
Group Cognitive Behavioural Therapy for Non-Rapid Eye Movement Parasomnias: Long-Term Outcomes and Impact of COVID-19 Lockdown


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
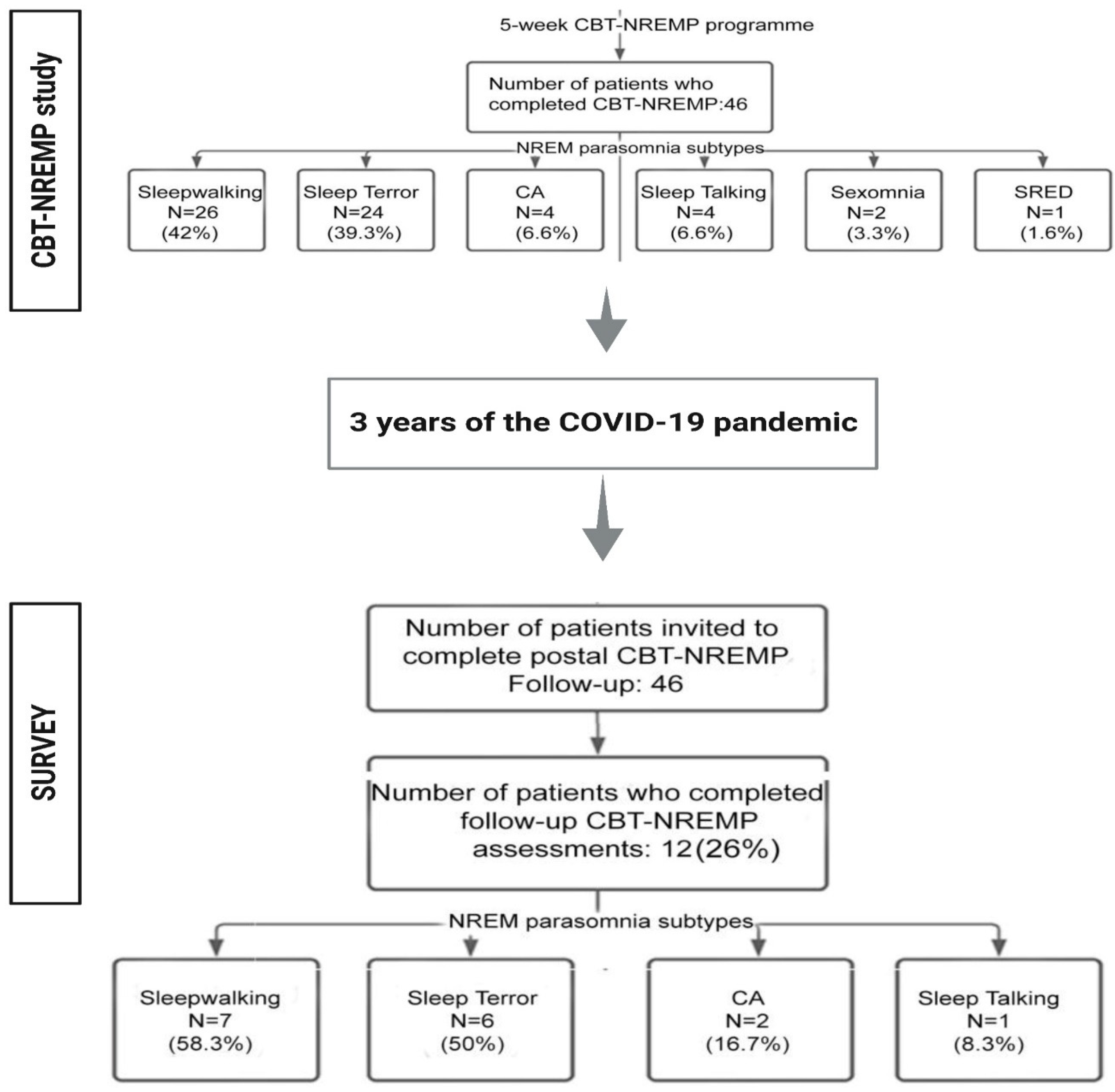
2.1. Design, Ethics and Data Collection
2.2. Statistical Analysis
3. Results
3.1. Preliminary Findings on Sustainability of the CBT-NREMP Intervention
3.2. Comparisons between Survey Responders and Non-Responders
3.3. Impact of COVID-19 Lockdowns as Explored by ICLQ
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Castelnovo, A.; Lopez, R.; Proserpio, P.; Nobili, L.; Dauvilliers, Y. Nrem sleep parasomnias as disorders of sleep-state dissociation. Nat. Rev. Neurol. 2018, 14, 470–481. [Google Scholar] [CrossRef] [PubMed]
- O’Regan, D.; Nesbitt, A.; Biabani, N.; Drakatos, P.; Selsick, H.; Leschziner, G.D.; Steier, J.; Birdseye, A.; Duncan, I.; Higgins, S.; et al. A novel group cognitive behavioral therapy approach to adult non-rapid eye movement parasomnias. Front. Psychiatry 2021, 12, 679272. [Google Scholar] [CrossRef] [PubMed]
- Drakatos, P.; Marples, L.; Muza, R.; Higgins, S.; Gildeh, N.; Macavei, R.; Dongol, E.M.; Nesbitt, A.; Rosenzweig, I.; Lyons, E.; et al. Nrem parasomnias: A treatment approach based upon a retrospective case series of 512 patients. Sleep Med. 2019, 53, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.L.; Foldvary-Schaefer, N. Clinical neurophysiology of nrem parasomnias. Handb. Clin. Neurol. 2019, 161, 397–410. [Google Scholar] [PubMed]
- Arnulf, I.; Zhang, B.; Uguccioni, G.; Flamand, M.; Noel de Fontreaux, A.; Leu-Semenescu, S.; Brion, A. A scale for assessing the severity of arousal disorders. Sleep 2014, 37, 127–136. [Google Scholar] [CrossRef]
- Ito, E.; Inoue, Y. The International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA; Nihon Rinsho: Osaka, Japan, 2015; Volume 73. [Google Scholar]
- Bargiotas, P.; Arnet, I.; Frei, M.; Baumann, C.R.; Schindler, K.; Bassetti, C.L. Demographic, clinical and polysomnographic characteristics of childhood- and adult-onset sleepwalking in adults. Eur. Neurol. 2017, 78, 307–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montplaisir, J.; Petit, D.; Pilon, M.; Mongrain, V.; Zadra, A. Does sleepwalking impair daytime vigilance? J. Clin. Sleep Med. 2011, 7, 219. [Google Scholar] [CrossRef] [Green Version]
- Manfredini, D.; Arreghini, A.; Lombardo, L.; Visentin, A.; Cerea, S.; Castroflorio, T.; Siciliani, G. Assessment of anxiety and coping features in bruxers: A portable electromyographic and electrocardiographic study. J. Oral Facial Pain Headache 2016, 30, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Ingravallo, F.; Poli, F.; Gilmore, E.V.; Pizza, F.; Vignatelli, L.; Schenck, C.H.; Plazzi, G. Sleep-related violence and sexual behavior in sleep: A systematic review of medical-legal case reports. J. Clin. Sleep Med. 2014, 10, 927–935. [Google Scholar] [CrossRef] [Green Version]
- Gorgoni, M.; Scarpelli, S.; Mangiaruga, A.; Alfonsi, V.; Bonsignore, M.R.; Fanfulla, F.; Ferini-Strambi, L.; Nobili, L.; Plazzi, G.; De Gennaro, L.; et al. Persistence of the effects of the COVID-19 lockdown on sleep: A longitudinal study. Brain Sci. 2021, 11, 1520. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, I.; Mitrecic, D.; Petanjek, Z.; Duffy, B.; Young, A.H.; Nesbitt, A.D.; Morrell, M.J. Does damage to hypothalamic paraventricular nucleus underlie symptoms of ultradian rhythm disorder and an increased anxiety in coronavirus disease 2019? Croat. Med. J. 2020, 61, 377–380. [Google Scholar] [CrossRef] [PubMed]
- O’Regan, D.; Jackson, M.L.; Young, A.H.; Rosenzweig, I. Understanding the impact of the COVID-19 pandemic, lockdowns and social isolation on sleep quality. Nat. Sci. Sleep 2021, 13, 2053–2064. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; et al. SARS-Cov-2 is associated with changes in brain structure in uk biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Belleville, G.; Belanger, L.; Ivers, H. The insomnia severity index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Bastien, C. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Bishop, P.A.; Herron, R.L. Use and misuse of the likert item responses and other ordinal measures. Int. J. Exerc. Sci. 2015, 8, 297–302. [Google Scholar]
- Cellini, N.; Canale, N.; Mioni, G.; Costa, S. Changes in sleep pattern, sense of time and digital media use during COVID-19 lockdown in italy. J. Sleep Res. 2020, 29, e13074. [Google Scholar] [CrossRef]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of COVID-19 lockdown on mental health and sleep disturbances in italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef]
- Magill, E.; Siegel, Z.; Pike, K.M. The mental health of frontline health care providers during pandemics: A rapid review of the literature. Psychiatr. Serv. 2020, 71, 1260–1269. [Google Scholar] [CrossRef] [PubMed]
- Perlis, M.L. Cognitive Behavioral Treatment of Insomnia: A Session-by-Session Guide; Springer: New York, NY, USA, 2005; p. xviii. 182p. [Google Scholar]
- Hibbard, J.H.; Greene, J. What the evidence shows about patient activation: Better health outcomes and care experiences; fewer data on costs. Health Aff. 2013, 32, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.; Casement, M.D.; Kalmbach, D.A.; Castelan, A.C.; Drake, C.L. Digital cognitive behavioral therapy for insomnia promotes later health resilience during the coronavirus disease 19 (COVID-19) pandemic. Sleep 2021, 44, zsaa258. [Google Scholar] [CrossRef] [PubMed]
- Arnedt, J.T.; Conroy, D.A.; Mooney, A.; Furgal, A.; Sen, A.; Eisenberg, D. Telemedicine versus face-to-face delivery of cognitive behavioral therapy for insomnia: A randomized controlled noninferiority trial. Sleep 2021, 44, zsaa136. [Google Scholar] [CrossRef]
- Kaplowitz, M.D.; Hadlock, T.D.; Levine, R. A comparison of web and mail survey response rates. Public Opin. Q. 2004, 68, 94–101. [Google Scholar] [CrossRef] [Green Version]
- Simon, J.R.; Howard, J.H.; Howard, D.V. Adult age differences in learning from positive and negative probabilistic feedback. Neuropsychology 2010, 24, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Stedman, R.C.; Connelly, N.A.; Heberlein, T.A.; Decker, D.J.; Allred, S.B. The end of the (research) world as we know it? Understanding and coping with declining response rates to mail surveys. Soc. Nat. Resour. 2019, 32, 1139–1154. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Assessment n = 12 | PRE | POST | ||
|---|---|---|---|---|
| Mean (SD) | Median (Q1, Q3) | Mean (SD) | Median (Q1, Q3) | |
| ISI | 12.17 (3.71) | 12.5 (11, 14.25) | 11.75 (5.5) | 10 (7.75, 17.25) |
| HADS | 11.25 (5.15) | 12 (8.25, 15) | 15.9 (6.01) | 16 (11.25, 17.75) |
| HADS_A | 5 (2.52) | 5.5 (3, 6) | 6.9 (2.18) | 8 (6, 8) |
| HADS_D | 6.25 (4.18) | 6.5 (3, 9.25) | 9 (4.52) | 8 (6.25, 10) |
| PADSS | 19.08 (4.25) | 20 (15, 21) | 16.67 (3.58) | 17 (14, 18.5) |
| PADSS_A | 9.42 (3.85) | 9.5 (6.5, 11.25) | 7.08 (3.23) | 8 (4.5, 9.25) |
| PADSS_B | 4.42 (1) | 4 (4, 5) | 4 (1.54) | 4 (4, 4.25) |
| PADSS_C | 5.25 (1.82) | 5 (4, 7) | 4.27 (2) | 5 (3.5, 5.5) |
| PRE | POST | Different from PRE to POST Median (Q1, Q3) | Wilcoxon Signed-Rank Test ** | p * |
|---|---|---|---|---|
| SI.Pre | ISI.Post | −2 (−5.25, 4.5,) | 42 | 1 |
| HADS.Pre | HADS.Post | 3 (−2, 6.25) | 11 | 0.816 |
| HADS_A.Pre | HADS_A.Post | 2 (0, 3.5) | 6 | 0.84 |
| HADS_D.Pre | HADS_D.Post | 0.5 (−1.5, 5.5) | 12 | 1 |
| PADSS.Pre | PADSS.Post | −2.5 (−4, −0.75) | 50 | 0.194 |
| PADSS_A.Pre | PADSS_A.Post | −2 (−4, −0.75) | 52.5 | 0.094 |
| PADSS_B.Pre | PADSS_B.Post | 0 (−0.25, 0) | 6 | 1 |
| PADSS_C.Pre | PADSS_C.Post | 0 (−1.5, 0) | 19 | 0.719 |
| Responders (n = 12) | ||
|---|---|---|
| F Statistics (Degree of Freedom) | p-Value | |
| ISI | 0.495 | 0.614 |
| HADS | 1.654 | 0.208 |
| HADS_A | 1.495 | 0.240 |
| HADS_D | 0.946 | 0.399 |
| PADSS | 1.938 | 0.160 |
| PADSS_A | 2.627 | 0.087 |
| PADSS_B | 0.500 | 0.611 |
| PADSS_C | 0.941 | 0.401 |
| Non-Responders (n = 34) | Responders (n = 12) | p-Value | |
|---|---|---|---|
| Gender (%) | |||
| Male | 19 (55.9) | 7 (58.3) | p = 1.000 * |
| Female | 15 (44.1) | 5 (41.7) | |
| Age—mean (SD) | 32.8 (10.1) | 39.8 (9.4) | p = 0.042 ** |
| Pre—mean (SD) | |||
| ISI | 15.2 (4.5) | 13.5 (4.1) | p = 0.251 ** |
| HADS | 14.5 (6.2) | 12.9 (6.8) | p = 0.480 ** |
| HADS_A | 6.7 (4.7) | 5.8 (2.9) | p = 0.449 ** |
| HADS_D | 7.9 (4.4) | 7.2 (5.3) | p = 0.686 ** |
| PADSS | 19.2 (6.4) | 20.1 (5.1) | p = 0.636 ** |
| PADSS_A | 9.4 (4.7) | 10.6 (4.3) | p = 0.436 ** |
| PADSS_B | 4.5 (1.2) | 4.4 (0.9) | p = 0.877 ** |
| PADSS_C | 5.3 (1.8) | 5.1 (1.6) | p = 0.690 ** |
| Post—mean (SD) | |||
| ISI | 12.8 (4.2) | 12.2 (3.7) | p = 0.658 ** |
| HADS | 13.3 (6.5 | 11.2 (5.2) | p = 0.284 ** |
| HADS_A | 6.3 (4.4) | 5 (2.5) | p = 0.238 ** |
| HADS_D | 7 (3.8) | 6.2 (4.2) | p = 0.581 ** |
| PADSS | 17 (5.6) | 19.1 (4.3) | p = 0.203 ** |
| PADSS_A | 8 (4.2) | 9.4 (3.8) | p = 0.304 ** |
| PADSS_B | 4.3 (1.2) | 4.4 (1) | p = 0.819 ** |
| PADSS_C | 4.6 (2) | 5.2 (1.8) | p = 0.344 ** |
| Scale | Wilcoxon Signed-Rank Test Statistic | p * |
|---|---|---|
| ISI | 249.5 | 0.037 * |
| HADS | 184 | 0.509 |
| HADS_A | 157 | 1 |
| HADS_D | 234 | 0.434 |
| PADSS | 203.5 | 0.016 * |
| PADSS_A | 248.5 | 0.159 |
| PADSS_B | 46 | 1 |
| PADSS_C | 146.5 | 0.289 |
| Variable | n (Not Missing) | Mean (SD) | Median (Q1, Q3) |
|---|---|---|---|
| NREM events deteriorated | 12 | 6.17 (1.34) | 6.5 (5, 7) |
| Sleep deteriorated | 12 | 6.08 (1.78) | 6 (5, 7.25) |
| Lockdown continues to adversely affect my sleep | 12 | 5.08 (2.11) | 5 (3.75, 6.25) |
| Increased sleep onset latency | 12 | 5 (2.37) | 5 (4.5, 7) |
| Increased wake-after-sleep-onset | 12 | 5 (2.52) | 5 (3, 7) |
| Difficult to rise on time | 12 | 7.25 (2.18) | 7 (5, 9.25) |
| Excessive daytime somnolence | 12 | 4.92 (2.61) | 5 (3, 6.25) |
| Poor sleep quality | 12 | 6.25 (2.6) | 7 (4.75, 8) |
| Increased daytime tiredness | 12 | 6.5 (2.28) | 7 (5, 8) |
| Overactive mind at night | 12 | 7.08 (1.78) | 7.5 (5.75, 8) |
| Mood deteriorated | 12 | 6.25 (2.42) | 7 (4.75, 8) |
| Increased anxiety | 12 | 6.92 (2.35) | 7 (6, 8.25) |
| Increased depression | 12 | 6.17 (2.52) | 7 (5.75, 7.25) |
| Increased stress | 12 | 7.17 (2.62) | 8 (7, 8.25) |
| Reduced engagement with exercise | 12 | 5.75 (3.02) | 7 (2.75, 8) |
| Increased alcohol consumption | 12 | 6.17 (2.21) | 6.5 (5, 8) |
| Increased illicit substance use | 12 | 3.25 (2.01) | 4.5 (1, 5) |
| Poor diet | 12 | 6.42 (1.68) | 7 (6, 7.25) |
| Increased loneliness | 12 | 5.5 (2.24) | 5.5 (5, 7.25) |
| Relationships were adversely affected | 12 | 6.17 (2.72) | 7 (5.75, 8) |
| Ability to communicate with others were adversely affected | 12 | 6.17 (2.72) | 7 (5.75, 8) |
| Finances were adversely affected | 12 | 5 (1.86) | 5 (4, 6) |
| Working from home had a negative impact on my general wellbeing | 12 | 6.08 (2.35) | 6 (5.75, 7.25) |
| My responsibilities increased | 12 | 5 (2.86) | 5 (4, 7) |
| The negative effects of lockdown continue to impact my general wellbeing | 12 | 5.67 (2.23) | 6 (5, 7.25) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laroche, M.; Biabani, N.; Drakatos, P.; Selsick, H.; Leschziner, G.; Steier, J.; Young, A.H.; Eriksson, S.; Nesbitt, A.; Kumari, V.; et al. Group Cognitive Behavioural Therapy for Non-Rapid Eye Movement Parasomnias: Long-Term Outcomes and Impact of COVID-19 Lockdown. Brain Sci. 2023, 13, 347. https://doi.org/10.3390/brainsci13020347
Laroche M, Biabani N, Drakatos P, Selsick H, Leschziner G, Steier J, Young AH, Eriksson S, Nesbitt A, Kumari V, et al. Group Cognitive Behavioural Therapy for Non-Rapid Eye Movement Parasomnias: Long-Term Outcomes and Impact of COVID-19 Lockdown. Brain Sciences. 2023; 13(2):347. https://doi.org/10.3390/brainsci13020347
Chicago/Turabian StyleLaroche, Matthias, Nazanin Biabani, Panagis Drakatos, Hugh Selsick, Guy Leschziner, Joerg Steier, Allan H. Young, Sofia Eriksson, Alexander Nesbitt, Veena Kumari, and et al. 2023. "Group Cognitive Behavioural Therapy for Non-Rapid Eye Movement Parasomnias: Long-Term Outcomes and Impact of COVID-19 Lockdown" Brain Sciences 13, no. 2: 347. https://doi.org/10.3390/brainsci13020347