
Endoscopic Endonasal Approach in Craniopharyngiomas: Representative Cases and Technical Nuances for the Young Neurosurgeon
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
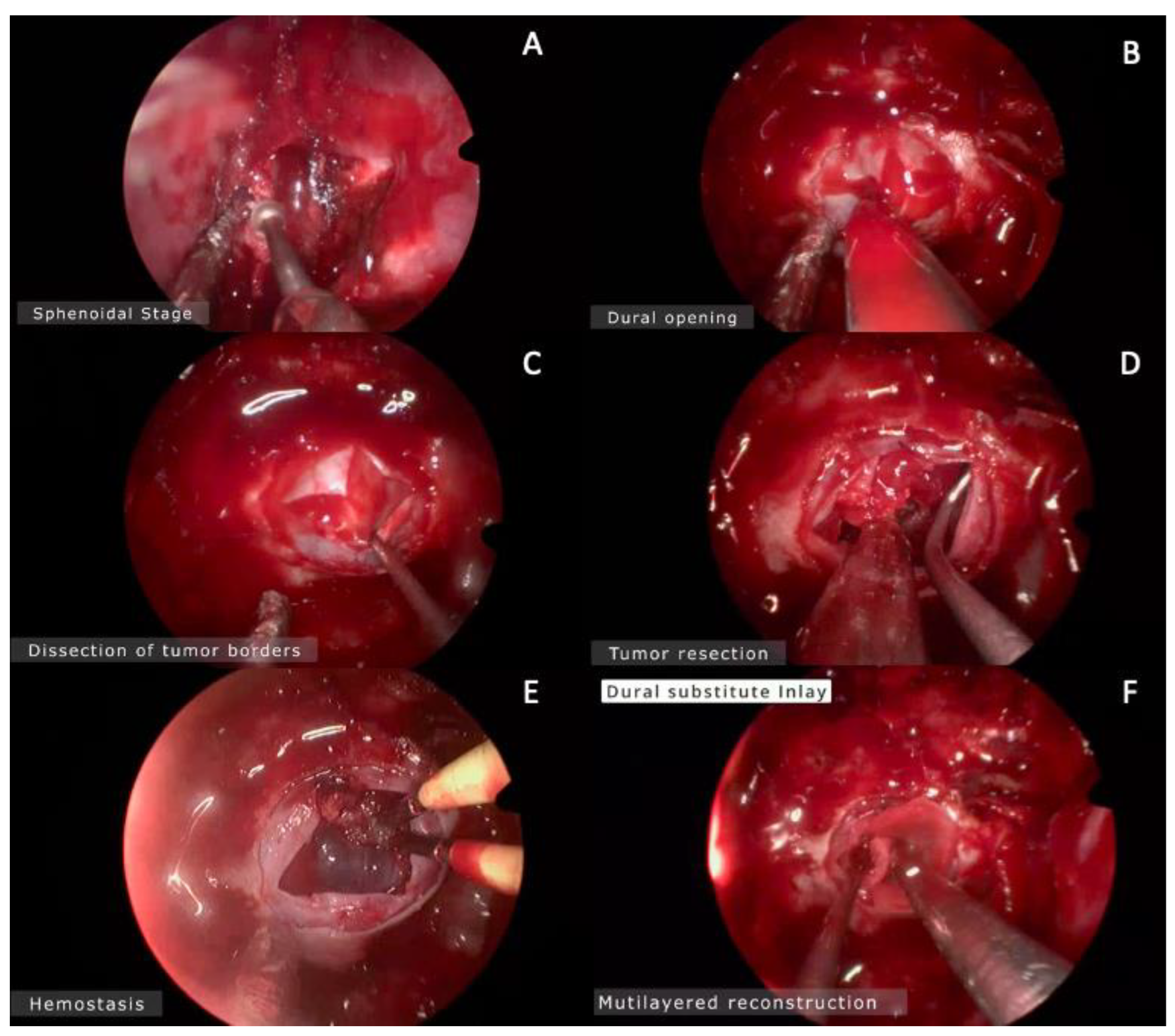
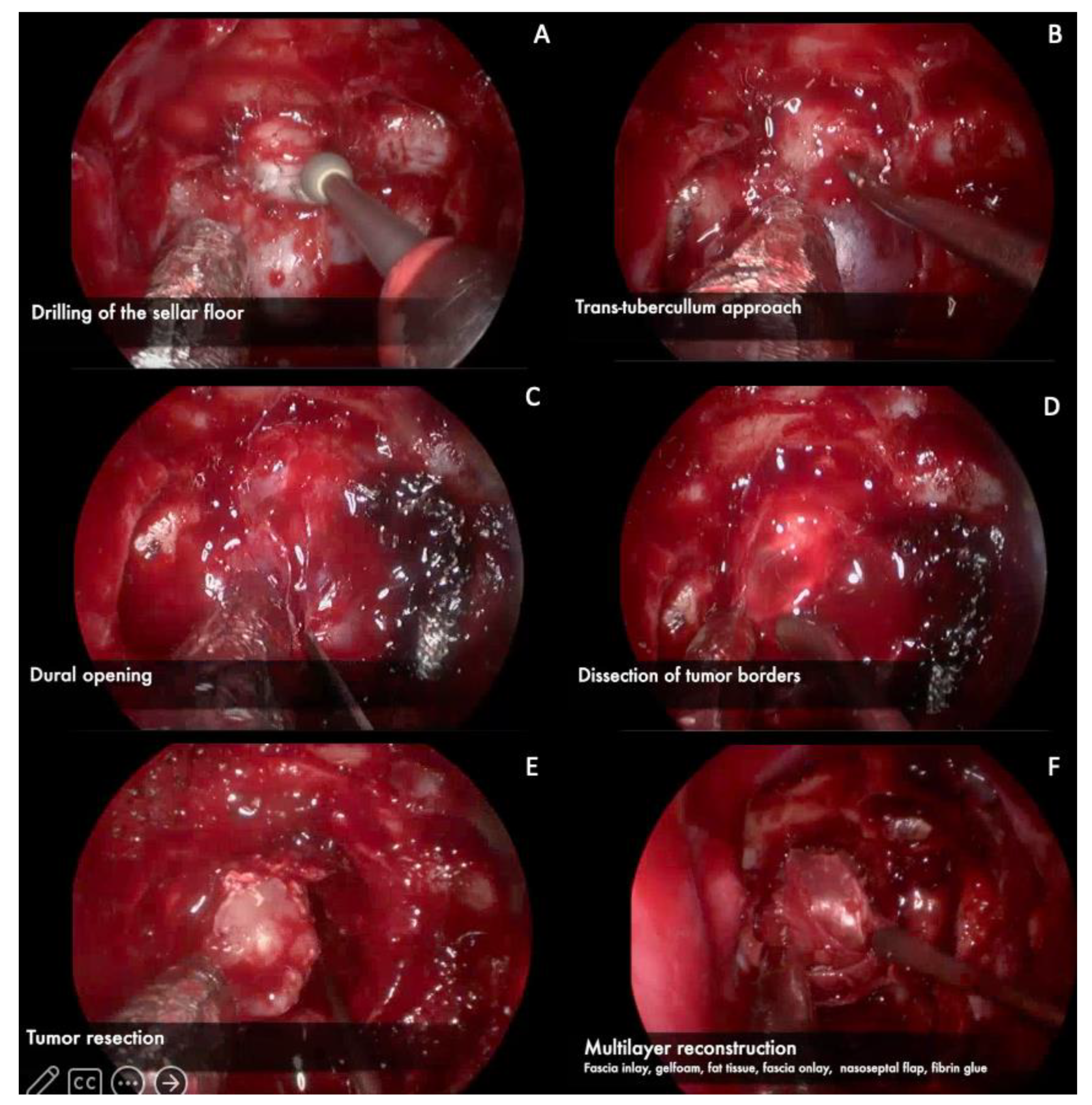
3.1. Endoscopic Endonasal Approach
3.1.1. Nasal Phase
3.1.2. Sphenoidal Phase
3.1.3. Sellar Phase
3.1.4. Closure
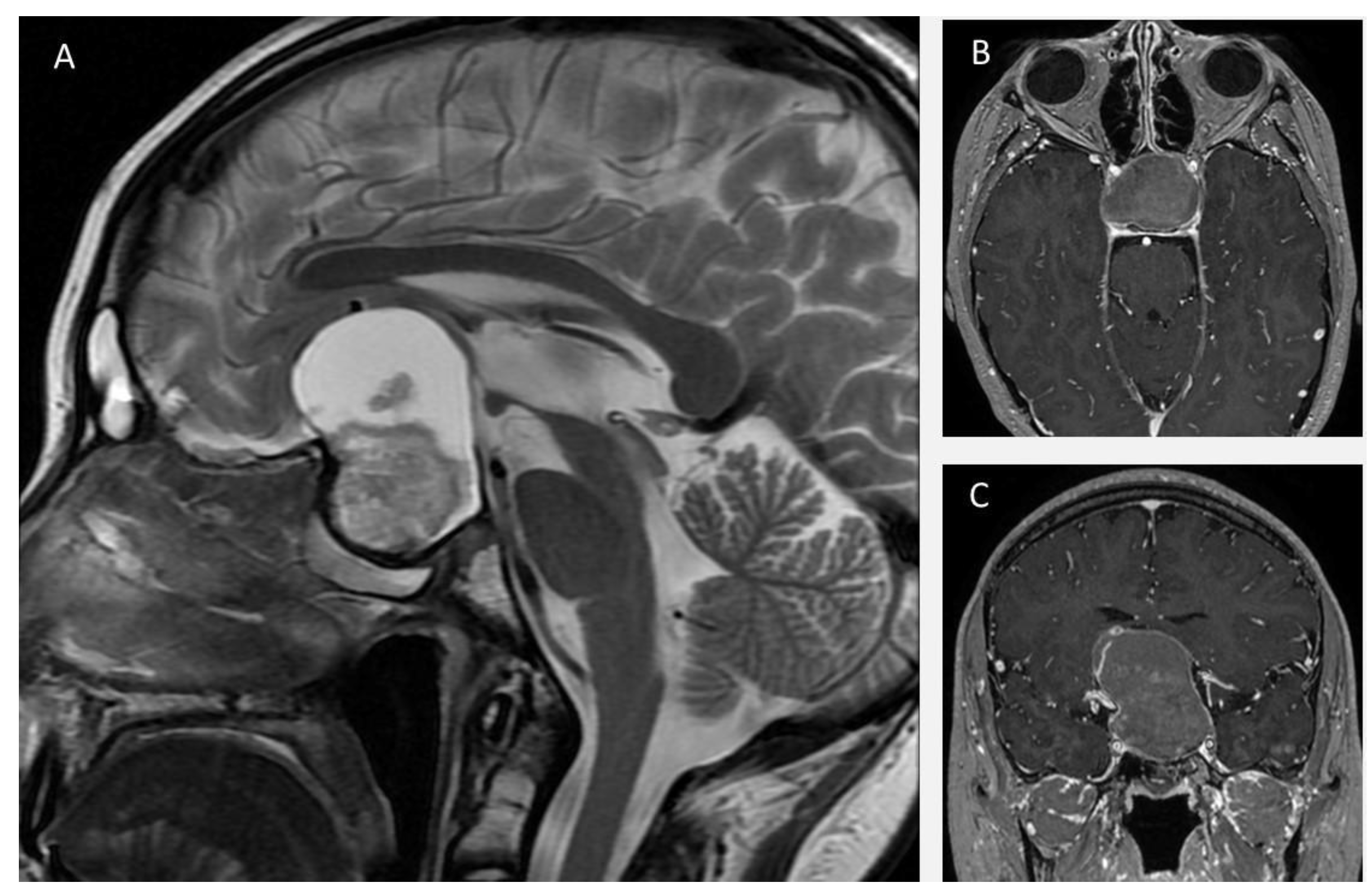
3.2. Representative Clinical Cases
3.2.1. Case 1
3.2.2. Case 2
3.2.3. Case 3
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Dahmani, K.; Mohammad, S.; Imran, F.; Theriault, C.; Doucette, S.; Zwicker, D.; Yip, C.E.; Clarke, D.B.; Imran, S.A. Sellar Masses: An Epidemiological Study. Can. J. Neurol. Sci. 2016, 43, 291–297. [Google Scholar] [CrossRef]
- Cavallo, L.M.; Somma, T.; Solari, D.; Iannuzzo, G.; Frio, F.; Baiano, C.; Cappabianca, P. Endoscopic Endonasal Transsphenoidal Surgery: History and Evolution. World Neurosurg. 2019, 127, 686–694. [Google Scholar] [CrossRef]
- Baldauf, J.; Hosemann, W.; Schroeder, H.W.S. Endoscopic Endonasal Approach for Craniopharyngiomas. Neurosurg. Clin. N. Am. 2015, 26, 363–375. [Google Scholar] [CrossRef]
- Liu, J.K.; Sevak, I.A.; Carmel, P.W.; Eloy, J.A. Microscopic versus endoscopic approaches for craniopharyngiomas: Choosing the optimal surgical corridor for maximizing extent of resection and complication avoidance using a personalized, tailored approach. Neurosurg. Focus 2016, 41, E5. [Google Scholar] [CrossRef]
- Jho, H.-D. Endoscopic transsphenoidal surgery. J. Neuro-Oncol. 2001, 54, 187–195. [Google Scholar] [CrossRef]
- Zador, Z.; Gnanalingham, K. Endoscopic Transnasal Approach to the Pituitary—Operative Technique and Nuances. Br. J. Neurosurg. 2013, 27, 718–726. [Google Scholar] [CrossRef]
- Youmans, J.R. Youmans and Winn Neurological Surgery; Winn, H.R., Ed.; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Hadad, G.; Bassagasteguy, L.; Carrau, R.L.; Mataza, J.C.; Kassam, A.; Snyderman, C.H.; Mintz, A. A Novel Reconstructive Technique after Endoscopic Expanded Endonasal Approaches: Vascular Pedicle Nasoseptal Flap. Laryngoscope 2006, 116, 1882–1886. [Google Scholar] [CrossRef]
- Kulwin, C.; Schwartz, T.H.; Cohen-Gadol, A.A. Endoscopic extended transsphenoidal resection of tuberculum sellae meningiomas: Nuances of neurosurgical technique. Neurosurg. Focus 2013, 35, E6. [Google Scholar] [CrossRef]
- Conger, A.R.; Lucas, J.; Zada, G.; Schwartz, T.H.; Cohen-Gadol, A.A. Endoscopic extended transsphenoidal resection of craniopharyngiomas: Nuances of neurosurgical technique. Neurosurg. Focus 2014, 37, E10. [Google Scholar] [CrossRef]
- Santos, R.D.P.; Zymberg, S.T.; Filho, J.Z.A.; Gregório, L.C.; Weckx, L.L.M. Endoscopic Transnasal Approach to Sellar Tumors. Braz. J. Otorhinolaryngol. 2007, 73, 463–475. [Google Scholar] [CrossRef]
- Leng, L.Z.; Brown, S.; Anand, V.K.; Schwartz, T.H. “Gasket-Seal” Watertight Closure in Minimal-Access Endoscopic Cranial Base Surgery. Oper. Neurosurg. 2008, 62, ONSE342–ONSE343. [Google Scholar] [CrossRef]
- Navarro, V.G.; Anand, V.K.; Schwartz, T.H. Gasket Seal Closure for Extended Endonasal Endoscopic Skull Base Surgery: Efficacy in a Large Case Series. World Neurosurg. 2013, 80, 563–568. [Google Scholar] [CrossRef]
- Scagnelli, R.J.; Patel, V.; Peris-Celda, M.; Kenning, T.J.; Pinheiro-Neto, C.D. Implementation of Free Mucosal Graft Technique for Sellar Reconstruction after Pituitary Surgery: Outcomes of 158 Consecutive Patients. World Neurosurg. 2019, 122, e506–e511. [Google Scholar] [CrossRef]
- Komotar, R.J.; Starke, R.M.; Raper, D.M.; Anand, V.K.; Schwartz, T.H. Endoscopic Endonasal Compared with Microscopic Transsphenoidal and Open Transcranial Resection of Craniopharyngiomas. World Neurosurg. 2012, 77, 329–341. [Google Scholar] [CrossRef]
- Cavallo, L.M.; Prevedello, D.M.; Solari, D.; Gardner, P.A.; Esposito, F.; Snyderman, C.H.; Carrau, R.L.; Kassam, A.B.; Cappabianca, P. Extended endoscopic endonasal transsphenoidal approach for residual or recurrent craniopharyngiomas. J. Neurosurg. 2009, 111, 578–589. [Google Scholar] [CrossRef]
- Kassam, A.B.; Gardner, P.A.; Snyderman, C.H.; Carrau, R.L.; Mintz, A.H.; Prevedello, D.M. Expanded endonasal approach, a fully endoscopic transnasal approach for the resection of midline suprasellar craniopharyngiomas: A new classification based on the infundibulum. J. Neurosurg. 2008, 108, 715–728. [Google Scholar] [CrossRef]
- Tang, B.; Xie, S.H.; Xiao, L.M.; Huang, G.L.; Wang, Z.G.; Yang, L.; Yang, X.Y.; Xu, S.; Chen, Y.Y.; Ji, Y.Q.; et al. A Novel Endoscopic Classification for Craniopharyngioma Based on Its Origin. Sci. Rep. 2018, 8, 10215. [Google Scholar] [CrossRef]
- Na, M.K.; Jang, B.; Choi, K.S.; Lim, T.H.; Kim, W.; Cho, Y.; Shin, H.G.; Ahn, C.; Kim, J.G.; Lee, J.; et al. Craniopharyngioma resection by endoscopic endonasal approach versus transcranial approach: A systematic review and meta-analysis of comparative studies. Front. Oncol. 2022, 12, 1058329. [Google Scholar] [CrossRef]
- Lei, C.; Chuzhong, L.; Chunhui, L.; Peng, Z.; Jiwei, B.; Xinsheng, W.; Yazhuo, Z.; Songbai, G. Approach selection and outcomes of craniopharyngioma resection: A single-institute study. Neurosurg. Rev. 2021, 44, 1737–1746. [Google Scholar] [CrossRef]
- Liu, J.K.; Eloy, J.A. Endoscopic endonasal transplanum transtuberculum approach for resection of retrochiasmatic craniopharyngioma. Neurosurg. Focus 2012, 32, E2. [Google Scholar] [CrossRef]
- de Divitiis, E.; Cavallo, L.M.; Cappabianca, P.; Esposito, F. Extended endoscopic endonasal transsphenoidal approach for the removal of suprasellar tumors: Part 2. Neurosurgery 2007, 60, 46–59. [Google Scholar] [CrossRef]
- Hannan, C.J.; Almhanedi, H.; Al-Mahfoudh, R.; Bhojak, M.; Looby, S.; Javadpour, M. Predicting post-operative cerebrospinal fluid (CSF) leak following endoscopic transnasal pituitary and anterior skull base surgery: A multivariate analysis. Acta Neurochir. 2020, 162, 1309–1315. [Google Scholar] [CrossRef]
- Soudry, E.; Turner, J.H.; Nayak, J.V.; Hwang, P.H. Endoscopic reconstruction of surgically created skull base defects: A systematic review. Otolaryngol. Head Neck Surg. 2014, 150, 730–738. [Google Scholar] [CrossRef]
- Azab, W.A.; Abdelnabi, E.A.; Mostafa, K.H.; Burhamah, T.A.; Alhaj, A.K.H.; Khalil, A.M.B.; Yousef, W.; Nasim, K. Effect of Sphenoid Sinus Pneumatization on the Surgical Windows for Extended Endoscopic Endonasal Transsphenoidal Surgery. World Neurosurg. 2020, 133, e695–e701. [Google Scholar] [CrossRef]
- Nie, C.; Ye, Y.; Wu, J.; Zhao, H.; Jiang, X.; Wang, H. Clinical Outcomes of Transcranial and Endoscopic Endonasal Surgery for Craniopharyngiomas: A Single-Institution Experience. Front. Oncol. 2022, 12, 755342. [Google Scholar] [CrossRef]
- Snyderman, C.; Kassam, A.; Carrau, R.; Mintz, A.; Gardner, P.; Prevedello, D.M. Acquisition of surgical skills for endonasal skull base surgery: A training program. Laryngoscope 2007, 117, 699–705. [Google Scholar] [CrossRef]
- Lavigne, P.; Faden, D.; Gardner, P.A.; Fernandez-Miranda, J.C.; Wang, E.W.; Snyderman, C.H. Validation of training levels in endoscopic endonasal surgery of the skull base. Laryngoscope 2019, 129, 2253–2257. [Google Scholar] [CrossRef]
- Cavallo, L.M.; Solari, D.; Esposito, F.; Cappabianca, P. The endoscopic endonasal approach for the management of craniopharyngiomas involving the third ventricle. Neurosurg. Rev. 2013, 36, 27–38. [Google Scholar] [CrossRef]
- Kassam, A.B.; Prevedello, D.M.; Carrau, R.L.; Snyderman, C.H.; Thomas, A.; Gardner, P.; Zanation, A.; Duz, B.; Stefko, S.T.; Byers, K.; et al. Endoscopic endonasal skull base surgery: Analysis of complications in the authors’ initial 800 patients. J. Neurosurg. 2011, 114, 1544–1568. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modified Level of Complexity in Endoscopic Endonasal Surgery | ||
|---|---|---|
| Level | Compartment | Pathology |
| I | Extradural | CSF leak Chordoma Carcinoma |
| II | Pituitary fossa | Pituitary adenoma Craniopharyngioma |
| III | Anterior skull base floor | Meningioma Esthesioneuroblastoma Fibrous displasia |
| IV | Orbit Pterygo-pallatine fossa Maxillary sinus | Trigeminal Schwannoma |
| V | Cisterns Interpeduncular fossa Clivus | Craniopharyngioma Chordoma Pituitary adenoma |
| VI | Cavernous sinus | Pituitary adenoma Hemangioblastoma Meningioma |
| VII | Vascular | Paraclinoid aneurysm ACo aneurysm Basilar aneurysm Vertebral aneurysm |
| VIII | Intrinsic | Cavernoma Metastasis Glioma |
| Categories of Technical Complexity and Surgical Expertise of Endoscopic Endonasal Approaches for Craniopharyngiomas | ||
|---|---|---|
| Category | Tumor Location/ Extension | Technical Nuances |
| A | Intrasellar/infradiaphragmatic | Anatomic relationships similar to that of pituitary adenomas. The sellar floor is enlarged providing enough space for resection and, thus, facilitating the approach. |
| B | Intra-suprasellar/infradiaphragmatic | Neurovascular structures in the suprasellar side of the tumor protected by the diaphragm. Sufficient space between pituitary gland and the optic chiasm for tumor resection. |
| C | Suprasellar/preinfundibular or transinfundibular | An extended endoscopic endonasal approach is required. Size of the sella is often normal or reduced, resulting in a narrower approach due to closeness of the two intracavernous carotids. Arteries of the circle of Willis are often displaced by the suprasellar mass. |
| D | Suprasellar/retroinfundibular | Requires a more posterior approach. Stretch relationship with important neurovascular structures such as the mammillary bodies and basilar apex. Requires a pituitary transposition, increasing the technical complexity of the approach. |
| E | Arising or extending into the third ventricle | Risk of injury to the hypothalamus, brainstem, and other important neurovascular structures. Increased risk for CSF fistula due to communication of the ventricular cavity with the sphenoid sinus. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aragón-Arreola, J.F.; Marian-Magaña, R.; Villalobos-Diaz, R.; López-Valencia, G.; Jimenez-Molina, T.M.; Moncada-Habib, J.T.; Sangrador-Deitos, M.V.; Gómez-Amador, J.L. Endoscopic Endonasal Approach in Craniopharyngiomas: Representative Cases and Technical Nuances for the Young Neurosurgeon. Brain Sci. 2023, 13, 735. https://doi.org/10.3390/brainsci13050735
Aragón-Arreola JF, Marian-Magaña R, Villalobos-Diaz R, López-Valencia G, Jimenez-Molina TM, Moncada-Habib JT, Sangrador-Deitos MV, Gómez-Amador JL. Endoscopic Endonasal Approach in Craniopharyngiomas: Representative Cases and Technical Nuances for the Young Neurosurgeon. Brain Sciences. 2023; 13(5):735. https://doi.org/10.3390/brainsci13050735
Chicago/Turabian StyleAragón-Arreola, Jorge F., Ricardo Marian-Magaña, Rodolfo Villalobos-Diaz, Germán López-Valencia, Tania M. Jimenez-Molina, J. Tomás Moncada-Habib, Marcos V. Sangrador-Deitos, and Juan L. Gómez-Amador. 2023. "Endoscopic Endonasal Approach in Craniopharyngiomas: Representative Cases and Technical Nuances for the Young Neurosurgeon" Brain Sciences 13, no. 5: 735. https://doi.org/10.3390/brainsci13050735