
Effects of Multidisciplinary Rehabilitation Enhanced with Neuropsychological Treatment on Post-Acute SARS-CoV-2 Cognitive Impairment (Brain Fog): An Observational Study
 , , , ,
, , , ,
Abstract
:1. Background
2. Methods
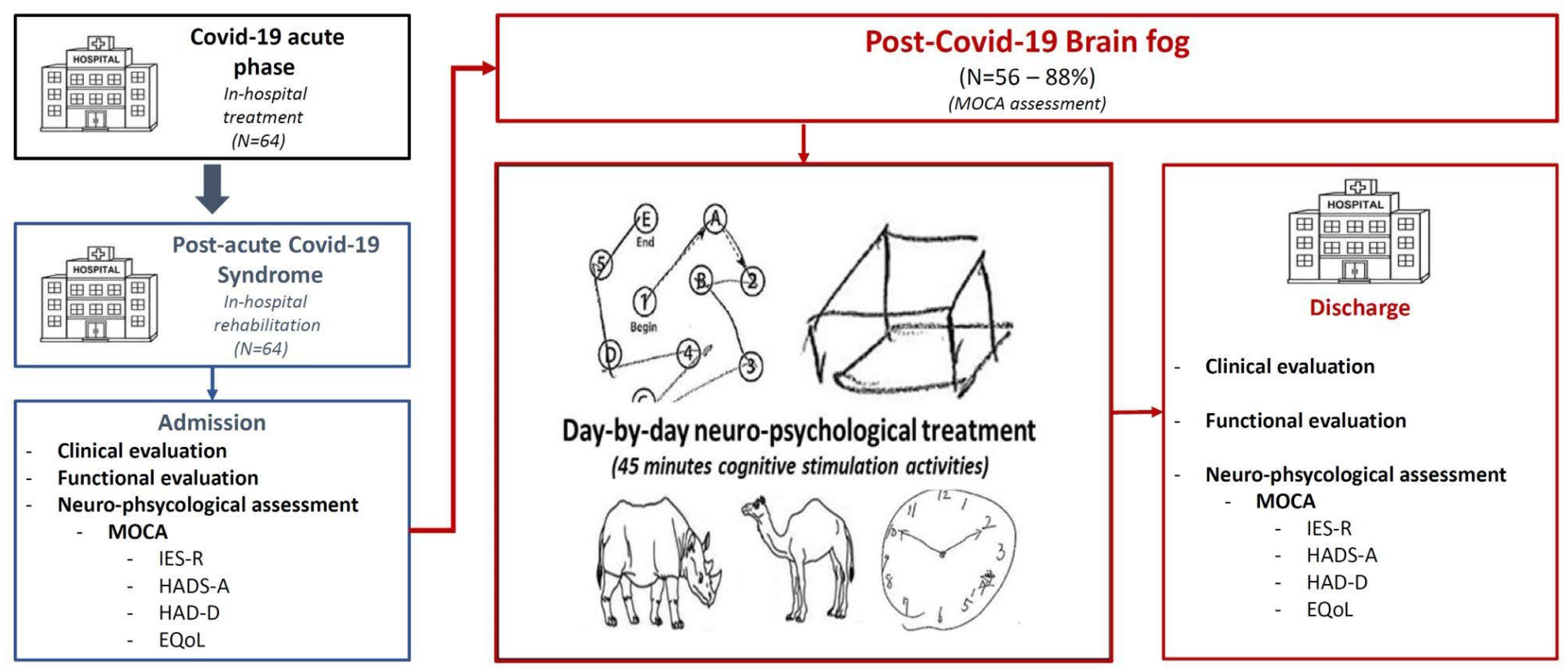
2.1. Neurocognitive Evaluation and Rehabilitation Program
2.1.1. Physiotherapy Rehabilitation Program
2.1.2. Psychological Rehabilitation Program
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
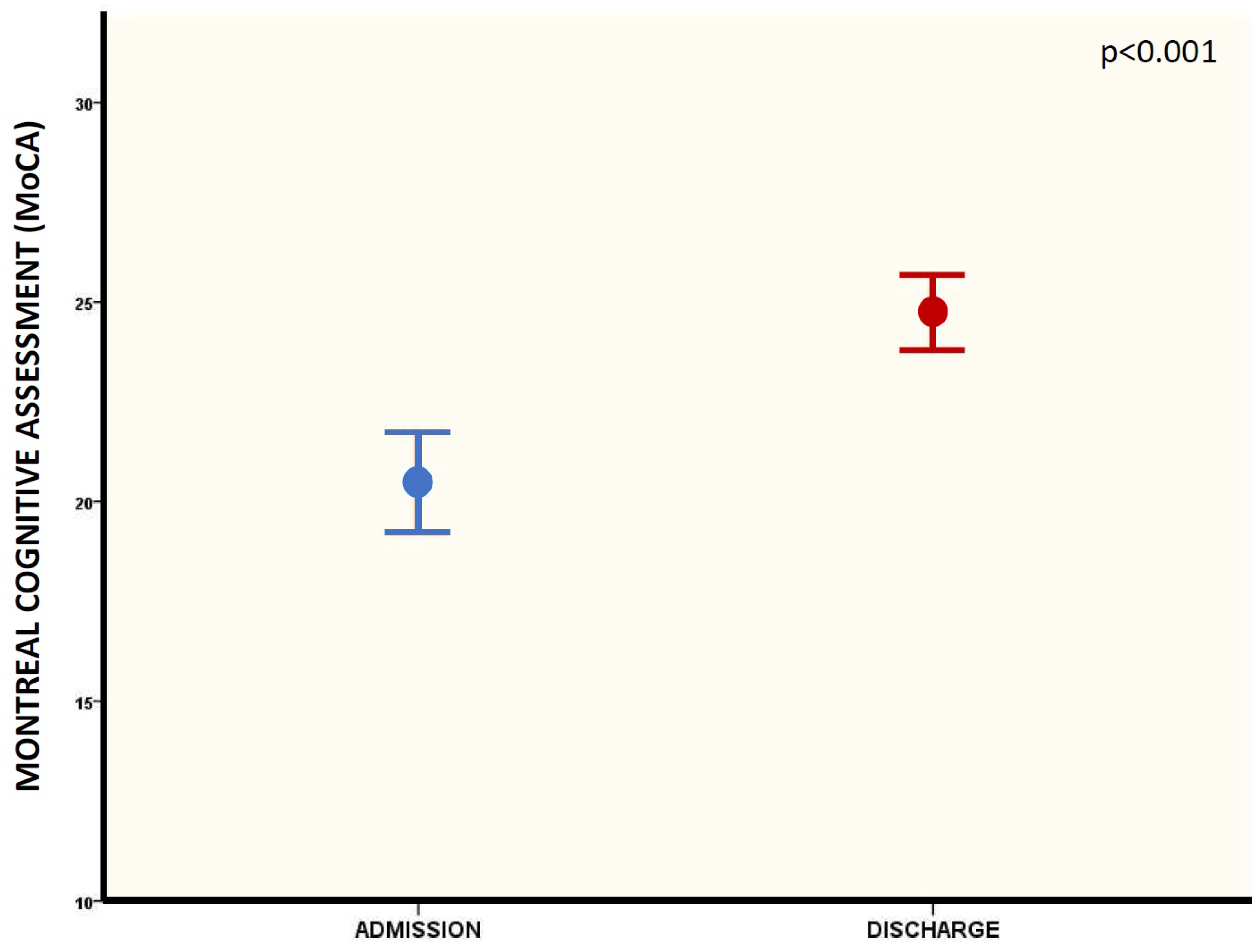
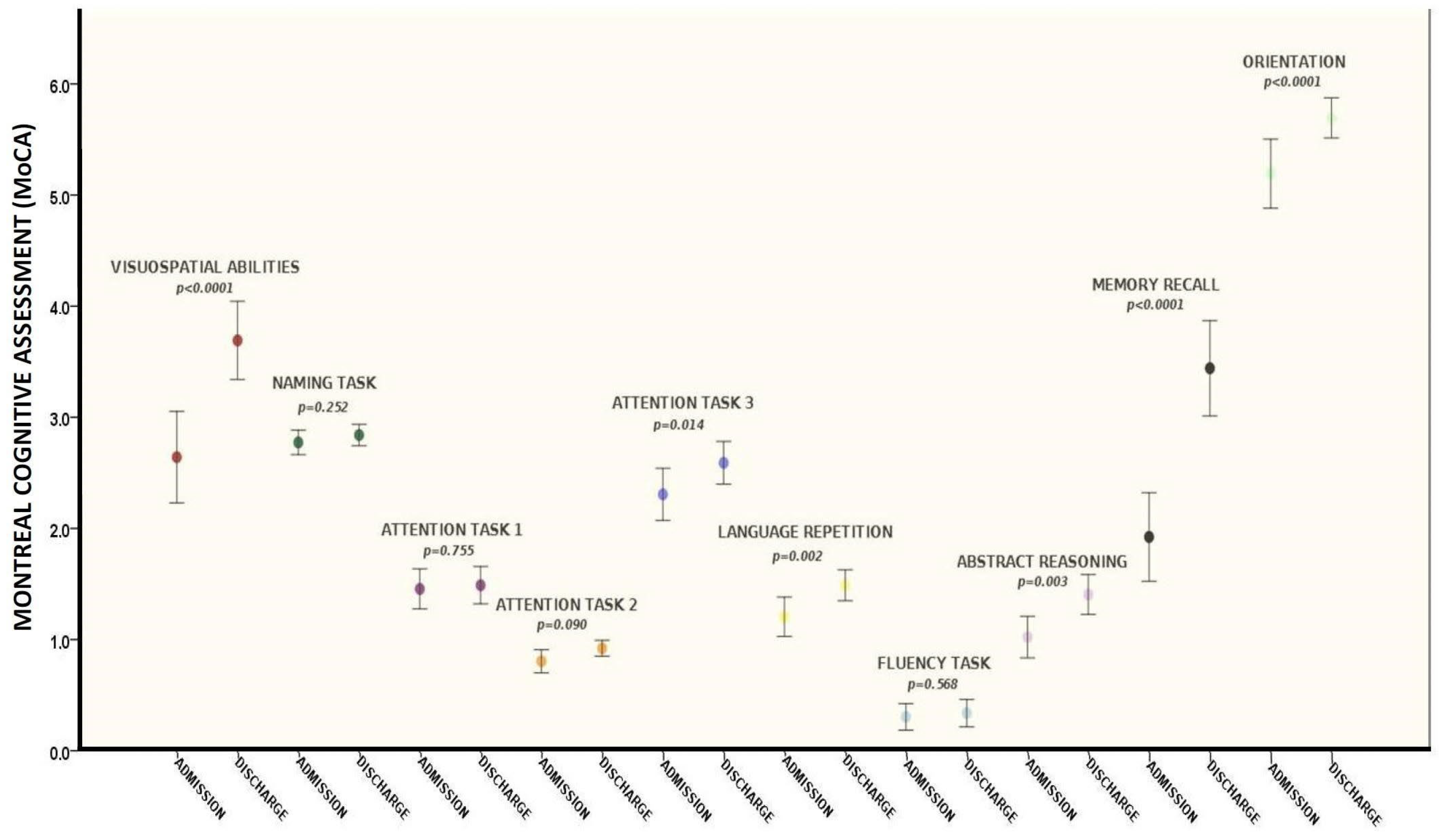
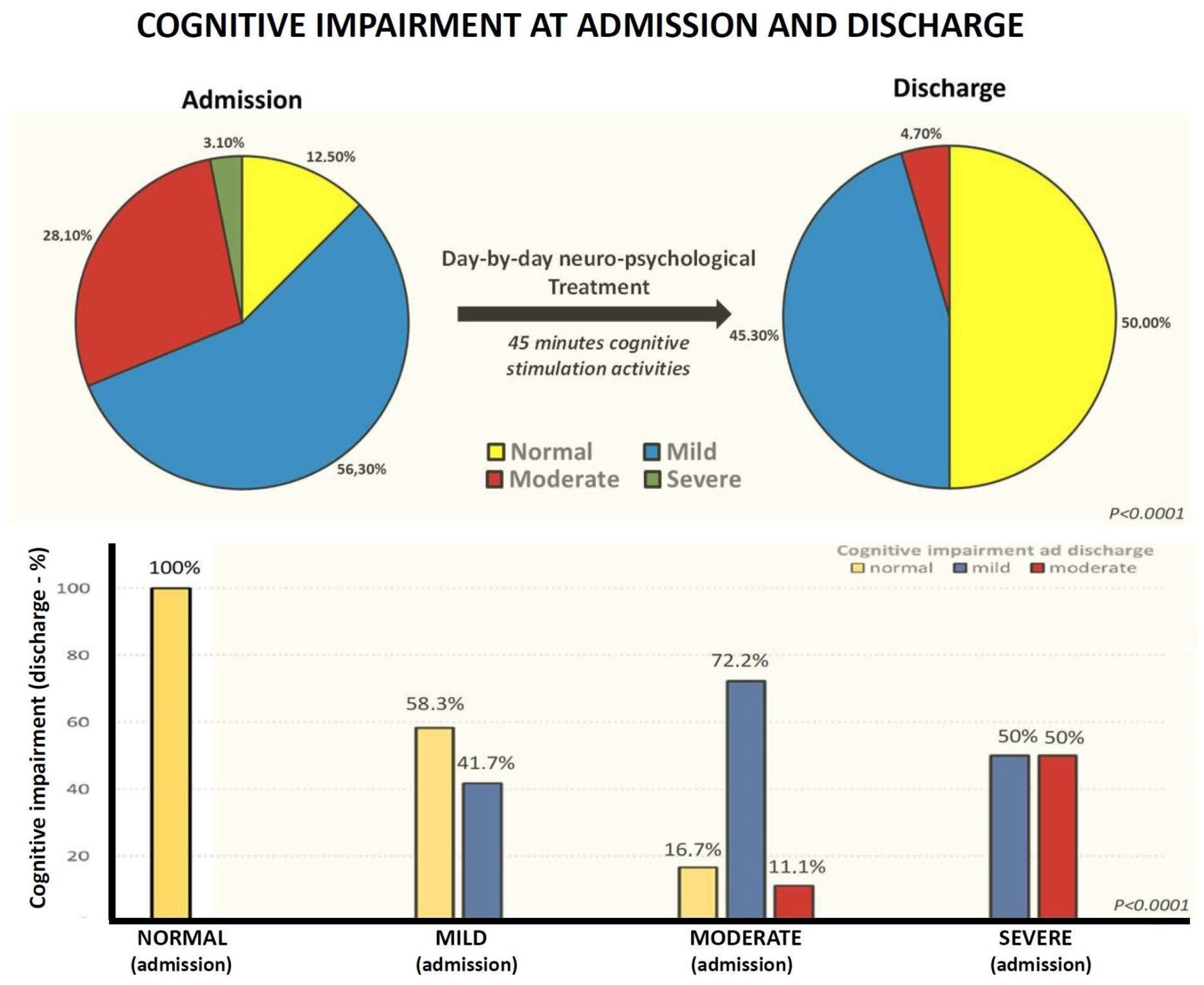
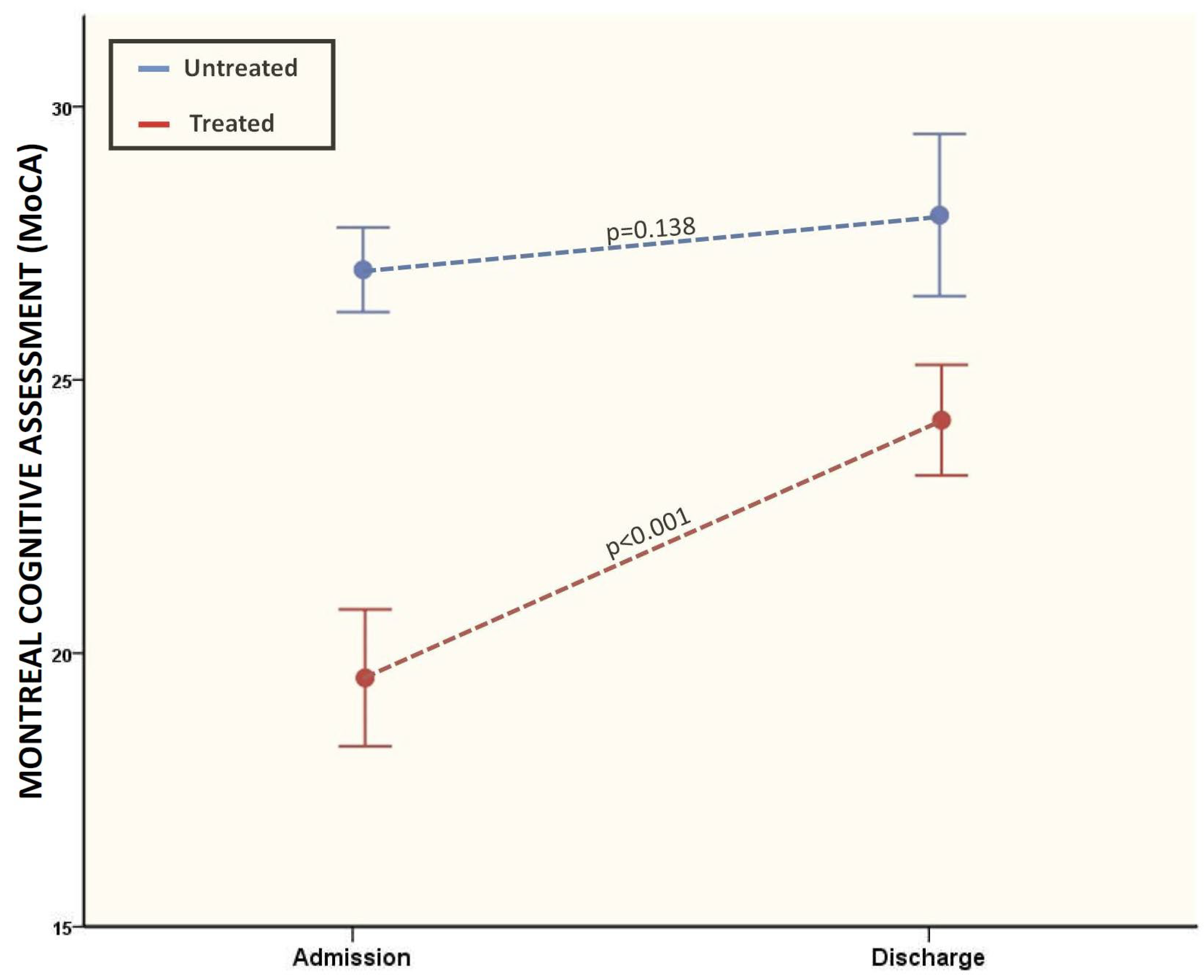
3.2. Cognitive Evaluations between Admission and Discharge (Pre- and Post-Treatment)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical Sequelae of COVID-19 Survivors in Wuhan, China: A Single-Centre Longitudinal Study. Clin. Microbiol. Infect. 2021, 27, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, P.; Granath, F.; Bruchfeld, J.; Askling, J.; Sjöholm, D.; Fored, M.; Färnert, A.; Naucler, P. Post COVID-19 Condition Diagnosis: A Population-Based Cohort Study of Occurrence, Associated Factors, and Healthcare Use by Severity of Acute Infection. J. Intern. Med. 2023, 293, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. WHO Clinical Case Definition Working Group on Post-COVID-19 Condition A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Khunti, K.; Nafilyan, V.; Maddox, T.; Humberstone, B.; Diamond, I.; Banerjee, A. Post-Covid Syndrome in Individuals Admitted to Hospital with COVID-19: Retrospective Cohort Study. BMJ 2021, 372, n693. [Google Scholar] [CrossRef] [PubMed]
- Hugon, J.; Msika, E.-F.; Queneau, M.; Farid, K.; Paquet, C. Long COVID: Cognitive Complaints (brain Fog) and Dysfunction of the Cingulate Cortex. J. Neurol. 2022, 269, 44–46. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Long COVID Syndrome-Associated Brain Fog. J. Med. Virol. 2022, 94, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Sia, A.L.-S.; Neo, J.E.; Jen-Wei Tan, B.; Tan, E.-K. “Brain Fog” and COVID-19. Am. J. Med. Sci. 2023, 365, 472–474. [Google Scholar] [CrossRef]
- Fernández-Castañeda, A.; Lu, P.; Geraghty, A.C.; Song, E.; Lee, M.-H.; Wood, J.; O’Dea, M.R.; Dutton, S.; Shamardani, K.; Nwangwu, K.; et al. Mild Respiratory COVID Can Cause Multi-Lineage Neural Cell and Myelin Dysregulation. Cell 2022, 185, 2452–2468.e16. [Google Scholar] [CrossRef]
- Gibson, E.M.; Nagaraja, S.; Ocampo, A.; Tam, L.T.; Wood, L.S.; Pallegar, P.N.; Greene, J.J.; Geraghty, A.C.; Goldstein, A.K.; Ni, L.; et al. Methotrexate Chemotherapy Induces Persistent Tri-Glial Dysregulation That Underlies Chemotherapy-Related Cognitive Impairment. Cell 2019, 176, 43–55.e13. [Google Scholar] [CrossRef]
- Manly, J.J.; Tang, M.-X.; Schupf, N.; Stern, Y.; Vonsattel, J.-P.G.; Mayeux, R. Frequency and Course of Mild Cognitive Impairment in a Multiethnic Community. Ann. Neurol. 2008, 63, 494–506. [Google Scholar] [CrossRef]
- Creamer, M.; Bell, R.; Failla, S. Psychometric Properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Lee, W.Y.; Basri, N.A.; Collinson, S.L.; Merchant, R.A.; Venketasubramanian, N.; Chen, C.L.-H. The Montreal Cognitive Assessment Is Superior to the Mini-Mental State Examination in Detecting Patients at Higher Risk of Dementia. Int. Psychogeriatr. 2012, 24, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Centorbi, C.S.; Garau, E.; Borsi, L.; Brambilla, V.; Brambilla, L.; Lazzeroni, D. Cardiovascular Post-Acute COVID-19 Syndrome: Definition, Clinical Scenarios, Diagnosis, and Management. In New Insights on Cardiomyopathy; IntechOpen: London, UK, 2022. [Google Scholar]
- Moderato, L.; Monello, A.; Lazzeroni, D.; Binno, S.; Giacalone, R.; Ferraro, S.; Piepoli, M.F.; Villani, G.Q. Takotsubo syndrome during SARS-CoV-2 pneumonia: A possible cardiovascular complication. G. Ital. Cardiol. 2020, 21, 417–420. [Google Scholar]
- Lazzeroni, D.; Concari, P.; Moderato, L. Simultaneous COVID-19 in Monozygotic Twins. Ann. Intern. Med. 2021, 174, 717–719. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major Findings, Mechanisms and Recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Oronsky, B.; Larson, C.; Hammond, T.C.; Oronsky, A.; Kesari, S.; Lybeck, M.; Reid, T.R. A Review of Persistent Post-COVID Syndrome (PPCS). Clin. Rev. Allergy Immunol. 2023, 64, 66–74. [Google Scholar] [CrossRef]
- Kopańska, M.; Ochojska, D.; Muchacka, R.; Dejnowicz-Velitchkov, A.; Banaś-Ząbczyk, A.; Szczygielski, J. Comparison of QEEG Findings before and after Onset of Post-COVID-19 Brain Fog Symptoms. Sensors 2022, 22, 6606. [Google Scholar] [CrossRef]
- Hugon, J. Long-COVID: Cognitive Deficits (brain Fog) and Brain Lesions in Non-Hospitalized Patients. Presse Med. 2022, 51, 104090. [Google Scholar] [CrossRef]
- Callan, C.; Ladds, E.; Husain, L.; Pattinson, K.; Greenhalgh, T. I Can’t Cope with Multiple Inputs’: A Qualitative Study of the Lived Experience of “Brain Fog” after COVID-19. BMJ Open 2022, 12, e056366. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; et al. SARS-CoV-2 Is Associated with Changes in Brain Structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Rodríguez-Jiménez, J.; Palacios-Ceña, M.; de-la-Llave-Rincón, A.I.; Fuensalida-Novo, S.; Florencio, L.L.; Ambite-Quesada, S.; Ortega-Santiago, R.; Arias-Buría, J.L.; Liew, B.X.W.; et al. Psychometric Properties of the Hospital Anxiety and Depression Scale (HADS) in Previously Hospitalized COVID-19 Patients. Int. J. Environ. Res. Public Health 2022, 19, 9273. [Google Scholar] [CrossRef] [PubMed]
- Tomasoni, D.; Bai, F.; Castoldi, R.; Barbanotti, D.; Falcinella, C.; Mulè, G.; Mondatore, D.; Tavelli, A.; Vegni, E.; Marchetti, G.; et al. Anxiety and Depression Symptoms after Virological Clearance of COVID-19: A Cross-Sectional Study in Milan, Italy. J. Med. Virol. 2021, 93, 1175–1179. [Google Scholar] [CrossRef]
- Aljaberi, M.A.; Lee, K.-H.; Alareqe, N.A.; Qasem, M.A.; Alsalahi, A.; Abdallah, A.M.; Noman, S.; Al-Tammemi, A.B.; Mohamed Ibrahim, M.I.; Lin, C.-Y. Rasch Modeling and Multilevel Confirmatory Factor Analysis for the Usability of the Impact of Event Scale-Revised (IES-R) during the COVID-19 Pandemic. Healthcare 2022, 10, 1858. [Google Scholar] [CrossRef] [PubMed]
- Alemanno, F.; Houdayer, E.; Parma, A.; Spina, A.; Del Forno, A.; Scatolini, A.; Angelone, S.; Brugliera, L.; Tettamanti, A.; Beretta, L.; et al. COVID-19 Cognitive Deficits after Respiratory Assistance in the Subacute Phase: A COVID-Rehabilitation Unit Experience. PLoS ONE 2021, 16, e0246590. [Google Scholar] [CrossRef] [PubMed]
- Albu, S.; Rivas Zozaya, N.; Murillo, N.; García-Molina, A.; Figueroa Chacón, C.A.; Kumru, H. Multidisciplinary Outpatient Rehabilitation of Physical and Neurological Sequelae and Persistent Symptoms of COVID-19: A Prospective, Observational Cohort Study. Disabil. Rehabil. 2022, 44, 6833–6840. [Google Scholar] [CrossRef]
- Prestia, A.; Caroli, A.; van der Flier, W.M.; Ossenkoppele, R.; Van Berckel, B.; Barkhof, F.; Teunissen, C.E.; Wall, A.E.; Carter, S.F.; Schöll, M.; et al. Prediction of Dementia in MCI Patients Based on Core Diagnostic Markers for Alzheimer Disease. Neurology 2013, 80, 1048–1056. [Google Scholar] [CrossRef]
- Handels, R.L.H.; Vos, S.J.B.; Kramberger, M.G.; Jelic, V.; Blennow, K.; van Buchem, M.; van der Flier, W.; Freund-Levi, Y.; Hampel, H.; Olde Rikkert, M.; et al. Predicting Progression to Dementia in Persons with Mild Cognitive Impairment Using Cerebrospinal Fluid Markers. Alzheimers. Dement. 2017, 13, 903–912. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal 8 (12.5) | Mild Cognitive Impairment 36 (56.3) | Moderate Cognitive Impairment 18 (28.1) | Severe Cognitive Impairment 2 (3.1) | p | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age (years), M (SD) | 61.6 (12.9) | 65.7 (8.8) | 72.2 (10.8) | 76.5 (2.1) | 0.030 * |
| Gender (male), N (%) | 0 (0) | 12 (33.3) | 9 (50) | 1 (50) | 0.095 |
| CV risk factors | |||||
| Hypertension, N (%) | 6 (75) | 26 (72.2) | 12 (66.6) | 1 (50) | 0.883 |
| Dyslipidemia, N (%) | 1 (12.5) | 6 (16.7) | 8 (44.4) | 2 (100) | 0.011 * |
| Active smokers, N (%) | 0 (0) | 10 (27.8) | 3 (16.6) | 1 (50) | 0.110 |
| Diabetes, N (%) | 1 (12.5) | 8 (22.3) | 3 (16.6) | 1 (50) | 0.655 |
| Comorbidities | |||||
| Cardiovascular, N (%) | 0 (0) | 12 (33.3) | 9 (50) | 2 (100) | 0.021 * |
| COPD, N (%) | 1 (12.5) | 0 (0) | 3 (16.6) | 2 (100) | <0.001 * |
| Renal, N (%) | 0 (0) | 4 (11.1) | 0 (0) | 0 (0) | 0.345 |
| Neurological, N (%) | 0 (0) | 1 (2.8) | 3 (16.6) | 0 (0) | 0.192 |
| Psychiatric, N (%) | 0 (0) | 3 (8.3) | 2 (11.1) | 0 (0) | 0.769 |
| Gastrointestinal, N (%) | 1 (12.5) | 9 (25) | 3 (16.6) | 1 (50) | 0.609 |
| Oncological, N (%) | 0 (0) | 3 (8.3) | 2 (11.1) | 0 (0) | 0.769 |
| Normal 8 (12.5) | Mild Cognitive Impairment 36 (56.3) | Moderate Cognitive Impairment 18 (28.1) | Severe Cognitive Impairment 2 (3.1) | p | |
|---|---|---|---|---|---|
| Hospitalization (ACUTE PHASE) | |||||
| Days, M (SD) | 72.3 (28.8) | 53.9 (23.5) | 54 (28.3) | 40 (14.1) | 0.232 |
| Severe infection, N (%) | 7 (10.9) | 23 (35.9) | 10 (15.6) | 2 (3.1) | 0.308 |
| Mechanical ventilation, N (%) | 7 (10.9) | 21 (33) | 11 (17) | 1 (2) | 0.393 |
| Rehabilitation (POST-ACUTE PHASE) Admission Clinical data | |||||
| SBP (mmHg), M (SD) | 123.5 (14.3) | 125.5 (20.9) | 132.6 (17.3) | 100 (0) | 0.134 |
| DBP (mmHg), M (SD) | 79.2 (13) | 73.1 (8.1) | 76.4 (10.5) | 55.1 (7) | 0.014 * |
| HR (bpm), M (SD) | 80.1 (12.8) | 80.6 (12.7) | 89.61 (16.5) | 72 (8.4) | 0.092 |
| SatO2 (%), M (SD) | 97 (2.3) | 96 (4.1) | 96.6 (1.8) | 99 (1.4) | 0.617 |
| O2 therapy, N (%) | 4 (7.1) | 28 (42.8) | 23 (35.7) | 4 (7.1) | 0.783 |
| Laboratory data | |||||
| Hb (g/dL), M (SD) | 10.0 (3.76) | 9.7 (4.1) | 8.7 (5) | 7.3 (8.9 | 0.752 |
| WBC (×103), M (SD) | 6.8 (1.1) | 7.1 (2.6) | 9.3 (4.4) | 7.8 (0.9) | 0.111 |
| RBC (×106), M (SD) | 3.7 (0.5) | 3.9 (0.4) | 3.9 (0.5) | 3.7 (0.7) | 0.693 |
| RDW, M (SD) | 14.7 (1.5) | 16.3 (3.3) | 15.5 (1.3) | 15.7 (2) | 0.480 |
| PLT (×103), M (SD) | 282 (84) | 270.5 (129.4) | 270.7 (89.5) | 224 (28.2) | 0.936 |
| Creatinine (mg/dL), M (SD) | 0.66 (0.2) | 0.68 (0.24) | 0.62 (0.15) | 0.41 (0.26) | 0.367 |
| CRP (mg/dL), M (SD) | 1.6 (2.7) | 2.4 (4.3) | 2.4 (3.3) | 3.1 (1.02) | 0.944 |
| ESR (mm/h), M (SD) | 25 | 26.2 (20.5) | 52 (27.2) | 0 (0) | 0.178 |
| D-dimer, M (SD) | 543 | 1006 (866) | 517 (600) | 0 (0) | 0.549 |
| COVID-19 therapy | |||||
| Steroids, N (%) | 7 (10.9) | 30 (46.9) | 15 (23.4) | 2 (3.1) | 0.925 |
| Beta blockers, N (%) | 4 (6.2) | 14 (21.8) | 10 (15.6) | 0 (0) | 0.384 |
| ACEi/ARBs, N (%) | 1 (1.56) | 7 (10.9) | 3 (4.6) | 1 (1.56) | 0.671 |
| ASA, N (%) | 2 (3.1) | 1 (1.56) | 3 (4.6) | 1 (1.56) | 0.050 |
| Antiviral, N (%) | 1 (1.56) | 6 (9.3) | 3 (4.6) | 0 (0) | 0.925 |
| LMWH, N (%) | 8 (12.5) | 37 (57.8) | 16 (25.0) | 2 (3.1) | 0.192 |
| Statins, N (%) | 1 (1.56) | 0 (0) | 3 (4.6) | 1 (1.56) | 0.017 * |
| O2, N (%) | 5 (7.14) | 27 (42) | 23 (35) | 5 (7.14) | 0.783 |
| Antidepressant, N (%) | 4 (6.2) | 9 (14) | 10 (16) | 1 (2) | 0.068 |
| Opioids, N (%) | 0 (0) | 1 (2.8) | 3 (16.7) | 0 (0) | 0.192 |
| Neuroleptics and BDZ, N (%) | 1 (12.5) | 11 (30.6) | 6 (33.3) | 2 (100) | 0.124 |
| Antibiotics, N (%) | 7 (10.9) | 27 (42.1) | 12 (18.7) | 2 (3.1) | 0.572 |
| Admission, M (SD) | Discharge, M (SD) | p | |
|---|---|---|---|
| MoCA overall | 20.4 (5) | 24.7 (3.7) | <0.0001 * |
| Attention task 1 | 1.4 (0.6) | 1.4 (0.6) | 0.755 |
| Attention task 2 | 0.8 (0.4) | 0.9 (0.2) | 0.090 |
| Attention task 3 | 2.3 (0.9) | 2.5 (0.7) | 0.014 |
| Fluency task | 0.3 (0.4) | 0.33 (0.47) | 0.568 |
| Language repetition | 1.2 (0.6) | 1.4 (0.5) | 0.002 |
| Memory recall | 1.9 (1.5) | 3.4 (1.6) | <0.0001 * |
| Naming task | 2.7 (0.4) | 2.8 (0.3) | 0.252 |
| Orientation | 5.1 (1.2) | 5.6 (0.7) | <0.0001 * |
| Visuo-spatial abilities | 2.6 (1.5) | 3.6 (1.3) | <0.0001 * |
| Abstract reasoning | 1.02 (0.7) | 1.4 (0.7) | 0.003 |
| Admission, M (SD) | Discharge, M (SD) | p | |
|---|---|---|---|
| MoCA overall | 20.4 (5) | 24.7 (3.7) | <0.0001 * |
| EQoL | 55.3 (21.1) | 66.1 (19) | 0.268 |
| IES-R score | 19.6 (15.6) | 15.5 (11.7) | 0.063 |
| Barthel index | 47.8 (18.4) | 83.5 (19.4) | <0.0001 * |
| HADS-A | 4.4 (3.3) | 4.1 (3.3) | 0.351 |
| HADS-D | 3.7 (3) | 3 (2.7) | 0.074 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabaiotti, P.; Ciracì, C.; Donelli, D.; Oggioni, C.; Rizzi, B.; Savi, F.; Antonelli, M.; Rizzato, M.; Moderato, L.; Brambilla, V.; et al. Effects of Multidisciplinary Rehabilitation Enhanced with Neuropsychological Treatment on Post-Acute SARS-CoV-2 Cognitive Impairment (Brain Fog): An Observational Study. Brain Sci. 2023, 13, 791. https://doi.org/10.3390/brainsci13050791
Rabaiotti P, Ciracì C, Donelli D, Oggioni C, Rizzi B, Savi F, Antonelli M, Rizzato M, Moderato L, Brambilla V, et al. Effects of Multidisciplinary Rehabilitation Enhanced with Neuropsychological Treatment on Post-Acute SARS-CoV-2 Cognitive Impairment (Brain Fog): An Observational Study. Brain Sciences. 2023; 13(5):791. https://doi.org/10.3390/brainsci13050791
Chicago/Turabian StyleRabaiotti, Paolo, Chiara Ciracì, Davide Donelli, Carlotta Oggioni, Beatrice Rizzi, Federica Savi, Michele Antonelli, Matteo Rizzato, Luca Moderato, Valerio Brambilla, and et al. 2023. "Effects of Multidisciplinary Rehabilitation Enhanced with Neuropsychological Treatment on Post-Acute SARS-CoV-2 Cognitive Impairment (Brain Fog): An Observational Study" Brain Sciences 13, no. 5: 791. https://doi.org/10.3390/brainsci13050791