects of the anterior clinoid process. In addition, removing the anterior clinoid process tip reveals the dural transition between the pretemporal dura and the lateral wall of the cavernous sinus in an anteromedial direction. These dural folds are relevant, as their early identification and dissection create a wide corridor to the cavernous sinus and its delicate contents. Thus, an adequate dissection of the meningo-orbital fold plays a crucial role in creating a wide corridor to access the orbital fissure, pretemporal dura, and lateral wall of the cavernous sinus (
Video S1).
Vascular damage, such as cavernous sinus or carotid artery injuries, was not observed during the E-SRA procedure. In one case, a vascular clip was applied at the origin of the contralateral posterior communicating artery during the craniopharyngioma’s capsule dissection.
When the approach to the sphenoid ridge was described, there was significant criticism regarding fixing complications related to vascular incidents. However, the video shows that it was possible to address this complication by placing an aneurysm clip at the origin of the posterior communicating artery. Clinically, the patient did not experience any functional decline, and subsequent imaging evaluations identified circulation in the affected vessel (
Video S2).
While transnasal endoscopic techniques help to treat tumors near the sphenoid sinus, their application in pediatric patients is limited and has specific challenges due to the poor pneumatization of the sphenoid sinus and an increased risk of vascular accidents. However, neuronavigation platforms can aid in directing a safe sphenoid bone removal to reach the sellar floor.
In conclusion, the extended sphenoid ridge approach is a safe and viable surgical option for treating intracranial tumors in pediatrics. This procedure should be considered among the available neurosurgical techniques, and our study provides a systematic description of skull base techniques for pediatric patients.
Author Contributions
Conceptualization, R.G.-N.; Data curation, R.G.-N., A.M.-B., J.T.-L. and J.L.P.-G.; Formal analysis, R.G.-N.; Investigation, R.G.-N.; Methodology, R.G.-N.; Visualization, R.G.-N.; Writing—original draft, R.G.-N.; Writing—review &editing, R.G.-N., A.M.-B., J.T.-L. and J.L.P.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no specific grant from the public, commercial, or not-for-profit funding agencies.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the National Institute of Pediatrics of Mexico (Protocol code GA143/2010, approved on 11 August 2010), for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all patient´s parents involved in the study.
Data Availability Statement
No data is available due to privacy or ethical restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| E-SRA | Extended Sphenoid Ridge Approach |
| SRA | Sphenoid Ridge Approach |
References
- Yasargil, M.G.; Antic, J.; Laciga, R.; Jain, K.K.; Hodosh, R.M.; Smith, R.D. Microsurgical pterional approach to aneurysms of the basilar bifurcation. Surg. Neurol. 1976, 6, 83–91. [Google Scholar]
- Alleyne, C.H., Jr.; Barrow, D.L.; Oyesiku, N.M. Combined transsphenoidal and pterional craniotomy approach to giant pituitary tumors. Surg. Neurol. 2002, 57, 380–390; discussion 390. [Google Scholar] [CrossRef]
- Al-Mefty, O. Supraorbital-pterional approach to skull base lesions. Neurosurgery 1987, 21, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Anson, J.A. Treatment strategies for intracranial fusiform aneurysms. Neurosurg. Clin. N. Am. 1998, 9, 743. [Google Scholar] [PubMed]
- Arnold, H.; Herrmann, H.D. Skull base chordoma with cavernous sinus involvement. Partial or radical tumour-removal? Acta Neurochir. 1986, 83, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Backlund, E.O. Pterional approach for orbital decompression. Acta Ophthalmol. 1968, 46, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Carmel, P.W.; Antunes, J.L.; Chang, C.H. Craniopharyngiomas in children. Neurosurgery 1982, 11, 382–389. [Google Scholar] [CrossRef]
- Carrizo, A.; Basso, A. Current surgical treatment for sphenoorbital meningiomas. Surg. Neurol. 1998, 50, 574–578. [Google Scholar] [CrossRef]
- Day, A.L. Aneurysms of the ophthalmic segment. A clinical and anatomical analysis. J. Neurosurg. 1990, 72, 677–691. [Google Scholar] [CrossRef] [Green Version]
- Alaywan, M.; Sindou, M. Fronto-temporal approach with orbito-zygomatic removal surgical anatomy. Acta Neurochir. 1990, 104, 79–83. [Google Scholar] [CrossRef]
- Cantore, G.; Santoro, A.; Da Pian, R. Spontaneous occlusion of supraclinoid aneurysms after the creation of extra-intracranial bypasses using long grafts: Report of two cases. Neurosurgery 1999, 44, 216–219; discussion 219–220. [Google Scholar] [CrossRef] [PubMed]
- Day, J.D.; Giannotta, S.L.; Fukushima, T. Extradural temporopolar approach to lesions of the upper basilar artery and infrachiasmatic region. J. Neurosurg. 1994, 81, 230–235. [Google Scholar] [CrossRef]
- Dolenc, V.V. A combined transorbital-transclinoid and transsylvian approach to carotid-ophthalmic aneurysms without retraction of the brain. Acta Neurochir. Suppl. 1999, 72, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Nathal, E.; Gomez-Amador, J.L. Anatomic and surgical basis of the sphenoid ridge keyhole approach for cerebral aneurysms. Neurosurgery 2005, 56 (Suppl. S1), 178–185, discussion 178–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolenc, V.V. Frontotemporal epidural approach to trigeminal neurinomas. Acta Neurochir. 1994, 130, 55–65. [Google Scholar] [CrossRef]
- Andaluz, N.; van Loveren, H.R.; Keller, J.T.; Zuccarello, M. The One-Piece Orbitopterional Approach. Skull Base 2003, 13, 241–245. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.J. The “no-drill” technique of anterior clinoidectomy: A cranial base approach to the paraclinoid and parasellar region. Neurosurgery 2009, 64 (Suppl. S3), ons96–105; discussion ons105–106. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, J.A.; Kawarazaki, A.; Hashimoto, N. Intradural en-bloc removal of the anterior clinoid process. Acta Neurochir. 2004, 146, 505–509. [Google Scholar] [CrossRef]
- Bayassi, S. Fałd oponowo-oczodołowy jako kierunkowskaz zewnatrzoponowego dojścia do wyrostka pochyłego przedniego [Meningo-orbital fold (MOF) as a guiding point in extradural approach to the anterior clinoid process]. Neurol. Neurochir. Pol. 2005, 39, 49–55. [Google Scholar]
- Lee, K.S. Extradural approach to the lateral sellar compartment. Yonsei Med. J. 2001, 42, 120–127. [Google Scholar] [CrossRef]
- Kobayashi, M.; Yoshida, K.; Kawase, T. Inter-dural approach to parasellar tumors. Acta Neurochir. 2010, 152, 279–284; discussion 284–285. [Google Scholar] [CrossRef] [PubMed]
- Coscarella, E.; Başkaya, M.K.; Morcos, J.J. An alternative extradural exposure to the anterior clinoid process: The superior orbital fissure as a surgical corridor. Neurosurgery 2003, 53, 162–166; discussion 166–167. [Google Scholar] [CrossRef] [PubMed]
- Visot, A.; Boulin, A. Les voies d’abord du sphénoïde [Sphenoid bone: Surgical techniques]. J. Neuroradiol. 2003, 30, 258–267. [Google Scholar] [PubMed]
- Acharya, R.; Shaya, M.; Kumar, R.; Caldito, G.C.; Nanda, A. Quantification of the advantages of the extended frontal approach to skull base. Skull Base 2004, 14, 133–142; discussion 141–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}